Abstract
The first cases of COVID-19 materialised in Malaysia in January 2020, and the trend of COVID-19 cases boosted remarkably. As the globe changes its usual services and norms with digitalisation, many countries have used information technology embedded within digitalisation to manage COVID-19. This applies specifically for containment and contact tracing among Malaysian citizens. Malaysia is one of the first countries in Southeast Asia to have designed digital applications to control and manage the COVID-19 pandemic, hence making it one of the top 50 nations under the UN’s 2020 E-Government Development Index (EGDI). This study intended to investigate the effectiveness of digitalisation in controlling the spread of COVID-19 outbreaks in Malaysia from 11 March to 9 June 2020 (90 days), with a specific focus on the aspects of containment and contact tracing. This research concluded that using digital applications and government administrative orders advised by national healthcare policy, through movement control orders (MCO) and conditional movement control orders (CMCO), slowed down the rate of COVID-19 cases in Malaysia. Similar endeavours by Malaysia’s neighbouring countries have also administered current technological advancements to battle the pandemic with healthcare efforts.
1. Introduction
The global data regarding COVID-19 infection have shown that the infection rate has not reached its exponent. Thus, eight billion lives are at risk. According to the World Health Organization’s (WHO) situation report 143, as of 11 June 2020, there have been 7,273,958 infected individuals, of whom 413,372 have died, across 212 countries and territories globally [1]. COVID-19 emerged in December 2019 in Wuhan, the capital city of Hubei in the People’s Republic of China, where patients experienced pneumonia cases with unknown causes and exhibited symptoms including fever, fatigue, coughing, and breathing difficulties [2]. It was not long before clinicians and scientists realised it was a novel virus capable of airborne transmission. On 31 January 2020, WHO announced COVID-19 as a public health emergency of international concern [3]. Nevertheless, the first case of COVID-19 was reported in Malaysia in January 2020, approximately one month after the outbreak of COVID-19 in Wuhan, China, when a Chinese traveller arriving from Singapore in Malaysia was diagnosed with COVID-19. Initially, the number of COVID-19 cases in Malaysia was relatively low, and most of the cases reported were imported (i.e., those travelling overseas). Nonetheless, the situation changed when a local cluster was detected from a religious congregation. The first infected patient was suspected of travelling from South Korea before joining the mass gathering in Sri Petaling, Kuala Lumpur. The pandemic became intense as the cases escalated quickly, and Malaysia then registered the most prominent accumulation of COVID-19 cases in Southeast Asia, reaching over 2000 cases at the end of March 2020.
As the COVID-19 infection rate started to rise, on 16 March, under the Infectious Disease Control Act 324, which was endorsed in 1988, Malaysia banned all visitors and prohibited residents from travelling overseas. Along with the closure of the country’s borders, Malaysia also shut down non-essential businesses, schools, and religious services. The move made by the Malaysian government could be considered a quarantine or lockdown by the global community. In contrast, in the local setting, it was known as a “Movement Control Order (MCO)” or cordon sanitaire. MCO is a preventive measure imposed by the government of Malaysia whereby citizens are urged to stay indoors and are only allowed to leave for essential outdoor activities such as buying groceries, obtaining healthcare and conducting postal services. Initially, the MCO was intended to end within 14 days, starting from 18 March 2020, but it was later partially extended and was still in effect until 31 August 2020. While restricting the movement of its citizens, information technology usage was also attended by the Malaysian government in combating COVID-19. This included using mobile apps to fight against COVID-19 in the healthcare sector. In a speech by the Prime Minister on 1 May 2020, he encouraged the public to help the government in preventive and contact-tracing measures by installing an app. In an attempt to battle COVID-19, contact tracing is paramount. The health frontliners must be informed of whom the infected person has been in contact with. To facilitate this, the government has made the MySejahtera and MyTrace apps available. “I hope those who own smartphones will support the effort in supporting the Ministry of Health to manage contact tracing if there are new infections. This is our shared responsibility” [4].
It has been acknowledged that the preparedness of digitalisation should focus on its implementation and on elements of infrastructure that are both tangible and intangible, reflecting how digital content and applications are virtual. Malaysia notably has concentrated on digitalisation by reducing the gap in its broadband to permit internet penetration throughout the nation. This plan has, since 2008, been officially known as The National Broadband Plan (NBP). This plan was perceived to cater to the mushrooming number of internet subscribers. It suggests a subscription base that has expanded from 900,000 in 2000 with the expansion of internet centres for learning and familiarisation purposes, and the extension of information and communication technology (ICT) catalysing digitalisation [5,6,7].
Malaysia is one of the first countries in Southeast Asia to have devised digital applications to control and manage the COVID-19 pandemic. It is also one of the top 50 countries under the UN’s 2020 E-Government Development Index (EGDI). In this narrative review with a scoping method, using the emerging evidence of pandemic occurrence, reported in detail, the researchers aimed to discuss the national efforts of the Malaysian government in containing and tracing COVID-19 and its use of digitalisation through available information technology to effectively control and monitor cases of COVID-19 during their establishment in the early stages of managing the pandemic. The number of global cases of COVID-19 has grown from 2020 until 2022. This is due to fresh variants such as Delta and Omicron [8,9]. This review, however, did not consider different variants of the virus. The researchers only underscored efforts by the Malaysian government to control the spread of COVID-19 outbreaks from 11 March to 9 June 2020 (90 days) with a specific emphasis on the aspects of containment and contact tracing. This review reported the use of digital applications and government administrative orders in slowing down the infection rate of COVID-19 in Malaysia. Readiness was measured by focusing on the implementation and adoption efforts of the Malaysian government in managing the containment and contact tracing of COVID-19 patients with the use of digitalisation during the early phase of the pandemic’s spread.
2. Digitalisation in Healthcare Services
In unified terms, digitalisation signifies a process for analysing and interpreting data sequences to aid precise decision making in resolving issues that obstruct an efficient and successful work process. It involves digitisation sequences concerning migration from analogue to digital bits of 1 s and 0 s with discrete and discontinuous values. Practitioners and academicians have been astonished by the potential of artificial intelligence since its revelation in 1956 at Dartmouth conferences [10,11]. Digital technology in healthcare transforms traditional services into an extension of upgraded management, including the adoption of both system applications and physical devices. Since the advances with usage of the “worldwide web”, known as the internet, the global network has positioned computers at the core of a modern communications medium as instrumental in inventing network technology. The internet evolved from a single experimental network serving a dozen sites in the United States to a global infrastructure connecting millions of computers between the late 1960s and the 1990s, which helped redefine the practice and sense of computing by making long-distance interaction among various types of computers possible [12].
