
The COVID-19 Pandemic Response and Its Impact on Post-Pandemic Health Emergency and Disaster Risk Management in the United States

1
School of Medicine, Johns Hopkins University, Baltimore, MD 21205, USA
2
Department of International Health, Johns Hopkins University, Baltimore, MD 21205, USA
3
Center for Global Emergency Care, Johns Hopkins University, Baltimore, MD 21205, USA
4
Office of Critical Event Preparedness and Response, Johns Hopkins University, Baltimore, MD 21209, USA
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(23), 16301; https://doi.org/10.3390/su142316301
Submission received: 20 October 2022
/
Revised: 24 November 2022
/
Accepted: 1 December 2022
/
Published: 6 December 2022
(This article belongs to the Special Issue Public Health and Health Emergency Disaster Risk Management during and Post COVID-19 Era)
Abstract
:Among the impacts of the Coronavirus Disease 2019 (COVID-19) pandemic on the public health system in the United States has been a reevaluation of emergency response systems and procedures. This study uses publicly available literature from government, private sector, and academic sources to identify changes and lessons learned during the COVID-19 pandemic in specific aspects of emergency response, namely human resources, health service delivery, and logistics, determined based on the World Health Organization Health Emergency and Disaster Risk Management (WHO Health EDRM) Framework. Major themes of changes implemented include those intended to increase mobility and flexibility of workforce and resources, integration of various parts of the health system, and effective communication, and are anticipated to be incorporated into response systems going forward.
1. Introduction
Coronavirus Disease 2019 (COVID-19) overwhelmed the health system in the United States (US) and changed emergency response operations. As of the end of July 2022, over 90,000,000 cases of COVID-19 have been reported in the US, with over 1,000,000 deaths [1]. Additionally, as of July 2022, the surveillance network COVID-NET reported a cumulative case count of over 345,000 COVID-19-associated hospitalizations within their network, which encompasses approximately 10% of the population of the US [2]. The notable scale of the pandemic’s impact on health system utilization has prompted a critical examination of our response capacity and coordination strategies.
This US-based case study focuses on COVID-19 responses in the World Health Organization (WHO) Health Emergency and Disaster Risk Management (Health EDRM) Framework. Released in 2019 and developed by WHO experts and administration with the collaboration of WHO Member States and partner organizations, this Framework is a consolidated and comprehensive high-level resource for emergency and disaster preparedness and management. While its focus is on the health sector, it emphasizes the necessity of cross-sector collaboration and draws from the experiences of numerous sectors involved in emergency response [3]. The Health EDRM Framework is also intended to be synergistic with other frameworks developed earlier, including the Sendai Framework for Disaster Risk Reduction 2015–2030, which set up a multisectoral “all-hazards approach” to Disaster Risk Management, including health-related disasters [4]. Action taken toward one framework should also contribute to advancing the goals of another.
The ten components of the Health EDRM Framework, each of which encompasses specific functions, are the following: (i) policies, strategies and legislation; (ii) planning and coordination; (iii) human resources; (iv) financial resources; (v) information and knowledge management; (vi) risk communications; (vii) health infrastructure and logistics; (viii) health and related services; (ix) community capacities for Health EDRM; and (x) monitoring and evaluation [3]. This study examines aspects of the COVID-19 response that relate to three selected components which pertain most directly to healthcare delivery: (iii) human resources; (vii) health infrastructure and logistics; and (viii) health and related services. The objective of this study is an examination of the US COVID-19 response using the structured health emergency and Disaster Risk Management framework to inform opportunities for strengthening future pandemic response.
We sought to answer the following key questions: (1) What difficulties and challenges has your country experienced during COVID-19 in terms of human resources, health service delivery and logistics? (2) How did your country respond to and deal with these challenges? (3) What did you learn from the current COVID-19 pandemic to prepare for the future response regarding human resources, health service delivery and logistics? (4) What influence have these challenges and responses had on the present and post-coronavirus Health-EDRM system, particularly on human resources, health service delivery and logistics? These key questions were formulated to investigate the practical national-level challenges encountered in responding to COVID-19, focusing on the most critical aspects of healthcare delivery and to better understand how a future pandemic response might be modified or adapted.
2. Materials and Methods
This is a grey literature review of publicly available information focused on the US COVID-19 pandemic response.
