
Maladaptive Cognitions in Adolescents and Young Adults When They Play: The Dysfunctional Cognitions in Gaming Scale (DCG)
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Dysfunctional Cognitions in Gaming Scale (DCG Scale)
2.2.2. Internet Gaming Disorder Scale—Short-Form, IGDS9-SF
2.2.3. General Health Questionnaire, GHQ-12
2.2.4. Frequency of Gameplay
2.3. Procedure
2.4. Data Analysis
2.4.1. Item Analysis
2.4.2. Factorial Validity
2.4.3. Measurement Invariance
2.4.4. Reliability
2.4.5. Other Evidence of Validity
2.5. Transparency and Openness
3. Results
3.1. Item Analysis
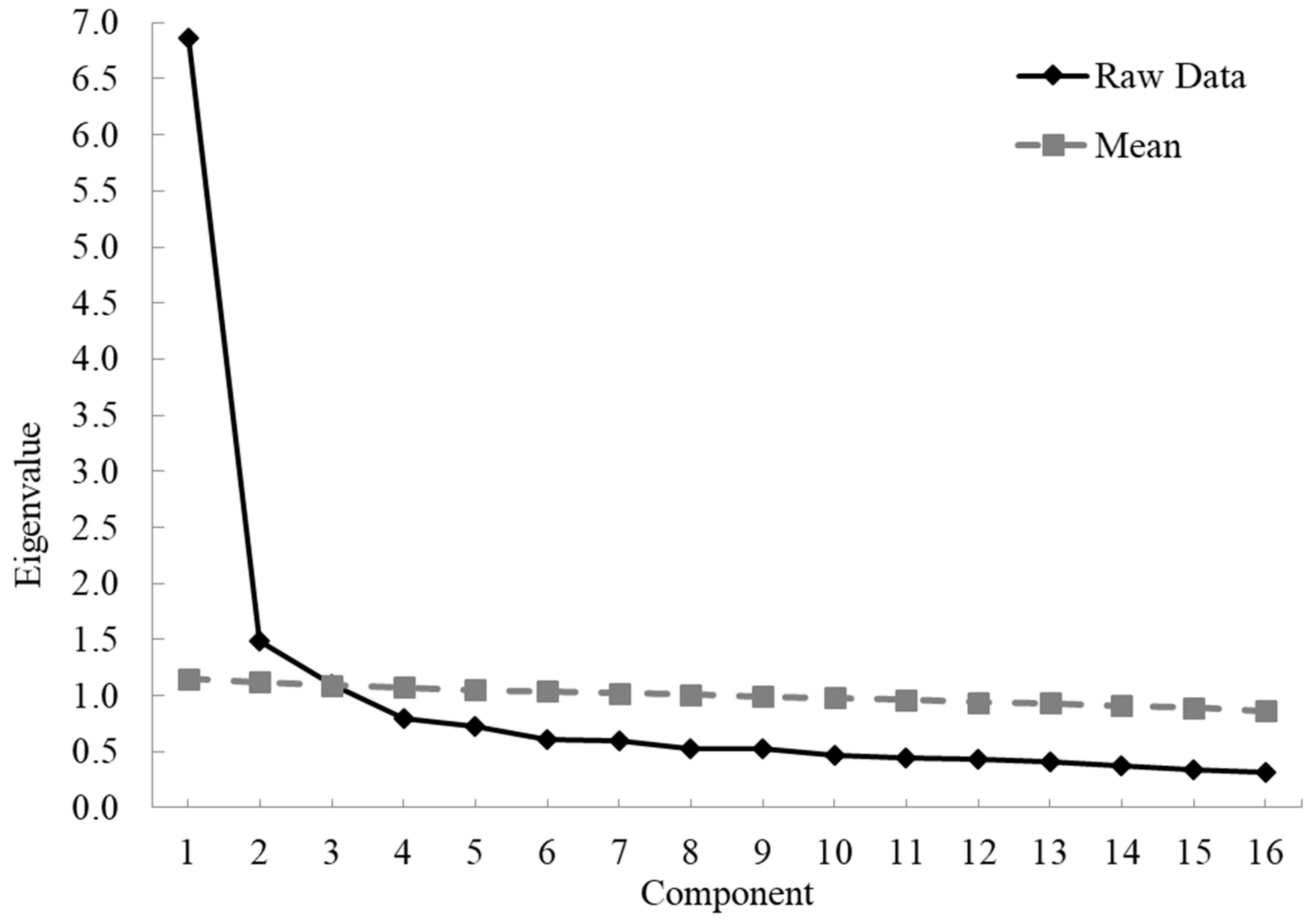
3.2. EFA
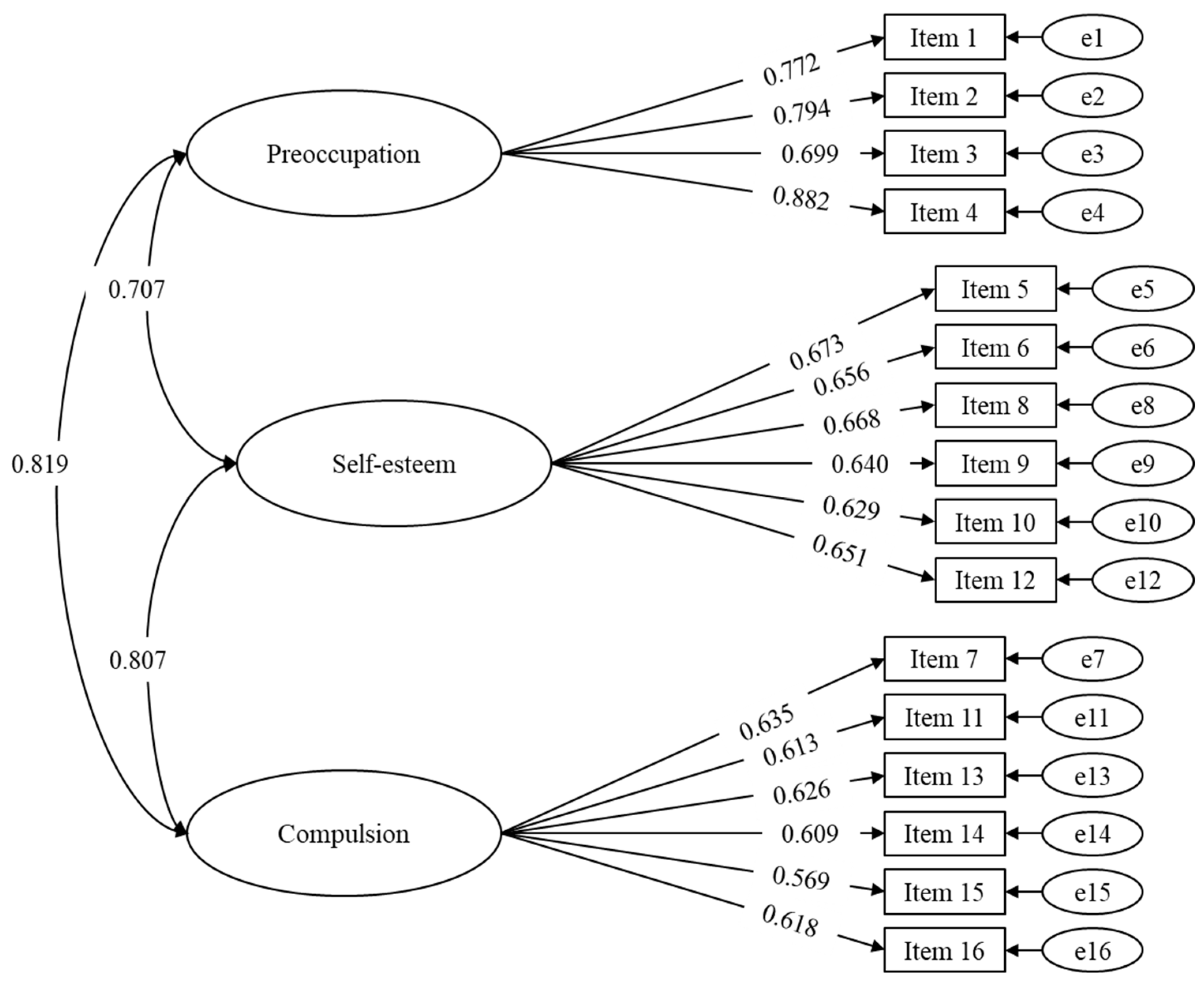
3.3. CFA
3.4. Measurement Invariance
3.5. Reliability
3.6. Other Evidence of Validity
3.6.1. Frequency of Playing Video Games
3.6.2. GHQ-12 and IGDS9-SF
3.7. Scale Scores and Percentile Ranks
4. Discussion
4.1. Maladaptive Cognitions, Gaming Frequency, Perceived Health, and Problems Using VGs
4.2. Implications for Evaluation and Intervention
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NewZoo Engagement and Revenues Continue to Thrive Across the Global Games Market. Global Games Market Report. 2020. Available online: https://newzoo.com/insights/articles/games-market-engagement-revenues-trends-2020-2023-gaming-report (accessed on 1 November 2022).
