Abstract
Higher injury rates among children is a significant post-COVID-19 phenomenon. This paper focuses on injury frequency in pre-school, as well as in younger school-age children, and maps the approaches used by families to prevent injuries and ensure child safety in the Czech Republic. The aim of the survey was to determine what types of serious injuries prevail among children, how parents or grandparents evaluate the awareness of children toward dangerous situations, and what opinions and preferences they have regarding educating their children about health and safety. The questionnaire survey among parents and grandparents (N = 278) of children from birth to the age of 12 was conducted at educational events for the wider public in 2017–2019. The survey showed that head injuries (27%) are prevalent among pre-school children; however, in children older than 5 years, injuries are due to increased outdoor activity and tend to be more associated with sports and leisure activities (fractures 31%, burns 23%). Most respondents considered their children to be more likely to recognize life-threatening risks, which is worrying in the context of the rising number of injuries in the Czech Republic in recent years.
1. Introduction
Ensuring the safety of children is an inseparable part of ensuring the health and well-being of the child. Therefore, it is necessary to address child injury prevention through education programs with a focus on developing knowledge, skills, and attitudes that can be monitored and evaluated [1]. Preventing child injuries falls mainly under the third Sustainable Development Goal (SDG) of good health and well-being, which addresses child health [2]. However, security issues are also included in other SGDs (SDG 11.2 focusing on road safety and 13 other SDGs of relevance) [3]. Protecting child health is also related to educating parents, especially mothers, and prioritizing health protection for children under the age of 5 [4]. The SDGs [5] highlight this age group as it is the one most impacted by child mortality on a global basis [6], while the group of children aged 5 to 14 years in Europe is the most impacted by fatalities among children [7].
The issue of the interconnection between health care and education is also included in the fourth SDG, quality education, because “education is one of the most potent ways to improve individuals’ health—and to make sure the benefits are passed on to future generations” [5] (p. 27). The effectiveness of educating a child to behave safely is closely related to the quality of the relationships between the educational environment of the family, pre-school and out-of-school institutions, and school education. However, it is worth noting the limitations of educating children under the age of 12; research shows that providing a safe environment and parental supervision has more substantial safety effects in ensuring effective injury prevention than simply teaching children [8]. The lifelong benefits for the sustainability of good behavior patterns are precisely those approaches that take account of the needs and attitudes of families in this area and respond to and complement them within the education of children from pre-school age and upward. This postulate is the basis of the present study, which investigates childhood injury rates and family views on children’s readiness to respond to danger, as well as ways of educating pre-school and younger school-age children to behave safely in the Czech Republic. The focus on the views and experiences of parents and grandparents as the main educators of their children is quite innovative in the Czech context. So far, this topic has been studied only from the perspective of the incidence of injuries and also in terms of injury prevention in schools and the development of educational material for teachers and parents. However, parents’ experiences, opinions, and family strategies in the field of health protection of their children have not been investigated.
2. Theoretical Backgrounds
2.1. Child Injuries in the World and European Region
According to the World Health Organization (WHO), “an injury is the damage caused by an acute transfer of energy, whether physical, thermal, chemical, or radiant, that exceeds the physiological threshold, or by the deprivation of a vital element” [7] (p. 6). WHO further distinguishes injuries into unintentional (caused by road traffic injuries, poisoning, falls, fire, heat and hot substances, drowning, or submersion) and intentional (interpersonal, self-directed violence, or collective violence). In this respect, the present study focuses only on accidental injuries.
The WHO reports that under-5 mortality from injury has declined significantly over the past 30 years, from 12.6 million in 1990 to 5 million in 2020. Regional differences are very significant, with 37 out of 1000 children at risk of death under the age of 5 years globally, with the highest in sub-Saharan Africa (72) and the Middle East (45) and the lowest in the Americas (13) and Europe (8) [9]. For children aged 5–14 years, the most common fatal injuries in the European region are first those caused by road injuries, followed by drowning, and other accidental injuries are in third place. For children aged 0–4 years, these other types of accidental injuries predominate over fatal injuries [7] (p. 10).
The present study investigated the rate of injury in the Czech Republic, which shows very low rates of deaths in children under 5 years of age in international comparisons; in the population of girls it is only 2.57‰ and for boys 3.25‰ [9]. However, an overall comparison of causes of death shows that in the latest data from 2017, the Czech Republic has a higher proportion of child deaths caused by injuries compared to other central and western European countries. Out of 53 countries in Europe, the Czech Republic ranks 36th with 0.07%, behind Ireland and Montenegro (0.02%), Denmark, Finland, Cyprus, and Croatia (0.03%), Italy, Slovakia, the UK, Norway, Sweden, Poland, or Switzerland (0.04%) [10]. Interventions are therefore needed in this area to create conditions for improvement and health and safety promotion in support of the SDGs.
