
The Three-Talk Model: Getting Both Evidence and Preferences into a Pre-Service Teacher Health Workshop


Abstract
:1. Introduction
2. Health and Illness in School—A Workshop for Pre-Service Teachers at the University of Teacher Education of Lucerne, Switzerland
3. Science Literacy and the Need for Additional Conceptual Background in the Workshop
3.1. The PISA 2006 Framework of Science Literacy
3.2. Evidence and Preference (E&P) in Medicine
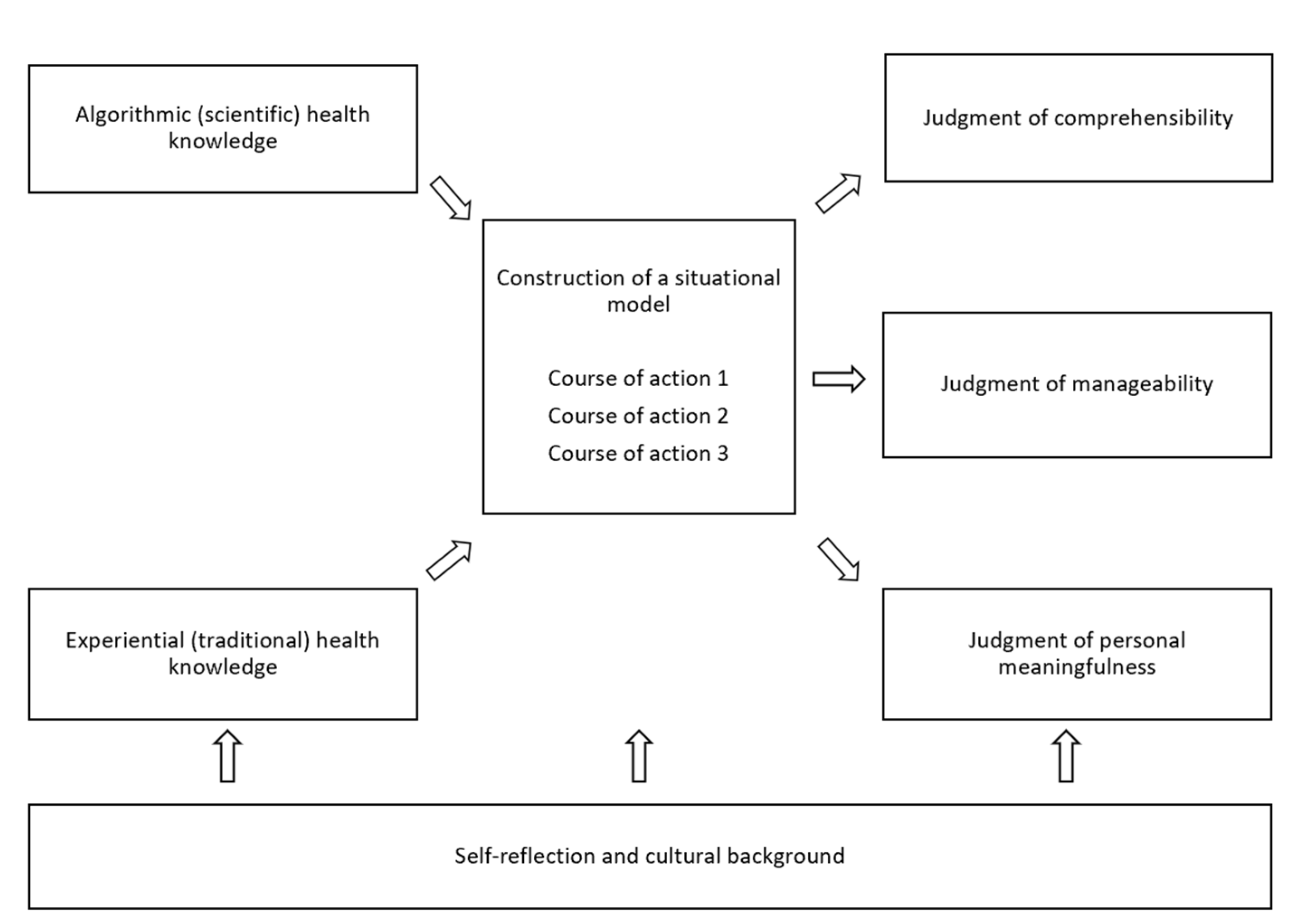
- The model emphasizes evidence instead of knowledge. Roughly speaking, knowledge is about truth, while evidence is about facts, i.e., the effectiveness of an intervention in achieving an outcome (e.g., [12]). This is a tribute to the complexity of health and medicine contexts. In complex contexts, because prediction is often flawed, scientific knowledge may suggest measures that do not work under real-world conditions, while, conversely, things may turn out to work that are not backed up by knowledge, or that are only backed up with the benefit of hindsight. For health and medicine clients, however, “what works” is much more important than “what is true”.