2.1. Search Strategy
Information was drawn from numerous official and non-official sources, inclusive of the period from 11 March 2020, when WHO declared COVID-19 a pandemic, through 1 August 2022, generated by the search terms “challenges”, “response” and “lessons learned” in combination with “COVID” and “human resources”, “health service delivery” and “logistics” using Google search tools. Individual topics, legislation, organizations, and initiatives that emerged from these aforementioned searches were then themselves used as keywords in Google search tools. Publicly available official documents in English from major relevant governmental agencies including the White House, Department of Health and Human Services (HHS), the Centers for Disease Control and Prevention (CDC), advisory committees including the Bipartisan Committee on Biodefense, the National Academies of Science, Engineering and Medicine (NASEM), medical associations such as the American Hospital Association (AHA), American Medical Association (AMA), consultancies such as McKinsey, and peer-reviewed journals, were identified, reviewed and summarized. Designated as authoritative sources by the team, these reflect official positions from government agencies, peer-reviewed conclusions from academic studies, and stances from recognized consulting bodies and other national and international organizations. Articles from recognized news organizations, such as National Public Radio (NPR), The New York Times, and Reuters were included, when relevant, to illustrate current events and contemporary reactions to them.
2.2. Data Abstraction
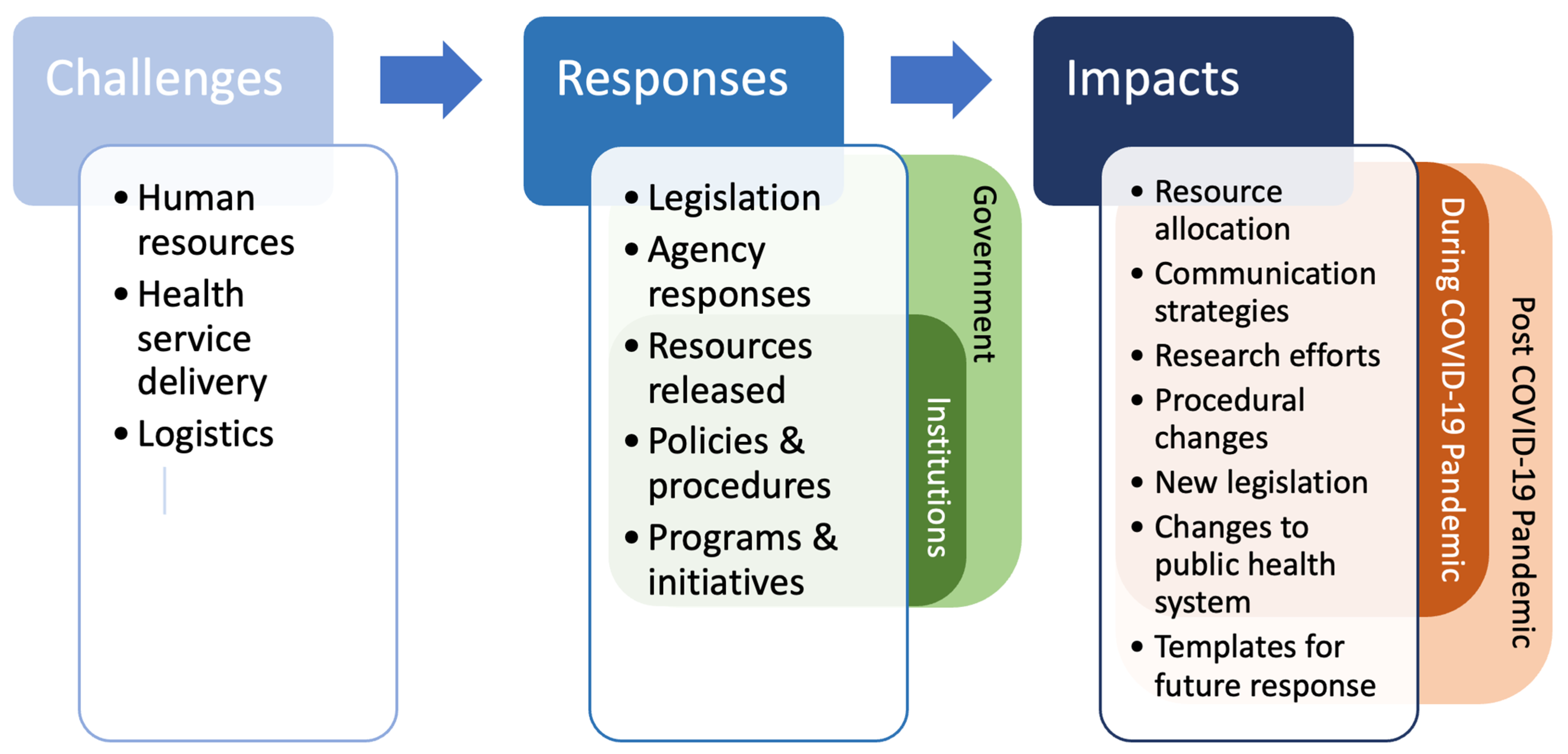
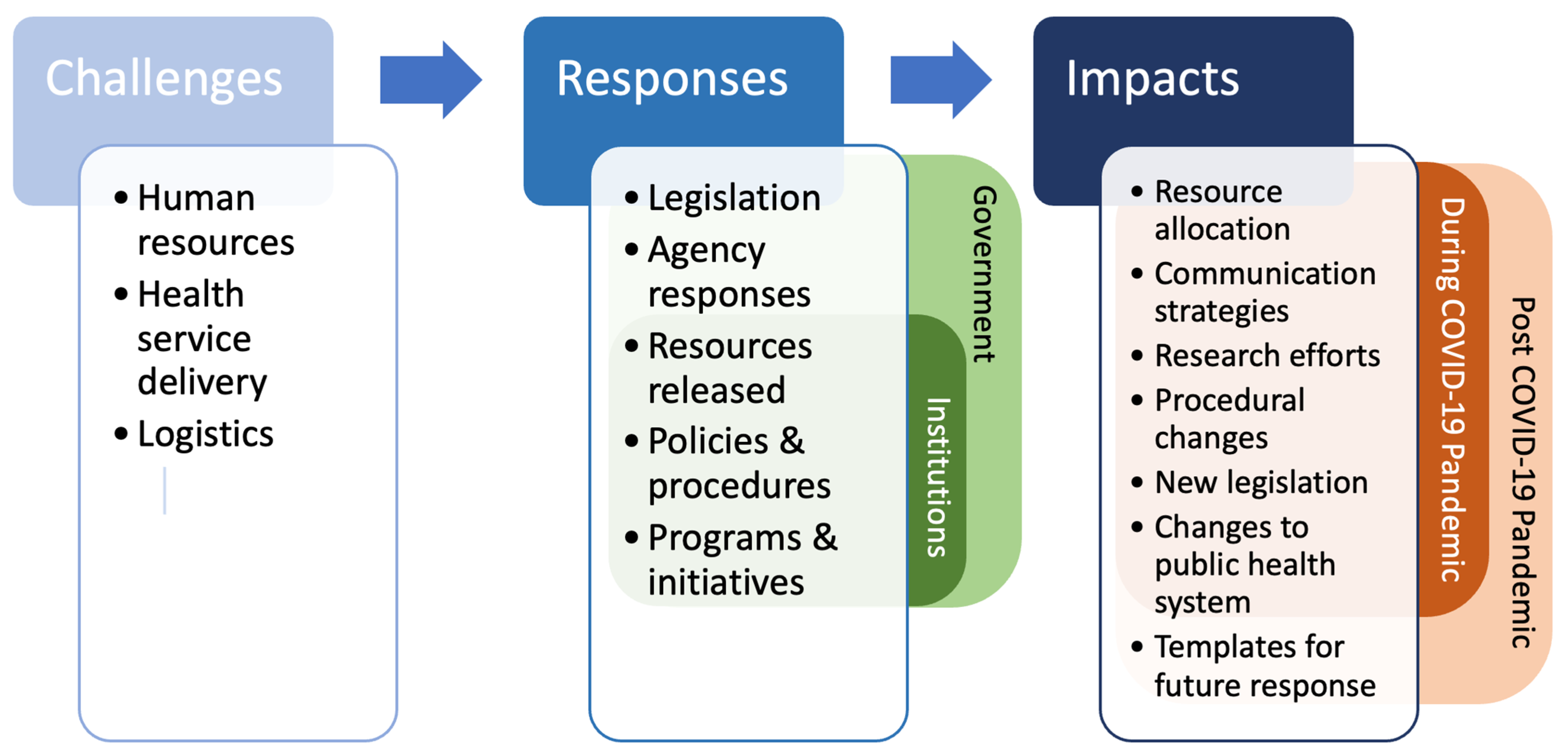
Data was abstracted using a structured template based upon the Health EDRM Framework developed by the WHO. The team extracted, collated and contextualized country level COVID-19 responses, and the continuing implementation of these responses, to challenges that could be categorized as related to human resources, health service delivery, and logistics. The organization of the findings, using the analytic framework noted in Figure 1, will be further discussed in the Results section. The Standards for Reporting Qualitative Research were taken into account and incorporated, with the exception of those standards that apply to research with human participants, which this study does not involve [5].