- Gong, X.; Chen, C.; Lee, M.K. What drives problematic online gaming? The role of IT identity, maladaptive cognitions, and maladaptive emotions. Comput. Hum. Behav. 2020, 110, 106386. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems (ICD); World Health Organization (WHO): Geneva, Switzerland, 2018.
- Davis, R. A cognitive-behavioral model of pathological Internet use. Comput. Hum. Behav. 2001, 17, 187–195. [Google Scholar] [CrossRef]
- Caplan, S.E. Preference for Online Social Interaction: A Theory of Problematic Internet Use and Psychosocial Well-Being. Commun. Res. 2003, 30, 625–648. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H. The cognitive psychology of Internet gaming disorder. Clin. Psychol. Rev. 2014, 34, 298–308. [Google Scholar] [CrossRef] [Green Version]
- King, D.L.; Delfabbro, P.H. The Cognitive Psychopathology of Internet Gaming Disorder in Adolescence. J. Abnorm. Child Psychol. 2016, 44, 1635–1645. [Google Scholar] [CrossRef] [PubMed]
- Moudiab, S.; Spada, M.M. The relative contribution of motives and maladaptive cognitions to levels of Internet Gaming Disorder. Addict. Behav. Rep. 2019, 9, 100160. [Google Scholar] [CrossRef]
- Bodi, G.; Maintenant, C.; Pennequin, V. The role of maladaptive cognitions in gaming disorder: Differences between online and offline gaming types. Addict. Behav. 2021, 112, 106595. [Google Scholar] [CrossRef]
- Forrest, C.J.; King, D.L.; Delfabbro, P.H. The measurement of maladaptive cognitions underlying problematic video-game playing among adults. Comput. Hum. Behav. 2016, 55, 399–405. [Google Scholar] [CrossRef]
- Forrest, C.J.; King, D.L.; Delfabbro, P.H. Maladaptive cognitions predict changes in problematic gaming in highly-engaged adults: A 12-month longitudinal study. Addict. Behav. 2017, 65, 125–130. [Google Scholar] [CrossRef]
- Yu, Y.; Mo, P.K.-H.; Zhang, J.; Li, J.; Lau, J.T.-F. Validation of the Chinese Version of the Revised Internet Gaming Cognition Scale among Adolescents in China: Maladaptive Cognitions as Potential Determinants of Internet Gaming Disorder. Int. J. Environ. Res. Public Health 2019, 17, 290. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. El análisis factorial exploratorio de los ítems: Una guía práctica, revisada y actualizada. An. Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Sánchez-Iglesias, I.; Bernaldo-De-Quirós, M.; Labrador, F.J.; Puig, F.J.E.; Labrador, M.; Fernández-Arias, I. Spanish Validation and Scoring of the Internet Gaming Disorder Scale–Short-Form (IGDS9-SF). Span. J. Psychol. 2020, 23, e22. [Google Scholar] [CrossRef] [PubMed]
- Pontes, H.M.; Griffiths, M.D. Measuring DSM-5 internet gaming disorder: Development and validation of a short psychometric scale. Comput. Hum. Behav. 2015, 45, 137–143. [Google Scholar] [CrossRef] [Green Version]
- López-Castedo, A.; Fernández, L. Psychometric Properties of the Spanish Version of the 12-Item General Health Questionnaire in Adolescents. Percept. Mot. Ski. 2005, 100, 676–680. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Labrador, F.J.; Bernaldo-de-Quirós, M.; Labrador, M.; Fernández-Arias, I.; Estupiñá, F.J.; González-Álvarez, M.; Sánchez-Iglesias, I.; Vallejo-Achón, M. Internet Gaming Disorder in Children and Adolescents. 2021. Available online: https://osf.io/nrv45/ (accessed on 1 November 2022).
