Abstract
In the New Normal era of “Living with COVID-19”, we need a measure of the safety of street spaces. Social distancing during a pandemic is considered an effective safety measure, but the current binary threshold approach to social distancing is clearly inadequate for evaluating and monitoring the risk of infection on urban streets. This study is to propose a social distancing indicator that can quantitatively evaluate the level of exposure to viral infection for pedestrians using urban streets during a pandemic, and to develop a statistical model to estimate the proposed indicator from simulations of pedestrian activity on urban streets. We assumed that the risk of infection on urban streets has a direct relationship with distance between pedestrians. The social distancing indicator was based largely on the findings of past studies. We developed a statistical model to relate the proposed indicator to three other explanatory variables: pedestrian density, clumpiness, and directional heterogeneity. We used pedestrian simulation to generate the raw data for these explanatory variables. The social distancing indicator demonstrated a statistically significant relationship with input variables and can be used to evaluate pedestrians’ social distancing on urban streets. We measured the relationship between different levels of pedestrian density, clumpiness, and directional heterogeneity and related the results to the potential level of exposure to viral infection. Health agencies can use the findings to develop appropriate policies for monitoring and improving the social distance between pedestrians on urban streets during a pandemic.
1. Introduction
The COVID-19 pandemic has greatly changed public health concepts and people’s daily lives. In addition to vaccination, various non-pharmacological interventions were taken to slow the spread of the virus. The interventions introduced in an attempt to minimize the spread of COVID-19 infection include personal hygienic measures (such as mask wearing and frequent hand-washing) and restrictions on socio-economic activities (e.g., stay at home order, work from home, and closing non-essential facilities) and personal movement (e.g., reducing passenger capacity in public transit facilities) [1,2,3,4,5,6].
These non-pharmacological interventions demonstrated an effect in reducing the spread of COVID-19, and after vaccine development, the number of confirmed cases dramatically decreased in countries with high vaccination rates. However, despite steady vaccination, COVID-19 continues to spread worldwide due to the occurrence of multiple variants. As a result, the New Normal era after this pandemic is more likely to be “Living with COVID-19”, and there has been a great deal of discussion about it [7,8,9].
The use of active transportation modes, including walking, increased during the COVID-19 pandemic [5,10]; in the New Normal era of “Living with COVID-19”, people are expected to actively use urban public spaces, including streets, as before the pandemic. Walking activities on urban streets are recognized as a basic catalyst for sustainable urban operation and an important factor determining the quality of urban life [11]. Walking activities in urban public spaces benefit people’s physical as well as mental health [12,13,14,15], and are also associated with the local economy [16,17]. However, unless the pandemic is completely over, direct close contact between people on the street can still cause the virus to spread. It is important to ensure that urban streets are safe from becoming a possible origin of future waves of COVID-19 [18,19].
Social distancing is regarded as one of the most effective interventions for preventing the spread of the virus and may need to be continued until the development of COVID-19 vaccines and possibly even after [2,20,21,22,23,24]. We understand that social distancing to reduce the chance of in-person contact includes isolation and quarantine at home and maintaining a certain physical distance (e.g., 2 m) between people in public spaces [25], but in this study, we use the term social distancing to refer to physical distancing between people in public spaces, such as urban streets.
Many cities have already implemented various mobility interventions to help improve social distancing in urban street spaces. Interventions include closing streets temporarily, changing the cross-sectional design to widen pedestrian walkways, controlling traffic volume, and/or expanding the active transportation network [18,26,27,28,29,30]. These measures are designed to promote social distancing by modifying the design and/or operational aspects of the existing infrastructure (e.g., the Slow Streets program in San Francisco [31] and ActiveTO program in Toronto [32]). Some cities in North America, for example, New York and Toronto, have introduced strong social distancing regulations (e.g., minimum 6 ft or 2 m) coupled with enforcement for people in some public spaces rather than simply relying on voluntary participation [33,34]. The underlying goal of these mobility interventions is the promotion of social distancing to prevent close contact between people who move around a city [18].
1.1. Importance of Social Distancing Evaluation
Urban Systems (2020) has proposed the development of a systematic urban street management plan to create a resilient and flexible urban street space for the post-COVID-19 era [29]. In addition to the recent mobility interventions, Urban Systems (2020) proposes short-, medium-, and long-term plans to prepare for future waves of virus spread [29]. The plans incorporate a set of flexible strategies that can be implemented according to the evaluation results of social distancing. However, despite the importance of monitoring for social distancing, a reasonable evaluation system for social distancing has not yet been established. Current social distancing approaches are based mainly on a single binary threshold for the recommended physical distance. For example, the threshold is 2 m (6 ft) for North American jurisdictions and the United Kingdom, 1.5 m for Germany and Australia, and 1 m for France and Denmark [35]. These binary thresholds have some limitations.