3. Results
Our analysis draws from around 80 publicly available data sources, ranging in time of publication from 2019, before the COVID-19 pandemic began in the US, to mid-2022. The plurality are resources published by US government entities, including the CDC, HHS, and the White House. Original research articles published in peer-reviewed journals, reports and statements from private sector organizations including the AHA, and articles published by news media organizations make up the majority of the remaining sources from which data were drawn. Most of the resources deal with health service delivery, due to the wide variety of topics with relevance to that subject.
The results are separated into three sections, each focusing on one Health EDRM component: human resources, followed by health service delivery, followed by logistics. Each section is subdivided into the relevant major challenges within those three components. As outlined in Figure 1, following each challenge is a discussion of the response to that challenge, whether governmental, by institutions, or both, followed by the immediate and ongoing implementation and impacts of those responses.
A summary of our findings is provided in Table 1 below:
3.1. Human Resources
3.1.1. Personnel Shortage
The magnitude of the outbreak in the US, in terms of numbers of people and the geographic range affected, placed a severe burden on healthcare workers, emergency responders, and medical laboratory personnel. In particular, there were notable shortages in respiratory therapists and ICU-trained nurses [6,7]. At the same time, when elective procedures were paused to free up capacity for anticipated COVID-19 cases, hospitals experienced revenue drops, which led to layoffs and furloughs of non-COVID focused healthcare workers [8].
Most facilities augmented the COVID workforce by cross-training staff or redeploying healthcare workers to different cities, for example, to New York City during the surge at the beginning of the pandemic [7,9,10,11]. Military medical teams were also deployed, as well as non-clinical staff, such as the National Guard, across various states, including New York, Michigan, Ohio, and Missouri throughout the pandemic [12,13]. Short-term staffing needs were filled by premium contractual workers, which, in the long run, caused staffing shortages elsewhere [6,14]. There were also efforts to recruit non-medical private citizens as contact tracers and volunteers at testing and vaccination sites, in roles for which they could be quickly and effectively trained [15,16,17,18].
Shortages of healthcare workers during the pandemic emphasized the importance of personnel surge capacity, and flexibility. Ways to address this include increasing the number of trained personnel as a whole, which can be supported through more investment in, and expansion of, training pipelines for doctors, nurses, and other healthcare professionals [6]. It also includes developing plans and strategies for cross-training to alleviate specific shortages. For example, toward the start of the pandemic, the Community HealthCare System in Onaga, Kansas created a working group to keep track of skill set availability and “cross-training potential” [19]. A nurse educator from Rochester, New York described creating resources such as booklets for nurses with less experience in critical care, and cross-training nurses in preparation for a surge in intensive care unit (ICU) needs [20]. For certain less technical roles, individuals without a clinical background can be trained to reduce the burden on clinical staff. The use of non-clinical individuals in roles such as contact tracers during the pandemic has helped establish a precedent.
3.1.2. Support of Healthcare Workers
Support of healthcare workers is also critical. Healthcare workers during the pandemic faced numerous physical and mental challenges due to increased workloads, constant exposure to infection, and the toll of caring for critically ill COVID-19 patients. Shortages of personal protective equipment exacerbated this, as did social responses, such as skepticism of the existence of the disease and misinformation surrounding treatments, which led to hostility against medical professionals [10,21]. In a nationwide 2020 study of healthcare workers, almost 50% of respondents reported burnout [22].
