1. Introduction
Obesity is a serious problem today. The worldwide prevalence of overweight and obesity has doubled since 1980. Almost a third of the world’s population is now classified as overweight or obese [
1]. Globally, the numbers of overweight and obese people are increasing dramatically. Current estimates suggest that up to 2.7 billion adults will be overweight or obese in 2025. Meanwhile, treatment for the obese is already in the trillions of dollars. The International Diabetes Federation (IDF) says that, over the next 25 years, there will be an increase in the number of diabetics in Europe of around 1 million new sufferers per year. The Ministry of Health of the Czech Republic reports that the direct cost of treating obese sufferers currently accounts for about 10% of the total health expenditure, and is thus around tens of billions of crowns per year. A 2013 Stenmark survey shows that 34% of adults are overweight and 21% of the population is obese. This corresponds to our results from the tested respondents.
The evolution of expenditure on obesity treatment in the Czech Republic is steadily increasing at an average annual rate of 8.95%. It is evident that, unless the trend in obesity numbers changes, it may become a real economic problem in the future, as spending on obesity treatment contributes more and more to the overall costs of the health system. The annual cost of treating a severely obese patient is over 100,000 CZK, and there are over 200,000 of these patients in the Czech Republic. Research has also shown that overweight people rarely take the time to analyse the diet and nutritional values of foods. Changing their approach to diet can be a key guide for them to start tackling their obesity.
In recent years, the increasing obesity of mankind and the associated health complications and the rise in health service expenditure have often been discussed. The subject of this article is an assessment of the current state of health and its sustainability in the Czech Republic based on an analysis of the development of the number of obese people and health care expenses for the obese population. The issue of obesity is also closely linked to the quality of food intake and the monitoring of nutritional values of food in the diet. The research thus involved evaluating and monitoring the nutritional values of people with different BMIs and finding a correlation between the nutritional values studied and the prevalence of obesity. This research is based on primary data obtained from a questionnaire survey of 324 respondents.
Food quality and the impact of junk and unhealthy foods on people’s health, sugar consumption, rising obesity, and the associated increase in spending on health services related to the treatment of obesity and accompanying diseases (such as diabetes, heart attack, and others) are, of course, also factored into the economic sustainability of this trend.
Individual demand is dependent on several factors, in particular its preferences [
2]. In recent years, these preferences have tilted strongly in favour of quality food, as the growing interest in healthy lifestyles in the growth of civilisation diseases, stress, and over-consumption of carbohydrates currently plays an important role in the thinking of individuals [
3]. Sugar is a commodity that is one of the key ingredients in our diet and cannot be completely taken off the menu [
4]. This is evidenced by the Czech Statistical Office, which shows a stable consumption of sugar that does not fall below 30 kg per person per year (beet sugar and cane sugar) [
5]. White beet sugar is currently the most used sweetener, even though many people rank it as harmful to health. Pitha [
6] points to the effect of its consumption on the growth of obesity and depression [
7]. As a result, there is growing demand for healthy, organic foods, and products with lower sugar content, although less sugar does not necessarily mean fewer calories [
8]. As Magkos points out [
9], consumers are dissatisfied with the quality of classic, conventional meals and so focus more attention on analysing the impact of traditional foods on our health [
10]. This is most often owing to the need to protect your and your family’s health [
11,
12]. Thanks to all these arguments, the number of organic farmers has grown considerably in recent years.
Using a questionnaire survey, the article examines the consumer habits of monitoring the nutritional values of foods in people with healthy and unhealthy BMIs and those engaged in regular sports, and vice versa. For example, whether people regularly take any supplements is also linked to a healthy lifestyle. As stated by Maughan [
13], approximately 85% of athletes take at least some dietary supplements. Froiland [
14] confirms this statement with research findings that dietary supplements are used by 89% of surveyed athletes. Research was carried out on German athletes by Braun et al. [
15], who concluded that more than 80% of athletes use some form of dietary supplement. Researchers such as Weiss [
16] deal with theories of athlete motivation. Theories of personality and the psychology of athletes, including their motivations and approach to health and healthy food, are addressed by Vealey [
17]. The role of gender in sport and exercise is addressed by Gill [
18].