Firstly, no single binary distance appears to have clear scientific support among health scientists regarding the presence or absence of viral infection risk. Feng et al. (2020) pointed out that a single threshold for social distancing contains large uncertainty and it is very difficult to use a single distance as a measure of the varying risk of virus transmission between people [36]. Many studies have investigated the risk of infection within certain distances. The possibility of person-to-person virus transmission arises when people exhale droplets that stay in the air. Blocken et al. (2020) used aerodynamics-based simulation to test the social distance required to minimize infection between pedestrians [37]. The simulation demonstrated the flow pattern of pedestrians’ droplets. The researchers found that if people were assumed to walk at a constant speed of 4 km/h, 5 m was a more appropriate social distance for avoiding exposure to other pedestrians’ droplets. Bourouiba (2020) pointed out that under certain warm and moist conditions, a person’s droplets can travel up to 8 m when sneezing [38]. At this moment, all we can say is that people’s risk of viral infection in a pandemic such as COVID-19 varies and depends in part on the distance between them.
Secondly, the distances between pedestrians on urban streets constantly vary and are not easy to measure accurately in real-time without advanced technology, such as computer vision sensor technology using CCTV [39].
Thirdly, even if distance is useful for evaluating the risk of infection and the most appropriate distance could be determined and maintained, the distance chosen does not translate into a direct indication of the proper type of mobility intervention (e.g., widening available walking space, enhancing public education, introducing policing enforcement, etc.) for a public space.
1.2. Study Goal and Objectives
This study goal is to develop a social distancing evaluation model that can measure different levels of social distancing under different pedestrian walking conditions to assess how well social distancing is being achieved, with a view to evaluating, monitoring, and managing the appropriate level of social distancing on urban streets during a pandemic.
The study has two objectives:
- to propose a social distancing indicator that can quantitatively evaluate different levels of social distancing and provide a more sophisticated approach than the current binary distance threshold approach, and
- to develop a statistical model to estimate the proposed indicator using selected explanatory variables that do not require measuring exact distance between pedestrians.
2. Method
The study adopted a two-step process: (1) development of a social distancing indicator (SDI) to provide an indication of the relative exposure to COVID-19 infection, and (2) development of a statistical model.
The proposed SDI can be regarded as a measure to evaluate the level of social distancing on urban streets. The indicator’s mathematical form was developed mainly from the findings of past studies. The statistical model was developed to relate the SDI to selected explanatory variables. The statistical model used the least square method to estimate the parameters associated with the explanatory variables. Pedestrian simulations were conducted under a variety of walking conditions to generate raw data for the SDI and other explanatory variables.
2.1. Developing the Social Distancing Indicator
To develop the SDI, we made four assumptions.
- We assumed that the SDI provides a surrogate safety measure that represents different levels of exposure to viral infection. However, the indicator is simply a relative risk measure and does not represent the absolute or real infection risk of contracting a virus.
- We assumed that the level of exposure to viral infection on urban streets has a direct relationship with distance between pedestrians (i.e., the risk increases as the distance between pedestrians decreases). Notice that in the SDI equations proposed, we did not explicitly consider factors that can also affect pedestrians’ risk of infection such as wind speed, walking speed, wearing a mask, etc. [36,37,40,41]. Note, however, that the effect of wearing a mask (presumably one of the most important personal protectives available) can be indirectly considered in a way by multiplying a carefully chosen factor value(s) to the proposed SDI in this study.
- We assumed that the level of social distancing for a particular space can be estimated as the sum of the indicator values estimated for all the individual pedestrians in the space at the same time. All pedestrians walk individually (not in pairs) with an assumption that none of the pedestrians live in the same household.
- We assumed that a pedestrian’s risk of viral infection is proportional to the length of time the individual is exposed to the potential infection risk measured by the proposed indicator. The risk increases as the exposure time to the proposed indicator increases.
We developed the SDI using a distance decay function. As the distance between people increases, the exposure to viral infection between people decreases by a certain ratio. Beyond a certain pre-set distance, the exposure eventually becomes zero. The mathematical form of the SDI for an individual can be defined as Equation (1):
where is the distance between pedestrians ( > 0), is the decreasing ratio of potential infection risk by distance (), and is a constant representing the maximum risk when the distance is equal to zero.
In this study, and were determined from past study results. Numerous studies have reported changes in the risk of viral infection according to distance. Chu et al. (2020) systematically reviewed 172 relevant studies and conducted a meta-analysis using 44 selected studies [40]. From the meta-analysis, they reported that each additional meter of social distance reduced the risk of viral infection by approximately 50% (=1/2.02). For the distance at which point the risk of infection is assumed to be zero (i.e., the boundary condition), we used 8 m. This is the distance reported by Bourouiba (2020), as the maximum distance droplets from human sneezing reached a certain air flow condition [38].
From these past studies, we set the decreasing rate of viral infection risk by distance d as 1/2.02, resulting in the mathematical form for the SDI provided in Equation (2).
As we assumed that each pedestrian had a potential exposure to infection from each pedestrian in the same space and that the exposures could be combined, the individual pedestrian’s social distancing indicator is calculated as Equation (3):
where, i indicates a target pedestrian, and j indicates all the other pedestrians in the same space.
By simply summing the for all pedestrians walking along the same space, we can estimate the total level of exposure in the space. However, since the SDI focuses on measuring how well social distancing is being achieved among people in that space, the average value of was assumed to be the SDI of the space (), as illustrated in Equation (4):
where, i indicates an individual pedestrian, and n indicates the total number of pedestrians in that space.