There were efforts to support healthcare workers physically, logistically, and financially, and to mitigate burnout. Hospitals made testing available for personnel, and healthcare workers were given priority when the vaccine was released [23]. The use of telemedicine was expanded to reduce provider exposure [24]. Programs were established, including by hospitals and state governments, to provide childcare, transportation, meals, and laundry services for healthcare workers, as well as financial bonuses and help with student loans [14,24]. Additionally, some hospitals offered counseling services, and the American Rescue Plan Act is making over $100 million available through funding opportunities intended to address healthcare worker mental health [25].
Programs to help healthcare workers with logistics, childcare, food, and finances are resources and services that organizations and employers can provide in future situations. Lack of childcare, especially due to school closures, was a notable stressor that influenced individuals’ decisions to leave clinical roles and should be considered [26]. Personnel and their families’ physical safety can be addressed by stockpiling personal protective equipment (PPE) in advance of emergencies and making testing readily available. The mental health of clinical staff can be supported by identifying stressors such as fear of exposure to infection, work overload, and feeling unvalued or unsupported by the organization, and addressing these at an institutional level [27]. The attrition rate of healthcare workers during the pandemic and continuing to the present day is strongly cautionary for institutions to solicit and respond to the concerns of their workforce; an AMA study reported that employees who felt valued by their institutions were 40% less likely to report burnout [27]. It should also prompt expansion of healthcare professional training pipelines to alleviate shortages that are impending or have already developed [28,29,30,31].
3.2. Health Service Delivery
3.2.1. Testing and Surveillance
The response to the COVID-19 pandemic was challenging from a public health and clinical standpoint. Public health issues included testing and surveillance. Toward the beginning of the pandemic, there was a shortage of available and accessible testing, including a lack of at-home testing options [32]. Surveillance and case reporting was also limited initially, with only a small number of states and healthcare facilities using Electronic Case Reporting (eCR). This automated system transmits information from electronic health records [33].
Testing capacity and surveillance capabilities have been built up over the past two years. Over 20,000 free testing sites were opened across the US, with testing also available at pharmacies, and provided by private entities in certain instances, such as universities providing testing for their students [32,34]. The development of at-home rapid tests allowed for individuals to test more conveniently, and in early 2022, the government initiated shipments of free at-home tests to US households [32]. Previously, there was heavy reliance on paper and manual methods for case reporting. Expansion of electronic case reporting was a significant response to the pandemic, and is expected to become standard going forward. Since the start of the pandemic, the number of healthcare facilities with eCR capability has increased from 187 to over 9400 in all 50 states. The Centers for Disease Control and Prevention is undergoing a Data Modernization Initiative to improve data collection and storage infrastructure [33]. Furthermore, the National Wastewater Surveillance System was established in September 2020 to track SARS-CoV-2 presence in wastewater, with benefits such as being an early warning system for outbreaks, covering areas where there may be limited testing for individuals, and helping to establish trends in a community’s COVID-19 infections [35].
3.2.2. Healthcare Disparities
Another public health consideration was the differing effects of COVID-19 on different populations. As the pandemic progressed, information emerged about certain populations and communities at higher risk of COVID-19 infection and/or severe disease, including older individuals, people with preexisting conditions, and individuals of certain races and ethnicities [36].
Disparities during the COVID-19 pandemic have highlighted the importance of collecting data separated by demographics, including age, health status, race and ethnicity, and socioeconomic status, without which, these disparities would not be identified. However, stratification of data reported to the CDC has been incomplete and inconsistent. For example, according to an HHS report on data for addressing health disparities, in January 2022, the CDC reported that data on 34% of COVID-19 cases were “missing race and ethnicity” [37]. Even when data were present, different jurisdictions that reported data on COVID-19 cases and deaths defined racial and ethnic categories differently. There were also no CDC standards for socioeconomic data, which were reported at the community rather than the individual level [37]. These challenges indicate that there is a need to establish, at a national level, definitions for categories within demographic factors, as well as standards and requirements for collecting demographic information.
3.2.3. Medical Countermeasures and Vaccines
The development, approval, and deployment of medical countermeasures and vaccines was an ongoing effort throughout the pandemic that extends to the current day. A balance needed to be struck to ensure that innovations from potentially lifesaving drugs and vaccines were being made available to the public at speed without sacrificing quality control, oversight, and safety. Changes were made to encourage medical countermeasure development and vaccine development. These included accelerated Food and Drug Administration authorization and funding for translational COVID-19-related research [32].