- Comunidad Autónoma de Madrid Buscador de Centros Educativos [Educative Centers Search Engine] 2017. Available online: http://www.madrid.org/wpad_pub/run/j/MostrarConsultaGeneral.icm (accessed on 1 November 2022).
- Korkmaz, S.; Goksuluk, D.; Zararsiz, G. MVN: An R Package for Assessing Multivariate Normality. R J. 2014, 6, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Kelley, K. MBESS: The MBESS R Package, R Package Version 4.4.3; 2018. Available online: www.cran.r-project.org/package=MBESS (accessed on 1 November 2022).
- Revelle, W. Psych: Procedures for Personality and Psychological Research. 2018. Available online: https://CRAN.R-project.org/package=psych (accessed on 1 November 2022).
- Dueber, D.M. Bifactor Indices Calculator 2017. Available online: https://github.com/ddueber/BifactorIndicesCalculator (accessed on 1 November 2022).
- Jorgensen, T.D.; Pornprasertmanit, S.; Schoemann, A.M.; Rosseel, Y. SemTools: Useful Tools for Structural Equation Modeling. R Package Version 0.5-1. 2018. Available online: https://github.com/simsem/semTools/wiki (accessed on 1 November 2022).
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Mardia, K.V. Measures of multivariate skewness and kurtosis with applications. Biometrika 1970, 57, 519–530. [Google Scholar] [CrossRef]
- Chau, P.Y. Reexamining a Model for Evaluating Information Center Success Using a Structural Equation Modeling Approach. Decis. Sci. 1997, 28, 309–334. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015; pp. 1–462. ISBN 978-1-4625-1779-4. [Google Scholar]
- Reise, S.P. The Rediscovery of Bifactor Measurement Models. Multivar. Behav. Res. 2012, 47, 667–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reise, S.P.; Scheines, R.; Widaman, K.; Haviland, M.G. Multidimensionality and Structural Coefficient Bias in Structural Equation Modeling: A Bifactor Perspective. Educ. Psychol. Meas. 2012, 73, 5–26. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- McDonald, R.P. Test Theory: A Unified Treatment; L. Erlbaum Associates: Mahwah, NJ, USA, 1999; ISBN 978-0-8058-3075-0. [Google Scholar]
- Appelbaum, M.; Cooper, H.; Kline, R.B.; Mayo-Wilson, E.; Nezu, A.M.; Rao, S.M. Journal article reporting standards for quantitative research in psychology: The APA Publications and Communications Board task force report. Am. Psychol. 2018, 73, 3–25. [Google Scholar] [CrossRef]
- Marino, C.; Spada, M.M. Dysfunctional Cognitions in Online Gaming and Internet Gaming Disorder: A Narrative Review and New Classification. Curr. Addict. Rep. 2017, 4, 308–316. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H. Treatment for IGD. In Internet Gaming Disorder; Elsevier: Amsterdam, The Netherlands, 2018; pp. 163–199. ISBN 978-0-12-812924-1. [Google Scholar]
