
Influence of Interpersonal Processes on the Performance of Primary Health Care Organizations

 ,
,
Abstract
:1. Introduction
1.1. Literature Review
1.2. Relationship between Research Dimensions
2. Materials and Methods
2.1. Data Collection and Sample
2.2. Data Analysis
3. Results
- Absence of depressive symptoms and emotional problems;
- Absence of sadness, gloom, and depression;
- Absence of worry, tension, and anxiety.
- Holistic approach that includes conversation about other possible issues, aside from the one that led to the visit (previous illnesses, personal problems, etc.);
- Detailed instructions in the event of deterioration of patient’s health;
- Encouraging active patient involvement;
- Active consulting with the patient on the method of and approach to treatment in order to build trust and understanding;
- Providing additional information to the patient regarding health status;
- Sharing information about the findings and giving the patient insight into all test results.
- Receiving appropriate medical care by the chosen physician in the past year;
- Receiving useful health advice by the chosen physician in the past year;
- Receiving full disclosure regarding the disease and its course from the chosen physician in the past year.
- Education and exchange of information on proper nutrition;
- Education and exchange of information on the importance of physical activity;
- Education and exchange of information on building stress resistance;
- Education and exchange of information on the harmfulness of smoking;
- Education and exchange of information on the harmfulness of alcohol.
- Medical doctors with permanent and fixed-term employment;
- Medical associates with university degrees, with permanent and fixed-term employment;
- Health workers with vocational degrees, with permanent and fixed-term employment;
- Administrative staff with permanent and fixed-term employment;
- Technical staff with permanent and fixed-term employment;
- Number of workshops and educational seminars held in health institution.
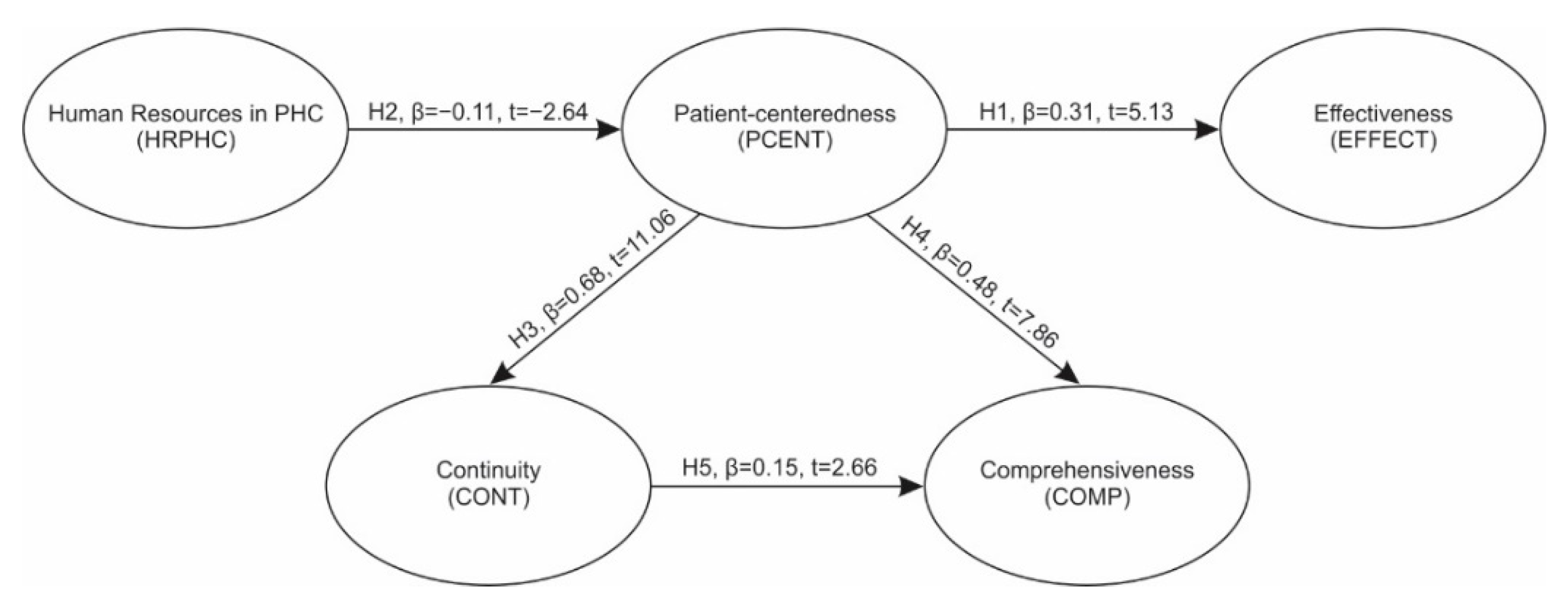
Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donabedian, A. An Introduction to Quality Assurance in Health Care; Bashshur, R., Ed.; Oxford University Press, Inc: New York, NY, USA, 2003. [Google Scholar]
- Starfield, B. Is primary care essential? (Primary Care Tomorrow). Lancet 1994, 334, 1129–1133. [Google Scholar] [CrossRef]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef] [Green Version]