In addition, if it is necessary to measure the amount of potential exposure to viral infection accumulated over time for an individual pedestrian and space , and can simply be integrated over time, as illustrated in Equations (5) and (6), respectively:
2.2. Developing the Statistical Model
A statistical model was developed to estimate the , using three explanatory variables. Equation (4) represents the response variable of the proposed statistical model and measures the potential exposure to viral infection in an area of study with a certain pedestrian flow. As social distancing between people in a space decreases, the increases.
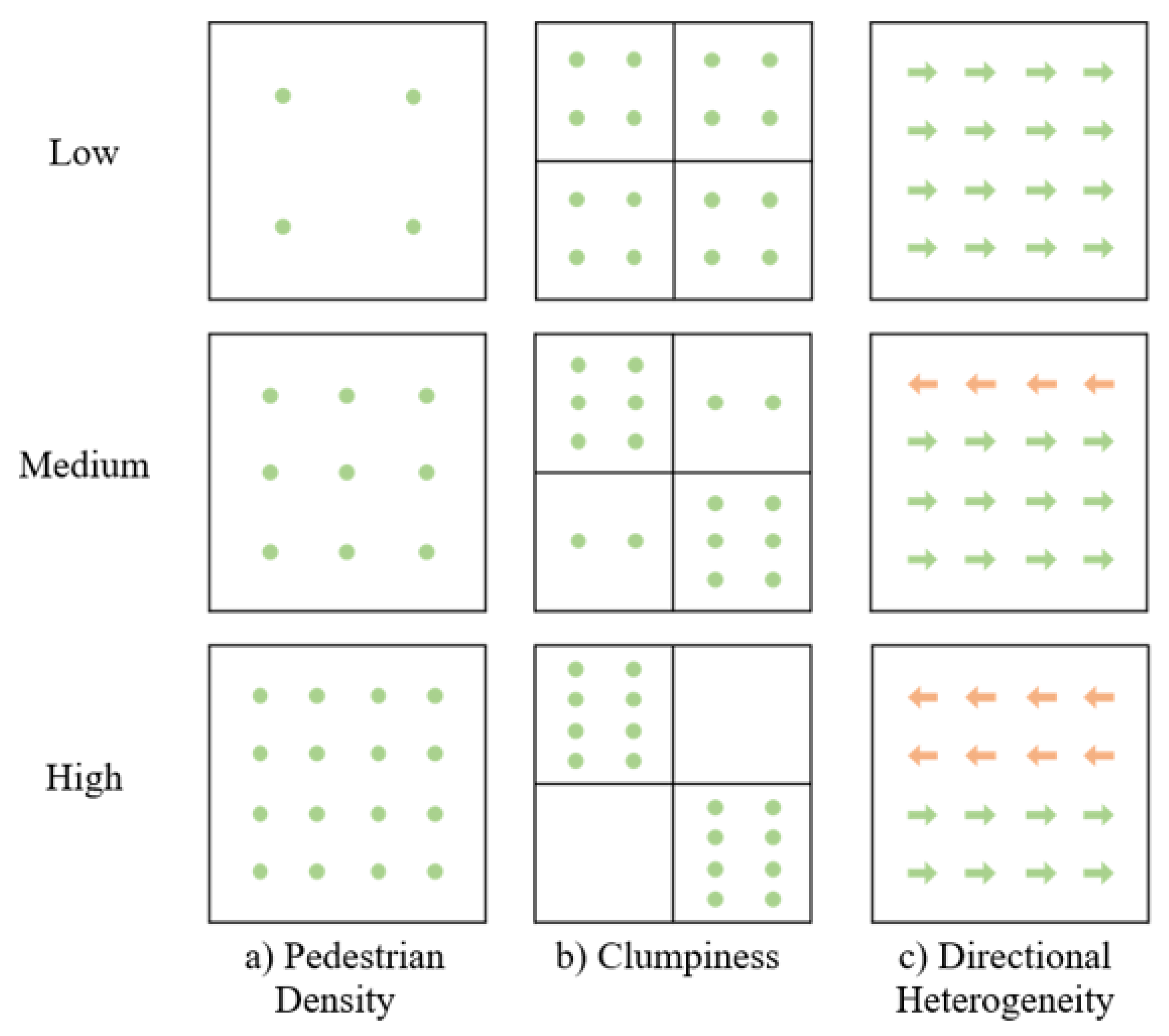
The study used three explanatory variables: pedestrian density, clumpiness, and directional heterogeneity. Figure 1 illustrates the concepts underlying the three variables. These three variables were expected to explain changes in and were designed to estimate the without needing to measure the varying distances between pedestrians in a study area over time.
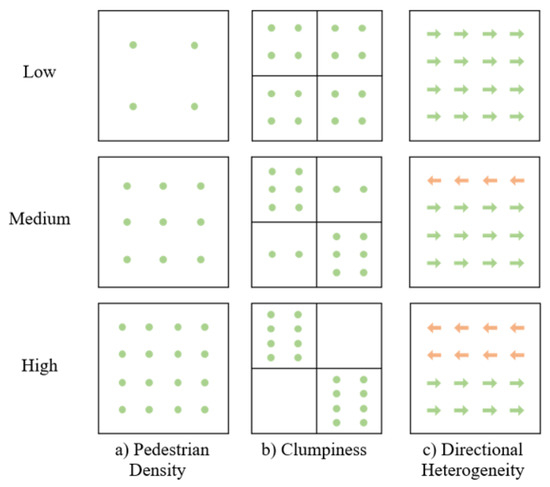
Figure 1.