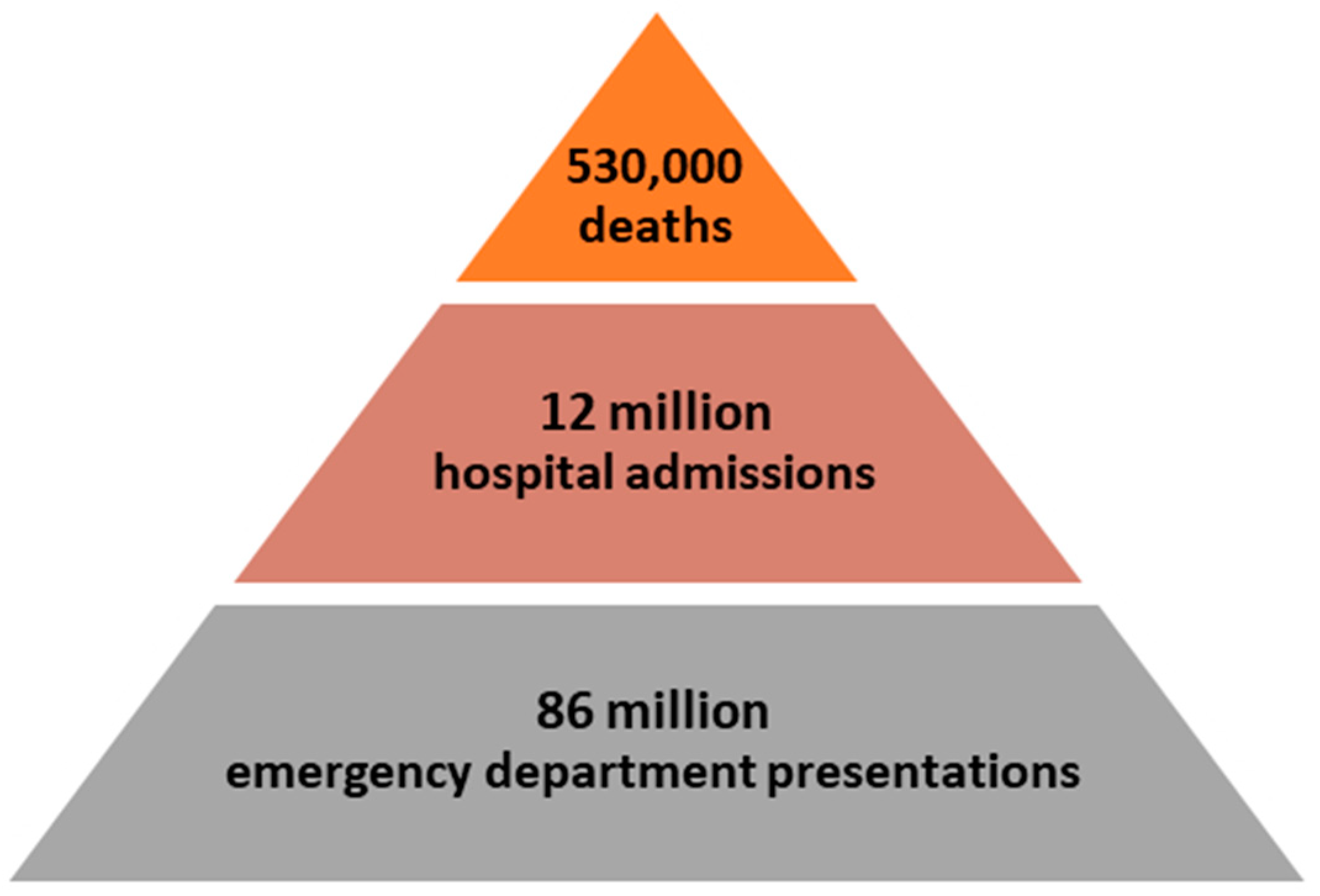
The values relate directly to child deaths that are due to injury, which the WHO monitors in relation to the promotion of SDG Target 3.2: newborn and child mortality. For younger school-age children (5–9 years), the WHO reports a dramatic reduction of 60% in the number of injuries leading to death since 1990 [11]. However, most injuries do not result in death directly but can result in varying degrees of disability or high healthcare costs and negatively affect the quality of later life of the children and their families. However, neither the WHO at the global level, nor the European Union within its countries, tracks the total number of nonfatal injuries. Nevertheless, the WHO [7] reports that there were approximately 166 nonfatal injuries per fatality in 2013–2015 (see Figure 1). Nonfatal injuries are therefore many times more in practice; however, overall information on the number of these injuries is not tracked and published by some countries for international comparison.
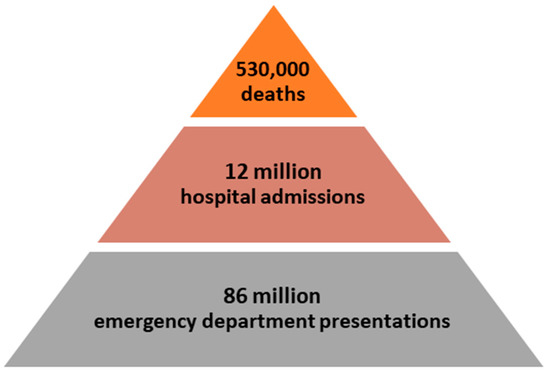
Figure 1.
Violence and injury pyramid in the EU, 2013–2015, adapted from [7] (p. 22).
Although the WHO works on an age division between children up to and including 4 years and 5 to 14 years, the present study uses an age division corresponding to the age classification in education systems and the psychological development of the child [12,13]. The pre-school age covers children from birth to 6 years. The second age group consists of children in the younger school-age range from 7 to 12 years, as this age group corresponds to the typical age of children in primary education in the country.
In the Czech Republic, overall injury data is not systematically collected at the national level. Partial information on childhood injuries is available through the reporting of individual healthcare facilities, which submit information on child patients to the National Injury Register. This register is managed by the Institute of Health Information and Statistics of the Czech Republic, which does not publish these data. Another source of data is reports on school injuries submitted by individual schools to the information system managed by the Czech School Inspectorate. However, even these data are not published; only aggregated information on the total number of school injuries and their distribution in different age groups of children is available, which the school inspectorate publishes in its annual report on the state of Czech education. Some data on child injuries are available in publications of the National Institute of Public Health. The most recent information from 2012 indicates that injuries and poisoning account for 36% of all deaths among children under 14 in the Czech Republic, which is approximately twice the rate of developed EU countries in international comparisons. Of the nonfatal injuries, the highest number of injuries was recorded in the category of fractures and bruises (64.5%), followed by skin injuries (27.6%). Hospitalization that is due to injury was reported in 17.4% of cases, with long-term or permanent aftereffects in 11.1% of children [14]. Injury rates in schools have declined in the last 2 years because of the COVID-19 pandemic and prolonged school closures. The most recent complete pre-pandemic data show that the overall injury index (number of injuries per 100 pupils) was at 2.6 in the 2018/2019 school year, with the injury index being lower in pre-schools (0.47) than in primary schools (3.08) but increasing at both levels since the 2012/2013 school year [15,16].
