1. Introduction
The lung disease COVID-19, caused by the novel coronavirus SARS-CoV-2, reached the European continent in January 2020 and the World Health Organization (WHO) declared the disease a pandemic on the 11th March 2020 [
1]. As a reaction, traditional public health measures such as shelter-in-place orders, social distancing and quarantine were introduced by a large number of countries to curb the spread of the virus and lower incidence rates and mortality [
2]. In Germany, the lockdown measures affected all non-essential businesses, including sports clubs, fitness studios, activity trails and playgrounds [
3]. Working from home was very strongly encouraged whenever possible. People were allowed to leave their houses, but seeing more than one person other than those living in the same household was forbidden. Despite progress in vaccination, mathematical modelling projections suggest that social distancing might be intermittently necessary as long as into 2022 [
4]. Indeed, by now (spring 2021) many countries are in the third wave and have had to impose lockdowns again.
The pandemic itself and the public health measures taken in the effort to contain the spread of the virus have produced an unprecedented disruption of daily life and impacted health-related lifestyles [
5,
6]. A large number of studies have documented the reduction in physical activity (PA) in the general population during the first lockdown in the spring of 2020 [
7]. This is alarming since PA levels are already low in many Western countries, including Germany [
8], and because physical inactivity is one of the major modifiable risk factors for chronic diseases and conditions with the highest burden of disease and premature death [
9]. There is also irrefutable evidence on the beneficial effect of regular moderate PA on the immune system [
10]. Modifiable risk factors for severe COVID-19 disease include chronic, inflammatory lifestyle-dependent diseases, such as obesity, diabetes, hypertension and cardiovascular diseases [
11,
12]. Emerging evidence also suggests that PA [
13], as well as cardiorespiratory [
14] and muscular fitness [
15], might protect against severe COVID-19 disease (defined as hospitalization). In sum, regular PA is of utmost importance to maintain good health, and might play an as of now underappreciated role in COVID-19.
In the anticipation of further reduction of PA in the general population and as a countermeasure against confinement and loss of social contact, many governmental, professional PA and health organizations have started campaigns and urged the population to become or remain active [
16,
17,
18]. The WHO Regional Office for Europe has provided basic information on the relevance of PA during self-isolation and recommended ways to be active, one of which was following “online exercise classes” [
16]. Additionally, the National Health Service has emphasized the importance of maintaining PA for health in all age groups [
17]. The Centers for Disease Control and Prevention has also endorsed “workout videos” [
19]. The National Health Service has recommended online exercise classes in order to improve and maintain mental health [
20].
Technology-supported approaches to promote PA have been shown to be effective in increasing PA, walking and energy expended [
21,
22,
23]. These interventions, however, are at least partially theory-based and use different support mechanisms, such as tailored PA advice, goal setting, feedback, PA tracking, tele-counselling, online resources and online social support [
22,
23], which are not readily available with online exercise classes (OEC). OEC, however, seem to have apparent appeal in general, and in pandemic times in particular, since they are cost and time efficient and can be flexibly used in an environment with no infection risk. A recent multinational survey with 10,433 participants examined the interest in digital home exercise programs, and found that 68% of respondents reported such interest [
24]. However, interest is not the same as (regular) use. FFurthermore, the survey did not provide any data on users’ attitude towards the digital classes.
Since OEC have been widely encouraged as a potential means of maintaining PA during self-isolation, data on actual use is of high relevance. To the best of our knowledge, no study so far has assessed the use of and users’ attitudes towards OEC in an ecological sample. The aim of the present study was to determine whether respondents knew of and, if they did, used OEC and with which frequency in Germany during the first COVID-19 related lockdown in the spring of 2020. Further, we were interested in users’ attitudes towards OEC. We hypothesized that the majority of respondents were aware of OEC, but many less used them regularly. We also hypothesized that facilitating factors (e.g., time flexibility) were seen as attractive, whereas lack of social interaction and lack of trainer’s supervision were perceived as barriers.