The concepts underlying the three explanatory variables. Each dot or arrow represents a pedestrian.
Figure 1a shows three different levels of pedestrian density (low, medium and high), and Equation (7) shows how we quantitatively estimated the density (persons/) of a study area. As pedestrian density increases, social distancing decreases.
where n is the number of pedestrians, and A is the study area ().
Figure 1b demonstrates different levels of clumpiness for the same level of pedestrian density. The figure clearly indicates that social distancing between people can vary even under the same level of pedestrian density. Equation (8) was used to measure the varying levels of clumpiness in a study area. The equation is a variance-to-mean ratio (VMR).
where and is the variance of the number of pedestrians among sub-areas.
In general, as clumpiness increases, the VMR increases. High Clumpiness in Figure 1b provides an example. As clumpiness decreases, the VMR value approaches 0 and pedestrians become evenly spread in the area. Low Clumpiness in Figure 1b provides an example.
Figure 1c illustrates different types of directional heterogeneity. Directional heterogeneity might have an effect on social distancing over time, as it is reasonable to expect that social distancing becomes more difficult as a higher number of pedestrians are walking towards each other. As a result, the City of New York and the Government of Canada, for example, encouraged unidirectional pedestrian travel on narrow walkway spaces [42,43].
Equation (9) illustrates how we can estimate the directional heterogeneity (DH) of pedestrian flows in a study area. DH ranges from 0 (completely uniform unidirectional pedestrian flow) to 0.5 (evenly distributed bidirectional pedestrian flow).
The relationship between the response variable () and the three explanatory variables was established using multiple linear regression.
2.3. Conducting the Pedestrian Simulations
To generate data (i.e., the response and explanatory variables) for our statistical model, we conducted a set of pedestrian simulations. We considered changing pedestrian flow conditions to obtain a wide spectrum for the and the three explanatory variables. We used PTV Viswalk, a popular pedestrian simulation tool in transportation engineering [44], to track pedestrian walking trajectories (i.e., x-y coordinate of pedestrians in a study area) over time. Pedestrian simulations have been widely used in many empirical studies to understand pedestrian flows for various study purposes [45].
PTV Viswalk relies on a social force model (SFM) [44] that simulates the movement of pedestrians in a space by mimicking the movement of magnetized objects in a magnetic field [46]. The model uses the concept of positive and negative magnetic poles to explain pedestrian movements in the sense that pedestrians are moving towards a destination that represents an attractive force (often represented as the negative magnetic pole) while avoiding collisions with other pedestrians and/or other physical obstacles (often represented as the positive magnetic pole). Helbing and Molnar (1995) provide an in-depth discussion of the SFM [47].
To simulate pedestrian flows on urban streets, we created a 20 m by 3 m virtual pedestrian walkway to represent a typical urban sidewalk in a downtown area. The distance between pedestrians is directly associated with pedestrian volume in an area. We simulated a range of pedestrian flows from 15 to 75 persons/minute/meter. These flows cover pedestrian levels of service A (free flow) to E (capacity) as defined in the U.S. Highway Capacity Manual (HCM) [48]. We gradually increased the pedestrian flows, and at the same time, set all pedestrians to appear at random time intervals to create various pedestrian flow conditions. We simulated three scenarios for directional pedestrian flow: (1) 100% unidirectional pedestrian movement, (2) 80%/20% split bi-directional pedestrian movement, and (3) 60%/40% split bi-directional pedestrian movement. We simulated each scenario twice for 130 min per simulation.
We extracted the x-y coordinates and the speed for each pedestrian’s second-by-second movement along the created virtual street for the 130 min of the simulations. This provides a 7800 (=60 s × 130 min) dataset that includes all pedestrians’ x-y position and speed information per second per scenario, and produced a total of 46,800 (=7800 × 3 scenarios × 2 times) datasets from all scenarios. The raw data were converted into the response and explanatory variables (see Equations (4) and (7)–(9)) and used to develop the statistical model. In the case of the clumpiness variable (Equation (8)), we used 10 sub-areas.
3. Results
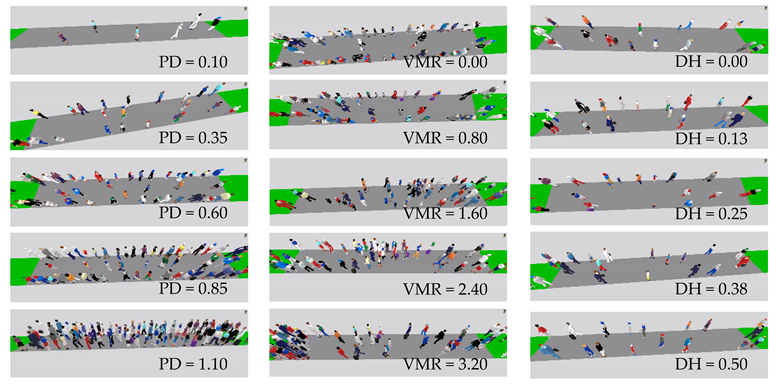
The simulation data were used to estimate the (i.e., to represent the relative exposure to viral infection for pedestrians on a walkway). The number of observations used in the statistical modelling was reduced from 46,800 to 45,664 after removing datasets that were biased in terms of pedestrian speed due to overcapacity situations in the simulation. Table 1 includes the descriptive statistics for the response and explanatory variables used in the statistical model and also provides simulation screens indicating how the values of pedestrian density, clumpiness, and directional heterogeneity appear in the simulation space.