Research logically confirms that healthy and organic foods purchased, e.g., at farmers markets are beneficial for health, as opposed to chemically modified and preserved foods. Farmers’ markets are places to buy healthy and fresh food [
19,
20,
21], but in recent years, their benefits have gone beyond the mere purchase of food. Farmers’ markets also meet the needs of consumers who shop in accordance with ethical obligations, environmental responsibilities, and green principles [
22]. Several studies on consumer incentives in farmers’ markets have been carried out to support the marketing of vendors [
23]. The growing number of farmers focusing on high-quality organic food [
24] stems from the growing demand of customers and their interest in the quality and composition of the food they consume [
25]. The issue of nutritional value and consumer incentives has also been addressed by Kozior et al. [
26].
This issue is also connected with sustainable agriculture, which means obtaining healthy and quality foods, conserving natural resources, and preserving biodiversity [
27]. Generally, sustainable development is one of the main objectives of the European Union. Sustainable economic development is also one of the main objectives of the common EU agricultural policy [
28]. According to its principles, the economic aspect of the development should perceive society and the natural environment not as its inhibitors, but rather as stimulants [
29,
30,
31,
32]. Prus [
30] further adds that sustainable development in agriculture means such programming of farming production so that it makes reasonable use of natural resources and the environment. It provides sufficient amounts of food while maintaining its high quality.
The importance of the food safety area is revealed by the very large amount of European acts passed during the year 2007 in order to regulate this area. With a total number of 309 passed regulatory acts, the veterinary sanitary and food safety area is subjected to a significant legislative pressure [
33,
34,
35,
36].
The aim of the text presented is to assess the sustainability of the trend of increasing numbers of overweight people (and suffering from health problems associated with it), increasing sugar consumption and spending on obesity treatment. At the same time, the article presents and analyses the results of its own primary research conducted on a group of people in the Czech Republic with a healthy and unhealthy BMI. The aim of this research was to analyse the consumer behaviour of these respondents in the Czech Republic, with emphasis on their consumption habits in health food shops and in particular their habits in monitoring the nutritional values of foods. In the first phase of research, an analysis of secondary data is carried out, namely data on the development of obesity numbers and the cost of obesity treatment, in order to detect a country-wide trend in development. In the second phase of the research, the results from the analysis of secondary data are confronted with primary data on the current consumer habits of the Czech population in the area of monitoring nutritional values.
2. Materials and Methods
The theoretical basis of the article was processed through the analysis and subsequent synthesis of secondary sources, and the basic method used was the examination of documents, in particular scientific articles, and professional publications. Statistical data and some additional information were obtained from current official Internet sources, the Czech Statistical Office, and Eurostat.
Analysis of time series, research on trend of number of obese in CR:
The first phase of the research is based on an analysis of time series, namely time series for the development of the number of overweight persons and an assessment of the costs of treating these persons. In particular, the time series analysis used trend analysis and the growth rate was assessed. Trend time series methods were used to analyse and predict the future development of the indicators. The choice of the appropriate trend function was evaluated using interpolation criteria and criteria from regression analysis. A function is selected that shows the minimum
MSE (mean square error) criterion is classified as statistically significant by the F-test, and a determination coefficient (R
2) has managed to explain a sufficient percentage of variability of the dependent variable. The
MSE is determined using the formula:
where
T is the number of observations,
yt are the measured values, and
are the expected values. This is one of the most widely used methods of interpolation, and by default, the best function is the one with the smallest
MSE. As a base, linear and quadratic regression functions were used to account for the evolution of time series.
Analysis of primary data, results from questionnaire investigation on access of Czech citizens to monitoring nutritional values of food:
The second stage of the research consists of analyzing the results of the questionnaire investigation. The primary data were obtained by conducting a questionnaire investigation to analyse consumer behavior regarding the monitoring of the nutritional values of the purchased foods depending on their BMI (BMI is calculated using the ratio between bodyweight in kg and height in meters squared). Primary data are thus based on quantitative research using a data collection questionnaire technique. The sample of respondents was obtained by deliberate selection, and respondents were selected considering the minimum education rate at the level of secondary education. The criterion of having at least secondary education was chosen on the basis of the fact that the population with secondary education forms the dominant group of the population and is thus a representative sample for the population of the Czech Republic. The research was carried out in 2020 in the months of January to March. The questionnaire survey was conducted throughout the Czech Republic, and the respondents were asked to fill out the questionnaire in printed form.
