
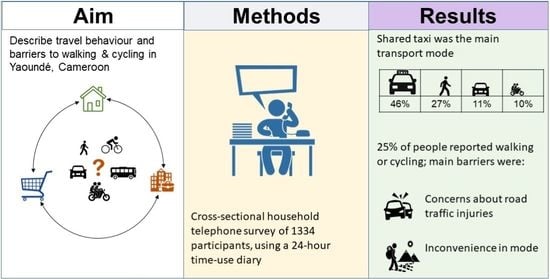
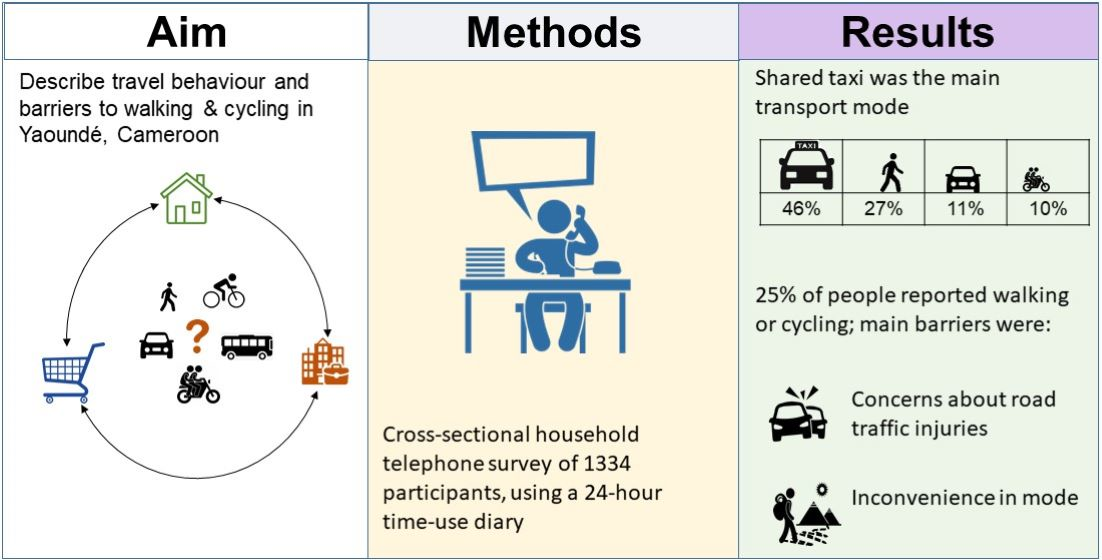
Travel Behaviour and Barriers to Active Travel among Adults in Yaoundé, Cameroon

 , , , , ,
, , , , ,
Abstract
:
1. Introduction
2. Literature on Travel Behaviour in Africa
3. Materials and Methods
3.1. Study Design
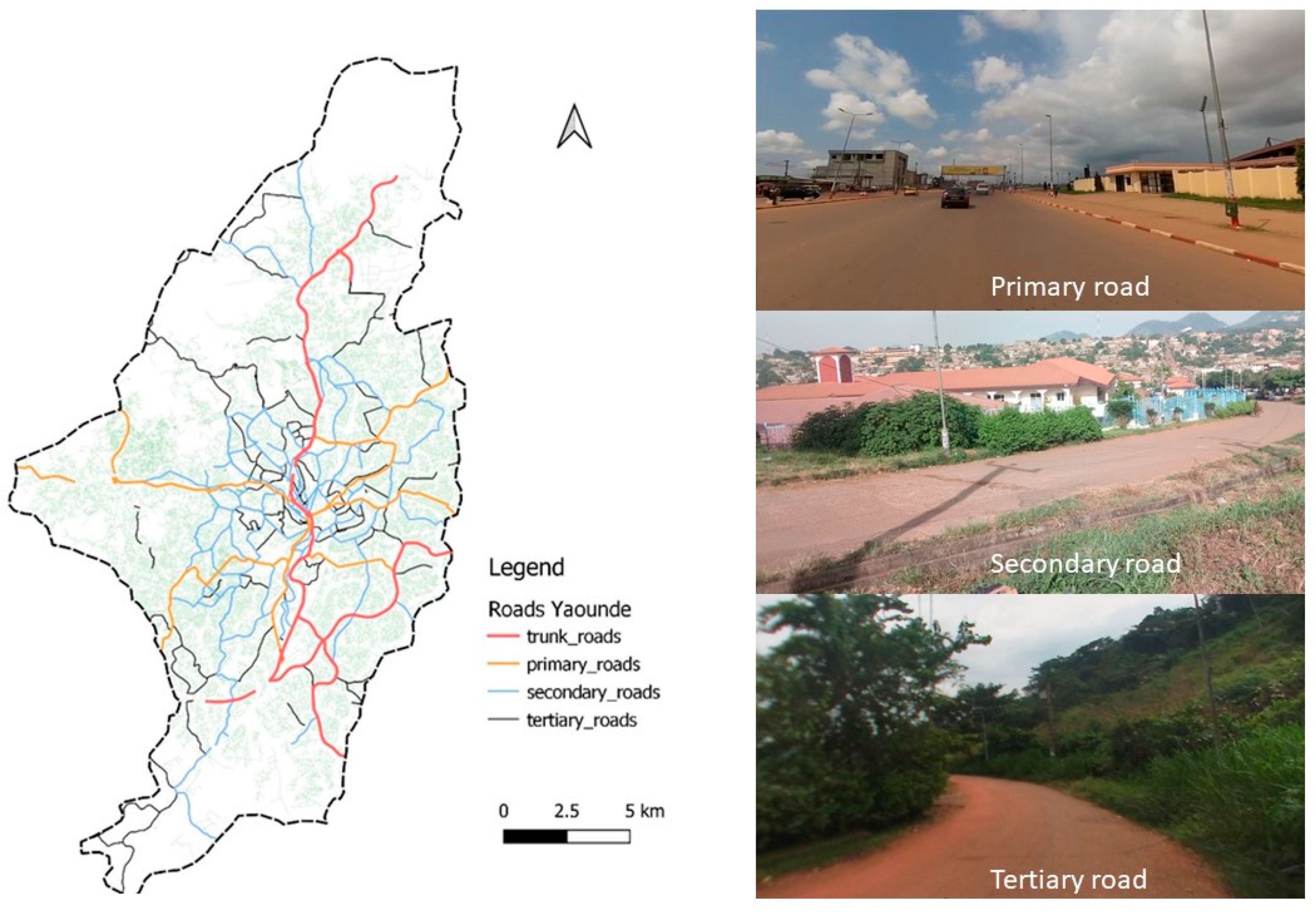
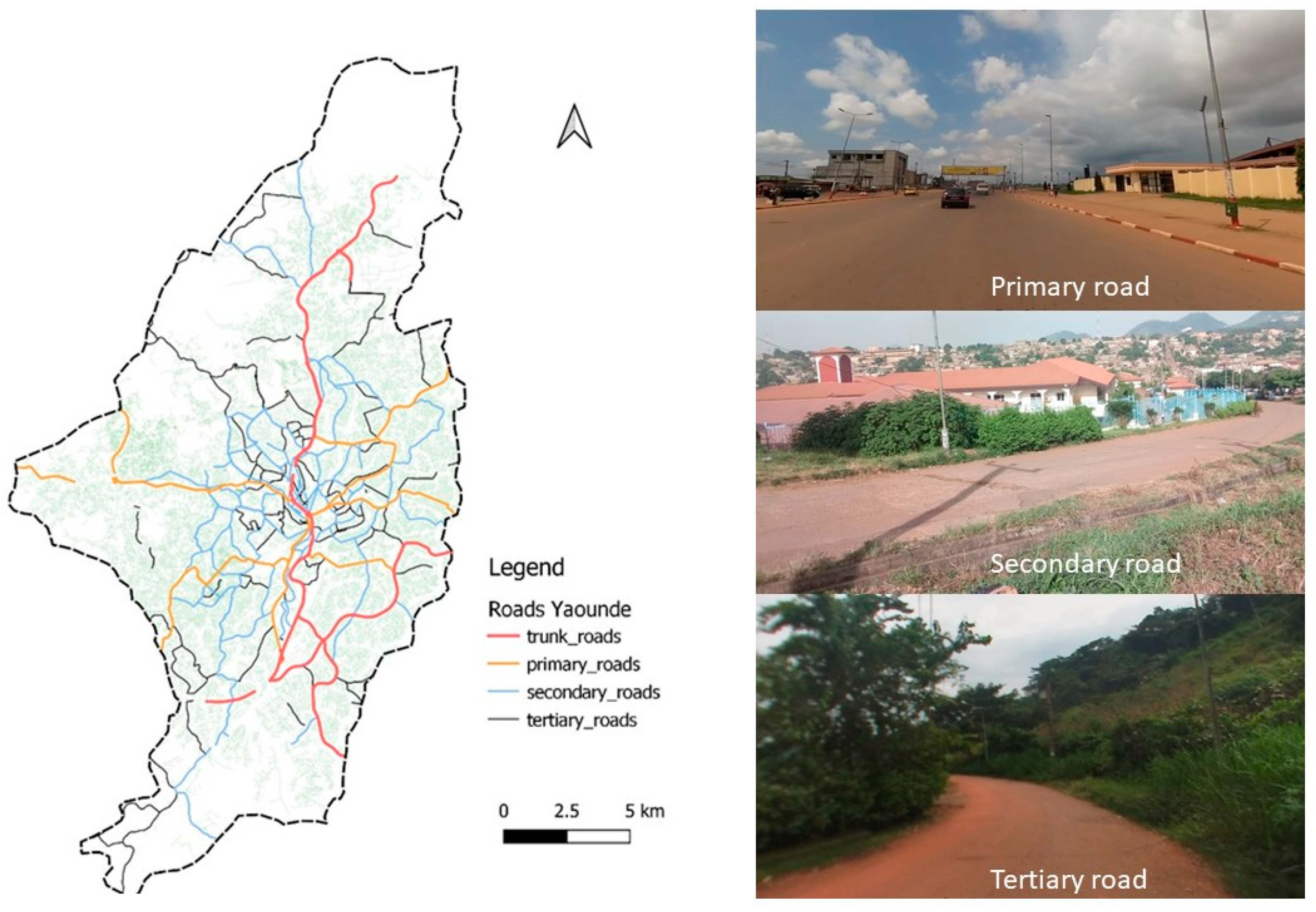
3.2. Setting
3.3. Participants
3.4. Sampling
3.5. Data Collection
3.6. Survey Instruments
3.7. Variables
3.7.1. Household Variables
3.7.2. Individual Variables
3.7.3. Trip Characteristics
3.7.4. Individual Travel Behaviour
3.7.5. Barriers to Active Travel
3.8. Statistical Analysis
4. Results
4.1. Characteristics of Survey Households and Participants
4.2. Trip Characteristics