In practice, therefore, we do not have up-to-date data on the overall injury rate of children in the Czech Republic, as many injuries in out-of-school activities or injuries without medical assistance are not recorded at all. In our study, we therefore try to provide a partial insight into the reality of the frequency and typology of injuries and to point out areas that need to be addressed in educational planning for children and families.
2.2. Injury Research in the Child Population
There are a variety of studies that look at the number and range of injuries in the pediatric population. In recent years, the issue of safety and injury prevention has gained increased attention and research reviews have been produced internationally, e.g., [17]. For example, Norway [18] has mapped this area, looking at injuries in children under 16 years of age (N = 7041). The results show that head injuries are the most common type of injury in 51% of the youngest children, who are mostly injured at home, and 46% of upper limb injuries in older children during sports activities, who are injured in both home and school settings. Research by Mohammed et al. [19] conducted in Egypt (N = 634) reported open wounds (45.5%) as the most common type of injury in pre-school children, followed by fractures (35.7%), burns (19.7%), and electric shock (1.9%). According Sengoelge et al. [20], fatal injuries in the home environment are most common in children under 5 years of age in a comparison of 16 European countries, followed by an increasing frequency of road traffic injuries, with 90% of all fatal home injuries being from drowning, burns, poisoning, and falls. These findings are consistent with the WHO’s overview reports presented above.
In the Czech Republic, according to official statistics presented by the Institute of Health Information and Statistics, children (0 to 19 years) are most often injured at home (23% of cases). School injuries (20% of cases) and injuries caused by sports and physical activities (19% of cases) also account for significant proportions. Other injuries are traffic accidents or injuries caused by other causes. For younger school-age children (5–9 years), the predominant injuries are fractures (56%), head injuries with concussion (19%), contusions (9%), and open wounds (6%). In fifth place are burns and scalds, which, although accounting for only 1.2% of injuries at this age, account for almost 10% of injuries in the younger age group (0–4 years). These injuries have the most serious health consequences, which is alarming [21,22].
As parents and their behavior play a key role in the prevention of home injury in young children [23], it is essential to pay attention to their views and the strategies and resources they use. Their attitudes toward child injury prevention determine their decisions about how they will supervise their children and protect them from injury [24,25]. Parents can reduce the risk of injury by building a safe environment, i.e., modifying the environment to eliminate hazards or access to hazards, supervising the activities of children, and teaching children the rules of safe behavior in appropriate ways [8,23]. The results of the study by Zhou, et al. [26] also demonstrate that instruction of children (N = 62,922) on safety rules by parents leads to a reduction in the risk of unintentional injury among Chinese pre-school children through improving children’s safety behaviors.
A qualitative study that focused on children’s perceptions of the risk of unintentional injury showed that parents were able to identify potential risks to children in everyday situations and offer alternative activities. However, parents did not perceive injury as something that could be prevented, but rather as an inevitable part of childhood [27]. A similar perception of injury as an inevitable part of life was also noted by Dalal et al. [28] in their study conducted in China, where more than half of the parents in the study sample (N = 986) felt their children’s injuries were not preventable. In this study, parents also cited lack of parental attention (41.6%), the environment (35.6%), and unsafe behavior of children (22.7%) as the most common barriers to preventing child injury. This lack of acknowledgement of the possibility of effective injury prevention for children illustrates the importance of producing awareness materials or programs and counseling for parents. The effectiveness of counseling in preventing child injury in families together with the toolkit is demonstrated by research conducted in Canada, the results of which showed a statistically significant difference in the direction of reduced child injury risk in families that received both the toolkit and used counseling, but also in families with counseling only, compared to families without these interventions [29].
3. Methodology
3.1. Aims
The main aim of this study is to map the existing approaches applied in our society for the prevention of injuries and damage to the health of children resulting from exposure to safety risks (at school, family, work with PCs, etc.), or for health and safety education. This will provide comprehensive information on the experiences, needs, and attitudes of parents and grandparents on the issue. Within the research itself, the focus will be primarily directed toward determining the relationship between children’s ages and the number of injuries, where this relationship will be conditioned by subintervening variables such as: (i) type of injury, (ii) parents’ and grandparents’ assessment of the child’s ability to recognize danger, (iii) number of injuries, (iv) parent/grandparent preferences for educating their children about health and safety, and (v) method of education. Therefore, the following research questions were formulated from the beginning:
(RQ1) What is the frequency and types of serious injuries that parents/grandparents see as prevalent in their children?
(RQ2) How do parents/grandparents rate their child’s readiness to recognize and respond to hazards and health threats?
(RQ3) What views and preferences do parents/grandparents have about health and safety education for their children?
(RQ4) In what ways do parents/grandparents think children should be educated about safe behaviors?
Within the individual research problems, it was necessary to make further clarifications. These are mainly RQ2 and RQ4. In the case of the second research question (RQ2), a partial refinement was made by dividing the research problem into three categories:
- (i)
- What is the difference in parents/grandparents’ assessment of the child’s ability to recognize danger for the mentioned age categories (RQ2-a)?
- (ii)
- What is the difference in the parents/grandparents’ ratings of the child’s ability to respond appropriately in the event of a life-threatening injury or for the mentioned age categories (RQ2-b)?
- (iii)
- What is the difference in the parents/grandparents’ views on whether the injury could have been prevented for the specific age categories (RQ2-c)?
A similar division was also made in the case of research question 4 (RQ4):
- (i)
- What types of education are used depending on age (RQ4-a)?
- (ii)
- What types of education are used depending on injury (RQ4-b)?
Detailed justification of these divisions is mentioned in Section 4, Results.