Computerised machines and devices are becoming accessible, remotely available, and wirelessly operative through applications, and can be handled by anyone in a community as the internet enhances its capacities alongside digitalisation. These advancements have impacted various aspects and made digital spatiality among industries differ from the perspective of digital space, in which how it “looks” and “behaves” varies depending on aspects of the point of entry, such as location, country and device [13]. Digitalisation empowers the networks to link to smartphones, as well as various telemedicine and online systems in healthcare. The improvement in digitalisation has enabled existing systems, such as telemedicine, to be used in healthcare. Telemedicine has boosted healthcare services at distant locations with virtual interactions. Therefore, it proves the value of telecommunications technology for medical diagnostics, monitoring and therapeutic purposes when distance and/or time separates the participants [14]. The Sixth Malaysia Plan initiated the incorporation of infrastructures, policies and execution related to ICT in 1991, and it was regarded as a new era of the Information Age. The Ministry of Health Malaysia (MOH) works as an enabler in promoting the role of systems and applications in Malaysia’s healthcare services. As Malaysia is being progressive in adopting “Technology in Healthcare”, this has marked the creation of IT-enabled facilities. The application of information technology in healthcare services began in 1997 under Malaysia’s Telemedicine Blueprint 1997 [15]. One of the ICT applications was establishing a Teleprimary Care (TPC) system that integrates and manages patients’ information throughout Malaysia. With the collaboration with stakeholders from both public and private sectors, several standards have been developed by MOH. Among them are included the “Functional Requirements Brief Hospital Information System”, which aspires to furnish functional requirements for the hospital to adopt contemporary technological advancements in their healthcare services [16]. In addition, the telemedicine blueprint “Leading Healthcare into Information Age” has laid the foundation for Malaysia’s planning and implementation of information technology initiatives, which can be established as a platform for future IR4.0 systems. These advancements in healthcare are crucial in converging technology for digitalisation, as they play a substantial role in battling the COVID-19 outbreak.
The use of mobile apps in Malaysia to manage COVID-19 has substantiated Malaysia’s initiatives for digitalisation by digitisation and digital transformation. This took place by coupling functions with the healthcare sector in pandemic management, such as the interoperability of systems automation, communication and internet technologies, using the current advancements in technologies emerging from advances in Information Science and Technology (IST), which served as an interdisciplinary science during the early years of computers’ introduction, leading to the digital shift in the 1960s [17].
3. Methods
In the review process, the researchers adopted a qualitative narrative review. The researchers searched relevant journal articles, official reports and policies from reliable databases (such as Science Direct and authorities’ websites) based on the keywords COVID-19, digitalisation, containment and/or contact tracing. The languages used in these references were English and Malay (Malaysia’s national language). The researchers admit that there are various methods for article review, such as SLR (Systematic Literature Review), PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and SANRA (Scale for the Assessment of Narrative Review Articles). However, since this article aimed to review the adoption of digitalisation in healthcare services in Malaysia, particularly the development of digital applications in battling COVID-19, most of the information was obtained from public-domain documents. Next, the researchers reviewed other academic publications related to digitalisation, including digitalisation in healthcare services and COVID management, as shown in Table 1.

Table 1.
Publications related to digitalisation.
The review process included the analysis of COVID-19 during 90 days of infection rate (from 11 March to 9 June 2020) because Malaysia recorded the most pertinent cumulative COVID-19 cases in Southeast Asia at the end of March 2020. During this period, the Malaysian government imposed administrative orders and established a digital application with the purpose of containment and contact tracing. The COVID-19 cases in Malaysia were gathered from cases reported during daily press statements by the Director-General of Health, Ministry of Health Malaysia, and Senior Minister for Security and Minister of Defence Malaysia. The data gathered were paramount in analysing the efficacy of the steps taken by the government, such as digitalisation adoption, for containment and contact-tracing purposes in the general public, among other methods used for public health in handling epidemic occurrences. Additionally, secondary data were also gathered from data published by relevant ministries and agencies in Malaysia and other academic journals related to digitalisation usages and implementations, focusing on COVID-19 with related healthcare services. These efforts aimed to contribute educational materials of future references enriching digitalisation endeavours in healthcare, especially in Southeast Asia, concentrating on Malaysia.
4. Pandemic Management with Digitalisation
Since the industrial revolution catalysed by digitalisation, business entities have adopted and increasingly invested in tools and solutions integrating productivity with their resources and equity. This approach intends to ensure the best outcome of produce. However, initiatives by official bodies such as governments, especially within the majority of ASEAN countries, are still insignificant as they materialise only in policy aspects. These efforts are still not on par with the global standards compared to the Western (USA and Canada), European (UK, France, and Germany), and Eastern tech giants such as Australia, China and Japan, who have effortlessly embedded them in their respective societies based on directives and focused on technological advancements [25,26,27,28,29,30]. In Asian countries, the familiarisation with and usage of digitalisation in citizens through media content has been established since 2004. It has continuously upgraded, led by Eastern tech giants such as China, Korea and Japan in mobile technology and various media platforms [18]. However, the assimilation of digitalisation in other branches of public benefits such as healthcare was not successfully embedded because it was not a necessity during those years. Nevertheless, the landscape changed, and effort doubled in most ASEAN countries with the invasion of the COVID-19 pandemic globally, unleashing digitalisation potential in dealing with it. Malaysia is one of the nine reported countries (including Hong Kong, Iceland, India, Indonesia, Poland, Singapore, South Korea and Taiwan) that have developed a digital application to manage the COVID-19 pandemic. Additionally, Malaysia was listed together with Italy, France and Germany as a country that has developed digital applications for contact tracing, which is vital in monitoring and managing the COVID-19 pandemic [19].