- Kuss, D.J.; Pontes, H.M. Internet Addiction; Advances in Psychotherapy—Evidence-Based Practice; Hogrefe: Boston, MA, USA, 2019; ISBN 978-0-88937-501-7. [Google Scholar]

{kind=link}
{kind=link}
| # | Item | M | SD | Mdn | IQR | Sk | K |
|---|---|---|---|---|---|---|---|
| 1 | I find myself thinking about video games when I’m not playing [Me encuentro pensando en videojuegos cuando no estoy jugando] | 1.0 | 0.9 | 1 | 2 | 0.8 | 0.3 |
| 2 | I say to myself “I wish I was playing right now” [Me digo “ojalá en este momento estuviera jugando”] | 1.0 | 1.0 | 1 | 2 | 0.9 | 0.3 |
| 3 | I couldn’t stand to wait much longer without playing [No soportaría esperar mucho más tiempo sin jugar] | 0.6 | 0.8 | 0 | 1 | 1.8 | 3.5 |
| 4 | I plan or think about what I will do next in the game to advance [Planeo o pienso lo siguiente que haré en el juego para avanzar] | 1.3 | 1.2 | 1 | 2 | 0.6 | −0.7 |
| 5 | I won’t stop until I get past it. Better now than tomorrow [No pararé hasta conseguir pasármelo. Mejor ahora que mañana] | 1.3 | 1.2 | 1 | 2 | 0.7 | −0.4 |
| 6 | This game, or these rivals, are not going to be able to beat me, I am better [Este juego o estos rivales no van a poder conmigo, yo soy mejor] | 1.5 | 1.3 | 1 | 2 | 0.5 | −0.8 |
| 7 | Stopping playing now will be a failure [Dejar de jugar ahora será un fracaso] | 0.8 | 1.0 | 0 | 1 | 1.4 | 1.6 |
| 8 | I cannot fail. Other players admire and respect my achievements in the game [No puedo fallar. Otros jugadores admiran y respetan mis logros en el juego] | 0.8 | 1.1 | 0 | 1 | 1.3 | 0.8 |
| 9 | I am very good and I feel good [Soy muy bueno y me siento bien] | 2.1 | 1.2 | 2 | 2 | 0.0 | −0.8 |
| 10 | I am better than the others [Soy mejor que otros] | 1.4 | 1.3 | 1 | 2 | 0.6 | −0.7 |
| 11 | I don’t want to know anything that happens around me, it’s secondary [No quiero saber nada de lo que ocurre a mi alrededor, es secundario] | 0.7 | 1.0 | 0 | 1 | 1.4 | 1.7 |
| 12 | It’s great to be able to spend time enjoying with these people [Es genial poder disfrutar de pasar tiempo con toda esta gente] | 2.2 | 1.2 | 2 | 2 | −0.2 | −0.8 |
| 13 | I think people who don’t play video games don’t understand me [Pienso que las personas que no juegan a videojuegos no me entienden] | 0.9 | 1.1 | 1 | 1 | 1.2 | 0.6 |
| 14 | I tell myself “just a few more minutes”, but then it’s much longer [Me digo a mí mismo “solo unos minutos más” pero luego es mucho más tiempo] | 1.5 | 1.2 | 1 | 1 | 0.5 | −0.7 |
| 15 | I don’t care at all how they react, I’m not going to stop [Me da exactamente igual como se pongan no voy a parar] | 0.4 | 0.8 | 0 | 1 | 2.2 | 4.7 |