4.3. Individual Travel Behaviour
4.3.1. Number of Trips
4.3.2. Use of Active, Motorised, and Public Transport Modes
4.3.3. Overall Travel Duration and Duration in Active, Motorised, and Public Transport
4.4. Barriers to Active Travel
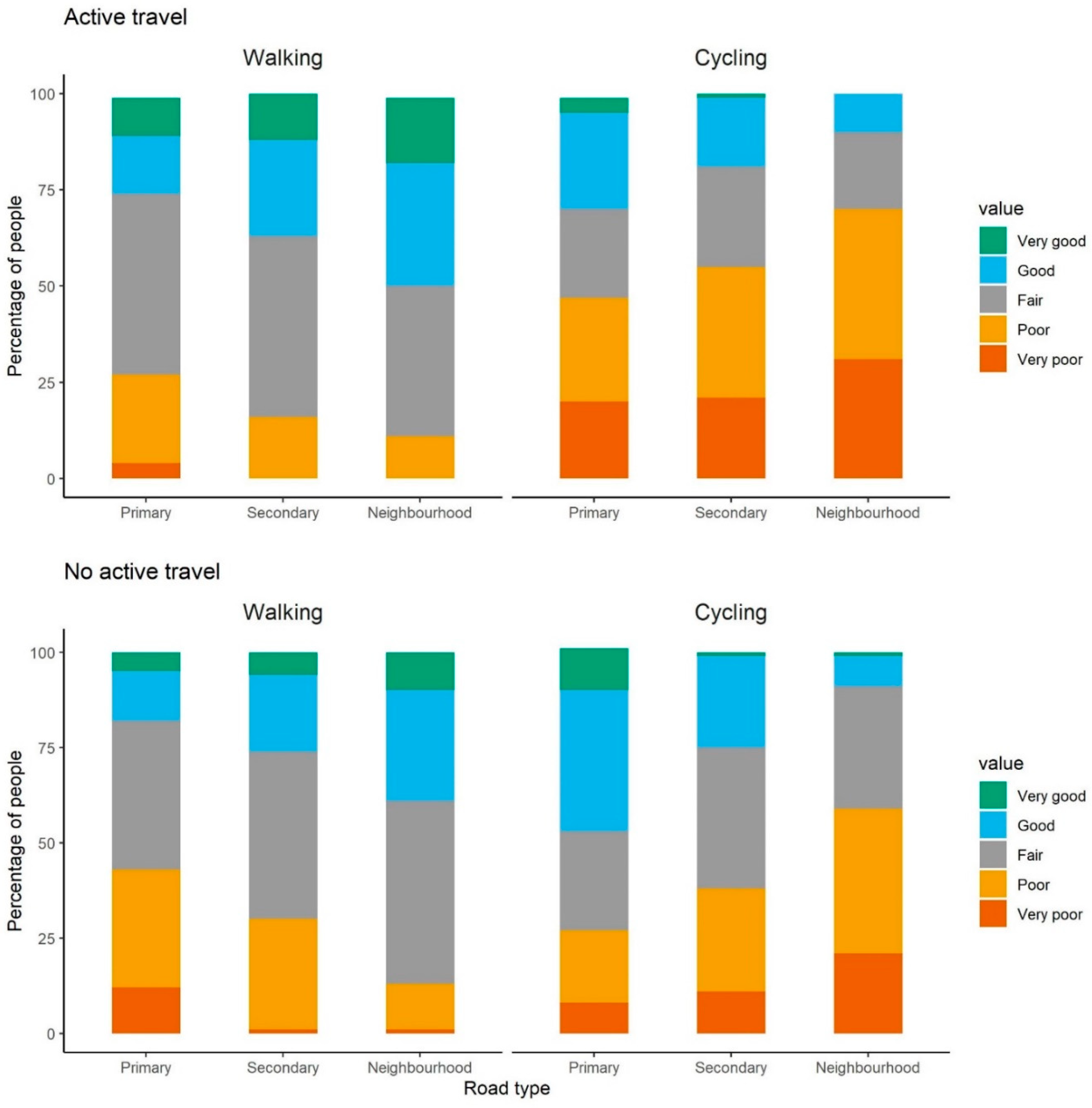
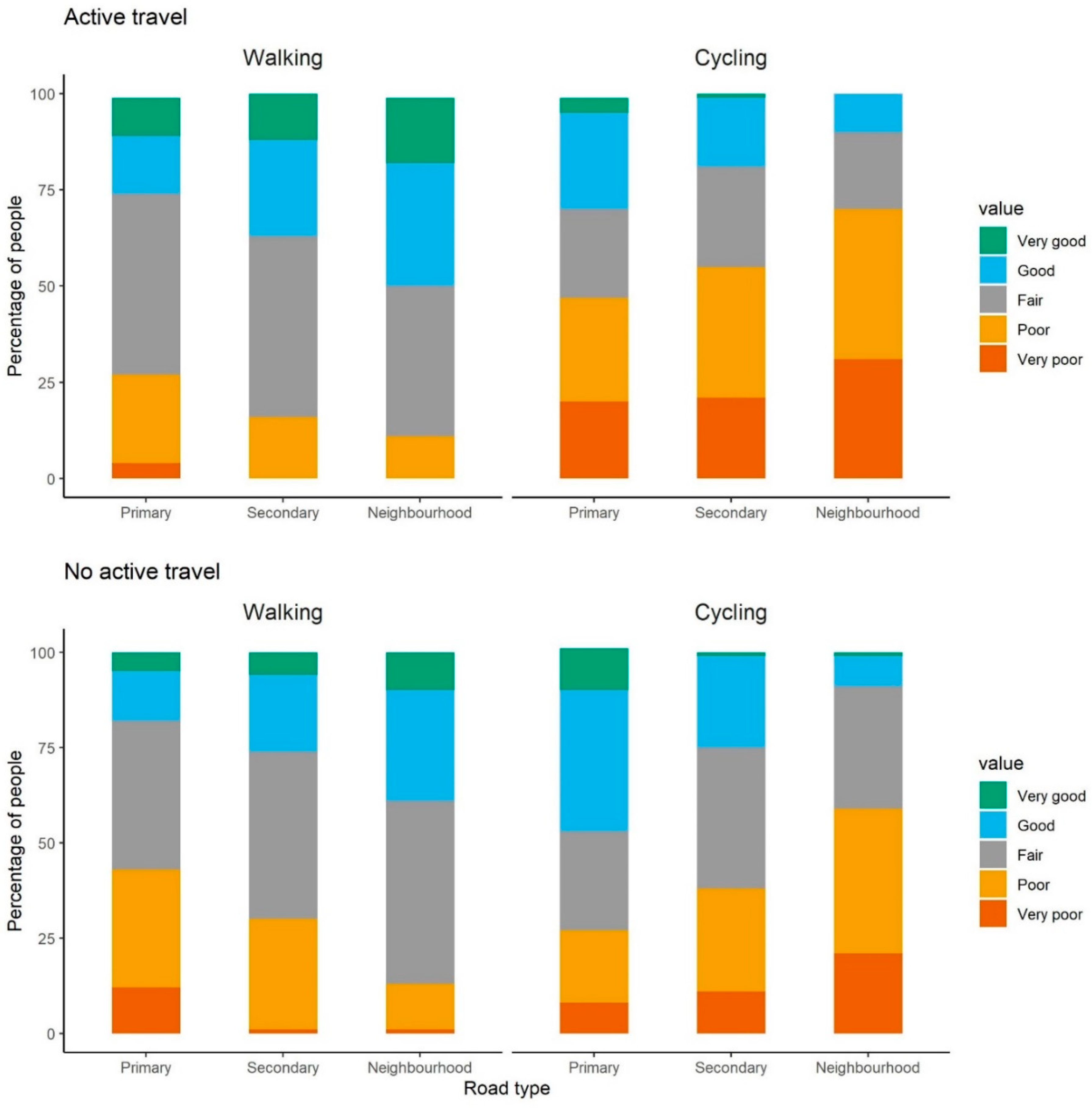
4.4.1. Perception of Active Travel Infrastructure
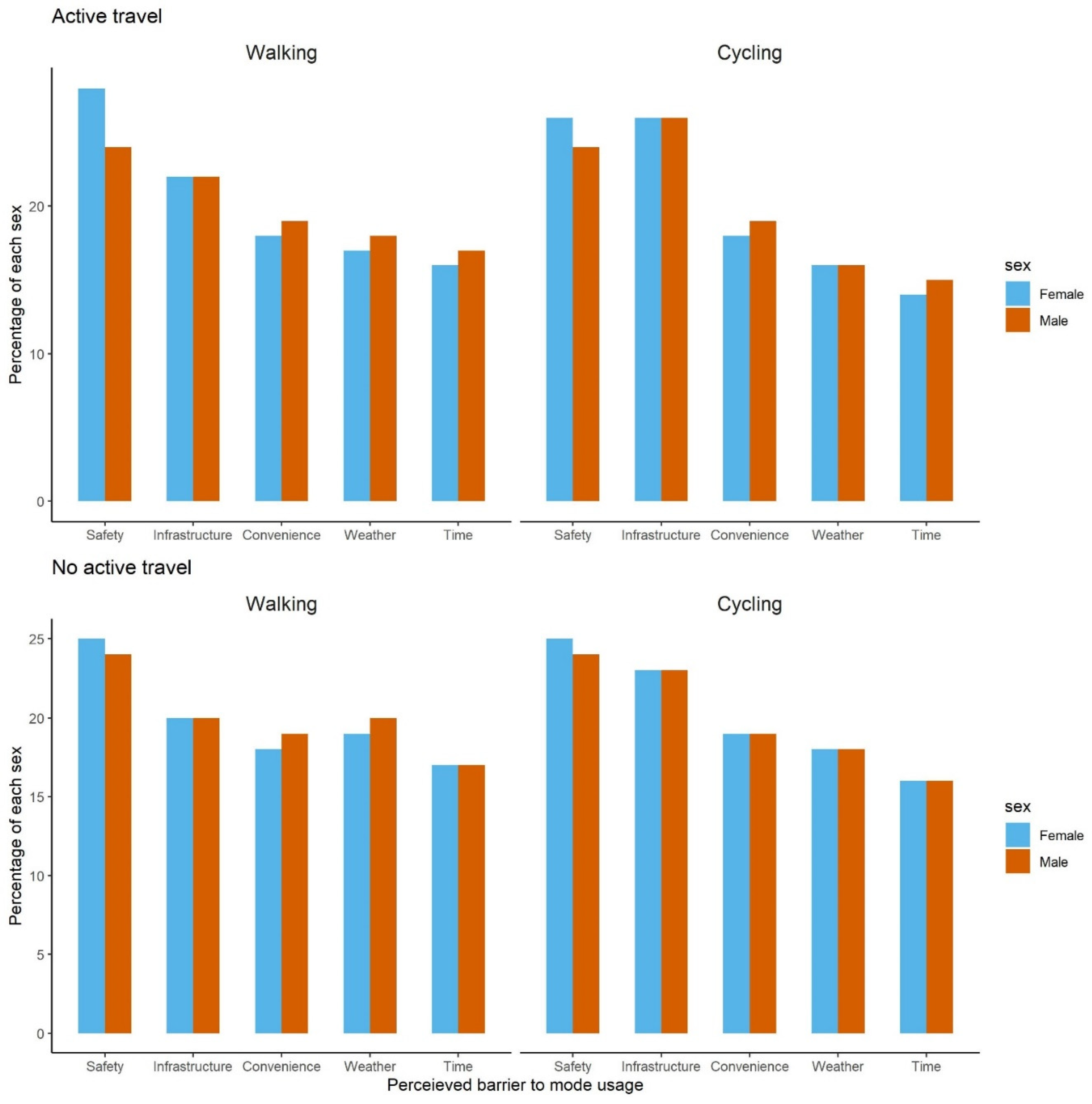
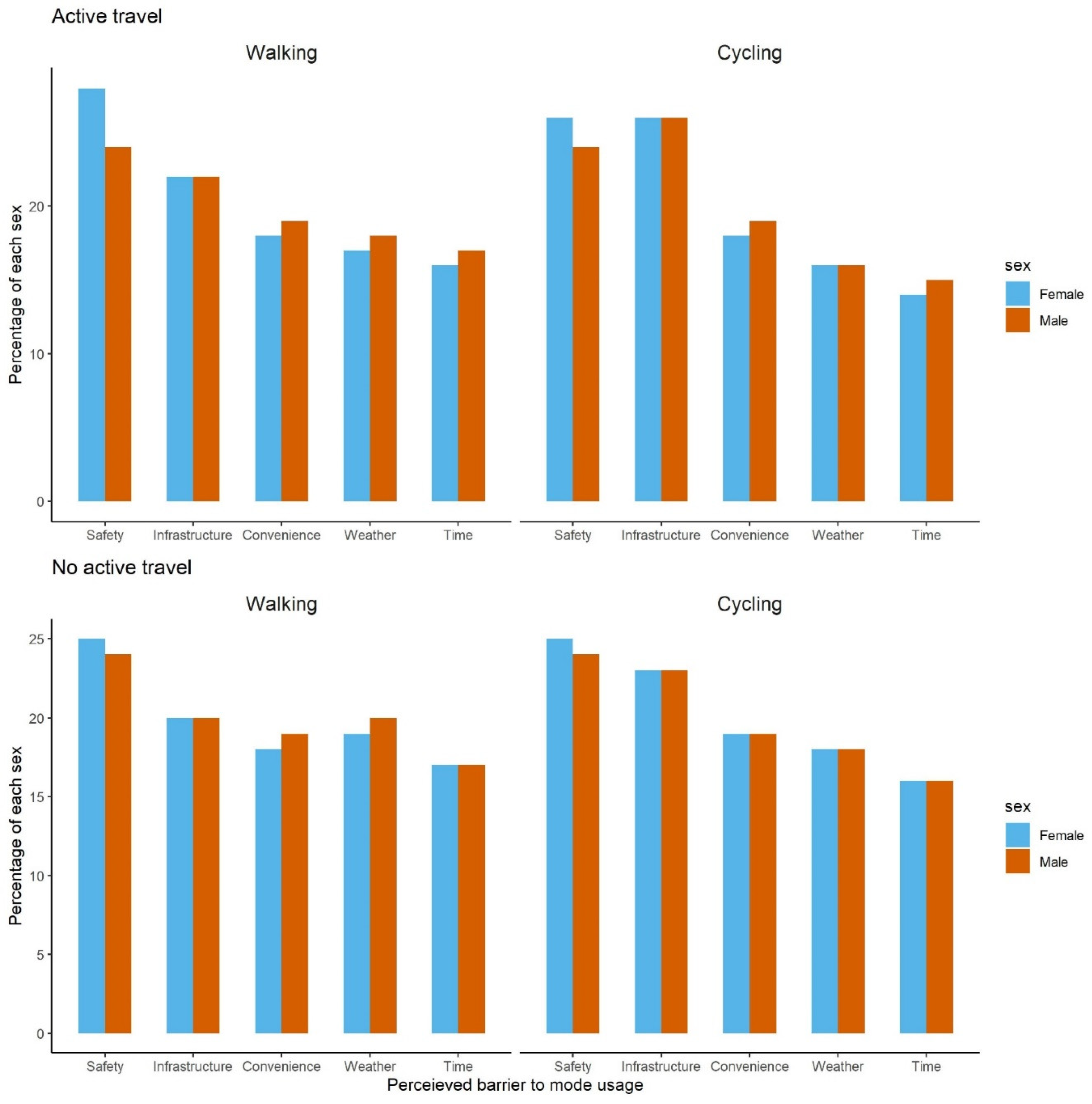
4.4.2. Perception of Key Barriers to Active Travel
5. Discussion
5.1. Summary of Findings
5.2. Study Limitations
5.3. Interpretation of Findings
5.4. COVID-19 and the Future of Urban Mobility in Africa