On 19 May 2020, the ASEAN countries had a meeting through The ASEAN Emergency Operations Centre Network for Public Health Emergencies (ASEAN EOC Network). It was hosted in Kuala Lumpur via video conferencing among health officials of the ASEAN Member States (AMS) and focused on significant government policies for containment, mitigation and recovery phases in confronting the COVID-19 pandemic. The meetings reported that Thailand was the first country to report pandemic cases outside of China, and on 9 May, it reported 3031 confirmed cases and 56 deaths. These situations were then revealed by each country in terms of their current situation, followed by a response with the implementation of policies, strategies and measures by respective members upon examining the potential challenges and concerns in the next phase of the pandemic response.
Malaysia, Singapore, Thailand, and Brunei mainly used the internet to communicate information to the public, by frequent updates regarding the guidelines and the current situation in terms of confirmed cases, recoveries and deaths from the pandemic. The Thailand health scientists and experts at Bamrasnaradura Infectious Diseases Institute (BIDI) agreed that integrating the current procedures and digitalisation is imperative. This involves the integration of healthcare experts from multi-disciplinary teams, from both public and private sectors, for an effective solution in battling the pandemic [31]. As a country with a population smaller than half a million, Brunei faced a tricky situation, as a small number of confirmed cases might have raised the percentage of the infected. Containment and tracing would fail without caution, causing the infectivity to be at its worst. Therefore, the government used the population as leverage in imposing stricter regulations at their inbound and outbound entry points. The National Disaster Council, a multi-agency group, was established to cater to COVID-19-specific needs. Although the council is occasionally convened, the Ministry of Health Emergency Operations Centre manages day-to-day issues with ad hoc support from other agencies [32]. Although the proximity of Singapore to Brunei is not high, Singapore’s high-density population made it complex to contain the infection. To address this shortcoming, the Singaporean government approached two aspects: government management and public responsibility. The government task force is transparent and frequently provides situational updates and new guidance for the public to engage socially. The information was relayed through every media source available, including press conferences, television broadcasts, and social media updates. In government policy, Singapore enforced the COVID-19 (Temporary Measures) Act and COVID-19 (Temporary Measures) (Control Orders) Regulations 2020 to complement policy measures in managing the outbreak. The legislation allows the government to manage any land, undertaking or other resource for a control order. The act is also based on a legal basis to enforce social distancing measures, such as a limitation on mass gatherings, and hold individuals and business owners accountable for violations [33].
The primary objectives of all the mitigation efforts by the governments of the respective countries were to ensure the maintenance of core health service capabilities nationwide, as a person infected with COVID-19 recovers within 14 days, as identified by WHO. During those two weeks, the country needs to stay focused on treating the infected, ensuring that no life-threatening incidents occur, mainly among vulnerable patients such as the elderly and those with complications and underlying health conditions. Mitigation by implementing technology and integrating it with public health policy, such as the effort shown by Singapore, should be an example to the ASEAN countries. This shows the effort of both the government and public health experts, which will instil confidence in the public and gain cooperation in containment and contact-tracing efforts. In Thailand, hospitals used robotic assistance to detect fevers, which was intended to protect overburdened medical workers. These automated gadgets were called “ninja robots”, first built to monitor recovering stroke patients. They were then enhanced to battle COVID-19 [34]. The endeavours to enhance the roles of robots were a high priority, whereby the features of robots could be upgraded to serve food and medicine to patients and disinfect the wards to curb infections. The Thailand government also announced their plans to provide artificial intelligence (AI) solutions and 5G technology to curb the pandemic. For example, the AI will help doctors with high accuracy by computed tomography (CT). At the same time, the 5G network assists in relieving network congestion to assure the quality of the medical service [35]. The government adopted digital technology in Singapore even before the COVID-19 pandemic. Due to the global public health concerns, the government of Singapore has enhanced its technology capacity in healthcare services. This includes the periodic upgrading of the Integrated Healthcare Information Systems (IHiS) since 2008. The IHiS can be integrated with other systems or devices, including AI devices such as the iThermo, which can perform accurate body temperature screening [36]. In addition, the robot’s functions, known as BeamPro, used for food and medicine dispensers, have also been enhanced [37]. In Brunei, the country focused on the containment of infected persons. The government issued tracking bracelets known as iMSafe for patients under home quarantine and recovered individuals on 30 April 2020, using IoT real-time monitoring and tracking by Bluetooth chips installed with a unique QR code once activated by the wearer [38]. Both academics and public health experts have shared guidance for harvesting more benefits by using the latest technology. These cohesive efforts are seen as shared objectives by all walks of the profession in terms of the shared responsibility to eliminate the infection threat globally. Among the relevant institutions is Johns Hopkins University, which shares its data resources through the Coronavirus Resource Centre online, publishing all aspects and efforts relating to the pandemic [39]. As for the initiatives, the usages of the technology have to be as transparent as possible in order to gain public engagement, which is essential in utilising the implemented systems. The government, in line with policy advised by public health experts, has to ensure the use of these digital data and technologies guided with real-time evidence by respective health experts to gain its buy-in from the public. Therefore, it enhances awareness and makes containment and contact tracing manageable. In battling the swift spread of the COVID-19 pandemic, the Malaysian government sought solutions through various resources, including the use of IR4.0 applications. Other countries have also taken measures to contain the spread of COVID-19. Every government should adhere to and manage the situation swiftly and make use of IR4.0 technology that focuses on containment and contact tracing in breaking the chain of infections. If needed actions are neglected, it will worsen the situation, coupled with anxiety among the public, as validated by studies in countries such as Iran [40] and India [41].