| 16 | If I stop playing I will feel bad [Si dejo de jugar voy a sentirme mal] | 0.4 | 0.7 | 0 | 0 | 2.6 | 7.3 |
| Factor Loading | |||
|---|---|---|---|
| Item | Preoccupation | Self-Esteem | Compulsion |
| 1 | 0.801 | 0.461 | 0.585 |
| 2 | 0.808 | 0.467 | 0.569 |
| 3 | 0.706 | 0.387 | 0.649 |
| 4 | 0.748 | 0.484 | 0.490 |
| 5 | 0.568 | 0.616 | 0.589 |
| 6 | 0.421 | 0.788 | 0.498 |
| 7 | 0.520 | 0.571 | 0.661 |
| 8 | 0.505 | 0.644 | 0.625 |
| 9 | 0.425 | 0.759 | 0.399 |
| 10 | 0.365 | 0.688 | 0.446 |
| 11 | 0.421 | 0.515 | 0.647 |
| 12 | 0.562 | 0.589 | 0.399 |
| 13 | 0.569 | 0.509 | 0.675 |
| 14 | 0.562 | 0.434 | 0.579 |
| 15 | 0.456 | 0.415 | 0.727 |
| 16 | 0.483 | 0.348 | 0.686 |
| Grouping Variable | Invariance Model | χ2 | df | Δχ2 | p (Δχ2) | CFI | ΔCFI | RMSEA | ΔRMSEA |
|---|---|---|---|---|---|---|---|---|---|
| Age | Configural | 1738.7 | 202 | - | - | 0.902 | - | 0.082 | - |
| Metric | 1803.8 | 215 | 60.034 | <0.001 | 0.899 | −0.003 | 0.081 | −0.001 | |
| Scalar | 1966.7 | 228 | 235.978 | <0.001 | 0.889 | −0.010 | 0.082 | 0.002 | |
| Gender | Configural | 1762.2 | 202 | - | - | 0.894 | - | 0.082 | - |
| Metric | 1827.0 | 215 | 48.534 | <0.001 | 0.890 | −0.003 | 0.080 | −0.001 | |
| Scalar | 2008.0 | 228 | 220.819 | <0.001 | 0.878 | −0.012 | 0.082 | 0.002 |
| α [95% CI] | ω [95% CI] | Rxx | |
|---|---|---|---|
| All 16 items | 0.907 [0.899, 0.915] | 0.908 [0.900, 0.914] | 0.91 |
| Preoccupation (4 items) | 0.843 [0.828, 0.855] | 0.849 [0.832, 0.859] | 0.85 |
| Self-esteem (6 items) | 0.829 [0.815, 0.838] | 0.832 [0.819, 0.845] | 0.83 |
| Compulsion (6 items) | 0.799 [0.779, 0.818] | 0.800 [0.784, 0.816] | 0.81 |
| IGDS9-SF | GHQ Total | GHQ Anxiety | GHQ Dysfunction | |
|---|---|---|---|---|
| DCG Total score | 0.697 | 0.200 | 0.165 | 0.060 |
| Preoccupation | 0.658 | 0.125 | 0.078 | 0.076 |
| Self-esteem | 0.535 | 0.199 | 0.134 | 0.107 |
| Compulsion | 0.658 | 0.182 | 0.210 | −0.036 ns |
| Male | Female | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 12 to 16 | 17 to 22 | 12 to 16 | 17 to 22 | 12 to 16 | 17 to 22 | 12 to 16 | 17 to 22 | ||
| (n = 1025) | (n = 522) | (n = 491) | (n = 135) | (n = 1025) | (n = 522) | (n = 491) | (n = 135) | ||
| Score | Percentile | Percentile | Score | Percentile | Percentile | ||||
| 0 | 1 | 1 | 6 | 4 | 33 | 88 | 93 | 97 | 98 |
| 1 | 1 | 3 | 8 | 10 | 34 | 89 | 93 | 97 | 99 |
| 2 | 1 | 4 | 14 | 15 | 35 | 90 | 95 | 98 | 99 |
| 3 | 2 | 5 | 18 | 22 | 36 | 91 | 95 | 98 | 99 |
| 4 | 3 | 8 | 25 | 26 | 37 | 92 | 95 | 98 | 99 |
| 5 | 5 | 9 | 29 | 33 | 38 | 94 | 95 | 98 | 99 |
| 6 | 7 | 11 | 34 | 36 | 39 | 95 | 97 | 98 | 99 |
| 7 | 10 | 13 | 41 | 43 | 40 | 95 | 97 | 99 | 99 |
| 8 | 12 | 16 | 45 | 48 | 41 | 96 | 98 | 99 | 99 |
| 9 | 15 | 19 | 51 | 56 | 42 | 96 | 98 | 99 | 99 |