4. Discussion
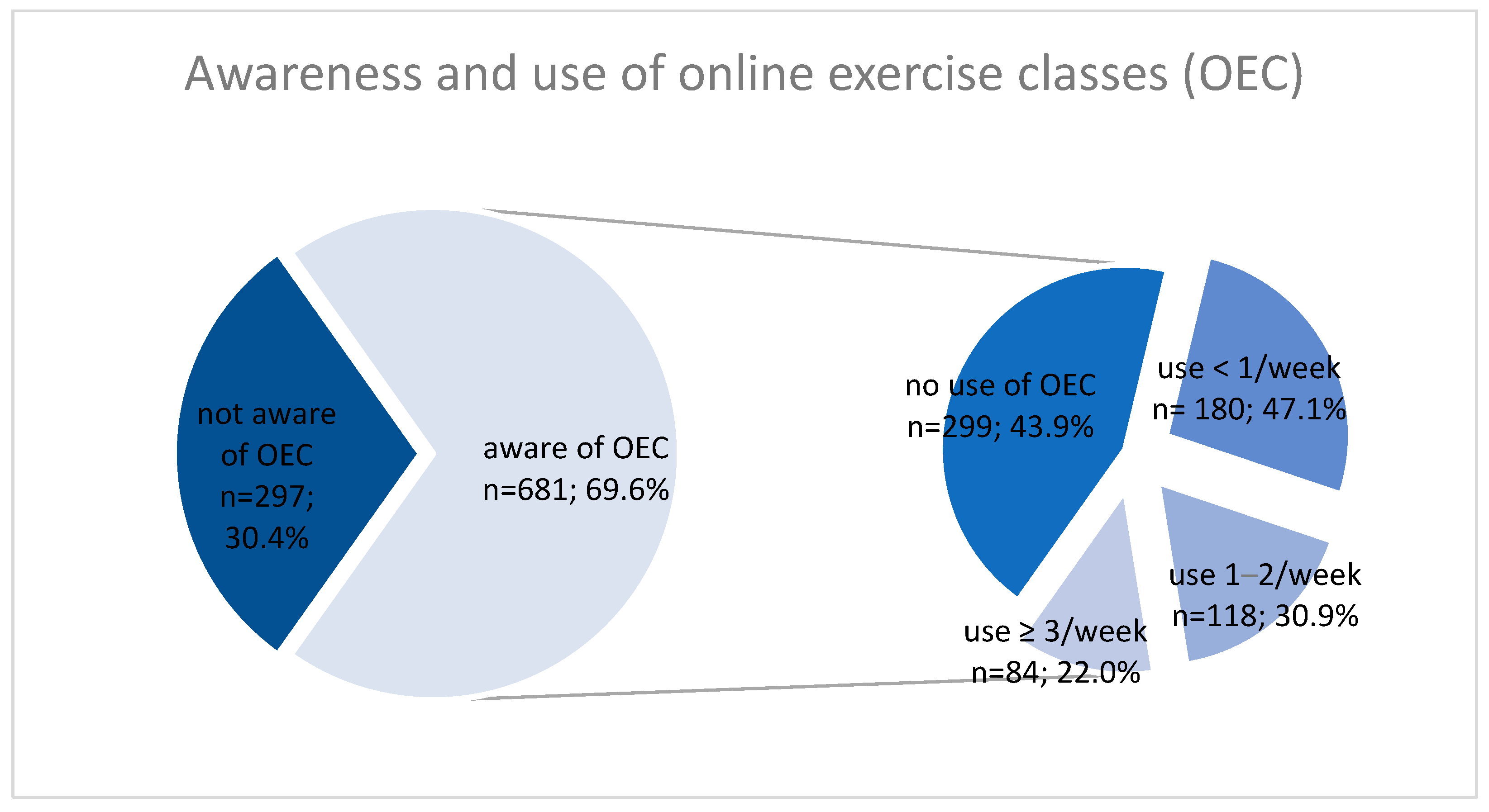
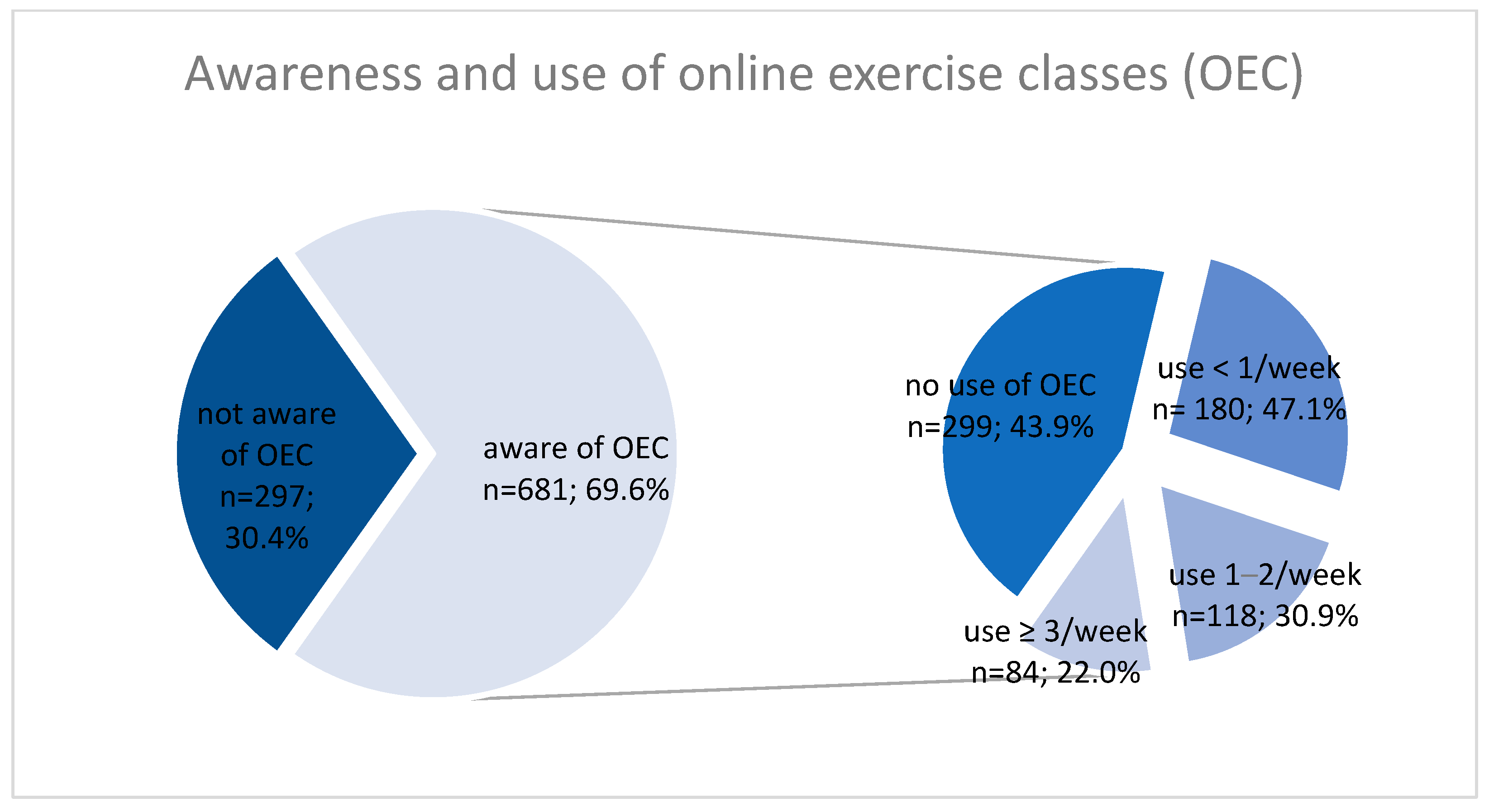
The main aim of our study was to assess to what extent German adults were aware of and used OEC, which have been promoted during the COVID-19 related lockdown in the spring of 2020. As hypothesized, in our sample almost 70% of all respondents reported being aware of such classes. At the same time, only about one in five of all respondents reported regular (at least once a week) use of OEC. Both awareness and use of OEC were higher in respondents who were complying with WHO PA recommendations during lockdown, who were younger and who had lower BMI. Additionally, frequency of use was significantly higher in active respondents. These characteristics might be indicative of an altogether higher health and PA consciousness.