Respondents were addressed randomly in various cities in the Czech Republic. After verifying the level of education, they were asked to complete a printed questionnaire. At the same time, the questionnaire was distributed to students of distance learning at universities who ensure they have a minimum secondary education. A total of 324 respondents participated in the questionnaire, representing an 82% return after discarding blank or incomplete questionnaires (a total of 395 questionnaires were obtained and 71 of them were excluded). The minimum number of questionnaires needed to evaluate the research hypotheses was set at 250. The gender composition of respondents was 174 (54%) male and 150 (46%) females. The age mix of respondents was divided into groups of 0–20 years, 21–30 years, 31–40 years, 41–50 years, 51–60 years, and 61 years or more. The 21–30-year-old group had the highest representation, with 146 respondents (45%), 88 respondents (27%) from the 31–40-year-old group, and 58 respondents (18%) from the 41–50-year-old group. The composition of respondents according to their BMI was as follows: 194 respondents (60%) had a normal BMI (i.e., a BMI in the range of 18.5–24.9); 82 respondents (25.3%) were overweight (i.e., had BMI values reaching 25–29.9); 42 respondents (i.e., 12.9%) were obese (with a BMI above 30); and 6 respondents had a BMI below the normal values, i.e., below 18. The following
Table 1 shows the basic characteristics of the respondents.
Respondents were further monitored by residence and their net monthly income. Here, the Central Bohemian region and people with income of 20,000–30,000 CZK had the absolute largest representation. Of the total number of respondents, a total of 320 (or 98.8%) respondents reported taking up sports activities (at least intermittently).
Absolute and relative frequencies were used in the descriptive statistics, and the data obtained were analysed using contingency tables and the chi square test. The obtained contingency tables contain the observed frequencies from the questionnaire survey of individual combinations of variables. From the differences (residues) of the observed frequencies and the frequencies obtained from the assumption of the null hypothesis, the total normalized residue is calculated. If its value is less than the critical value of distribution χ2 at the significance level 0.95 for the appropriate degree of freedom, the null hypothesis cannot be rejected at a significance level of 95%.
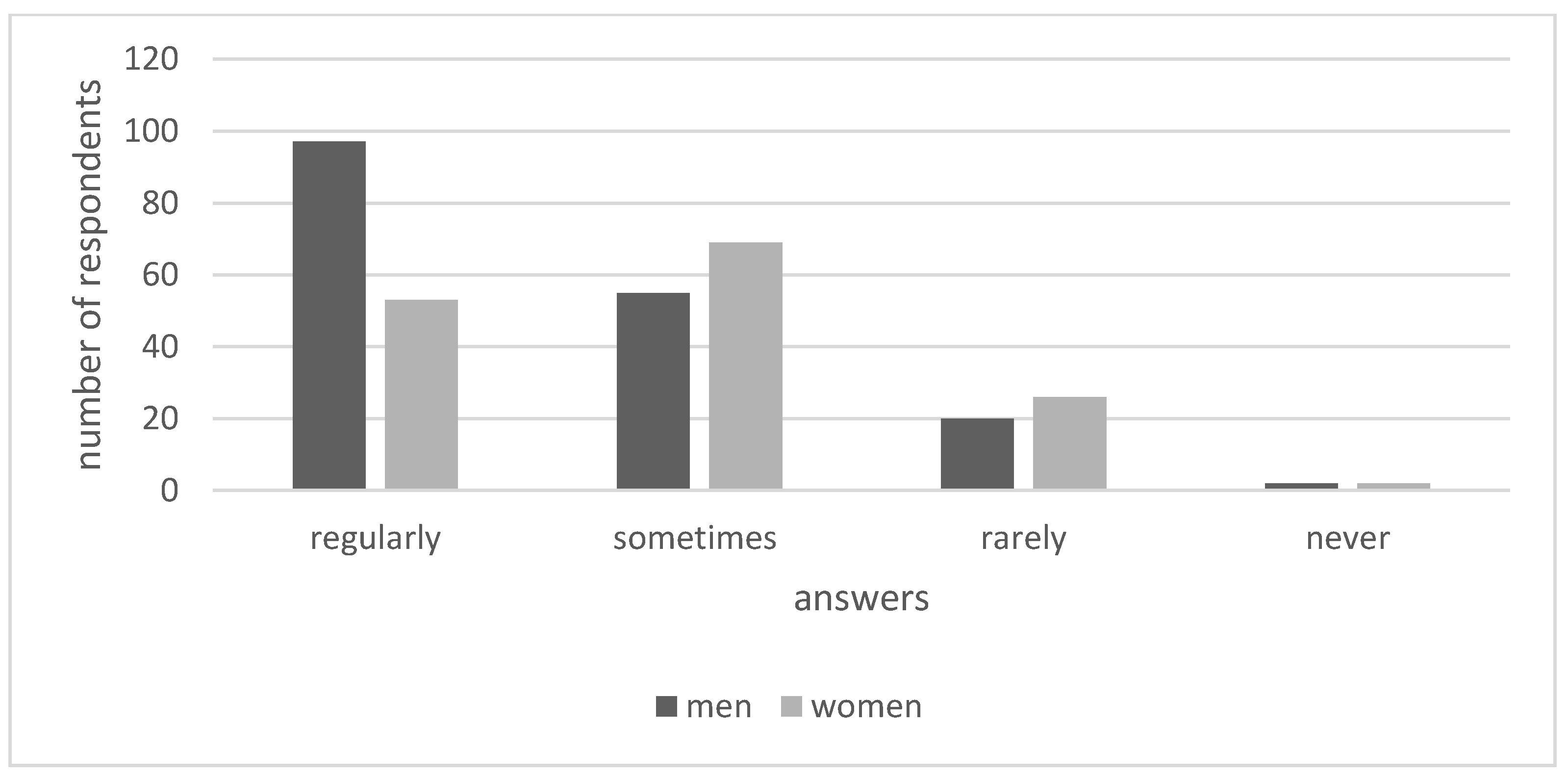
The basic characteristics of the respondents are supplemented by the following figure. The
Figure 1 shows the respondents answer to the frequency of their sport activities.
The analysis of the primary data was focused on testing the following null hypotheses. In the first stage, the respondents’ purchases in health food stores and the amount spent in these stores were analysed. It was determined whether these variables correlate with gender, age, income, and BMI.
Hypotheses 1 (H1). There is no dependency between shopping in health food stores and the gender of the respondents.
Hypotheses 2 (H2). There is no dependency between shopping in health food stores and the age of the respondents.
Hypotheses 3 (H3). There is no dependency between shopping in health food stores and the income of the respondents.