| 10 | 18 | 22 | 57 | 58 | 43 | 97 | 99 | 99 | 99 |
| 11 | 20 | 26 | 61 | 61 | 44 | 98 | 99 | 99 | 99 |
| 12 | 23 | 28 | 62 | 65 | 45 | 98 | 99 | 99 | 99 |
| 13 | 27 | 32 | 66 | 66 | 46 | 98 | 99 | 99 | 99 |
| 14 | 30 | 37 | 69 | 70 | 47 | 98 | 99 | 99 | 99 |
| 15 | 34 | 39 | 72 | 73 | 48 | 98 | 99 | 99 | 99 |
| 16 | 37 | 42 | 75 | 76 | 49 | 98 | 99 | 100 | 99 |
| 17 | 41 | 46 | 76 | 77 | 50 | 98 | 99 | 100 | 99 |
| 18 | 45 | 49 | 81 | 82 | 51 | 99 | 100 | 100 | 99 |
| 19 | 49 | 54 | 82 | 83 | 52 | 99 | 100 | 100 | 99 |
| 20 | 53 | 57 | 84 | 84 | 53 | 99 | 100 | 100 | 99 |
| 21 | 57 | 63 | 85 | 84 | 54 | 99 | 100 | 100 | 99 |
| 22 | 60 | 69 | 86 | 85 | 55 | 99 | 100 | 100 | 99 |
| 23 | 63 | 72 | 87 | 86 | 56 | 99 | 100 | 100 | 99 |
| 24 | 67 | 75 | 88 | 90 | 57 | 99 | 100 | 100 | 99 |
| 25 | 70 | 77 | 90 | 93 | 58 | 99 | 100 | 100 | 99 |
| 26 | 74 | 78 | 91 | 95 | 59 | 99 | 100 | 100 | 99 |
| 27 | 77 | 83 | 92 | 95 | 60 | 99 | 100 | 100 | 99 |
| 28 | 80 | 85 | 93 | 95 | 61 | 100 | 100 | 100 | 99 |
| 29 | 81 | 87 | 93 | 95 | 62 | 100 | 100 | 100 | 99 |
| 30 | 83 | 89 | 94 | 96 | 63 | 100 | 100 | 100 | 99 |
| 31 | 85 | 91 | 95 | 97 | 64 | 100 | 100 | 100 | 100 |
| 32 | 87 | 92 | 96 | 97 | |||||
| Gender | Age | n | M | SD | Mdn | IQR | Min | Max | Sk | K |
|---|---|---|---|---|---|---|---|---|---|---|
| Male | 12 to 16 | 1025 | 20.88 | 10.95 | 20 | 14 | 0 | 64 | 0.8 | 1.06 |
| 17 to 22 | 522 | 18.71 | 10.07 | 19 | 13.8 | 0 | 61 | 0.55 | 0.59 | |
| Female | 12 to 16 | 491 | 11.85 | 9.84 | 9 | 12 | 0 | 60 | 1.4 | 2.55 |
| 17 to 22 | 135 | 11.34 | 9.75 | 9 | 12 | 0 | 64 | 1.71 | 5.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Iglesias, I.; Bernaldo-de-Quirós, M.; Estupiñá, F.J.; Fernández-Arias, I.; Labrador, M.; Vallejo-Achón, M.; Saiz, J.; Labrador, F.J. Maladaptive Cognitions in Adolescents and Young Adults When They Play: The Dysfunctional Cognitions in Gaming Scale (DCG). Sustainability 2022, 14, 16109. https://doi.org/10.3390/su142316109
Sánchez-Iglesias I, Bernaldo-de-Quirós M, Estupiñá FJ, Fernández-Arias I, Labrador M, Vallejo-Achón M, Saiz J, Labrador FJ. Maladaptive Cognitions in Adolescents and Young Adults When They Play: The Dysfunctional Cognitions in Gaming Scale (DCG). Sustainability. 2022; 14(23):16109. https://doi.org/10.3390/su142316109
Chicago/Turabian StyleSánchez-Iglesias, Iván, Mónica Bernaldo-de-Quirós, Francisco J. Estupiñá, Ignacio Fernández-Arias, Marta Labrador, Marina Vallejo-Achón, Jesús Saiz, and Francisco J. Labrador. 2022. "Maladaptive Cognitions in Adolescents and Young Adults When They Play: The Dysfunctional Cognitions in Gaming Scale (DCG)" Sustainability 14, no. 23: 16109. https://doi.org/10.3390/su142316109