5. Malaysia Healthcare Services
Malaysia has been recognised as a country with robust healthcare services [42]. This triumph is evidence of the Malaysian government’s enhancement of healthcare services after its independence in 1957. Since partial healthcare services were privatised in the 1970s, the coverage of healthcare services has been enhanced, especially in population-dense areas. The MOH governs the healthcare service in Malaysia. This includes managing healthcare facilities in Malaysia, consisting of rural clinics, community clinics, health clinics and hospitals. Hospitals are split into secondary and tertiary healthcare services. According to Health Facts 2019, published by the MOH, there are 144 government hospital facilities, providing 42,424 beds, and 1090 government clinics as primary care. Next, private healthcare facilities comprise 210 private hospitals, providing 16,957 beds, and 7718 private clinics. This comes with a total ratio of doctors to patients of 1 to 530 nationwide, with healthcare services expenditure of 4.24% of 2017 GDP. These services have increased Malaysians’ life expectancy to 72.7 years old among males and 75 years old among females [43]. The MOH desires to assist each individual in achieving a level of health which enables them to manage their life economy and be socially productive, while taking the social responsibilities to give the best and most effective health services. The MOH’s mission is to create a nation of healthy individuals, families and communities supported through an affordable, equitable, technologically appropriate, efficient, consumer-friendly, and environmentally adaptable health system [44].
6. Pandemic in Malaysia
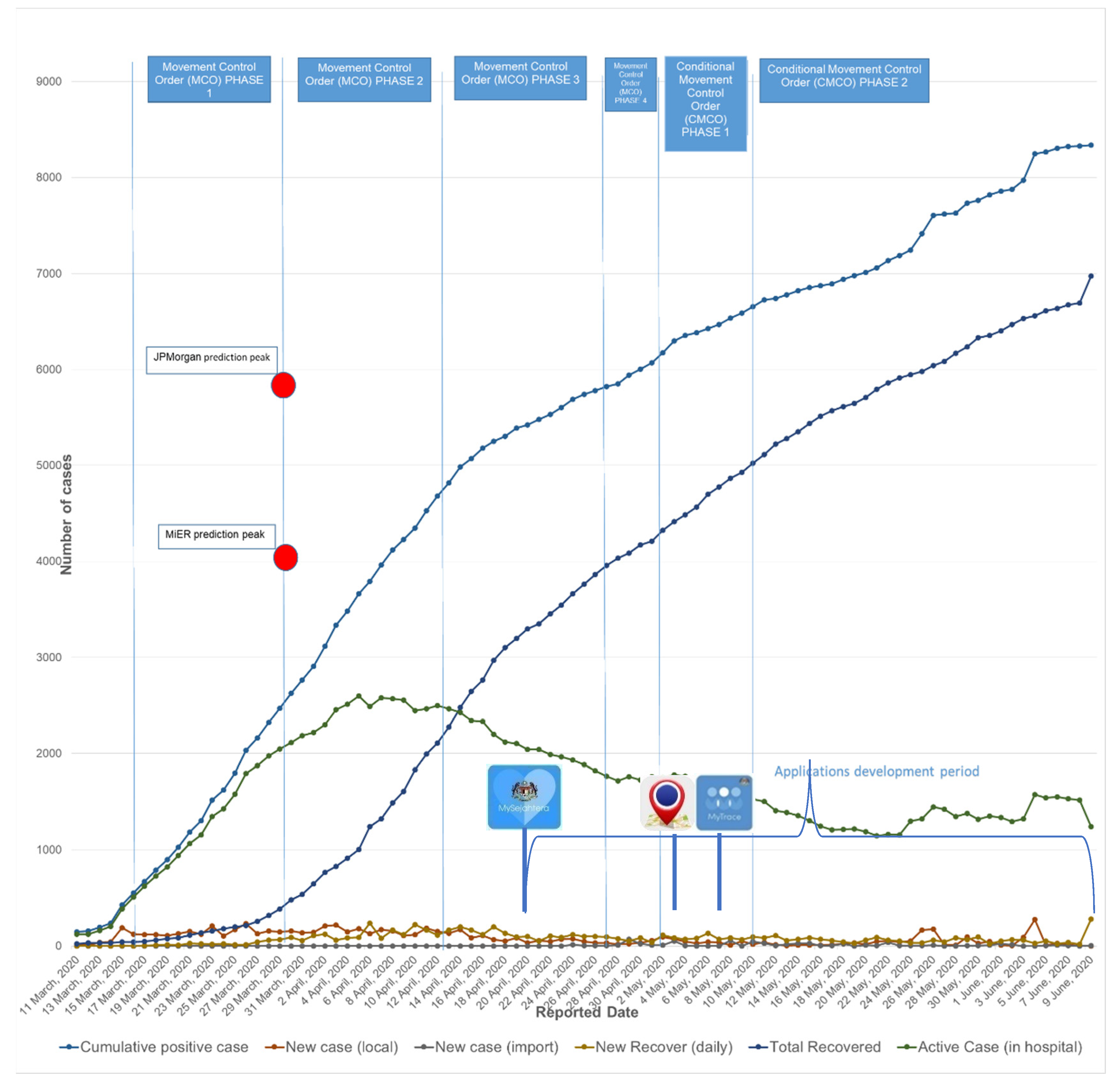
As COVID-19 spread across the globe, including in Malaysia, some studies predicted the infection exponent, such as those by JPMorgan Chase & Co and the Malaysian Institute of Economic Research (MiER). As the virus is relatively unexplored, the MOH considered every related report and carefully analysed the contents. The infection rate and demographic were thoroughly analysed to find the best solution for flattening the curve and leading the country out of the exponential. Among the reports are local research studies conducted by JPMorgan and MiER. In the press statement made by MiER, they projected that the number of Malaysians infected with COVID-19 by the end of March 2020 would be approximately 4087 cases, where 12.51% of the increase in cases lies between 24 to 31 March. This projection is compared to the actual percentage of reported cases, which has a point margin of 5.02%. Meanwhile, on 25 March 2020, JPMorgan projected that the COVID-19 cases in Malaysia would peak with 6300 cases in April.
There were four phases of Movement Control Order (MCO) and two phases of Conditional Movement Control Order (CMCO) from 18 March 2020 until 9 June 2020 to control the spread of COVID-19, as shown in Table 2. The data set shown in Figure 1 presents data in parallel coordinates consisting of cumulative positive cases, daily recovery cases, new local transmission, current active cases and new cases detected from quarantine (compulsory 14 days for coming from abroad), and the data range from 11 March to 9 June 2020. From the linear regression graph, to quantify the prediction and forecasting of the infection and analyse different phases of MCO, it is shown that the efforts in reducing new cases were practical during the implementation of MCOs. The active cases started to decline in the second phase of MCO, and in the same phase, the figure also shows the inclining daily recovery that exceeded the number of active cases. From the daily press statement made by MOH, the daily positive cases of COVID-19 were on average 70% lower than daily recovered cases starting 8 April during the second phase of MCO. The incline in recovering cases shows positive signs in terms of Malaysia’s healthcare as the situation is under control. This has resulted in advantages to the MOH in providing treatment to all patients diagnosed with COVID-19.