- The model puts preferences on a level playing field with evidence. Preferences are the totality of what we roughly called values, like the clients’ environment, needs, emotions, and fears, as well as the subjective knowledge of their health and disease they bring to the discussion. There is no such thing as “overruling preferences by evidence” [11].
- The model shares responsibilities. The doctor is responsible for knowing the best evidence and communicating it appropriately to the client. Notice that it is not only the doctor’s personal evidence that counts, but also the totality of the professionally negotiated evidence, condensed in professional guidelines that the doctor draws from. Usually, these guidelines result from the summary of a systematic and strict review of existing studies done by specialists [12]. The patient is responsible for featuring their value perspective and communicating it to the doctor. Of course, as always in good medical practice, the patient always has the final say.
3.3. The Three-Talk Model in Medicine
4. How the E&P Approach and the Three-Talk Model Connect to the Workshop
4.1. Educational Methods Used in the Workshop
- Autonomous learning sequences. In these sequences, the students read scientific documents in order to improve their scientific knowledge about the issues at stake. For example, they read a short text about diabetes mellitus or epilepsy, or study short passages about the male and the female anatomy to set the scene for further instruction on contraception and STDs.
- Lectures about health and medical issues in school. These lectures were evidence-based. For example, information was presented on what is known about the incidence of poisoning accidents in children and youths, about the substances that were involved, and about evidence-based first-aid measures that should be taken in case of an incident. A further example was the presentation of evidence about the current STD situation in Switzerland and about the effectiveness of various contraception methods for preventing different STDs. Medical doctors and other health experts gave these lectures.
- Workshops. In 90-min workshops, the health and medical issues were contextualized for school life. School experts in sex education, for example, presented educational methods and discussed practical challenges with the students. A school nurse talked about her experiences with chronic illness in school, like cystic fibrosis, coeliac disease, diabetes, and asthma, and reflected with the students on tasks and challenges for teachers when confronted with chronically ill children in their classes, and the handling of parents, colleagues, and other students.
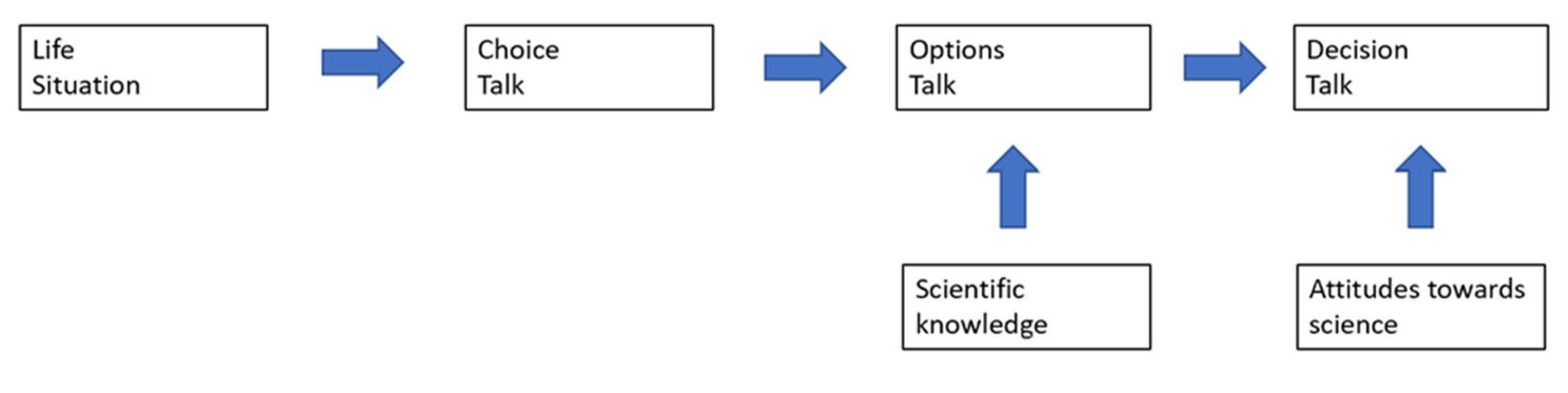
4.2. How Can the Three-Talk Model Be Used to Structure the Workshop?
4.2.1. Step 1: Choice Talk
4.2.2. Step 2: Options Talk
4.2.3. Step 3: Decision Talk
4.3. A Comparison of Scientific Literacy and the Evidence and Preference Approach
4.4. The Role of Knowledge and Fake Knowledge
5. The E&P Approach and the Three-Talk Model in School
5.1. An Example of a Full-Blown Expansion of the Three-Talk Model
5.2. Variants and Shortcuts
6. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zeyer, A.; Dillon, J. Science|Environment|Health—The Emergence of a New Pedagogy of Complex Living Systems. Discip. Interdiscip. Sci. Educ. Res. 2019, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Zeyer, A.; Dillon, J. Science|Environment|Health—Towards a reconceptualization of three critical and inter-linked areas of education. Int. J. Sci. Educ. 2014, 36, 1409–1411. [Google Scholar] [CrossRef]
- Schroeder, M. Value theory. In The Stanford Encyclopedia of Philosophy; Zalta, E.N., Ed.; 2021; Available online: https://plato.stanford.edu/archives/fall2021/entries/value-theory/ (accessed on 30 October 2021).