Table 1.
Descriptive statistics for the response and explanatory variables.
3.1. Social Distancing Indicator
The of our virtual street varied from 0.00 to 6.49. If there were very few people on the street, we might expect minimum exposure to viral infection between pedestrians. In this case, the was set as zero. If all the pedestrians moved in one direction at uniform intervals while maintaining a minimum distance of 2 m from each other, the estimated value of was very close to 1. If pedestrians were moving in one direction 1 m distance (instead of 2 m) apart, the estimated value of was greater than 4. When it comes to pedestrian density, the data covered situations where 1 (pedestrian density of 0.017) to 74 (pedestrian density of 1.233) pedestrians existed on the virtual street.
3.2. Statistical Model
Table 2 provides the results of the statistical model. No statistically significant correlation was found between explanatory variables (low VIF values). All three explanatory variables had a statistically significant relationship with the social distancing indicator, . The results can be described as Equation (10):
where is the intercept and are the coefficients of explanatory variables.
Table 2.
Results of the statistical model.
The model explains that the potential exposure to viral infection, as measured by the , increases with increased pedestrian density, increased clumpiness, and increased directional heterogeneity. If the estimated was lower than 0, it was regarded as 0.
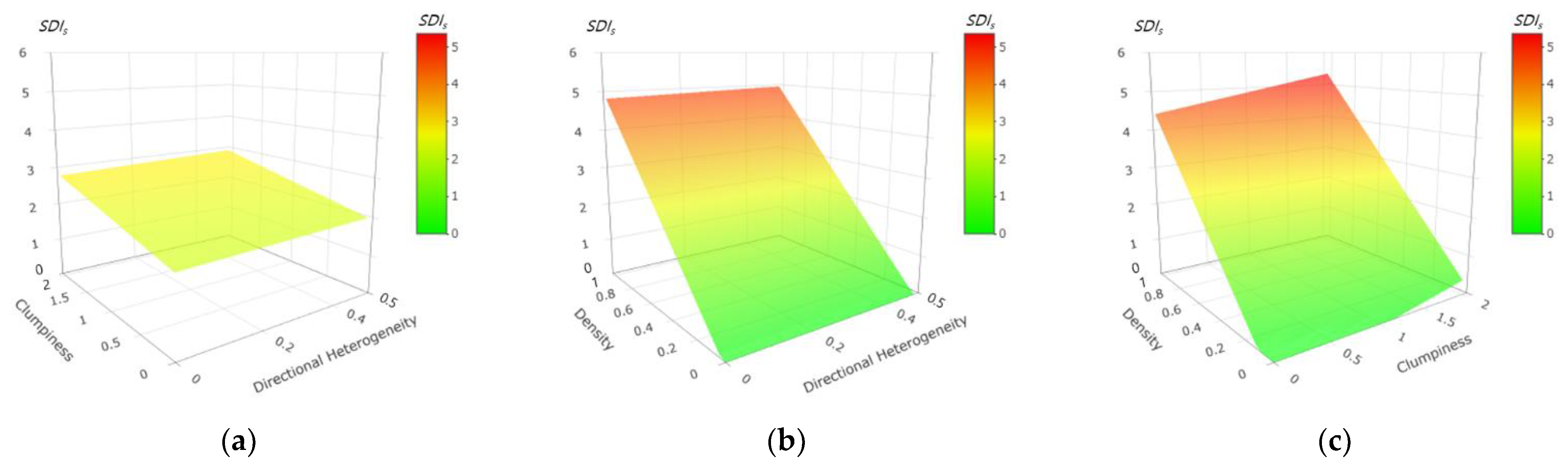
Figure 2 illustrates the results of the statistical model as 3D-surface plots. Green indicates a low exposure (low ), and red indicates a high exposure (high ). We found that pedestrian density (PD) had more influence on than did clumpiness (VMR) or directional heterogeneity (DH). For instance, Figure 2a demonstrates that if the PD value was fixed as 0.50, the value of did not change significantly (from 1.88 to 2.93) even when the VMR and/or DH changed significantly. However, Figure 2b,c indicate that if the VMR and DH values were fixed, the value of changed greatly. If the VMR value was fixed as 1.00, the value of changed from 0.00 to 4.96 when the PD and/or DH changed significantly. Similarly, if the DH value was fixed as 0.25, the value of changed from 0.00 to 5.35 when the PD and/or VMR changed significantly.
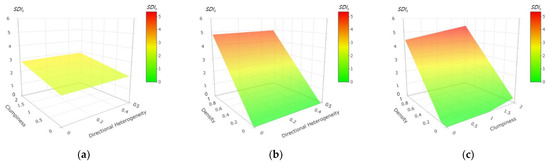
Figure 2.