3.2. Research Sample
A questionnaire survey conducted during educational events carried out for the general public in the Czech Republic identified a total of N = 408 children in the statements of parents and grandparents, N = 245 of whom were from birth to the age of 6 years and N = 163 aged 7–12 years. However, some of the respondents answered for two or more children at the same time. Thus, for example, they reported having one child aged 0–6 years and one aged 7–12 years. For these children, they then collectively reported having 1–3 injuries in the past year. Due to this fact, it was not possible to determine for all respondents which of the children had sustained an injury, and therefore the research sample of this study consists of 278 children who could be differentiated by age according to the statements of their parents or grandparents (N = 180 for from birth to the age of 6 years, N = 98 for 7–12 years). We worked with the same number of respondents throughout the research population. The calculation of the size of the file was calculated based on the sample size calculator with a confidence level of 95% and a margin of error of 5% (population proportion 50%) with a base file of N = 1,450,000. The detected sample size is N = 385. This means 385 or more measurements/surveys are needed to have a confidence level of 95% that the real value is within ±5% of the measured/surveyed value.
3.3. Description of the Research Tool
The questionnaire for parents and grandparents consisted of 10 closed questions. The first question was demographic, asking for the age of the child to which the questionnaire responses were linked. Respondents could choose from age groups. For the present study, these were pre-school age (from birth to the age of 6 years) and younger school age (7–12 years). The questionnaire items were designed as a list of items or a 4-point Likert scale. They first ascertained the frequency, type, and circumstances of childhood injuries reported by the respondents. Next, they explored respondents’ views on whether the injuries that occurred could have been prevented and asked about the means that the respondents considered appropriate for preventing child injuries. The last two items were devoted to the theme of edification; on the one hand, they asked for opinions on how education should be carried out and, on the other hand, they asked how satisfied respondents were with the current state of education and upbringing of children in the field of safety and health protection.
The questionnaires were distributed at educational events aimed at the general public, through an educational stand organized by the Expert Institute of Health and Safety in 2017–2019. The primary target group of these events was families with children. Respondents were parents or grandparents who visited the educational stand with their children or grandchildren. The vast majority of adults present (over 90%) were willing to participate in the questionnaire survey. Time and space conditions were created for them to do so, as their children were engaged in educational activities at the time and the respondents had space to complete the questionnaire in a focused manner. Respondents were instructed on how to complete the questionnaire. From a methodological point of view, this was an opportunity research sample, as these were respondents who had visited the educational stand on their own and of their own free will and had also volunteered to take part in the survey.
3.4. Data Analyses
Given the nature of the data, we will primarily use the chi-square goodness-of-fit test, since, like the Pearson test, the chi-square goodness-of-fit test is primarily designed for evaluating discrete random variables, where we assume that the random variable X takes on r different values A1, A2, …., Ar, each with a pre-specified probability. We reject the null hypothesis that the distribution of the quantity X coincides with the assumed theoretical distribution at the α significance level (in our case, primarily 0.05) when the realization of the test statistic exceeds the relevant quantile of the chi-squared distribution. Null hypotheses will always continue to be formulated within the relevant analysis. Since a significant drawback of the p-value (the measure of statistical significance of the result) is its strong dependence on the size of the research population, we will also supplement the relevant analyses with substantive significance measures, primarily Cramer’s ϕ (Phi-coefficient) assuming work with a four-field table (Equation (1)) or Cramer’s V if the contingency table dimension is larger than 2 × 2 (Equation (2)):
The more the value of Cramer’s V approaches 1, the more we can talk about the higher level of substantive significance; on the contrary, the more the value of Cramer’s V approaches 0, the more we can talk about low substantive significance. Generalization is then only possible based on confidence intervals (provided that we do not generalize on the basis of statistical significance alone). Here we use SPSS Bootstrap for estimation (we also worked with Excel spreadsheet editor and STATISTICA v.13.3/StatSoft Inc., TIBCO Software, Palo Alto, CA, USA) and let the appropriate number (e.g., 1000) of bootstrap samples be made. This will yield a bootstrap confidence interval for Cramer’s V (default 95%). We should add that proponents of substantive significance measures often point out the problematic nature of statistical testing (p-values) and promote the use of confidence intervals as an alternative to statistical tests, e.g., [30,31], among others.
4. Results
In the case of the first research question (RQ1), which is descriptive in nature, the different types of injuries can also be divided according to two age categories (0–6 years; 7–12 years). We worked with the following types of serious injuries: A—burn, B—fracture, C—injury to internal organs, D—head injury, E—loss of finger or limb, F—electric shock, G—burns, H—visual impairment, I—hearing impairment, J—severe bleeding, K—drowning, L—suffocation, M—severe abrasions/scalping, N—psychological trauma, and O—other. The corresponding values are given in both absolute and relative numbers. The absolute and relative frequencies corresponding to each type of injury are given in the following Table 1:

Table 1.
Absolute and relative numbers of injury types by age category.
The absolute frequencies in the tables do not correspond to the total number of respondents, mainly because some parents did not want to answer the question (this situation also occurs in other cases). The relative numbers show that categories A—burn, B—fracture, and D—head injury.
As discussed in Section 3.1 Aims: in the case of the second research question (RQ2), a partial refinement was made by dividing the research problem into three categories according to the nature of the data obtained. In this case, the following questions were addressed: (i) What is the difference in parents/grandparents’ assessment of the child’s ability to recognize danger for the mentioned age categories (RQ2-a)? (ii) What is the difference in the parents/grandparents’ ratings of the child’s ability to respond appropriately in the event of a life-threatening injury or for the mentioned age categories (RQ2-b)? (iii) What is the difference in the parents/grandparents’ views on whether the injury could have been prevented for the specific age categories (RQ2-c)? For all three domains, parents and grandparents answered the questions using a four-point Likert-type scale [32], which is widely used in educational research; see, e.g., [33,34]. These questions were as follows: (a) Do you think that your child/grandchild can recognize an imminent danger? (e.g., at home, in traffic, at school, at play, etc.); (b) Do you think that your child/grandchild is able to react appropriately in case of a threat to his/her life or health? (c) Do you think that the above-mentioned injury could have been prevented in any way? The descriptive analysis for a given RQ is presented in Table 2:
Table 2.