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foley, L.; Brugulat-Panés, A.; Woodcock, J.; Govia, I.; Hambleton, I.; Turner-Moss, E.; Mogo, E.R.I.; Awinja, A.C.; Dambisya, P.M.; Matina, S.S.; et al. Socioeconomic and Gendered Inequities in Travel Behaviour in Africa: Mixed-Method Systematic Review and Meta-Ethnography. Soc. Sci. Med. 2021, 292, 114545. [Google Scholar] [CrossRef] [PubMed]
- Glazener, A.; Sanchez, K.; Ramani, T.; Zietsman, J.; Nieuwenhuijsen, M.J.; Mindell, J.S.; Fox, M.; Khreis, H. Fourteen Pathways between Urban Transportation and Health: A Conceptual Model and Literature Review. J. Transp. Health 2021, 21, 101070. [Google Scholar] [CrossRef]
- Hamilton, I.; Kennard, H.; McGushin, A.; Höglund-Isaksson, L.; Kiesewetter, G.; Lott, M.; Milner, J.; Purohit, P.; Rafaj, P.; Sharma, R.; et al. The Public Health Implications of the Paris Agreement: A Modelling Study. Lancet Planet. Health 2021, 5, e74–e83. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Moudon, A.V.; Lowe, M.; Adlakha, D.; Cerin, E.; Boeing, G.; Higgs, C.; Arundel, J.; Liu, S.; Hinckson, E.; et al. Creating Healthy and Sustainable Cities: What Gets Measured, Gets Done. Lancet Glob. Health 2022, 10, e782–e785. [Google Scholar] [CrossRef]
- Diaz Olvera, L.; Plat, D.; Pochet, P. The Puzzle of Mobility and Access to the City in Sub-Saharan Africa. J. Transp. Geogr. 2013, 32, 56–64. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation Global Status Report on Road Safety 2018. Available online: https://www.who.int/publications-detail-redirect/9789241565684 (accessed on 4 September 2021).