3D-surface plots demonstrating the results of statistical model. (a) Pedestrian Density = 0.50. (b) Clumpiness = 1.00. (c) Directional Heterogeneity = 0.25.
4. Discussions and Conclusions
This study has proposed a social distancing indicator, the , designed to estimate the potential exposure to COVID-19 infection for pedestrians on an urban street. This indicator can also be used in any future infectious diseases caused by airborne transmission. As mentioned, the proposed SDI does not represent an absolute risk of viral infection between people and it can be interpreted as an index to present relative risk between areas with varying pedestrian flows. The proposed indicator can be used to:
- compare the different levels of social distancing found on different urban streets,
- assess changes in social distancing occurring with or without mobility interventions on a street, and
- monitor progress towards a jurisdiction’s specific social distancing goal, for example an of less than 1 (i.e., value when all pedestrians maintain 2 m distance from each other) for an urban street.
Furthermore, the results of our statistical model suggest some important public health policy issues related to various social distancing interventions.
- To secure proper social distancing along an urban street, controlling pedestrian density should be the first priority. Pedestrian density can be lowered by discouraging pedestrian use of a street or by expanding the walking space. Pedestrian density might be lowered, for example, by suspension of facility operation or facility entrance management connected with sidewalks, and pedestrian walkway closure. Additional walking space can be temporarily provided by, for example, converting roadside street parking or even shoulder-side lanes to pedestrian walking space.
- Lowering the level of pedestrian clumpiness can also be effective for increasing social distancing between pedestrians on urban streets. Health agencies can, for example, introduce educational interventions such as campaigns and/or signage showing social distancing regulations, as well as consider police enforcement in serious situations.
- Lowering the degree of pedestrian directional heterogeneity can have some impact on increasing social distancing. Health agencies can, for example, designate one-way pedestrian walkways and/or separation of counter pedestrian flows.
We think future studies should answer some important and unresolved questions in this study.
- Future study needs to consider other factors that affect the chance of contracting a virus. The actual chance of contracting COVID-19 (or any airborne transmission of respiratory viruses) varies with many factors that we were unable to consider in this study. The factors include temperature, humidity, strength and direction of wind, etc. However, we consider this issue to be outside the scope of this particular study.
- Future study needs to develop a similar model to measure the relative exposure to viral infection between pedestrians in indoor spaces (e.g., corridors in large shopping malls/plaza or major transportation facilities such as airport or railway stations). Indoor spaces could have additional challenges compared with outdoor spaces since they potentially have other important factors to be considered (e.g., type of building ventilation such as wind-driven ventilation; pressure-driven flows).
- Future study needs to consider pedestrians’ mask wearing effect more explicitly. Liang et al. (2020) analyzed the efficacy of mask wearing in preventing respiratory virus transmission based on a systematic literature review and meta-analysis [41]. They reported that non-health care workers can reduce virus transmission by 47% by wearing masks, although the effectiveness may vary according to other conditions such as mask type and region. A straightforward approach to reflect the mask wearing effect could be simply multiplying a factor value (e.g., 0.53 if we use the Liang et al.’s study finding) to the estimated SDI.
- Future study needs to validate the accuracy and usefulness of the proposed statistical model by using real movement data for pedestrians. To collect the data, a computer vision-based detection technology could be a useful tool for measuring and monitoring positioning data (x-y coordinates) for pedestrians moving on the target sidewalks. The pedestrians’ positioning data could then be used to estimate the three explanatory variables (pedestrian density, clumpiness, and directional heterogeneity) and validate the proposed statistical model.
In conclusion, we think this study will be useful to health agencies responding to the challenges involved in managing the spread of a pandemic among pedestrians using urban streets, as the proposed in this study can be used to monitor the degree of social distancing on urban streets. Monitoring the on urban streets can provide important raw data for a city planning more resilient future streets designed to minimize the adverse impact of a current or future pandemic caused by airborne transmission. The study’s statistical modeling can be used to demonstrate the potential effectiveness of various mobility interventions for designing future urban streets with consideration for public health.
Author Contributions
Conceptualization, S.Y. and P.Y.P.; methodology, S.Y. and P.Y.P.; software, T.U.C., S.Y. and A.M.; validation, S.Y. and P.Y.P.; formal analysis, S.Y.; resources, T.U.C.; data curation, T.U.C. and A.M.; writing—original draft preparation, S.Y. and T.U.C.; writing—review and editing, S.Y. and P.Y.P.; visualization, T.U.C. and S.Y.; supervision, P.Y.P.; project administration, P.Y.P.; funding acquisition, P.Y.P. and S.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Natural Sciences and Engineering Research Council of Canada and Hanbat National University.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bruin, Y.; Lequarre, A.; McCourt, J.; Clevestig, P.; Pigazzani, F.; Zare Jeddi, M.; Colosio, C.; Goulart, M. Initial impacts of global risk mitigation measures taken during the combatting of the COVID-19 pandemic. Saf. Sci. 2020, 128, 104773. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Social Distancing. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html (accessed on 7 July 2020).