Parent/grandparent assessment of the child’s readiness to recognize and respond to hazards and health risks—descriptive analysis.
Within each category, there is a prevailing trend of rating (rather YES) and ignoring the two antagonistic options (NO—YES), even assuming that a verbal rating (absolutely NO—absolutely YES) was not used. If any respondent answered twice (has multiple children) and did not split his/her rating for the respective child, he/she was removed from the data matrix. The values of the corresponding inductive analysis, supplemented by the bootstrap confidence interval for Cramer’s V, are then as follows (see Table 3):
Table 3.
Assessment of the child’s readiness by parents/grandparents to recognize and respond to hazards and threats to health—inductive analysis.
In the case of the interpretation of Cramer’s ϕ or Cramer’s V, the interpretation (1) 0.1–0.29 = small effect, (2) 0.3–0.49 = medium effect, and (3) 0.5 or more = large effect is usually used. Although Cohen [35] established these recommendations, they tend to be criticized in the literature, so we decided to leave the interpretation of Cramer’s V to the reader according to the current recommendations. Based on the inductive analysis, it can be seen that significant differences occur in all cases: in the first two cases at the 1% significance level. In the case of RQ2-b, the absolute numbers in each field are small in some cases (see Table 2). If we proceeded to combine the extreme values (i.e., Rather No + No; Rather Yes + Yes), there would be no change in the conclusion because the null hypotheses addressed speaking of the independence of the random variables. Although the χ2 value would decrease to 14.566, the p-value would still be below 0.001 and the Cramer’s V would be 0.24 with intervals of 0.121 (lower limit) and 0.351 (upper limit), respectively.
It is interesting to observe the different groups in terms of the proportion of responses for each item as shown in Table 4:
Table 4.
Parents’/grandparents’ assessment of a child’s readiness to recognize and respond to health hazards and threats—proportion of responses.
Although the data are ordinal in nature, it is possible to observe noticeable differences in the frequency of responses within each RQ. For example, for RQ2-a, almost 57% of parents/grandparents in the age group of children under six think that the child is able to recognize danger. For the age category 7–12 years, more than 76 respondents expressed the same opinion. Within this question, it was expected that older children would be more trusted by parents/grandparents. Surprisingly, however, almost 60% of respondents trusted children under six. A similar conclusion can also be drawn in the case of RQ2-b. The responses in case RQ2-c are interesting, where the question of whether the injury could have been prevented is addressed. Here, the same percentage of respondents thought rather not. However, differences occur for the antagonistic rating options, where more respondents caring for children under six years of age think that the injury could not have been prevented (24.66%) compared to 15.25% for respondents in the older age group. These findings contrast with the responses that imply that the injury could have been prevented (26.03% versus 13.56%), again in favor of younger children.
In the case of RQ3, based on the descriptive analysis describing the absolute counts, it was necessary to merge the outliers with the others as these values were only represented in minimal numbers (see Table 5).
Table 5.
Parent/grandparent evaluation of the edification.
In this case, the parents/grandparents were answering the question: “Are you satisfied with the current state of health and safety edification and education for children?” A χ2 value of 0.705 and a p-value of 0.401 indicate that the null hypothesis cannot be rejected. The differences are also insignificant in terms of substantive significance (ϕ = 0.051; lower limit = 0.004; upper limit = 0.176) and Kendall’s tau b and c values, with b = 0.051 and c = 0.046. The interpretation can also be based on the proportional representation in each age category for different response choices, where this representation is almost identical (see Table 5). If we had performed the same analysis assuming that we did not combine outliers, our conclusions would have been the same, both for statistical and substantive significance.
The last research question (RQ4) is descriptive in nature but still needs to be specified as follows: (i) What types of education are used depending on age (RQ4-a)? (ii) What types of education are used depending on injury (RQ4-b)? The findings, both in absolute and relative frequencies, are presented in Table 6:
Table 6.
Absolute and relative frequency of types of edification depending on the age and number of injuries to the child.
The numbers in Table 6 indicate the absolute numbers where one respondent can tick more than one option. The numbers represent the answer to the question: “In what way should education and training of children in safe behavior be carried out?” So, this is the idea of parents/grandparents. Most of them believe that school is the appropriate place. In the case of children under the age of seven, school facilities are meant in the sense of kindergarten. Therefore, the total may not correspond to the number of respondents and may exceed it (however, we still work with respondents aged from birth to 12 years). It is gratifying to see that the maximum form of support in terms of injury awareness is given to children at school. It is a little surprising that TV programs come second and only in the last place is the initiative of individuals.
Research Limitations
The limitations of the research are mainly: (i) the selection of respondents (in this case, there were situations where parents/grandparents reported multiple injuries for multiple children at the same time; if it happened that it was not possible to clearly assign a specific injury to a child, the respondent was excluded from the data set); (ii) the reluctance of some parents/grandparents to answer the questions; and (iii) the lack of distribution of questions among several age groups of children. The selection of the representatives of the research sample was not and could not have been random, as it had to be guided by certain predetermined criteria, which are the injuries. In the second case, the insufficient number of respondents in some categories is accounted for by grouping them and adding confidence intervals for effect size with the aim of generalizing individual conclusions. This is mainly for the following reasons: proponents of substantive significance measures often point to the problematic nature of statistical testing (p-values) and promote the use of confidence intervals as an alternative to statistical tests, among others. In the third case, some respondents had to be excluded from the data matrix because, for example, a mother with two children did not fill in the questionnaire twice but only once. Thus, it was not possible to distinguish which of the children had suffered a given injury.