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1·6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Antonel, J.; Chowdhury, Z. Measuring Ambient Particulate Matter in Three Cities in Cameroon, Africa. Atmos. Environ. 2014, 95, 344–354. [Google Scholar] [CrossRef]
- Charmes, J. Time-Use Surveys in Africa: Problems and Prospects. In Mainstreaming Unpaid Work; Oxford University Press: Delhi, India, 2017; ISBN 978-0-19-946825-6. [Google Scholar]
- Poushter, J.; Oates, R. Cell Phones in Africa: Communication Lifeline. In Pew Research Center’s Global Attitudes Project; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Wesolowski, A.; Eagle, N.; Noor, A.M.; Snow, R.W.; Buckee, C.O. The Impact of Biases in Mobile Phone Ownership on Estimates of Human Mobility. J. R. Soc. Interface 2013, 10, 20120986. [Google Scholar] [CrossRef]
- Ortiz-Ospina, E.; Giattino, C.; Roser, M. Time Use; Our World in Data: Oxford, UK, 2020. [Google Scholar]
- Hubert, J.-P.; Toint, P.L. From Average Travel Time Budgets to Daily Travel Time Distributions: Appraisal of Two Conjectures by Kölbl and Helbing and Some Consequences. Transp. Res. Rec. 2006, 1985, 135–143. [Google Scholar] [CrossRef]
- Hubert, J.; Armoogum, J.; Axhausen, K.W.; Madre, J. Immobility and Mobility Seen through Trip-Based Versus Time-Use Surveys. Transp. Rev. 2008, 28, 641–658. [Google Scholar] [CrossRef]
- Global Centre of Excellence on Gender Statistics Measuring Time Use: An Assessment of Issues and Challenges in Conducting Time-Use Surveys with Special Emphasis on Developing Countries. Available online: https://data.unwomen.org/publications/measuring-time-use-assessment-issues-and-challenges-conducting-time-use-surveys (accessed on 12 June 2022).
- Garcia, L.; Johnson, R.; Johnson, A.; Abbas, A.; Goel, R.; Tatah, L.; Damsere-Derry, J.; Kyere-Gyeabour, E.; Tainio, M.; de Sá, T.H.; et al. Health Impacts of Changes in Travel Patterns in Greater Accra Metropolitan Area, Ghana. Environ. Int. 2021, 155, 106680. [Google Scholar] [CrossRef] [PubMed]
- Behrens, R.; Olvera, L.D.; Plat, D.; Pochet, P. Meta-Analysis of Travel of the Poor in West and Southern African Cities. In Proceedings of the WCTRS, ITU. 10th World Conference on Transport Research—WCTR’04, Istanbul, Turkey, 4–8 July 2004; WCTRS: Montréal, QC, Canada, 2004; p. 19. [Google Scholar]
- World Bank. Planning for Uganda’s Urbanization; World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Rwakarehe, E.E. Review of Strategies for Curbing Traffic Congestion in Sub-Saharan Africa Cities: Technical and Policy Perspectives. Tanzan. J. Eng. Technol. 2022, 40, 24–32. [Google Scholar] [CrossRef]
- Gonzales, E.; Chavis, C.; Li, Y.; Daganzo, C.F. Multimodal Transport in Nairobi, Kenya: Insights and Recommendations with a Macroscopic Evidence-Based Model. In Proceedings of the Transportation Research Board 90th Annual Meeting, Washington, DC, USA, 23–27 January 2011. [Google Scholar]
- Melbye, D.C.; Møller-Jensen, L.; Andreasen, M.H.; Kiduanga, J.; Busck, A.G. Accessibility, Congestion and Travel Delays in Dar Es Salaam—A Time–Distance Perspective. Habitat Int. 2015, 46, 178–186. [Google Scholar] [CrossRef]
- Andreasen, M.H.; Møller-Jensen, L. Access to the City: Mobility Patterns, Transport and Accessibility in Peripheral Settlements of Dar Es Salaam. J. Transp. Geogr. 2017, 62, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Salon, D.; Gulyani, S. Mobility, Poverty, and Gender: Travel ‘Choices’ of Slum Residents in Nairobi, Kenya. Transp. Rev. 2010, 30, 641–657. [Google Scholar] [CrossRef]
- Janusz, K.; Kesteloot, C.; Vermeiren, K.; Van Rompaey, A. Daily Mobility, Livelihoods and Transport Policies in Kampala, Uganda: A Hägerstrandian Analysis. Tijdschr. Voor Econ. En Soc. Geogr. 2019, 110, 412–427. [Google Scholar] [CrossRef]
- Tembe, A.; Nakamura, F.; Tanaka, S.; Ariyoshi, R.; Miura, S. The Demand for Public Buses in Sub-Saharan African Cities: Case Studies from Maputo and Nairobi. IATSS Res. 2019, 43, 122–130. [Google Scholar] [CrossRef]
- Evans, J.; O’Brien, J.; Ch Ng, B. Towards a Geography of Informal Transport: Mobility, Infrastructure and Urban Sustainability from the Back of a Motorbike. Trans. Inst. Br. Geogr. 2018, 43, 674–688. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 82, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Valérie, O.; Epo, B. Suburbanization and Inequality in Transport Mobility in Yaoundé, Cameroon: Drawing Public Policy for African Cities; Global Development Network: New Delhi, India, 2013. [Google Scholar]
- Yaounde SUMP Summary. Available online: https://www.mobiliseyourcity.net/sites/default/files/2021-03/Yaounde%20SUMP%20Summary_final.pdf (accessed on 15 June 2022).
- Himelein, K.; Eckman, S.; Lau, C.; McKenzie, D. Mobile Phone Surveys for Understanding COVID-19 Impacts: Part II Response, Quality, and Questions. Available online: https://blogs.worldbank.org/impactevaluations/mobile-phone-surveys-understanding-covid-19-impacts-part-ii-response-quality-and (accessed on 21 February 2022).
- Demographic and Health Surveys The DHS Program—Wealth-Index-Construction. Available online: https://dhsprogram.com/topics/wealth-index/Wealth-Index-Construction.cfm (accessed on 26 February 2022).
- Chakraborty, N.M.; Fry, K.; Behl, R.; Longfield, K. Simplified Asset Indices to Measure Wealth and Equity in Health Programs: A Reliability and Validity Analysis Using Survey Data From 16 Countries. Glob. Health Sci. Pract. 2016, 4, 141–154. [Google Scholar] [CrossRef] [Green Version]
- Smits, J.; Steendijk, R. The International Wealth Index (IWI). Soc. Indic. Res. 2015, 122, 65–85. [Google Scholar] [CrossRef]
- Dake, F.; Tatah, L.; Goel, R.; Woodcock, J. Travel Behaviour Characteristics from a Time Use and Travel Diary Survey in Accra, Ghana; MRC Epidemiology Unit, University of Cambridge: Cambridge, UK, 2022. [Google Scholar]
- Tatah, L.; Foley, L.; Oni, T.; Pearce, M.; Lwanga, C.; Were, V.; Assah, F.; Wasnyo, Y.; Mogo, E.; Okello, G.; et al. Travel Behaviour Characteristics and Correlates in Nairobi and Kisumu, Kenya; MRC Epidemiology Unit, University of Cambridge: Cambridge, UK, 2022. [Google Scholar]
- Salon, D.; Gulyani, S. Commuting in Urban Kenya: Unpacking Travel Demand in Large and Small Kenyan Cities. Sustainability 2019, 11, 3823. [Google Scholar] [CrossRef] [Green Version]
- Greater London Authority. Travel Patterns and Trends; London Datastore: London, UK, 2012.
- Australian Capital Territory Governmnet ACT and Queanbeyan-Palerang Household Travel Survey (ACTQP HTS). Available online: https://www.transport.act.gov.au/about-us/planning-for-the-future/household-travel-survey (accessed on 15 June 2022).