- Toussaint, L.; Cheadle, A.; Fox, J.; Williams, D. Clean and contain: Initial development of a measure of infection prevention behaviors during the COVID-19 pandemic. Ann. Behav. Med. 2020, 54, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Moeckel, R.; Moreno, A.; Shuai, B.; Gao, J. A work-life conflict perspective on telework. Transp. Res. Part A Policy Pract. 2020, 141, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Azimian, A. Exploring the factors affecting travel behaviors during the second phase of the COVID-19 pandemic in the United States. Transp. Lett. 2021, 13, 331–343. [Google Scholar] [CrossRef]
- Yao, W.; Yu, J.; Yang, Y.; Chen, N.; Jin, S.; Hu, Y.; Bai, C. Understanding travel behavior adjustment under COVID-19. Commun. Transp. Res. 2022, 2, 100068. [Google Scholar] [CrossRef]
- Murakami, M.; Yasutaka, T.; Onishi, M.; Naito, W.; Shinohara, N.; Okuda, T.; Fujii, K.; Katayama, K.; Imoto, S. Living with COVID-19: Mass gatherings and minimizing risk. QJM-Int. J. Med. 2021, 114, 437–439. [Google Scholar] [CrossRef]
- Sheer, B.; Russell, N. Living with COVID-19: Voices from the grassroots. J. Am. Assoc. Nurse Pract. 2021, 33, 416–418. [Google Scholar] [CrossRef]
- Uysal, B.; Görmez, V.; Eren, S.; Morgül, E.; Öcal, N.B.; Karatepe, H.T.; Yanık, M. Living with COVID-19: Depression, anxiety and life satisfaction during the new normal in Turkey. J. Cogn. Psychother. 2021, 10, 257. [Google Scholar] [CrossRef]
- Kamelifar, M.J.; Ranjbarnia, B.; Masoumi, H. The determinants of walking behavior before and during COVID-19 in Middle-East and North Africa: Evidence from Tabriz, Iran. Sustainability 2022, 14, 3923. [Google Scholar] [CrossRef]
- Transform Transport. How COVID-19 Is Affecting Pedestrian Modelling. 2020. Available online: https://research.systematica.net/journal/how-covid-19-is-affecting-pedestrian-modelling/ (accessed on 7 July 2020).
- Johansson, M.; Hartig, T.; Staats, H. Psychological benefits of walking: Moderation by company and outdoor environment. Appl. Psychol. Health Well-Being 2011, 3, 261–280. [Google Scholar] [CrossRef]
- Roe, J.; Aspinall, P. The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place 2011, 17, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Robertson, R.; Robertson, A.; Jepson, R.; Maxwell, M. Walking for depression or depressive symptoms: A systematic review and meta-analysis. Ment. Health Phys. Act. 2012, 5, 66–75. [Google Scholar] [CrossRef]
- Bornioli, A.; Parkhurst, G.; Morgan, P. Affective experiences of built environments and the promotion of urban walking. Transp. Res. Part A Policy Pract. 2019, 123, 200–215. [Google Scholar] [CrossRef]
- Lyons, G. Walking as a service—Does it have legs? Transp. Res. Part A Policy Pract. 2020, 137, 271–284. [Google Scholar] [CrossRef]
- Wen, L.; Marinova, D.; Kenworthy, J.; Guo, X. Street recovery in the age of COVID-19: Simultaneous design for mobility, customer traffic and physical distancing. Sustainability 2022, 14, 3653. [Google Scholar] [CrossRef]
- National Association of City Transportation Officials. Streets for Pandemic Response & Recovery. 2020. Available online: https://nacto.org/wp-content/uploads/2020/05/NACTO_Streets-for-Pandemic-Response-and-Recovery_2020-05-21.pdf (accessed on 7 July 2020).
- Hassan, A.M.; Megahed, N.A. COVID-19 and urban spaces: A new integrated CFD approach for public health opportunities. Build. Environ. 2021, 204, 108131. [Google Scholar] [CrossRef]
- Bourassa, K.; Sbarra, D.; Caspi, A.; Moffitt, T. Social distancing as a health behavior: County-level movement in the United States during the COVID-19 pandemic is associated with conventional health behaviors. Ann. Behav. Med. 2020, 54, 548–556. [Google Scholar] [CrossRef]
- Hagger, M.; Smith, S.; Keech, J.; Moyers, S.; Hamilton, K. Predicting social distancing intention and behavior during the COVID-19 pandemic: An integrated social cognition model. Ann. Behav. Med. 2020, 54, 713–727. [Google Scholar] [CrossRef]
- Hong, B.; Bonczak, B.J.; Gupta, A.; Thorpe, L.E.; Kontokosta, C.E. Exposure density and neighborhood disparities in COVID-19 infection risk. Proc. Natl. Acad. Sci. USA 2021, 118, e2021258118. [Google Scholar] [CrossRef]
- Jiao, J.; Bhat, M.; Azimian, A. Measuring travel behavior in Houston, Texas with mobility data during the 2020 COVID-19 outbreak. Transp. Lett. 2021, 13, 461–472. [Google Scholar] [CrossRef]
- Mohammadi, A.; Chowdhury, T.U.; Yang, S.; Park, P.Y. Developing levels of pedestrian physical distancing during a pandemic. Saf. Sci. 2021, 134, 105066. [Google Scholar] [CrossRef]
- Maragakis, L.L. Coronavirus, Social and Physical Distancing and Self-Quarantine. 2020. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-social-distancing-and-self-quarantine (accessed on 29 August 2020).