5. Discussion
In our opinion, the relevance of the study conducted in the Czech Republic is significant in the context of a sustainable environment and for its local focus. It highlights the need to address the issue of potential injuries to children depending on their age from the perspective of their caregivers (parents/grandparents). The main objective was to map both the current injury rates of pre-school and younger school-age children and the approaches applied by parents and grandparents to prevent injuries to children and damage to their health from exposure to safety hazards. A hazard was seen as a source or situation that could cause injury or damage to a child’s health. The authors are aware that the nature of the danger of objects and situations that a child encounters is conditioned by the child’s development and the extent of their life experience. The situations and objects included in the questionnaire items are based on a review of risks identified [36,37].
In terms of the frequency and types of serious injuries (RQ1), the data obtained from the respondents corresponds with data published in older studies of Czech and foreign origin [14,18,36,37,38,39]. The investigation showed that head injuries predominate in pre-school children. On the other hand, in children over 5 years of age, injuries are caused by increased outdoor activity, so they tend to be more associated with sports and leisure activities, with fractures and burns predominating, and head injuries and other injuries coming third.
It turns out that the individual perspectives of the respondents can vary considerably, depending on the age category of the children. Significant differences are identified in the case of the assessment of a child’s readiness to recognize and respond to danger and health threats (RQ2). The majority of parents and grandparents of pre-school (57%) and younger school-age children (76%) consider their children to be rather capable of recognizing life-threatening risks. In addition, a majority of respondents (62%) consider their younger school-age children to be able to react appropriately in a risky situation.
However, this finding can be considered rather worrying as, on the one hand, parents rate their children as prepared but, on the other hand, the number of injuries to children has actually increased in recent years [15,16]. Moreover, parents are also convinced that injuries are only preventable to a certain extent. For the cohort of pre-school children, an almost equal proportion of parents and grandparents are inclined to think that injuries were not preventable, while for the cohort of younger school-age children, 59% of parents thought that injuries were preventable.
A feature of contemporary childhood is the significantly reduced freedom of movement of children outdoors, dependence on adult accompaniment and supervision, and the later assumption of responsibility for oneself [40]. To develop adequately, children need to experience situations in which they encounter a safe level of risk, as overcoming these challenges is important for the development of their creativity, independence, decision making, and awareness of the limits to their abilities [41,42,43,44]. This limitation of children’s experience represents a risk aspect that is also reflected in the numerical increase in the epidemiology of injuries in the national and international context in recent years, as we show in the theoretical background. Therefore, a balance between safety measures and the benefits of risk-taking situations needs to be sought in the education of children in family and school settings [41,45,46,47]. Current studies investigating parental perceptions of risk also focus on sub-issues, such as their perceptions in relation to pre-school children’s risky outdoor play [48].
In terms of satisfaction with edification (RQ3), the responses of the respondents in our study from both age groups agree in terms of proportional frequency. According to the respondents, the school environment has a significant influence. Thus, in terms of its content (RQ4), our study resonates with the results of the study by Peterson and Mori [49]. They used the epidemiological model of host, agent, and environment to describe the areas at risk of childhood injury and proposed a conceptual model of preventive intervention that was tested in eight children (aged 7 years 7 months to 9 years 7 months). Their model describes prevention goals (harm agent, caregiver, and child), methods (legislative/mandated or educational/persuasive), and tactics (population-wide, milestone, and high-risk group). Thus, reviews in this area have also emphasized the importance of intensive and sustained home visits and early childhood education programs for young children [39,50]. Parenting interventions, which are most often delivered in the home through multifaceted interventions, are effective in reducing child injury [51].
6. Conclusions
Research has shown that the frequency and types of injuries to children aged from birth to 12 years in the Czech Republic have remained similar over the last two decades, with head injuries predominating in pre-school children and injuries in younger school-age children occurring mainly in connection with outdoor activities. The majority of parents of children of both ages are confident that their children will be able to recognize the risk, and, for younger school children, most parents anticipate that their children will even be able to respond appropriately to the emerging risk. From our perspective, a very important observation is that parents still consider the school as the main actor in their children’s safety education and expect educational institutions to fulfil this role.
Thus, collaboration between educational institutions and families has significant potential for preventing child injuries and developing children’s health competencies consistent with ideas of sustainable development. However, the data published in our research point to the fact that this issue is still not given sufficient attention. This is a challenge for follow-up investigations and for the development of appropriate educational materials to significantly reduce injuries in young school-age children by raising awareness of the risks of childhood injuries among parents and others involved in their upbringing and education.
Author Contributions
Conceptualization, P.S. and B.L.S.; methodology, E.M. and V.C.; data curation, V.C.; formal analysis, V.C.; writing—original draft preparation, B.L.S., V.C., K.C., M.B., P.S. and E.M.; writing—review and editing, K.C., B.L.S. and M.B.; visualization, K.C.; supervision, B.L.S.; project administration, B.L.S.; funding acquisition, B.L.S. All authors have read and agreed to the published version of the manuscript.
Funding
The paper was developed with state budget funding provided by the Technology Agency of the Czech Republic within the ETA Programme in the frame of the project named Analysis and Support of Children’s Competence at Health and Safety, grant number: TL03000213.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gururaj, G. Injury Prevention and Care: An Important Public Health Agenda for Health, Survival and Safety of Children. Indian J. Pediatr. 2013, 80, S100–S108. [Google Scholar] [CrossRef] [PubMed]
- United-Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2016. Available online: https://sdgs.un.org/sites/default/files/publications/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 5 June 2022).