Table 2.
The implementation of Movement Control Order (MCO) and Conditional Movement Order (CMCO) in Malaysia.
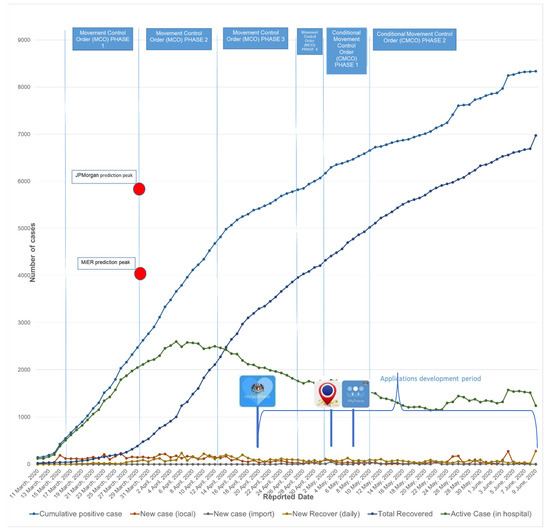
Figure 1.
Malaysia COVID-19 infection demographic with MCO, CMCO and new digital application implementation.
The data gathered as tabulated in Figure 1 show that Malaysia defied the projection report from MiER and JPMorgan Chase & Co. (Hong Kong) [45,46], whereby Malaysia flattened the curve of active cases during the second phase of MCO, or after 19 days since the first phase of MCO was enforced. Although there were new cases every day, the hike was neither steep nor a surge. The efforts during the MCO were supported by MOH medical capabilities and an inter-agency initiative with the objective to achieve containment and contact tracing. The relevant actions include preparing a designated quarantine centre, enhancing the virus test centre, dedicated COVID-19 hospitals for treatment, and contact tracing. During COVID-19, the MOH managed its hospitals throughout the nation by segregating them into prominent roles. Of 144 total government hospitals nationwide, only selected hospitals were involved: 57 hospitals for screening; 28 hospitals as referral hospitals for attending persons under investigation (PUI) or confirmed cases; 18 hospitals as testing laboratories; and 26 dedicated treatment hospitals [47].
When a person is confirmed to be infected with COVID-19, the person is questioned to determine the origin of infection and their travelling history. These tasks are handled by the District Health Office and the police. There are 167 District Health Offices in Malaysia, and each plays a momentous role in delivering public health services and managing resources within a district. The MOH’s effort in reducing the spread of COVID-19 consists of implementing targeted approach action performed by the District Health Office with their surveillance and prevention team. As of 12 May 2020, 271,721 tests had been conducted by the MOH. Of those tests, 2.48% or 6742 cases were found to be positive for COVID-19. Of the total reported positive cases, 77% recovered, which left 23% able-to-infect or active cases nationwide, confirming the lowest daily case count ever compared to the cases before 12 May 2020 [48]. During the outbreak, one of the essential efforts to control the spread is via health screening and isolation [49]. Advancements in technology, mainly using digital applications, can reduce the virus spread via the monitoring performed by authorities, and patients being able to monitor their health and isolation status [19,20]. The data and information obtained from digital transformations in healthcare, especially those related to remote usage such as mobile applications, can serve as essential inputs for extensive data analysis, enabling better future planning [21].
7. Malaysia Digitalisation Leap
The Malaysian government tried to flatten the exponential curve of COVID-19 cases by implementing MCO on 18 March 2020. At the same time, the Malaysian government also utilised IR4.0 in battling the disease. The IR4.0 initiative has been progressing slowly in past years. However, due to COVID-19, there has been a global shift in IR4.0. For example, China and South Korea are using the application of IR4.0 to trace and contain patients diagnosed with COVID-19 [22]. Although Malaysia may not be the first of the Southeast Asian countries to have implemented and used applications of IR4.0, the current initiative in Malaysia has shown that the government’s efforts are in line with the global trend. This especially applies in embracing the new technology disciplines and the inception of a new era. There are four applications officially announced by the Malaysian government to control the spread of COVID-19. Three of them are newly developed, as shown in Figure 1.
The first application is known as The DoctorOncall. This application was developed in 2016 but was further enhanced in 2020 to incorporate public–private healthcare collaboration to battle COVID-19. The enhanced feature of The DoctorOncall is providing virtual health advice from both the public and healthcare professionals to the address worries and panic accompanying the current COVID-19 spread. This health advice is provided free of charge to Malaysian citizens, where information dissemination through risk communication is essential to provide proper guidance during the outbreak [23]. Besides The DoctorOncall, the Malaysiam government has developed another smartphone app to address COVID-19 issues, known as Gerak Malaysia. Gerak Malaysia was launched on 17 April 2020 to help the police and Ministry of Health (MOH) to trace and analyse users’ movement nationwide to contain the spread of the pandemic. Gerak Malaysia provides a digital ID in the form of a QR code that contains users’ personal information, where users need to register or apply for inter-state travelling permission via the applications from their smartphones instead of applying manually at police stations. During the second phase of MCO and after the launching of Gerak Malaysia, on 21 April 2020, the application MySejahtera was launched to strengthen the effort to give the correct information about COVID-19 updates. The MySejahtera apps were jointly developed by four government bodies, which are the Multimedia Commission of Malaysia (MCMC), National Security Council (NSC), Ministry of Science and Technology (MOSTI) and MOH, enduring strategic partnership in the application development. This app is designed for the public to receive the latest information and statistics on the COVID-19 pandemic in Malaysia. The MySejahtera apps are also applicable for persons under investigation (PUI) quarantined during the MCO. The apps deliver a self-evaluation feature that evaluates whether a person is at risk of infection. It also guides needed action if a person is infected with COVID-19, and the apps also frequently revise infection hotspots. The MySejahtera apps served as an interaction platform between authorities and the public, which is the key to pandemic risk management [24].