- Donabedian, A. The Quality of Care, How Can It Be Assessed? JAMA J. Am. Med. Assoc. 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Kalinichenko, O.; Amado, A.F.C.; Santos, P.S. Performance Assessment in Primary Health Care: A Systematic Literature Review; CEFAGE-UE Working Paper; University of Algarve—Faculty of Economics and CEFAGE-UE, CEFAGE-UE, Universidade de Évora: Évora, Portugal, 2013. [Google Scholar]
- Institute of Medicine—IOM. Performance Measurement: Accelerating Improvement; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar] [CrossRef] [Green Version]
- Elg, M.; Engström, J.; Witell, L.; Poksinska, B. Co-creation and learning in health-care service development. J. Serv. Manag. 2012, 23, 328–343. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, D.; Rogers, L.; Jo Heier, E. Overview, History, and Objectives of Performance Measurement. Health Care Financ. Rev. 2001, 22, 7–21. [Google Scholar] [PubMed]
- Moullin, M. Eight essentials of performance measurement. Int. J. Health Care Qual. Assur. 2004, 17, 110–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.-c.; Lin, W.S.; Northcott, N.D. The NHS Performance Assessment Framework, A “balanced scorecard” approach? J. Manag. Med. 2002, 16, 345–358. [Google Scholar] [CrossRef]
- Moullin, M. Performance measurement definitions, Linking performance measurement and organisational excellence. Int. J. Health Care Qual. Assur. 2007, 20, 181–183. [Google Scholar] [CrossRef] [Green Version]
- Aday, A.L.; Begley, E.; Lairson, R.D.; Slater, H.C.; Richard, J.A.; Montoya, D.I. A Framework for Assessing the Effectiveness, Efficiency and Equity of Behavioral Healthcare. Am. J. Manag. Care 1999, 5, 25–44. [Google Scholar]
- Kelley, E.; Hurst, J. Health Care Quality Indicators Project: Conceptual Framework. OECD HealthWorking Papers; No. 23; OECD Publishing: Paris, France, 2006. [Google Scholar]
- OECD. Health at a Glance 2013: OECD Indicators; OECD Publishing: Paris, France, 2013. [Google Scholar] [CrossRef] [Green Version]
- WHO—World Health Organization. Improving Quality Primary Health Care, From Measurement to Improvement: A roadmap. In Proceedings of the Primary Health Care Improvement, Global Stakeholder Meeting, Geneva, Switzerland, 6–8 April 2016. [Google Scholar]
- Braithwaite, J.; Hibbert, P.; Blakely, B.; Plumb, J.; Hannaford, N.; Long, J.C.; Marks, D. Health system frameworks and performance indicators in eight countries: A comparative international analysis. SAGE Open Med. 2017, 5, 2050312116686516. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Evans, D.B. Health Systems Performance Assessment: Debates, Methods and Empiricism; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Rodella, S.; Bellini, P.; Braga, M.; Rebba, V. Measuring and Comparing Performance of Health Services: A Conceptual Model. to Support. Selection and Validation of Indicators; Commissione per laGaranzia dell’Informazione Statistica (CGIS): Rome, Italy, 2003. [Google Scholar]