There might be several reasons for limited regular use of OEC. With a higher number of sunny hours, higher temperatures and lower precipitation than usual the weather was very pleasant in Germany during the first lockdown [
31]. Compared to other European countries, such as Italy and Spain, lockdown measures in Germany were less strict, and leaving one’s house was never limited [
32]. These two factors combined might have made using OEC in one’s home less appealing. A further aspect might be the missing of social interaction, as was also documented in our results. In line with our findings, a recent qualitative study from France found that older adults were not interested in training videos that were offered to them during the lockdown, and perceived being alone as demotivating for PA [
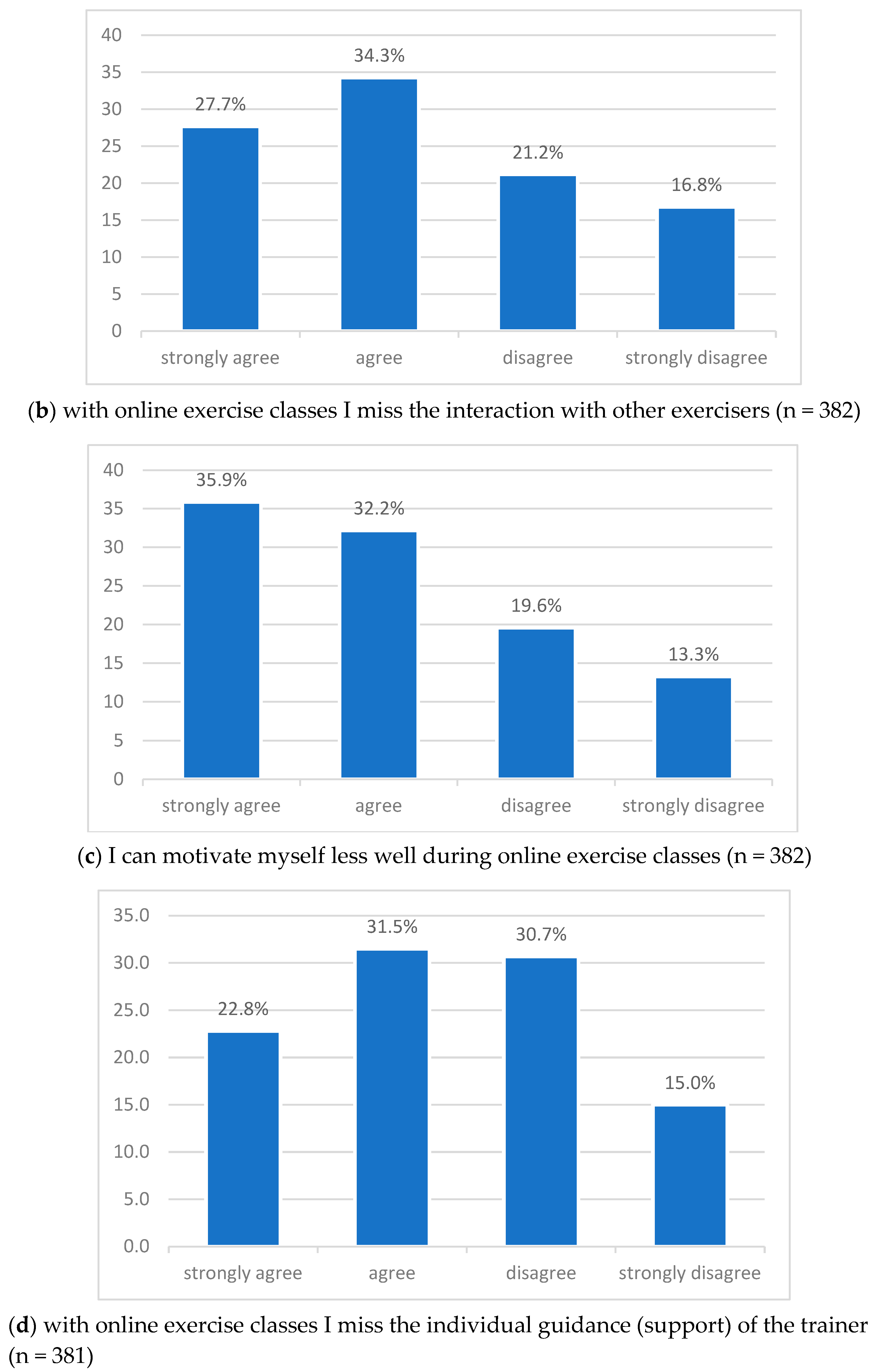
33]. Almost 70% of OEC users in our survey strongly agreed or agreed that they had to motivate themselves harder when engaging in OEC than in regular ones. This result is confirmed by qualitative studies in which participants report a challenge in finding the motivation to regularly exercise in lockdown, even if internet-based alternatives are available [
34,
35]. Barrett and colleagues also reported that some participants indeed tried OEC but were not able to keep with it because of motivational factors [
35]. Over 60% of OEC users in our sample reported missing the interaction with other exercisers. Being part of a group, peer encouragement and PA as an opportunity to socialize are established facilitators for PA [
36,
37]. Indeed, in the elderly engagement in PA is often motivated by the wish to increase social connections [
38], and social motives might be more relevant for older than younger adults [
39]. Safety aspects, such as fear of injury or fall, might have also prevented some from exercising using an OEC without an instructor’s individual guidance. Finally, in Germany fast internet is not available everywhere, and certain population groups’ digital skills are partially limited [
40].