This continuous effort by the government, promoted through its branch of ministries and agencies, has resulted in various applications to manage the pandemic effectively. In the beginning, the application known as MyTrace was launched on 4 May 2020. Objectively, MyTrace, developed by the Ministry of Science and Technology (MOSTI), acts as a contact-tracing tool to avoid the second wave of the spread. The application aims to help the government to trace individuals who may have met anyone carrying the COVID-19 virus. The application operates with wave detection by Bluetooth connectivity, which recognises the distance and duration of the devices approaching patients diagnosed with COVID-19. The data collected are kept for 21 days in the users’ devices for contact tracing. The government gave assurances that the users’ data would be anonymised and that MyTrace was not meant to collect geo-location information. In order to encourage public use and create one single point of contact and information source, both MySejahtera and MyTrace are interconnected to complement the services provided by both apps.
Table 3 shows the digital applications used to control the spread of COVID-19 in Malaysia at the beginning of the pandemic. The coupling of administrative orders with digital applications in terms of usage effectiveness in Malaysia can be evaluated by R Naught or R0 indicators. This mathematical term indicates how contagious and infectious a disease is. Malaysia initially recorded an R0 of 3.5 when the Movement Control Order (MCO) was imposed nationwide on 18 March. According to The Edge Market report referring to statements from the Director-General of Health, the value, however, was successfully reduced to 0.3 following positive outcomes of governmental actions taken and strict compliance with the standard operating procedures among the public [50]. Actions such as implementing IR4.0 usage initiatives for containment and contact tracing contributed to these results.
Table 3.
Digital applications used to manage the COVID-19 pandemic in Malaysia.
The use of digital systems in healthcare services was initiated around the 1960s, due to the invention of the computer and ICT [51]. In 2020, particularly during the COVID-19 pandemic, WHO has encouraged all its member countries to invest in and prioritise digital systems in healthcare services [52]. Many countries have adopted the use of digital applications in the COVID-19 pandemic. Hence, comparing countries with and without digital applications is problematic. Furthermore, many other factors influence cases of COVID-19, aside from digital applications. This paper strived to show the success story in Malaysia using digital applications, where the use of such applications has, in a way, controlled and monitored the cases of COVID-19. This initiative follows Malaysia’s Public Sector Digitalisation Strategic plan 2021–2025, released under the 12th Malaysia Plan [53].
8. Conclusions
One of the pursuits of developing digital applications is to ‘flatten the curve’ of COVID-19 infection, where such applications are expected to be capable of being integrated with artificial intelligence (AI), machine learning, deep learning, big data analytics, Google trends and others. These digital applications should be assessed to ensure they have fulfilled the development objectives. The design and establishment of a digital application should also assess the socio-technical aspect and the policy directions in ensuring the community’s social well-being during the pre- and post-technology intervention.
Ergo, this article confirmed that the digital applications developed to control and manage the COVID-19 pandemic succeeded, particularly in Malaysia, focusing on containment and contact tracing. The digital application is a quintessential tool for the general public, medical officers, and decision makers to control and manage the COVID-19 pandemic. A limitation of the study was the timeframe, as this article did not capture a longer timeframe. Furthermore, as discussed above, even if the researchers extended the timeframe, other factors, such as the existence of different virus variants, might influence the review. Accordingly, this review only focused on the efforts by the Malaysian government in controlling the spread of COVID-19 outbreaks in Malaysia from 11 March to 9 June 2020 (90 days) with a distinct focus on the aspects of containment and contact tracing.
Containment and contact tracing work as crucial tools in public health as a pandemic response which has been proven to break the chain of transmission and limit the spread. Although managing the COVID-19 pandemic requires unprecedented tactics and roles from governments across the globe, the key objectives remain similar. Therefore, assimilating the latest technology through digitalisation is among the initiatives enhancing the tools of pandemic control in public health, alongside the “old ways” (manual record and analysis), which has proven beneficial and provided hope to win the battle. The initiative by the Malaysian government to optimise digital technologies usage by developing applications to break the chain of COVID-19 infection has aided both the public and the government.
This review established that the implementation of MCO in its early phase was not effective in contact tracing and isolation. Hence, there were growing clusters of COVID-19 cases and the emergence of new cluster cases, even though the numbers of positive cases were low. Nonetheless, with the establishment of digital applications during MCO, the spread of COVID-19 was controlled in Malaysia. The use of digital technology reflects the hope which holds the key to these unified objectives. In contrast, constant upgrades will soon provide Malaysia with an accessible, integrated, high-quality, and reasonable healthcare system. The coupling of digital applications and the government administrative orders was proved to flatten the curve of COVID-19 in Malaysia, as analysed successfully. In future research, more detailed studies that consider a longer timeframe, different variants of the virus, and the global trends of COVID-19 should be conducted to authenticate the digital applications’ effectiveness in controlling and monitoring the COVID-19 pandemic.
Author Contributions
Conceptualisation, M.F.B.M.A.; methodology, M.F.B.M.A.; software, M.F.B.M.A.; validation, M.F.B.M.A. and G.C.T.; formal analysis, M.F.B.M.A. and G.C.T.; investigation, M.F.B.M.A.; resources, M.F.B.M.A.; data curation, M.F.B.M.A. and G.C.T.; writing—original draft preparation, M.F.B.M.A.; writing—review and editing, G.C.T.; visualisation, G.C.T.; supervision, G.C.T.; project administration, G.C.T.; funding acquisition, G.C.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). Situation Report 143. Available online: www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 11 June 2020).
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 June 2020).
- Wang, Z. The Coronavirus Prevention Handbook 101Science Based Tips That Could Save Your Life; Simon and Schuster: New York, NY, USA, 2020; Print ISBN 978-1-5107-6241-1; EBook ISBN 978-1-5107-6244-2. [Google Scholar]
- Malaysia Prime Minister. Malaysia Labour Day 2020 Special Address Speech. 2020. Available online: https://www.pmo.gov.my/2020/05/perutusan-khas-perdana-menteri-sempena-hari-pekerja-2020/ (accessed on 13 June 2020).