- Schäfer, W.L.A.; Boerma, W.G.W.; Kringos, S.D.; De Ryck, E.; Heinemann, S.; Greß, S.; Murante, A.M.; Rotar-Pavlic, D.; Schellevis, F.; Seghieri, C.; et al. Measures of quality, costs and equity in primary health care: Instruments developed to analyse and compare primary health care in 35 countries. Qual. Prim. Care 2013, 21, 67–79. [Google Scholar] [PubMed]
- Schäfer, W.L.A. Primary Care in 34 Countries: Perspectives of General Practitioners and Their Patients; NIVEL: Utrecht, The Netherlands, 2016. [Google Scholar]
- Kringos, S.D. The Strength of Primary Care in Europe; NIVEL: Utrecht, The Netherlands, 2012. [Google Scholar]
- Kringos, S.D.; Boerma, W.G.W.; Hutchinson, A.; van der Zee, J.; Groenewegen, P.P. The breadth of primary care: A systematic literature review of its core dimensions. BMC Health Serv. Res. 2010, 10, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PHCPI—Primary Health Care Performance Initiative. Methodology Note. Available online: https://improvingphc.org/measuring-primary-health-care-performance (accessed on 7 September 2021).
- PHCPI—Primary Health Care Performance Initiative. Primary Health Care Progression Model Assessment Tool. Available online: https://improvingphc.org/sites/default/files/PHC-Progression%20Model%202019-04-04_FINAL.pdf (accessed on 7 September 2021).
- Burches, E.; Burches, M. Efficacy, Effectiveness and Efficiency in the Health Care: The Need for an Agreement to Clarify its Meaning. Int. Arch. Public Health Community Med. 2020, 4. [Google Scholar] [CrossRef]
- Bourne, M.; Neely, A.; Mills, J.; Platts, K. Implementing performance measurement systems: A literature review. Int. J. Bus. Perform. Manag. 2003, 5, 1–24. [Google Scholar] [CrossRef]
- Fung, H.C.; Eliot, N.M.; Hays, D.R.; Kahn, L.K.; Kanouse, E.D.; McGlynn, A.E.; Spranca, D.M.; Shekelle, G.P. Patients’ Preferences for Technical Versus Interpersonal Quality When Selecting a Primary Care Physician. Health Serv. Res. 2005, 40, 957–977. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine—IOM. Crossing the Quality Chasm, A New Health System for the 21st Century; Committee on Quality of Health Care in America, National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- National Health Service—NHS. NHS Performance Assessment Framework; NHS Department of Health: London, UK, 1999.
- National Health Service—NHS. The NHS Performance Framework: Implementation Guidance; NHS Department of Health, NHS Finance, Performance & Operations Directorate: London, UK, 2012.