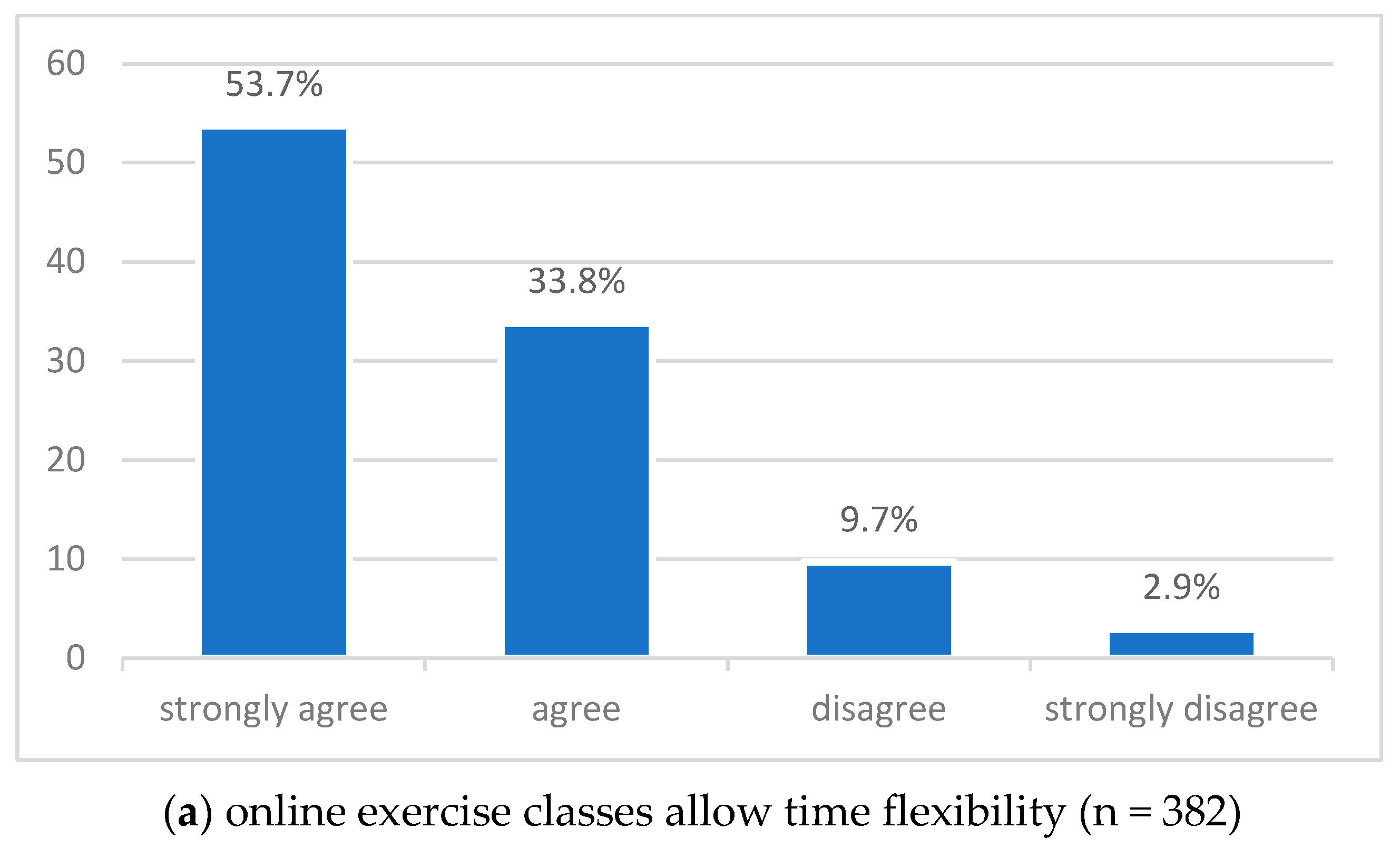
The large majority of OEC users (87.5%) appreciated the time flexibility offered by this format. This finding is not surprising since time constraints and management including competing duties, such as child care, are often cited barriers to regular PA [
36,
41]. This could have even been further exacerbated during lockdown with increased care work [