- Faziharudean, T.M.; Mitomo, H. Explaining Digital Divide as a Consequence of Uneven Digital Opportunities between Urban and Rural Areas: A Case of Internet Usage among Senior High School Students in Kelantan, Malaysia. Stud. Reg. Sci. 2002, 33, 287–298. [Google Scholar] [CrossRef]
- Razak, N.; Malek, J. Bridging digital divide in Malaysia: Cyber learning for the marginalized community. Distance Learn. Internet Conf. 2008, 2008, 235–239. Available online: http://www.waseda.jp/DLI2008/program/proceedings/pdf/session9-1.pdf (accessed on 5 July 2021).
- Sheikh Dawood, S.R.; Ghazali, S.; Samat, N. Digital divide and poverty eradication in the rural region of the northern Peninsular Malaysia. Indones. J. Geogr. 2019, 51, 172–182. [Google Scholar] [CrossRef]
- Alidjinou, E.K.; Demaret, J.; Faure, K.; Deplanque, D.; Bocket, L.; Duhamel, A.; Sobaszek, A.; Hober, D.; Hisbergues, M. Articles Immunogenicity of BNT162b2 vaccine booster against SARS-CoV-2 Delta and Omicron variants in nursing home residents: A prospective observational study in older adults aged from 68 to 98 years. Lancet Reg. Health-Eur. 2022, 17, 100385. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Théberge, P. Digitalization. In The Routledge Reader on the Sociology of Music; Routledge: Abingdon, UK, 2015; pp. 329–338. [Google Scholar] [CrossRef]
- Ritter, T.; Pedersen, C.L. Digitization capability and the digitalization of business models in business-to-business firms: Past, present, and future. Ind. Mark. Manag. 2020, 86, 180–190. [Google Scholar] [CrossRef]
- Abbate, J. Inventing the Internet. In Inventing the Internet; The MIT Press: Cambridge, MA, USA; London, UK, 1999. [Google Scholar] [CrossRef]
- Gairola, R.K.; Roth, M. Cyber zones: Digital spatialities and material realities across Asia. Asiascape: Digit. Asia 2019, 6, 4–16. [Google Scholar] [CrossRef]
- Hersh, W.R.; Hickam, D.H.; Severance, S.M.; Dana, T.L.; Krages, K.P.; Helfand, M. Diagnosis, access and outcomes: Update of a systematic review of telemedicine services. J. Telemed. Telecare 2006, 12, 3–31. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. Telemedicine Flagship Application: Malaysia’s Telemedicine Blueprint Leading Healthcare into the Information Age. 1997. Available online: https://www.moh.gov.my/moh/resources/auto%20download%20images/5ca1b20928065.pdf (accessed on 5 July 2021).
- Ministry of Health. FRB/HIS/LIS/2005/Version 1.2; Ministry of Health: Putrajaya, Malaysia, 2006; ISBN 983-9417-51-7. [Google Scholar]
- Bowker, C.G.; Star, S.L. Science and Technology, Social Study of: Computers and Information Technology; Elsevier Ltd.: Orlando, FL, USA, 2001; Volume 20, pp. 13638–13644. [Google Scholar]
- Schneider, F.; Goto-Jones, C. Revisiting the Emancipatory Potential of Digital Media in Asia—Introduction to the Inaugural Issue of Asiascape: Digital Asia. Asiascape Digit. 2014, 1, 3–13. [Google Scholar] [CrossRef]
- John, H.; Singh, L.; Couch, D.; Yap, K. Mobile Health Apps That Help With COVID-19 Management: Scoping Review. JMIR Nurs. 2020, 3, e20596. [Google Scholar] [CrossRef]
- Rahmet GÜNER, İmran HASANOĞLU, Firdevs AKTAŞ COVID-19: Prevention and control measures in community. Turk. J. Med. Sci. 2020, 50, 571–577. [CrossRef]
- Kondylakis, H.; Katehakis, D.G.; Kouroubali, A.; Logothetidis, F. COVID-19 Mobile Apps: A Systematic Review of the Literature. J. Med. Internet Res. 2020, 22, e23170. [Google Scholar] [CrossRef]
- Alsunaidi, S.J.; Almuhaideb, A.M.; Ibrahim, N.M.; Shaikh, F.S.; Alqudaihi, K.S.; Alhaidari, F.A.; Khan, I.U.; Aslam, N.; Alshahrani, M.S. Applications of Big Data Analytics to Control COVID-19 Pandemic. Sensors 2021, 21, 2282. [Google Scholar] [CrossRef]
- Husnayaina, A.; Fuad, A.; Sua, E.C.-Y. Applications of Google Search Trends for risk communication in infectious disease management: A case study of the COVID-19 outbreak in Taiwan. Int. Soc. Infect. Dis. 2020, 95, 221–223. [Google Scholar] [CrossRef]
- Elavarasan, R.M.; Pugashendhi, R. Restructured society and environment: A review on potential technological strategies to control the covid-19 pandemic. Sci. Total Environ. 2020, 725, 138858. [Google Scholar] [CrossRef]
- Revitalization, T.H. for J.E. New Robot Strategy, Japan’s Robot Strategy. 2015. Available online: https://www.meti.go.jp/english/press/2015/0123_01.html (accessed on 5 July 2021).
- Yves Paindaveine. Overall Analysis of National Initiatives for Digitising European Industry. 2017. Available online: https://ec.europa.eu/futurium/en/system/files/ged/national_initiatives_for_digitising_industry_across_the_eu.pdf (accessed on 5 July 2021).
- Fuchs, C. Industry 4.0: The Digital German Ideology. Triplec Commun. Capital. Crit. 2018, 16, 280–289. [Google Scholar] [CrossRef]
- Ma, H.; Wu, X.; Yan, L.; Huang, H.; Wu, H.; Xiong, J.; Zhang, J. Strategic Plan of Made in China 2025 and Its Implementations. In Analysing the Impacts of Industry 4.0 i9n Business Environments; IGI Global: Hershey, PA, USA, 2018; pp. 1–23. ISBN 13: 9781522534686. [Google Scholar]
- Ministry of Economy, Trade and Industry Government of Japan Japan’s New Robot Strategy. 2018. Available online: https://www.djw.de/ja/assets/media/Veranstaltungen/Symposium,%20MGV/duesseldorf-20180416/djw-symposium-duesseldorf-16.04.2018-kurihara-meti.pdf (accessed on 5 July 2021).