- Grol, R.; Wensing, M.; Mainz, J.; Jung, H.P.; Ferreira, P.; Hearnshaw, H.; Hjortdahl, P.; Olesen, F.; Reis, S.; Ribacke, M.; et al. Patients in Europe evaluate general practice care: An international comparison. Br. J. Gen. Pract. 2000, 50, 882–887. [Google Scholar]
- Levinson, W.; Lesser, S.C.; Epstein, M.R. Developing Physician Communication Skills for Patient-Centered Care. Health Aff. 2010, 29, 1310–1318. [Google Scholar] [CrossRef]
- Starfield, B. Is Patient-Centered Care the Same as Person-Focused Care? Perm. J. 2011, 15, 63–69. [Google Scholar] [CrossRef]
- Haggerty, L.J.; Reid, J.R.; Freeman, K.G.; Starfield, H.B.; Adair, E.C.; McKendry, R. Continuity of care: A multidisciplinary review. BMJ 2003, 327, 1219–1221. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, D.; Hirschhorn, L.R.; Kim, J.H.; Ratcliffe, H.L.; Bitton, A. Continuity in primary care: A critical but neglected component for achieving high-quality universal health coverage. BMJ Glob. Health 2019, 4, e001435. [Google Scholar] [CrossRef] [Green Version]
- Alyafei, A.; Al Marri, S.S. Continuity of Care at the Primary Health Care Level: Narrative Review. Fam. Med. Prim. Care Rev. 2020, 4, 146. [Google Scholar] [CrossRef]
- Boerma, W.G.W.; Van der Zee, J.; Fleming, M.D. Service profiles of general practitioners in Europe. Br. J. Gen. Pract. 1997, 47, 481–486. [Google Scholar]
- Campbell, M.S.; Roland, O.M.; Buetow, A.S. Defining quality of care. Soc. Sci. Med. 2000, 51, 1611–1625. [Google Scholar] [CrossRef]
- Hair, F.J., Jr.; Hult, M.T.; Ringle, M.C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; SAGE Publications, Inc.: New York, NY, USA, 2017. [Google Scholar]
- Hu, L.-T.; Bentler, M.P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hair, F.J., Jr.; Sarstedt, M.; Matthews, M.L.; Ringle, M.C. Identifying and treating unobserved heterogeneity with FIMIX-PLS: Part I—Method. Eur. Bus. Rev. 2016, 28, 63–76. [Google Scholar] [CrossRef]
- Matthews, M.L.; Sarstedt, M.; Hair, F.J., Jr.; Ringle, M.C. Identifying and treating unobserved heterogeneity with FIMIX-PLS: Part II—A case study. Eur. Bus. Rev. 2016, 28, 208–224. [Google Scholar] [CrossRef]
- Fajgelj, S. Psihometrija—Metod i Teorija Psihološkog Merenja; Centar za Primenjenu Psihologiju: Beograd, Srbija, 2003. [Google Scholar]
- Berenson, A.R.; Pronovost, J.P.; Krumholz, M.H. Achieving the Potential of Health Care Performance Measures; Timely Analysis of Immediate Health Policy Issues; Robert Wood Johnson Foundation: Washington, DC, USA; Urban Institute: Washington, DC, USA, 2013. [Google Scholar]
- Scopetti, M.; Padovano, M.; Manetti, F.; Gatto, V.; D’Errico, S.; Santurro, A.; Frati, P.; Fineschi, V. Key Performance Indicators in Claims Management: Definition of a set of indicators for the evaluation of the Medico-Legal Activity. Curr. Pharm. Biotechnol. 2021, 22, 1971–1984. [Google Scholar] [CrossRef]
- Scopetti, M.; Santurro, A.; Gatto, V.; Padovano, M.; Manetti, F.; D’Errico, S.; Fineschi, V. Information, Sharing, and Self-Determination: Understanding the Current Challenges for the Improvement of Pediatric Care Pathways. Front. Pediatrics 2020, 8. [Google Scholar] [CrossRef]
- Davis, R.E.; Sevdalis, N.; Jacklin, R.; Vincent, C.A. An examination of Opportunities for the Active Patient in Improving Patient Safety. J. Patient Saf. 2012, 8, 36–43. [Google Scholar] [CrossRef]