- Arnold, J.C. An integrated model of decision-making in health contexts: The role of science education in health education. Int. J. Sci. Educ. 2018, 40, 519–537. [Google Scholar] [CrossRef]
- Barratt, A. Evidence Based Medicine and Shared Decision Making: The challenge of getting both evidence and preferences into health care. Patient Educ. Couns. 2008, 73, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Zeyer, A. A Win-Win Situation for Health and Science Education: Seeing through the Lens of a New Framework Model of Health Literacy. In Science|Environment|Health. Towards a Renewed Pedagogy for Science Education; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Dordrecht, Germany, 2012; pp. 147–173. [Google Scholar]
- Elwyn, G.; Durand, M.; Song, J.; Aarts, J.; Barr, P.J.; Berger, Z.; Cochran, N.; Frosch, D.; Galasiski, D.; Gulbrandsen, P.; et al. A Three-Talk Model for Shared Decision Making: Multistage Consultation Process. BMJ 2017, 359, i4891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elwyn, G.; Laitner, S.; Coulter, A.; Walker, E.; Watson, P.; Thomson, R. Implementing Shared Decision Making in the NHS. BMJ 2010, 341, c5146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, M.; Kraft, E. Shared Decision Making—Arzt Und Patient Entscheiden Gemeinsam. Schweiz. Arzteztg. 2014, 95, 1883–1889. [Google Scholar]
- Zeyer, A. Coping with structural uncertainty in complex living systems. In Science|Environment|Health—Towards a Science Pedagogy of Complex Living Systems; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2021; in print. [Google Scholar]
- Toon, P. Theories of Knowledge What is evidence? Lond. J. Prim. Care 2014, 6, 95–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bybee, R. Scientific literacy in environmental and health education. In Science|Environment|Health. Towards a Renewed Pedagogy for Science Education; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Dordrecht, Germany, 2012; pp. 49–67. [Google Scholar]
- Sharon, A.J.; Baram-Tsabari, A. Can science literacy help individuals identify misinformation in everyday life? Sci. Educ. 2020, 104, 873–894. [Google Scholar] [CrossRef]
- Fooladi, E.C. Between Education and Opinion-Making: Dialogue between Didactic/Didaktik Models from Science Education and Science Communication in the Times of a Pandemic. Sci. Educ. 2020, 29, 1117–1138. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.; Bauer, D. The Role of Science Education in Decision Making Concerning Health and Environmental Issues. In Science|Environment|Health–Towards a New Science Pedagogy of Complex Living Systems; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Dordrecht, Germany, 2021; in print. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Step 1: Choice Talk | Offer choice. Be aware that patients often misconstrue the presentation of choice and think that the clinician is either incompetent or uninformed, or both. Justify choice. Emphasize: (1) the importance of respecting individual preferences, and (2) the role of uncertainty. Personalizing preferences. Explaining that different issues matter more to some people than to others. Uncertainty. Patients are often unaware of the extent of uncertainty in medicine: that evidence may be lacking and that individual outcomes are unpredictable at the individual level. Defer closure. Some patients react by asking clinicians to “tell me what to do…” We suggest deferring closure if this occurs, reassuring that you are willing to support the process. |
| Step 2: Option talk | List options. Make a clear list of the options, as it provides a good structure. Describe options. Generate dialogue and explore preferences. Describe the options in practical terms. Harms and benefits. Being clear about the pros and cons of different options lies at the heart of shared decision-making. |
| Step 3: Decision talk | Focus on preferences. Guide the patient to form preferences. Suggested phrases: “From your point of view, what matters most?” Elicit a preference. Be ready with a back-up plan by offering more time or being willing to guide the patient, if they indicate that this is their wish. Moving to a decision. Try checking for the need to either defer a decision or make a decision. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeyer, A.; Arnold, J. The Three-Talk Model: Getting Both Evidence and Preferences into a Pre-Service Teacher Health Workshop. Sustainability 2021, 13, 13937. https://doi.org/10.3390/su132413937
Zeyer A, Arnold J. The Three-Talk Model: Getting Both Evidence and Preferences into a Pre-Service Teacher Health Workshop. Sustainability. 2021; 13(24):13937. https://doi.org/10.3390/su132413937
Chicago/Turabian StyleZeyer, Albert, and Julia Arnold. 2021. "The Three-Talk Model: Getting Both Evidence and Preferences into a Pre-Service Teacher Health Workshop" Sustainability 13, no. 24: 13937. https://doi.org/10.3390/su132413937