- Ma, T.; Peden, A.E.; Peden, M.; Hyder, A.A.; Jagnoor, J.; Duan, L.; Brown, J.; Passmore, J.; Clapham, K.; Tian, M.; et al. Out of the silos: Embedding injury prevention into the Sustainable Development Goals. Inj. Prev. 2021, 27, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Awate, S.; Gorana, R.; Hoffmann, T.; Joon, D.; Morel, W.; Nkomo, E.; O’Donoghue, R.; Pape, N.; Rončević, K.; Taylor, J.; et al. Teaching the Sustainable Goals; Hoffmann, T., Rajeswari, G., Eds.; Engagement Global: Bonn, Germany, 2017. [Google Scholar]
- Unesco. Education 2030: Incheon Declaration and Framework for Action for the Implementation of Sustainable Development Goal 4: Ensure Inclusive and Equitable Quality Education and Promote Lifelong Learning. 2016. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000245656/PDF/245656eng.pdf.multi (accessed on 5 June 2022).
- Meddings, D. Child injury prevention: An overlooked challenge for child survival. Int. J. Environ. Res. Public Health 2013, 10, 568–570. [Google Scholar] [CrossRef] [PubMed]
- WHO. Violence and Injuries in Europe: Burden, Prevention and Priorities for Action; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Morrongiello, B.A. Preventing Unintentional Injuries to Young Children in the Home: Understanding and Influencing Parents’ Safety Practices. Child Dev. Perspect. 2018, 12, 217–222. [Google Scholar] [CrossRef]
- WHO. SDG Target 3.2 End Preventable Deaths of Newborns and Children under 5 Years of Age. Available online: https://www.who.int/data/gho/data/themes/topics/sdg-target-3_2-newborn-and-child-mortality (accessed on 5 June 2022).
- WHO. Distribution of Causes of Death among Children Aged <5 Years (%). Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/89 (accessed on 5 June 2022).
- WHO. Older Children and Young Adolescent Mortality (5 to 14 Years): Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/mortality-among-children-aged-5-14-years (accessed on 5 June 2022).
- Meadows, S. Understanding Child Development: Psychological Perspectives and Applications, 2nd ed.; Routledge: London, UK, 2017; p. 354. [Google Scholar]
- UNESCO. International Standard Classification of Education: ISCED 2011; UNESCO Institute for Statistics: Montreal, QC, Canada, 2012. [Google Scholar]
- Zvadová, Z.; Janoušek, S.; Roth, Z. Úrazovost u dětí školního věku–současné směry prevence. Prevence Úrazů Otrav A Násilí 2012, 8, 7–17. [Google Scholar]
- Zatloukal, T.; Andrys, O.; Basl, J.; Bláhová, A.; Blažek, R.; Bogdanowicz, R.; Borkovcová, I. Kvalita a Efektivita Vzdělávání a Vzdělávací Soustavy ve Školním Roce 2018/2019: Výroční Zpráva České Školní Inspekce; ČŠI: Praha, Czech Republic, 2019; Available online: https://www.csicr.cz/Csicr/media/Prilohy/PDF_el._publikace/V%c3%bdro%c4%8dn%c3%ad%20zpr%c3%a1vy/Vyrocni-zprava-Ceske-skolni-inspekce-2019-2020_zm.pdf (accessed on 7 June 2022).
- Zatloukal, T.; Andrys, O.; Basl, J.; Bláhová, A.; Blažek, R.; Bogdanowicz, R.; Borkovcová, I. Kvalita a efektivita vzdělávání a vzdělávací soustavy ve školním roce 2020/2021: Výroční zpráva České školní inspekce; ČŠI: Praha, Czech Republic, 2021; Available online: https://csicr.cz/CSICR/media/Prilohy/2021_p%c5%99%c3%adlohy/Dokumenty/VZ_CSI_2021_e-verze_22_11.pdf (accessed on 7 June 2022).
- Sleet, D.A. The Global Challenge of Child Injury Prevention. Int. J. Environ. Res. Public Health 2018, 15, 1921. [Google Scholar] [CrossRef]
- Brudvik, C. Child injuries in Bergen, Norway. Inj.-Int. J. Care Inj. 2000, 31, 761–767. [Google Scholar] [CrossRef]
- Mohammed, Z.; Aledhaim, A.; AbdelSalam, E.M.; El-Setouhy, M.; El-Shinawi, M.; Hirshon, J.M. Factors associated with injuries among preschool children in Egypt: Demographic and health survey results, 2014. BMC Public Health 2020, 20, 595. [Google Scholar] [CrossRef]
- Sengoelge, M.; Hasselberg, M.; Laflamme, L. Child home injury mortality in Europe: A 16-country analysis. Eur. J. Public Health 2011, 21, 166–170. [Google Scholar] [CrossRef]
- Institute of Health Information and Statistics (IHIS). ZDRAVÍ 2030—Analytická Studie: Zdravotní Stav Obyvatelstva: Úrazy, Otravy. 2020. Available online: https://zdravi2030.mzcr.cz/zdravi-2030-analyticka-studie-stav-obyvatelsva.pdf (accessed on 17 August 2022).
- Boček, J. Přes 40 Procent Závažných Dětských Úrazů Se Stane Doma. Irozhlas. 2016. Available online: https://www.irozhlas.cz/zpravy-domov/pres-40-procent-zavaznych-detskych-urazu-se-stane-doma_201603270600_jbocek (accessed on 17 August 2022).