- Strain, T.; Wijndaele, K.; Garcia, L.; Cowan, M.; Guthold, R.; Brage, S.; Bull, F.C. Levels of Domain-Specific Physical Activity at Work, in the Household, for Travel and for Leisure among 327 789 Adults from 104 Countries. Br. J. Sports Med. 2020, 54, 1488–1497. [Google Scholar] [CrossRef] [PubMed]
- Tatah, L.; Mapa-Tassou, C.; Shung-King, M.; Oni, T.; Woodcock, J.; Weimann, A.; McCreedy, N.; Muzenda, T.; Govia, I.; Mbanya, J.C.; et al. Analysis of Cameroon’s Sectoral Policies on Physical Activity for Noncommunicable Disease Prevention. Int. J. Environ. Res. Public Health 2021, 18, 12713. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Barrett, F. Africa Infrastructure Country Diagnostic. Stuck in Traffic:Urban Transport in Africa; World Bank and Sub-Saharan Transport Policy Program (SSATP): Washington, DC, USA; Bamako, Mali, 2008. [Google Scholar]
- Joly, I. Travel Time Budget—Decomposition of the Worldwide Mean. In Proceedings of the IATUR, ISTAT. Italian National Statistical Institute. Time Use: What’s New in Methodology and Application Fields? Rome, Italy, 27–29 October 2004; p. 23. [Google Scholar]
- Tranter, P.J. Speed Kills: The Complex Links Between Transport, Lack of Time and Urban Health. J. Urban Health 2010, 87, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Ng, W.-S.; Acker, A. Understanding Urban Travel Behaviour by Gender for Efficient and Equitable Transport Policies; International Transport Forum Discussion Paper; OECD: Paris, France, 2018. [Google Scholar]
- Bartlett, L. Specifying Hybrid Models of Teachers’ Work During COVID-19. Educ. Res. 2022, 51, 152–155. [Google Scholar] [CrossRef]
- Ozimek, A. The Future of Remote Work; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Triyason, T.; Tassanaviboon, A.; Kanthamanon, P. Hybrid Classroom: Designing for the New Normal after COVID-19 Pandemic. In Proceedings of the 11th International Conference on Advances in Information Technology, Bangkok, Thailand, 1–3 July 2020; Association for Computing Machinery: New York, NY, USA, 2020; pp. 1–8. [Google Scholar]
- Teachout, M.; Zipfel, C. The Economic Impact of COVID-19 Lockdowns in SubSaharan Africa. Available online: https://www.theigc.org/wp-content/uploads/2020/05/Teachout-and-Zipfel-2020-policy-brief-.pdf (accessed on 9 June 2022).
- Brooks, J.H.M.; Tingay, R.; Varney, J. Social Distancing and COVID-19: An Unprecedented Active Transport Public Health Opportunity. Br. J. Sports Med. 2021, 55, 411–412. [Google Scholar] [CrossRef]
- Klopp, J.; Mitullah, W. Politics, Policy and Paratransit: A View from Nairobi. In Paratransit in African Cities; Routledge: London, UK, 2015; ISBN 978-1-315-84951-5. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Activity
| Duration (minutes) | Location
| Mode of Travel
| Who with
|
| 7:00–7:30 | |||||
| 7:30–8:00 | |||||
| 8:00–8:30 | |||||
| 8:30–9:00 | |||||
| 9:00–9:30 |
| Summary of Household Characteristics | Summary of Individual Characteristics | |||
|---|---|---|---|---|
| Unweighted | Weighted | |||
| n | 1199 | n | 1334 | 1334 |
| Household size (median (IQR) | 3 (1–4) | Female (%) | 505 (38) | 616 (46) |
| Households headed by females = Yes (%) | 302 (28) | Age (mean (SD)) | 38 (12) | 36 (13) |
| Education of household head (%) | Age group (%) | |||
| Primary school or less | 130 (12) | ≤24 years | 85 (6) | 255 (19) |
| JHS/middle school | 227 (21) | 25 to 34 years | 523 (39) | 491 (37) |
| SHS/secondary school | 224 (20) | 35 to 44 years | 385 (29) | 287 (22) |
| High school | 515 (47) | 45 to 54 years | 197 (15) | 157 (12) |
| ≥55 years | 144 (11) | 144 (11) | ||
| Occupation of the house heads (%) | Education (%) | |||
| Employed | 696 (64) | Primary school or less | 164 (12) | 172 (13) |
| Student | 102 (9) | JHS/middle school | 278 (21) | 269 (20) |
| Not employed or not applicable | 119 (11) | SHS/secondary school | 282 (21) | 273 (21) |
| Other | 179 (16) | High school | 610 (46) | 621 (47) |
| Household vehicle ownership | Marital status (%) | |||
| Any vehicle | 415 (35) | Never married | 458 (34) | 561 (42) |
| Car | 256 (21) | Formerly married | 127 (10) | 126 (9) |
| Motorcycle | 139 (12) | Living together | 280 (21) | 263 (20) |
| Bicycle | 96 (8) | Married | 469 (35) | 384 (29) |
| Household Wealth | Occupation (%) | |||
| Poorer | 400 (33) | Employed | 815 (61) | 735 (55) |
| Middle | 400 (33) | Student | 141 (11) | 218 (16) |
| Richer | 399 (33) | Not employed or not applicable | 177 (13) | 204 (15) |
| Other | 201 (15) | 177 (13) | ||
| Relationship to head (%) | ||||
| Head | 1096 (82) | 1015 (76) | ||
| Spouse | 149 (11) | 161 (12) | ||
| Son or daughter | 51 (4) | 96 (7) | ||
| other | 38 (3) | 63 (5) | ||
| Any vehicle in house = Yes (%) | 471 (35) | 434 (33) | ||
| Cars/motorcycles in house = Yes (%) | 424 (32) | 388 (29) | ||
| Household Wealth | ||||
| Poorer | 435 (33) | 479 (36) | ||
| Middle | 450 (34) | 444 (33) | ||
| Richer | 449 (34) | 411 (31) | ||
| Both Sexes | Females | Males | ||||
|---|---|---|---|---|---|---|