Hypotheses 4 (H4). There is no dependency between shopping at health food stores and the size of respondents’ BMIs.
Hypotheses 5 (H5). There is no dependency between the amount spent in health food stores and the gender of the respondents.
Hypotheses 6 (H6). There is no dependency between the amount spent in health food stores and the age of the respondents.
Hypotheses 7 (H7). There is no dependency between the amount spent in health food stores and the income of the respondents.
Hypotheses 8 (H8). There is no dependency between the amount spent in health food stores and the size of the respondents’ BMIs.
The second stage of the research focused on analysing the degree to which the respondents monitored nutritional values. The correlation between the monitoring of nutritional values and the gender, age, level of income, and BMI of the respondents was examined. The examination of the degree to which the respondents monitored the sugar content in their food was of key importance.
Hypotheses 9 (H9). There is no dependency between the monitoring of selected nutritional values and gender.
Hypotheses 10 (H10). There is no dependency between the monitoring of selected nutritional values and the age of the respondents.
Hypotheses 11 (H11). There is no dependency between the monitoring of selected nutritional values and the income of the respondents.
Hypotheses 12 (H12). There is no dependency between the monitoring of selected nutritional values and the size of respondents’ BMIs.
Hypotheses 13 (H13). There is no dependency between the type of nutritional value monitored and the gender of the respondents.
Hypotheses 14 (H14). There is no dependency between the type of nutritional value monitored and the age of the respondents.
Hypotheses 15 (H15). There is no dependency between the type of nutritional value monitored and the income of the respondents.
Hypotheses 16 (H16). There is no dependency between the type of nutritional value monitored and the size of respondents’ BMIs.
3. Results
The evolution of absolute indicators was expressed and evaluated to analyse the evolution of the number of overweight and obese people. The assessment showed clear growth with an average annual growth rate of 3.4% per year.
The evolution of absolute indicators corresponds to a linear function, as illustrated in
Figure 2. A regression analysis was carried out to detect and describe the function characterising the evolution of absolute indicators. The linear trend function managed to explain 94.66% of the variability of the dependent variable. We assess the significance of the model using the
p-value (the smallest level of significance at which we reject the zero hypothesis of the insignificance of the model), which shows a value of 0.004198. The
p-value is less than the default chosen materiality level of 5%, so we confirmed significance of the linear model. The estimate of the regression coefficient (β0) gives a value of 43.753 and the estimate of the slope parameters of the regression line is 2.0085. Thus, the evolution function of the absolute indicator of overweight and obese people is described by the following:
where
y is an absolute indicator of the number of obese and overweight people and
t is the years. This function then simulates the values for the expected absolute values of this indicator for the following period. This prediction is also captured in
Figure 2.