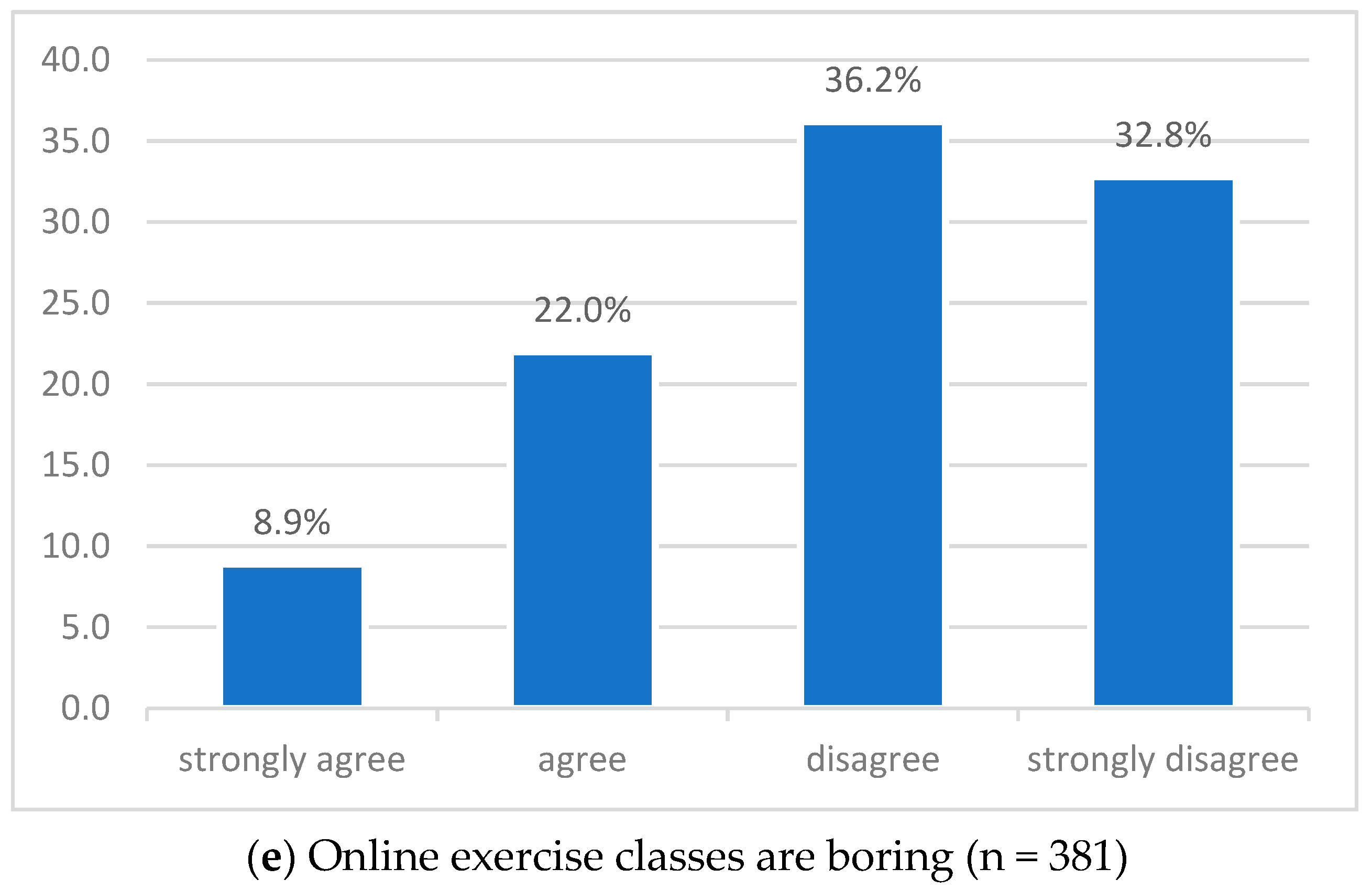
42]. About 70% of OEC users did not perceive OEC as boring, which is an additional asset. Experience of boredom has been identified as a barrier to PA [
43] and might detrimentally affect performance as well as contributing to a feeling of exercise being more taxing [
44].