| Trip Mode | Share (%) (n = 2153) | Mean (IQR) Minutes | Share (%) (n = 907) | Mean (IQR) | Share (%) (n = 1245) | Mean (IQR) Minutes |
| Walk | 26.6 | 41 (30–60) | 27.5 | 40 (30–60) | 25.9 | 43 (30–60) |
| Bicycle | 0.2 | 36 (30–30) | … | … | 0.3 | 36 (30–30) |
| Motorcycle | 5 | 42 (30–60) | 0.8 | 49 (20–90) | 8 | 41 (30–60) |
| Motorcycle taxis | 10.3 | 39 (30–30) | 11.8 | 37 (30–30) | 9.2 | 41 (30–30) |
| Car | 10.6 | 59 (30–60) | 4.8 | 49 (30–60) | 14.8 | 62 (30–60) |
| Taxi | 45.7 | 50 (30–60) | 54 | 48 (30–60) | 39.7 | 51 (30–60) |
| Public bus | 0.6 | 146 (60–210) | 0.1 | 360 (360–360) | 1 | 129 (60–210) |
| Opep | 0.8 | 55 (30–60) | 0.9 | 30 (30–30) | 0.7 | 78 (30–120) |
| Other | 0.3 | 52 (30–80) | … | … | 0.5 | 52 (30–80) |
| Overall | 100 | 48 (30–60) | 100 | 45 (30–60) | 100 | 50 (30–60) |
| Characteristic | Percentage |
|---|---|
| Participants (n= 1334) | |
| % People reporting walking | 25% |
| Walking trip stages (n = 845) | |
| % Of walking as the main mode | 85% |
| % Of walking accompanying taxi | 12% |
| % Of walking accompanying motorcycle | 2% |
| % Accompanying other modes | 1% |
| Shared taxi trips (n = 999) | |
| % Accompanied by walking | 6% |
| % Accompanied by motorcycle | 2% |
| % Accompanied by other mother modes | 3% |
| % Unaccompanied by other modes | 89% |
| Motorcycle taxi trips (n = 207) | |
| % Accompanied by walking | 6% |
| % Unaccompanied by other modes | 83% |
| Made Trip | Number of Trips Made | ||||||
|---|---|---|---|---|---|---|---|
| No | Yes | p | 1 Trip | 2 Trips | 3 Trips | 4+ Trips | |
| n (%) | 487 (37) | 847 (63) | 108 (13) | 409 (48) | 172 (20) | 153 (19) | |
| Female (%) | 54 | 42 | 0.00 | 48 | 46 | 32 | 39 |
| Age group (%) | 0.00 | ||||||
| ≤24 years | 25 | 16 | 17 | 17 | 19 | 8 | |
| 25 to 34 years | 29 | 42 | 41 | 39 | 44 | 46 | |
| 35 to 44 years | 22 | 21 | 19 | 20 | 18 | 28 | |
| 45 to 54 years | 11 | 12 | 11 | 12 | 13 | 12 | |
| ≥55 years | 12 | 10 | 11 | 12 | 6 | 6 | |
| Education (%) | 0.66 | ||||||
| ≤ Primary school | 14 | 12 | 9 | 12 | 13 | 13 | |
| Middle school | 20 | 20 | 20 | 20 | 20 | 21 | |
| Secondary school | 21 | 20 | 24 | 22 | 18 | 17 | |
| ≥High school | 45 | 48 | 46 | 47 | 49 | 49 | |
| Marital status (%) | 0.32 | ||||||
| Never married | 40 | 43 | 43 | 39 | 49 | 49 | |
| Formerly married | 11 | 9 | 7 | 9 | 6 | 11 | |
| Living together | 21 | 19 | 15 | 19 | 22 | 16 | |
| Married | 28 | 29 | 35 | 32 | 23 | 24 | |
| Occupation (%) | 0.00 | ||||||
| Employed | 44 | 62 | 54 | 65 | 58 | 62 | |
| Student | 19 | 15 | 16 | 16 | 15 | 9 | |
| Not employed | 18 | 14 | 20 | 9 | 18 | 16 | |
| Other | 19 | 10 | 11 | 9 | 9 | 13 | |
| Relationship (%) | 0.00 | ||||||
| Head | 67 | 81 | 73 | 75 | 90 | 92 | |
| Spouse | 19 | 8 | 13 | 12 | 2 | 3 | |
| Son or daughter | 9 | 6 | 9 | 8 | 5 | 3 | |
| Other | 6 | 4 | 6 | 5 | 3 | 1 | |
| Any vehicle (%) | 41 | 28 | 0.00 | 31 | 29 | 24 | 27 |
| Car/motorcycle (%) | 36 | 25 | 0.00 | 29 | 26 | 22 | 24 |
| Household Wealth | 0.00 | ||||||
| Poorer | 27 | 41 | 35 | 37 | 50 | 47 | |
| Middle | 34 | 33 | 38 | 32 | 30 | 35 | |
| Richer | 39 | 26 | 28 | 31 | 21 | 18 | |
| Any Active Travel | Active Travel ≥ 30 min | Motorised Transport | Public Transport | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p | No | Yes | p | No | Yes | p | No | Yes | p | |
| n(%) | 1001 (75) | 333 (25) | 1078 (81) | 256 (19) | 636 (48) | 698 (52) | 753 (56) | 580 (44) | ||||
| Female (%) | 47 | 42 | 0.18 | 47 | 42 | 0.20 | 52 | 41 | 0.00 | 46 | 46 | 0.93 |
| Age group (%) | 0.30 | 0.10 | 0.00 | 0.00 | ||||||||
| ≤24 years | 19 | 20 | 18 | 22 | 26 | 13 | 23 | 14 | ||||
| 25 to 34 years | 35 | 42 | 35 | 43 | 30 | 43 | 29 | 48 | ||||
| 35 to 44 years | 23 | 18 | 22 | 19 | 20 | 23 | 23 | 20 | ||||
| 45 to 54 years | 12 | 11 | 13 | 9 | 11 | 13 | 13 | 10 | ||||
| ≥55 years | 11 | 10 | 12 | 7 | 13 | 9 | 13 | 8 | ||||
| Education (%) | 0 | 0.10 | 0.67 | 0.00 | 0.00 | |||||||
| ≤ Primary school | 12 | 16 | 12 | 15 | 17 | 9 | 16 | 9 | ||||
| Middle school | 19 | 23 | 20 | 20 | 21 | 20 | 22 | 18 | ||||
| Secondary school | 21 | 18 | 21 | 18 | 20 | 21 | 20 | 21 | ||||
| High school | 48 | 43 | 46 | 47 | 43 | 50 | 43 | 52 | ||||
| Marital status (%) | 0 | 0.00 | 0.00 | 0.12 | 0.04 | |||||||
| Never married | 37 | 57 | 37 | 63 | 45 | 39 | 41 | 44 | ||||
| Formerly married | 10 | 8 | 10 | 6 | 10 | 9 | 9 | 10 | ||||
| Living together | 22 | 13 | 22 | 11 | 19 | 20 | 18 | 22 | ||||
| Married | 31 | 22 | 31 | 20 | 26 | 31 | 32 | 25 | ||||
| Occupation (%) | 0.06 | 0.06 | 0.00 | 0.00 | ||||||||
| Employed | 56 | 53 | 56 | 51 | 43 | 66 | 48 | 64 | ||||
| Student | 16 | 19 | 15 | 21 | 21 | 12 | 18 | 14 | ||||
| Not employed | 14 | 19 | 14 | 19 | 19 | 12 | 18 | 12 | ||||
| Other | 15 | 10 | 14 | 9 | 16 | 11 | 16 | 10 | ||||
| Relationship (%) | 0.01 | 0.00 | 0.00 | 0.13 | ||||||||
| Head | 74 | 82 | 74 | 83 | 69 | 82 | 73 | 80 | ||||
| Spouse | 14 | 5 | 14 | 4 | 15 | 9 | 14 | 10 | ||||
| Son or daughter | 7 | 7 | 8 | 5 | 9 | 6 | 8 | 6 | ||||