Expenditure on treating obese people is also rising in response to the growing number of obese people. The
Table 2 shows the evolution of the cost of treating the obesity of insured persons of the Czech Industrial Health Insurance Corporation (CIHIC).
The following research was thus focused on research into respondents’ approach to monitoring food nutritional values. The findings of the questionnaire analysis are interpreted as follows in
Table 3.
In the last stage of the research, the specific nutritional values monitored by the respondents were examined. The respondents had calories, energy values, carbohydrates, vitamins, minerals, and sugar from which to choose. Calories were the most monitored nutritional value by a clear margin, followed by carbohydrates and sugars. The analysis showed that, except for minerals, all the monitored values are monitored more by women than by men. Fifty-nine percent of all the respondents (54% of men and 46% of women) consume added sugar. The results of monitored nutritional values by gender shows
Figure 3. Alcohol consumption is closely related to BMI and health. The Czech Republic is a leader in alcohol consumption. The following
Figure 4 shows alcohol consumption in the Czech Republic.
The demonstrated growing wine consumption also corresponds to the results of the authors’ survey. The respondents, on whose questioning the presented research was based, were also asked about alcohol (i.e., wine) consumption. Women have a higher frequency of wine consumption than men, wine consumption increases with age, and wine consumption is higher in people with a lower education. White wine consumption is significantly higher. White wine is the clear preference of women, and it also dominates across all age categories. The consumption of semi-sweet wines clearly dominates the discussion on wine consumption in relation to the sugar content in wine. In groups with higher levels of education, the consumption of sweet wines is lower and consumer preferences are shifted in favor of dry wines. Consumption of dry wines also increases with income, and consumption of sweet wines decreases with increasing income. Of course, added sugars in alcohol have a negative effect on BMI, but a correlation between BMI development and wine consumption has not been demonstrated. This also corresponds to the conclusions of the study by Kleiner et al. [
38].
4. Discussion
Hypotheses 1 (H1): There is no dependency between shopping in health food stores and the gender of the respondents. The value of the calculated statistic χ2 (18.911) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. The strength of dependence measured by Cramer’s V is 0.242. There is a correlation between shopping in health food stores and gender, but the strength of dependence measured by Cramer’s V is weak. From the respondents, women shop in health food stores more than men (88% of women stated that they shop in health food stores at least occasionally, while in the case of male respondents, it was 70%).
Hypotheses 2 (H2): There is no dependency between shopping in health food stores and the age of the respondents. The value of the calculated statistic χ2 (54.355) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. The strength of dependence measured by Cramer’s V is 0.205. There is a correlation between shopping in health food stores and the age of the respondents, but the strength of dependence measured by Cramer’s V is weak. Research on differences has shown that the 21–30 age group shops the most in health food stores.
Hypotheses 3 (H3): There is no dependency between shopping in health food stores and the income of the respondents. The value of the calculated statistic χ2 (43.499) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. There is a correlation between shopping in health food stores and the respondents’ income. However, the strength of dependence measured by Cramer’s V is weak (0.183). The largest group of respondents who shop in health food stores is inhabitants with incomes ranging between 20,000 and 30,000 CZK per month.
Hypotheses 4 (H4): There is no dependency between shopping at health food stores and the size of respondents’ BMIs. The value of the calculated statistic χ2 (18.459) is greater than the critical value χ2 of the 3-degree freedom distribution at the probability level of 0.95. The zero hypothesis can thus be rejected. There is an connection between shopping at health food stores and the BMI of respondents. However, the dependency strength measured by Cramer’s V is weak (0.089).
Hypotheses 5 (H5): There is no dependency between the amount spent in health food stores and the gender of the respondents. The value of the calculated statistic χ2 (2.767) is less than the critical value χ2 of the 1-degree freedom distribution at a probability level of 0.95. The zero hypothesis cannot thus be dismissed, and it cannot be concluded that there is a relationship between the level of spending in health food shops and gender. Differentiation research has shown that women spend more than men in these stores.
Hypotheses 6 (H6): There is no dependency between the amount spent in health food stores and the age of the respondents. The value of the calculated statistic χ2 (48.132) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. A correlation was found between age and the amount spent in health food stores. The strength of dependence measured by Cramer’s V is 0.193.