Slightly more than half of OEC users reported missing the individual guidance of an exercise instructor. It is plausible that some of the OEC users in the current study were experienced exercisers who did not feel the need of supervision. Older people, however, typically appreciate the presence of a qualified instructor; indeed, a systematic review found that the elderly often perceive exercise without an instructor as not being safe [
37].
The correlation analysis indicates that OEC might be differentially attractive to people according to PA status, frequency of use, BMI and age, implying that the very same aspects of OEC might be perceived differentially. Frequent users seemed to appreciate the beneficial aspect of OEC (flexible time management) and did not perceive apparent negative factors such as lack of social interaction and instructor’s support, lower level of motivation or boredom as barriers. Similarly, for younger respondents lack of instructor’s support and boringness were less of a barrier. On the other hand, people with a higher BMI perceived OEC as requiring more self-motivation and being boring.
We are not aware of previous reports on the use of and attitudes towards OEC during the first COVID-19 related lockdown, and comparison with other forms of technology-supported approaches are limited. Digital health interventions and internet-delivered interventions have been shown to lead to a small but significant increase in PA [
45,
46]. These studies and interventions typically provide participants with various forms of support, but even so Davies and colleagues caution about the generalizability of the results if widely disseminated [
45]. This caution seems to be well founded, since large differences in dropout and website usage have been reported in a randomized controlled trial and a randomized ecological trial with the same content (walking promotion) [
47]. All in all, because of very high attrition and low usage, real-world impact of web-based interventions seems to be less well established [
47]. In this sense, our survey is closer to an ecological approach, and results should be seen in this context.
Schwartz and colleagues have designed and tested a live, online, group training intervention among elderly adults during the first COVID-19 related lockdown in Israel. This tailored approach with technical support was feasible, and participants enjoyed live interactions with the instructors and personal feedback during the sessions [
48]. Another study in Israel also found that a custom-made intervention with technical and motivational support was perceived as enjoyable in the elderly sample, so much so that about half of the participants wished to continue with the OEC even after the lockdown [
49]. These studies highlight the necessity of designing interventions for specific target groups and underline the relevance of providing support. This approach however cannot realistically be used at the population level, since with the self-organized use of OEC neither technical nor motivational support is available [
35].
Our study has important practical implications. With ever emerging new variants of the coronavirus [
50], recurring lockdowns and closure of PA infrastructure cannot be fully ruled out. As such, it is important to improve PA options with low infection risk, such as OEC, and learn more about their use. Taken together, OEC have certain advantages, such as low cost, time efficiency and flexibility, and might be regularly used by a small group of people. Lack of motivational support, interaction, instructor supervision and safety concerns however might make them less attractive as a regular exercise option for others [
35,
47]. Tailoring OEC to specific groups, such as the overweight, which currently tend not to use these, and providing feedback and support might improve uptake. Future research should confirm our results in a representative sample using validated instruments. Furthermore, qualitative approaches might shed light on further barriers to OEC use and ways to overcome those.
Our study has some strengths and limitations. To the best of our knowledge, this is the first report on the use of and attitudes towards OEC during the COVID-19 related lockdown, and as such provides the first data on this topic. The relatively large sample size has allowed a detailed analysis to describe users’ and non-users’ profiles. A further strength of our study is the use of the validated EHIS questionnaire to assess PA and anthropometric data. Our survey is limited by self-reporting, the comparatively low number of male respondents and respondents with lower educational attainment. Self-selection bias cannot be ruled out. Additionally, the instrument used to assess attitudes towards OEC has not been validated.








{kind=link}
{kind=link}
{kind=link}
{kind=link}