- New York Post. De Blasio Calls Off Coronavirus Street Closures, Citing Lack of NYPD Resources. 2020. Available online: https://nypost.com/2020/04/06/coronavirus-in-ny-de-blasio-calls-off-street-closures/ (accessed on 7 July 2020).
- Miller, M. This Is What One-Way Sidewalks Could Look like in Toronto. 2020. Available online: https://www.blogto.com/city/2020/04/what-one-way-sidewalks-could-look-toronto/ (accessed on 7 July 2020).
- Portland Bureau of Transportation. Safe Streets: Adapting Portland’s Streets for Restarting Public Life. 2020. Available online: https://www.portland.gov/sites/default/files/2020-05/safe-streetspublicreview-draft052020a.pdf (accessed on 7 July 2020).
- Federation of Canadian Municipalities. COVID-19 Street Rebalancing Guide. 2020. Available online: https://data.fcm.ca/documents/COVID-19/COVID-19-Street-Rebalancing-Guide-EN.pdf (accessed on 7 July 2020).
- Vancouver Public Space Network. COVID-19 Response—Creating Safe & Open Streets in Vancouver. 2020. Available online: http://vancouverpublicspace.ca/2020/03/27/covid-19-response-creating-safe-open-streets-in-vancouver/ (accessed on 7 July 2020).
- San Francisco Municipal Transportation Agency. Slow Streets Program to Help with Social Distancing. 2020. Available online: https://www.sfmta.com/blog/slow-streets-program-help-social-distancing (accessed on 7 July 2020).
- City of Toronto. COVID-19: ActiveTO. 2020. Available online: https://www.toronto.ca/home/covid-19/covid-19-protect-yourself-others/covid-19-reduce-virus-spread/covid-19-activeto/ (accessed on 29 August 2020).
- City News. Police to Start ‘Zero Tolerance’ Social Distancing Enforcement. 2020. Available online: https://toronto.citynews.ca/2020/04/11/mayor-tory-calls-on-police-bylaw-officers-to-issue-more-tickets/ (accessed on 7 July 2020).
- The Hill. Cuomo Says NYPD Needs to Enforce Social Distancing Rules. 2020. Available online: https://thehill.com/homenews/state-watch/490623-cuomo-says-nypd-needs-to-enforce-social-distancing-rules (accessed on 7 July 2020).
- BBC. Coronavirus: Could Social Distancing of Less Than Two Metres Work? 2020. Available online: https://www.bbc.com/news/science-environment-52522460 (accessed on 7 July 2020).
- Feng, Y.; Marchal, T.; Sperry, T.; Yi, H. Influence of wind and relative humidity on the social distancing effectiveness to prevent COVID-19 airborne transmission: A numerical study. J. Aerosol Sci. 2020, 147, 105585. [Google Scholar] [CrossRef] [PubMed]
- Blocken, B.; Malizia, F.; van Druenen, T.; Marchal, T. Towards Aerodynamically Equivalent COVID-19 1.5 m Social Distancing for Walking and Running. 2020. Available online: http://www.urbanphysics.net/COVID19_Aero_Paper.pdf (accessed on 7 July 2020).
- Bourouiba, L. Turbulent gas clouds and respiratory pathogen emissions. JAMA 2020, 323, 1837–1838. [Google Scholar] [CrossRef] [PubMed]
- Porter, B. Amazon Introduces ‘Distance Assistant’. 2020. Available online: https://blog.aboutamazon.com/operations/amazon-introduces-distance-assistant?utm_source=social (accessed on 7 July 2020).
- Chu, D.; Akl, E.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; COVID-19 Systematic Urgent Review Group Effort (SURGE). Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Liang, M.; Gao, L.; Cheng, C.; Zhou, Q.; Uy, J.; Heiner, K.; Sun, C. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 36, 101751. [Google Scholar] [CrossRef]
- Government of Canada. Risk Mitigation Tool for Workplaces/Businesses Operating during the COVID-19 Pandemic. 2020. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/risk-informed-decision-making-workplaces-businesses-covid-19-pandemic.html (accessed on 7 July 2020).
- New York Post. New Yorkers Ignore ‘One Way’ Instructions on Lower Manhattan Sidewalks. 2020. Available online: https://nypost.com/2020/06/30/new-yorkers-ignore-one-way-instructions-on-sidewalks/ (accessed on 7 July 2020).
- PTV. PTV Vissim 2020 User Manual; PTV: Karlsruhe, Germany, 2020. [Google Scholar]
- Kim, I.; Galiza, R.; Ferreira, L. Modeling pedestrian queuing using micro-simulation. Transp. Res. Part A Policy Pract. 2013, 49, 232–240. [Google Scholar] [CrossRef]
- Okazaki, S.; Matsushita, S. A study of simulation model for pedestrian movement with evacuation and queuing. In Proceedings of the International Conference on Engineering for Crowd Safety, London, UK, 18 March 1993. [Google Scholar]
- Helbing, D.; Molnár, P. Social force model for pedestrian dynamics. Phys. Rev. E 1995, 51, 4282–4286. [Google Scholar] [CrossRef] [Green Version]
- Transportation Research Board. Highway Capacity Manual; Transportation Research Board: Washington, DC, USA, 2020. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).