- Morrongiello, B.A.; Ondejko, L.; Littlejohn, A. Understanding toddlers’ in-home injuries: II. Examining parental strategies, and their efficacy, for managing child injury risk. J. Pediatr. Psychol. 2004, 29, 433–446. [Google Scholar] [CrossRef]
- Morrongiello, B.A.; Klemencic, N.; Corbett, M. Interactions between child behavior patterns and parent supervision: Implications for children’s risk of unintentional injury. Child Dev. 2008, 79, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Schell, S.L. Child Injury: The Role of Supervision in Prevention. Am. J. Lifestyle Med. 2010, 4, 65–74. [Google Scholar] [CrossRef]
- Zhou, H.-Z.; Fan, L.-J.; Wu, C.-A.; Luo, A.-F.; Mo, C.-Q.; He, G.-H.; Ruan, Z.-L.; Jing, J.; Jin, Y.; Chen, W.-Q. Understanding the associations among parents teaching safety rules to children, safety behaviors and unintentional injuries in Chinese preschool children. Prev. Med. 2019, 118, 98–103. [Google Scholar] [CrossRef]
- Whitehead, E.; Owens, D. Parental perceptions of unintentional injury risks to children. Int. J. Health Promot. Educ. 2012, 50, 20–27. [Google Scholar] [CrossRef]
- Dalal, K.; Lao, Z.Q.; Gifford, M.; Wang, S.M. Knowledge and attitudes towards childhood injury prevention: A study of parents in Shanghai, China. Healthmed 2012, 6, 3783–3789. [Google Scholar]
- Sznajder, M.; Leduc, S.; Janvrin, M.P.; Bonnin, M.H.; Aegerter, P.; Baudier, F.; Chevallier, B. Home delivery of an injury prevention kit for children in four French cities: A controlled randomized trial. Inj. Prev. 2003, 9, 261–265. [Google Scholar] [CrossRef]
- Steiger, J.H.; Fouladi, R.T. Noncentrality interval estimation and the evaluation of statistical models. In What If There Were No Significance Tests; Harlow, L.L., Mulaik, S.A., Steiger, J.H., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1997; pp. 197–229. [Google Scholar]
- Vacha-Haase, T.; Thompson, B. How to Estimate and Interpret Various Effect Sizes. J. Couns. Psychol. 2004, 51, 473–481. [Google Scholar] [CrossRef]
- Likert, R. A Technique for the Measurement of Attitudes; The Science Press: New York, NY, USA, 1932; Volume 22. [Google Scholar]
- Šmejkal, P.; Skoršepa, M.; Stratilová Urválková, E.; Teplý, P. Chemické úlohy se školními měřicími systémy: Motivační orientace žáků v badatelsky orientovaných úlohách. Sci. Educ. 2016, 7, 29–48. [Google Scholar] [CrossRef]
- Vácha, Z.; Ditrich, T. Efektivita badatelsky orientovaného vyučování na primárním stupni základních škol v přírodovědném vzdělávání v České republice s využitím prostředí školních zahrad. Sci. Educ. 2016, 7, 65–79. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Truellová, I. Aktuální údaje úrazovosti dětí v České republice. Prevence Úrazů Otrav A Násilí 2008, 4, 57–61. [Google Scholar]
- Frišová, L.; Coufalová, L.; Soukupová, K.; Kostner, R.; Blažek, J. Úrazy Dětí; Vzdělávací Institut Ochrany Dětí: Prague, Czech Republic, 2006; p. 36. [Google Scholar]
- Pomerantz, W.J.; Gittelman, M.A.; Hornung, R.; Husseinzadeh, H. Falls in children birth to 5 years: Different mechanisms lead to different injuries. J. Trauma Acute Care Surg. 2012, 73, S254–S257. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Lu, G.; Ma, J.; Zheng, J.; Hu, F.; Liu, J.; Song, J.; Hu, S.; Sun, L.; Chen, Y.; et al. Causes and Characteristics of Children Unintentional Injuries in Emergency Department and Its Implications for Prevention. Front. Public Health 2021, 9, 669125. [Google Scholar] [CrossRef] [PubMed]
- Helus, Z. Dítě v Osobnostním Pojetí: Obrat k Dítěti jako Výzva a Úkol Pro Učitele i Rodiče, 2nd rev. and expanded ed.; Portál: Prague, Czech Republic, 2009. [Google Scholar]
- Ball, D.J. Playgrounds-Risks, Benefits and Choices; HSE Books: Sudbury, ON, Canada, 2002.
- Stephenson, A. Physical Risk-taking: Dangerous or endangered? Early Years 2003, 23, 35–43. [Google Scholar] [CrossRef]
- Tovey, H. Playing Outdoors: Spaces and Places, Risk and Challenge: Spaces and Places, Risks and Challenge; McGraw-Hill Education: New York, NY, USA, 2007. [Google Scholar]
- Nikiforidou, Z. ‘It is riskier’: Preschoolers’ reasoning of risky situations. Eur. Early Child. Educ. Res. J. 2017, 25, 612–623. [Google Scholar] [CrossRef]
- Smith, S.J. Risk and Our Pedagogical Relation to Children: On the Playground and Beyond; State University of New York Press: New York, NY, USA, 1998. [Google Scholar]
- Sandseter, E.B.H. Categorising risky play—How can we identify risk-taking in children’s play? Eur. Early Child. Educ. Res. J. 2007, 15, 237–252. [Google Scholar] [CrossRef]
- Lavrysen, A.; Bertrands, E.; Leyssen, L.; Smets, L.; Vanderspikken, A.; De Graef, P. Risky-play at school. Facilitating risk perception and competence in young children. Eur. Early Child. Educ. Res. J. 2017, 25, 89–105. [Google Scholar] [CrossRef]
- MacQuarrie, M.; McIsaac, J.-L.D.; Cawley, J.; Kirk, S.F.L.; Kolen, A.M.; Rehman, L.; Spencer, R.A.; Stone, M.R. Exploring parents’ perceptions of preschoolers’ risky outdoor play using a socio-ecological lens. Eur. Early Child. Educ. Res. J. 2022, 30, 372–387. [Google Scholar] [CrossRef]
- Peterson, L.; Mori, L. Prevention of child injury: An overview of targets, methods, and tactics for psychologists. J. Consult. Clin. Psychol. 1985, 53, 586–595. [Google Scholar] [CrossRef]
- Lagerberg, D. Secondary prevention in child health: Effects of psychological intervention, particularly home visitation, on children’s development and other outcome variables. Acta Paediatr. 2000, 89, 43–52. [Google Scholar] [CrossRef]
- Kendrick, D.; Mulvaney, C.A.; Ye, L.; Stevens, T.; Mytton, J.A.; Stewart-Brown, S. Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane Database Syst. Rev. 2013, 2013, Cd006020. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).