| Other | 4 | 6 | 4 | 8 | 7 | 3 | 6 | 4 | ||||
| Any vehicle (%) | 36 | 21 | 0.00 | 35 | 22 | 0.00 | 36 | 30 | 0.02 | 45 | 17 | 0.00 |
| Car/motorcycle (%) | 33 | 18 | 0.00 | 32 | 17 | 0.00 | 32 | 27 | 0.07 | 41 | 14 | 0.00 |
| Household Wealth | 0.00 | 0.00 | 0.09 | 0.00 | ||||||||
| Poorer | 30 | 53 | 31 | 56 | 34 | 38 | 31 | 43 | ||||
| Middle | 35 | 29 | 35 | 27 | 32 | 34 | 31 | 36 | ||||
| Richer | 35 | 18 | 34 | 17 | 34 | 28 | 38 | 22 | ||||
| All Participants | Participants Who Travelled | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Overall | Active | Motorised | Public | Overall | Active | Motorised | Public |
| All | 77 (0–120) | 18 (0–0) | 56 (0–90) | 43 (0–60) | 121 (60–150) | 28 (0–45) | 88 (30–120) | 67 (0–90) |
| Sex | ||||||||
| Male | 88 (0–120) | 18 (0–30) | 66 (0–90) | 44 (0–60) | 129 (60–150) | 27 (0–40) | 96 (40–120) | 65 (0–90) |
| Female | 63 (0–90) | 16 (0–0) | 45 (0–60) | 41 (0–60) | 110 (60–150) | 29 (0–60) | 78 (30–120) | 71 (10–120) |
| Age group (years) | ||||||||
| ≤24 years | 49 (0–80) | 18 (0–30) | 28 (0–60) | 27 (0–60) | 95 (60–120) | 35 (0–60) | 55 (0–60) | 51 (0–60) |
| 25 to 34 years | 87 (0–120) | 19 (0–30) | 64 (0–90) | 54 (0–90) | 121 (60–150) | 27 (0–40) | 90 (30–120) | 75 (30–120) |
| 35 to 44 years | 84 (0–120) | 12 (0–0) | 68 (0–100) | 47 (0–60) | 135 (60–150) | 20 (0–30) | 109 (60–120) | 75 (0–120) |
| 45 to 54 years | 82 (0–120) | 18 (0–0) | 60 (0–90) | 36 (0–60) | 126 (60–150) | 27 (0–30) | 93 (50–120) | 56 (0–90) |
| ≥55 years | 73 (0–120) | 21 (0–0) | 49 (0–60) | 33 (0–60) | 127 (60–150) | 35 (0–60) | 85 (0–120) | 58 (0–90) |
| Education | ||||||||
| ≤Primary school | 74 (0–120) | 30 (0–30) | 41 (0–60) | 32 (0–60) | 125 (60–150) | 51 (0–60) | 70 (0–90) | 54 (0–90) |
| Middle school | 77 (0–120) | 22 (0–30) | 52 (0–90) | 39 (0–60) | 123 (60–150) | 34 (0–60) | 83 (30–120) | 62 (0–100) |
| Sec school | 70 (0–120) | 16 (0–0) | 50 (0–60) | 37 (0–60) | 111 (60–150) | 26 (0–30) | 79 (30–120) | 59 (0–90) |
| High school | 80 (0–120) | 13 (0–0) | 65 (0–90) | 50 (0–90) | 124 (60–150) | 20 (0–30) | 99 (60–120) | 77 (0–105) |
| Occupation | ||||||||
| Employed | 82 (0–120) | 16 (0–0) | 63 (0–90) | 47 (0–85) | 116 (60–150) | 23 (0–30) | 89 (45–120) | 67 (0–100) |
| Student | 62 (0–90) | 20 (0–30) | 39 (0–60) | 38 (0–60) | 110 (60–120) | 36 (0–60) | 69 (0–90) | 66 (0–90) |
| Not employed | 73 (0–120) | 22 (0–30) | 47 (0–90) | 37 (0–60) | 129 (60–180) | 39 (0–60) | 83 (0–120) | 65 (0–120) |
| Other | 76 (0–120) | 14 (0–0) | 59 (0–90) | 37 (0–60) | 156 (60–180) | 29 (0–30) | 121 (60–150) | 76 (0–120) |
| Marital status | ||||||||
| Never married | 77 (0–120) | 23 (0–30) | 51 (0–80) | 45 (0–60) | 117 (60–150) | 36 (0–60) | 77 (0–120) | 68 (0–90) |
| Formerly married | 67 (0–120) | 18 (0–0) | 48 (0–90) | 39 (0–60) | 117 (60–150) | 31 (0–60) | 83 (40–120) | 68 (30–105) |
| Living together | 76 (0–120) | 13 (0–0) | 61 (0–90) | 48 (0–90) | 126 (60–150) | 21 (0–30) | 100 (60–135) | 80 (30–120) |
| Married | 80 (0–120) | 12 (0–0) | 64 (0–90) | 38 (0–60) | 124 (60–150) | 19 (0–20) | 99 (60–120) | 58 (0–90) |
| Vehicle in house | ||||||||
| No vehicle | 79 (0–120) | 22 (0–30) | 55 (0–90) | 52 (0–90) | 117 (60–150) | 32 (0–60) | 80 (30–120) | 76 (30–120) |
| Any vehicle | 71 (0–120) | 9 (0–0) | 59 (0–90) | 24 (0–0) | 131 (60–160) | 17 (0–30) | 109 (60–150) | 45 (0–60) |
| Car/Motorcycle | 72 (0–120) | 7 (0–0) | 62 (0–90) | 23 (0–0) | 132 (60–160) | 13 (0–15) | 113 (60–150) | 43 (0–60) |
| Household Wealth | ||||||||
| Poorer | 85 (0–120) | 27 (0–60) | 55 (0–90) | 50 (0–80) | 117 (60–150) | 38 (0–60) | 76 (10–120) | 69 (0–100) |
| Middle | 79 (0–120) | 15 (0–0) | 61 (0–90) | 47 (0–90) | 126 (60–150) | 24 (0–30) | 97 (60–120) | 75 (0–120) |
| Richer | 65 (0–90) | 9 (0–0) | 52 (0–90) | 30 (0–45) | 121 (60–150) | 17 (0–15) | 97 (60–120) | 55 (0–90) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatah, L.; Wasnyo, Y.; Pearce, M.; Oni, T.; Foley, L.; Mogo, E.; Obonyo, C.; Mbanya, J.C.; Woodcock, J.; Assah, F. Travel Behaviour and Barriers to Active Travel among Adults in Yaoundé, Cameroon. Sustainability 2022, 14, 9092. https://doi.org/10.3390/su14159092
Tatah L, Wasnyo Y, Pearce M, Oni T, Foley L, Mogo E, Obonyo C, Mbanya JC, Woodcock J, Assah F. Travel Behaviour and Barriers to Active Travel among Adults in Yaoundé, Cameroon. Sustainability. 2022; 14(15):9092. https://doi.org/10.3390/su14159092
Chicago/Turabian StyleTatah, Lambed, Yves Wasnyo, Matthew Pearce, Tolu Oni, Louise Foley, Ebele Mogo, Charles Obonyo, Jean Claude Mbanya, James Woodcock, and Felix Assah. 2022. "Travel Behaviour and Barriers to Active Travel among Adults in Yaoundé, Cameroon" Sustainability 14, no. 15: 9092. https://doi.org/10.3390/su14159092
APA StyleTatah, L., Wasnyo, Y., Pearce, M., Oni, T., Foley, L., Mogo, E., Obonyo, C., Mbanya, J. C., Woodcock, J., & Assah, F. (2022). Travel Behaviour and Barriers to Active Travel among Adults in Yaoundé, Cameroon. Sustainability, 14(15), 9092. https://doi.org/10.3390/su14159092