Hypotheses 7 (H7): There is no dependency between the amount spent in health food stores and the income of the respondents. The value of the calculated statistic χ2 (58.874) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. Therefore, the null hypothesis can be rejected, and it can be concluded that there is a correlation between the income of the respondents and the amount spent in health food stores. The strength of dependence measured by Cramer’s V is 0.213.
Hypotheses 8 (H8): There is no dependency between the amount spent in health food stores and the size of the respondents’ BMIs. The value of the calculated statistic χ2 (12.452) is greater than the critical value χ2 of the 3-degree freedom distribution at the probability level of 0.95. The zero hypothesis can thus be dismissed, stating that there is a dependency between the BMI of respondents and the level of spend in health food shops. The dependency strength measured by Cramer’s V is 0.087.
Hypotheses 9 (H9): There is no dependency between the monitoring of selected nutritional values and gender. The value of the calculated statistic χ2 (2.126) is smaller than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus not be rejected. There is no correlation between the monitoring of selected nutritional values and gender.
Hypotheses 10 (H10): There is no dependency between the monitoring of selected nutritional values and the age of the respondents. The value of the calculated statistic χ2 (31.931) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. A correlation was confirmed between age and the monitoring of nutritional values. Research on differences has shown that people aged 21–30 monitor nutritional values the most. However, the strength of dependence measured by Cramer’s V is weak (0.157). Coufalová [39] came to a similar conclusion, namely that Czech athletes are interested in their diet and that there is a correlation between age and interest in quality of food. The conclusions correspond to the conclusions of Ronsen et al. [40] concerning the eating habits of Norwegian athletes, which state that 80% of respondents have good eating habits. Burke et al. [41] published a study looking at the eating habits of athletes in the Australian Olympic team, in which it examined the quality of their diet and came to a similar conclusion. Research on athletes’ eating habits has also been conducted by Sundgot [42], who states that the difference in the use of dietary supplements between elite athletes in Norwegian national teams and randomly selected Norwegian athletes is statistically significant only for men. Hypotheses 11 (H11): There is no dependency between the monitoring of selected nutritional values and the income of the respondents. The value of the calculated statistic χ2 (25.020) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. A correlation was found between the income of the respondents and the monitoring of nutritional values of food. However, the strength of dependence measured by Cramer’s V is low (0.139).
Hypotheses 12 (H12): There is no dependency between the monitoring of selected nutritional values and the size of respondents’ BMIs. The value of the calculated statistic χ2 (10.267) is greater than the critical value χ2 of the 3-degree freedom distribution at a probability level of 0.95. The zero hypothesis can thus be rejected. A link between the monitoring of selected nutritional values and the size of respondents’ BMIs was shown. However, the dependency strength measured by Cramer’s V is low (0.085).
Hypotheses 13 (H13): There is no dependency between the type of nutritional value monitored and the gender of the respondents. The value of the calculated statistic χ2 (3.645) is less than the critical value χ2 of the 1-degree freedom distribution at the probability level of 0.95. Therefore, the zero hypothesis cannot be rejected. There was no evidence of a relationship between the type of nutritional value followed and the gender of respondents.
Hypotheses 14 (H14): There is no dependency between the type of nutritional value monitored and the age of the respondents. The value of the calculated statistic χ2 (59.010) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. The null hypothesis can thus be rejected. A correlation was found between the observed nutritional values and the age of the respondents. However, the strength of dependence measured by Cramer’s V is again very low (0.158).
Hypotheses 15 (H15): There is no dependency between the type of nutritional value monitored and the income of the respondents. The value of the calculated statistic χ2 (35.499) is greater than the critical value of distribution χ2 by 1 degree of freedom at the probability level of 0.95. Therefore, the null hypothesis can be rejected, and it can be concluded that there is a correlation between the monitored nutritional values and the respondents’ level of income. The strength of dependence measured by Cramer’s V is 0.122.
Hypotheses 16 (H16): There is no dependency between the type of nutritional value monitored and the size of respondents’ BMIs. The value of the calculated statistic χ2 (3.059) is greater than the critical value χ2 of the 3-degree freedom distribution at the probability level of 0.95. Therefore, the zero hypothesis cannot be rejected. There was no evidence of a relationship between the type of nutritional value followed and the BMI of respondents. The research is complemented, for example, by Kolarzyk et al. [43]. BMI research in India was conducted by Naidu [44]. 






{kind=link}
{kind=link}
{kind=link}
{kind=link}