- Davis, R.E.; Sevdalis, N.; Vincent, C.A. Patient Involvement in Patient Safety: The Health-Care Professional’s Perspective. J. Patient Saf. 2012, 8, 182–188. [Google Scholar] [CrossRef]
- Rhondali, W.; Perez-Cruz, P.; Hui, D.; Chisholm, G.B.; Dalal, S.; Baile, W.; Chittenden, E.; Bruera, E. Patient-Physician Communication about Code Status Preferences: A Randomized Controlled Trial. Cancer 2013, 119, 2067–2073. [Google Scholar] [CrossRef] [PubMed]
- Longtin, Y.; Sax, H.; Leape, L.L.; Sheridan, S.E.; Donaldson, L.; Pittet, D. Patient Participation: Current Knowledge and Applicability to Patient Safety. Mayo Clin. Proc. 2010, 85, 53–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Institute for Health Information. Primary Health Care (PHC) Indicators Chartbook: An. Illustrative Example of Using PHC Data for Indicator Reporting; Canadian Institute for Health Information: 495 Richmond Road, Ottawa, ON, Canada, 2008. [Google Scholar]
- Coulter, A.; Ellins, J. Effectiveness of strategies for informing, educating and involving patients: An overview of systematic reviews. BMJ 2007, 335, 24–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Health Status | Number | % |
|---|---|---|
| Poor | 41 | 6.6 |
| Fair | 171 | 27.5 |
| Good | 191 | 30.8 |
| Very good | 120 | 19.3 |
| Excellent | 84 | 13.5 |
| I don’t know or I’m not sure | 11 | 1.8 |
| I prefer not to answer | 3 | 0.5 |
| Total | 621 | 100.0 |
| CR | AVE | MSV | MaxR(H) | HRPHC | CONT | COMP | PCENT | EFFECT | |
|---|---|---|---|---|---|---|---|---|---|
| HRPHC | 0.977 | 0.876 | 0.017 | 0.991 | 0.936 | ||||
| CONT | 0.860 | 0.674 | 0.482 | 0.879 | −0.129 | 0.821 | |||
| COMP | 0.910 | 0.671 | 0.341 | 0.931 | −0.076 | 0.494 | 0.819 | ||
| PCENT | 0.864 | 0.516 | 0.482 | 0.874 | −0.105 | 0.694 | 0.584 | 0.718 | |
| EFFECT | 0.843 | 0.583 | 0.028 | 0.885 | −0.070 | 0.167 | −0.059 | 0.161 | 0.763 |
| Hypothesis | Path | β | SE | t | p | Supported? |
|---|---|---|---|---|---|---|
| H1 | PCENT → EFFECT | 0.31 | 0.071 | 5.132 | 0.000 | YES |
| H2 | HRPHC → PCENT | −0.113 | 0.028 | −2.644 | 0.008 | YES |
| H3 | PCENT → CONT | 0.685 | 0.068 | 11.055 | 0.000 | YES |
| H4 | PCENT → COMP | 0.484 | 0.084 | 7.861 | 0.000 | YES |
| H5 | CONT → COMP | 0.148 | 0.07 | 2.664 | 0.008 | YES |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čučković, D.; Ćosić, I.; Delić, M.; Miškić, M.; Ranisavljev Kovačev, S. Influence of Interpersonal Processes on the Performance of Primary Health Care Organizations. Sustainability 2021, 13, 12243. https://doi.org/10.3390/su132112243
Čučković D, Ćosić I, Delić M, Miškić M, Ranisavljev Kovačev S. Influence of Interpersonal Processes on the Performance of Primary Health Care Organizations. Sustainability. 2021; 13(21):12243. https://doi.org/10.3390/su132112243
Chicago/Turabian StyleČučković, Duško, Ilija Ćosić, Milan Delić, Miroslav Miškić, and Slavica Ranisavljev Kovačev. 2021. "Influence of Interpersonal Processes on the Performance of Primary Health Care Organizations" Sustainability 13, no. 21: 12243. https://doi.org/10.3390/su132112243
APA StyleČučković, D., Ćosić, I., Delić, M., Miškić, M., & Ranisavljev Kovačev, S. (2021). Influence of Interpersonal Processes on the Performance of Primary Health Care Organizations. Sustainability, 13(21), 12243. https://doi.org/10.3390/su132112243