- European Comission. Monitoring Progress in National Initiatives on Digitising Industry—Country Report Finland; European Comission: Brussels, Belguim, 2019. [Google Scholar]
- Koh, D. COVID-19: Lessons from Thailand’s BIDI & Samitivej Group of Hospitals. 2020. Available online: https://www.healthcareitnews.com/news/apac/covid-19-lessons-thailand-s-bidi-samitivej-group-hospitals (accessed on 10 August 2021).
- Wong, J.; Koh, W.C.; Alikhan, M.F.; Aziz, A.B.Z.A.; Naing, L. Responding to COVID-19 in Brunei Darussalam: Lessons for small countries. J. Glob. Health 2020, 10, 010363. [Google Scholar] [CrossRef]
- Chua, A.Q.; Tan, M.M.J.; Verma, M.; Han, E.K.L.; Hsu, L.Y.; Cook, A.R.; Teo, Y.Y.; Lee, V.J.; Legido-Quigley, H. Health system resilience in managing the COVID-19 pandemic: Lessons from Singapore. BMJ Glob. Health 2020, 5, e003317. [Google Scholar] [CrossRef]
- The Star. Covid-19: Thai Hospitals Deploy ‘Ninja Robots’ to Aid Virus Battle. 2020. Available online: https://www.thestar.com.my/tech/tech-news/2020/03/19/covid-19-thai-hospitals-deploy-ninja-robots-to-aid-virus-battle (accessed on 10 August 2021).
- The Star. Thai Hospital Uses AI Solutions and 5G Technology to Fight Covid-19. 2020. Available online: https://www.thestar.com.my/news/regional/2020/04/16/thai-hospital-uses-ai-solutions-and-5g-technology-to-fight-covid-19 (accessed on 10 August 2021).
- Ramanathan, N. Battling Covid-19 with Transformational Tech: Singapore Case Study. 2020. Available online: https://www.luxresearchinc.com/blog/battling-covid-19-with-transformational-tech-singapore-case-study (accessed on 10 August 2021).
- The Scoop. COVID-19 Live Updates: April archive: An Archive of Our Live Blog from 4–30 April 2020. Available online: https://thescoop.co/2020/04/04/covid-19-live-updates-2/ (accessed on 10 August 2021).
- Harian, S.; Brunei Guna Gelang Jejak Individu Dikuarantin. Sinar Harian. 2020. Available online: https://www.sinarharian.com.my/article/82548/GLOBAL/Brunei-guna-gelang-jejak-individu-dikuarantin (accessed on 10 August 2021).
- Johns Hopkins University & Medicine. Coronavirus Resource Center. 2020. Available online: https://coronavirus.jhu.edu/about (accessed on 10 August 2021).
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Roya, D.; Tripathya, S.; Kara, S.K.; Sharmaa, N.; Vermaa, S.K.; Kaushalb, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Asia Pacific Observatory on Health Systems and Policies. In Malaysia Health System Review; Health Systems in Transition; (NLM Classification: WA 540); WHO Press: Geneva, Switzerland, 2012; Volume 2, ISBN 978 92 9061 584 2. [Google Scholar]
- Ministry of Health Malaysia. Health Facts 2019. Planning Division Health Informatics Centre. Planning Division Health Informatics Centre. MOH/S/RAN/152.19 (PT)-e. 2019. 2020. Available online: https://www.moh.gov.my/moh/resources/Penerbitan/Penerbitan%20Utama/HEALTH%20FACTS/Health%20Facts%202019_Booklet.pdf (accessed on 5 July 2021).
- Ministry of Health Malaysia (MOH). Planning Division. Healthcare Services Transformation Planning 2015. Available online: https://www.moh.gov.my/index.php/file_manager/dl_item/554756755a584a6961585268626939515a57356c636d4a706447467549465630595731684c31426c62474675494652795957357a5a6d39796257467a6153424c5a584e706147463059573476524739726457316c626c39515a577868626c3955636d467563325a76636d316863326c6655475679613268705a473168644746755830746c63326c6f59585268626c39665a6d6c75595777756347526d (accessed on 5 July 2021).
- JPMorgan. JPMorgan Says Worst Is Yet to Come, Predicts Malaysia’s Covid-19 Infection Rate Will Peak Mid-April. 2020. Available online: https://www.malaymail.com/news/malaysia/2020/03/24/jpmorgan-says-worst-is-yet-to-come-predicts-malaysias-covid-19-infection-ra/1849724 (accessed on 10 August 2021).
- Malaysian Institute of Economic Research (MiER). MIER TIGER Research Group. 2020. Available online: https://www.mier.org.my/the-economic-impacts-of-covid-19/ (accessed on 10 August 2021).
- Ministry of Health Malaysia (MOH). 2020. Available online: http://www.moh.gov.my/index.php/pages/view/2264 (accessed on 5 July 2021).
- Ministry of Health Malaysia (MOH). Malaysia COVID-19: Officials Report Lowest Daily Case Count Ever. 2020. Available online: http://outbreaknewstoday.com/malaysia-covid-19-officials-report-lowest-daily-case-count-ever-69826/ (accessed on 10 August 2021).
- Bernama Radio Bernama TV. Using IR 4.0 Apps to Combat COVID-19. 2020. Available online: https://www.bernama.com/en/features/news.php?id=1832865 (accessed on 15 December 2020).
- The Edge Market. Health DG Warns of Exponential Surge of COVID-19 Cases in June If Malaysians Do Not Comply with SOP. 2020. Available online: https://www.theedgemarkets.com/article/moh-says-covid19-infection-rate-will-rise-again-if-people-do-not-comply-sop (accessed on 10 August 2021).
- Arvanitis, S.; Loukis, E.N. Investigating the effects of ICT on innovation and performance of European hospitals: An exploratory study. Eur. J. Health Econ. 2016, 17, 403–418. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Report on Health Data Systems and Capacity; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Star, T.; Digitalisation Innovates Public. The Star 2021. Available online: https://www.thestar.com.my/news/nation/2021/10/03/digitalisation-innovates-public-service-delivery (accessed on 20 January 2022).




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).