Operation Warp Speed, involving several government agencies and departments, as well as private partners, provided resources and government support for the development, evaluation, mass manufacture, and distribution of vaccine candidates with the original goal of 300 million vaccine doses by January 2021 [38]. The National Institutes of Health program, Accelerating COVID-19 Therapeutic Interventions and Vaccines, supported vaccine treatment and development, similarly involving both government and private partners [39]. When the first vaccine was authorized for emergency use in the US on December 11, 2020, distribution began within three days and progressed in phases [40]. Healthcare workers and residents of long-term care facilities were prioritized, followed by at-risk individuals, other essential workers, and the general public [41]. Initiatives to reduce barriers to vaccination included private groups that provided transportation to vaccination sites, employers offering time off, and CDC resources to help community partners increase vaccination rates among minority and non-English-speaking populations [32,42]. Information campaigns were conducted by federal and local governments to combat misinformation and encourage vaccination, including among minority populations that initially had lower vaccination rates [43]. As of November 2022, over 80% of the US population has received at least one dose [40].
Vaccination has had a profound impact on the effect of COVID-19 on the US, especially due to its progress before the Delta variant surge, with one study estimating that it prevented 58% of potential deaths and another study estimating that it prevented over 1 million deaths [44,45]. However, the US’s vaccination rate is lower than that of about 50 other nations [46]. There are also racial and ethnic disparities in vaccine coverage, which have evolved since the vaccination effort began. A CDC survey found that by May 2021, the percentage of White and Asian respondents who had received at least one dose was highest, around 60% and 70%, respectively, while coverage among Hispanic, Black, Native Hawaiian or other Pacific Islander (NH/OPI), and American Indian or Alaska Native (AI/AN) respondents was lower, under 50%. Some of these disparities have since narrowed, as by December 2021, the percentage of respondents receiving at least one dose was between 75–82% for White, Hispanic, Black, and NH/OPI respondents, over 90% for Asian respondents, and around 60% for AI/AN respondents [47].
One roadblock that vaccine campaigns have run into is the issue of vaccine hesitancy, or the choice to not get an available vaccine. Reasons for hesitancy include concerns about side effects and vaccine safety, lack of trust in the government and institutions, and belief that vaccination is unnecessary [48,49,50]. The misinformation underlying some individuals’ hesitancy illustrates one aspect of communication during the pandemic. Communication with the public has always been a challenge during public health emergencies, with serious consequences if not done effectively; in the case of the COVID-19, pandemic misinformation led to vocal resistance to public health measures. In the modern era, a unique aspect of this challenge is the plethora of information accessible to the average citizen, much of which is not official, and which may be channels for inadvertent or deliberate misinformation [21].
The prevalence of misinformation during the COVID-19 pandemic has highlighted the impact of social media as a communication tool. The WHO has warned about the “infodemic”—a term which predates COVID-19—associated with this pandemic. As the WHO states, an infodemic is an excess of information, some of which may be inadvertently or deliberately inaccurate, that leads to “confusion and risk-taking behaviours”, and erodes trust in official public health responses. The WHO, among other organizations, is highlighting strategies to manage infodemics in the case of outbreaks or other health emergencies [51]. These experiences have emphasized the importance of clearly indicated, understandable, and regularly updated official sources of information.
3.2.4. Clinical Practices
Clinically, COVID-19 has also been a multifaceted challenge. As an emerging virus with which healthcare and public health professionals had no experience, there were delays in clear guidelines for clinical infection control, for example, with information about PPE best practices [52]. Case surges occurred at different times across the US, which the healthcare system was under-equipped to handle due to gaps in coordination between different hospitals and between hospitals and other healthcare providers, emergency services, and medical labs [53]. In anticipation of, and response to, surges, other clinical services were suspended, and individuals also chose to postpone seeking care [54]. These included routine checkups and screenings, non-essential surgeries, and in some cases, treatment of chronic conditions [55,56]. Information also began to emerge about long COVID, resulting in ongoing health issues for individuals months and potentially years after acute infection. More is also being learned about long COVID, as new basic research emerges and individuals with long COVID continue to receive clinical treatment and monitoring [57].
COVID-19 has changed the way care is delivered as a result of staffing shortages and concerns about infection of clinical staff. There was a significant increase of the use of telemedicine during the COVID-19 pandemic, and while there is acknowledgement that many services are best provided in person, with retirement of certain emergency telehealth policies, the continued support of telemedicine is expected in other situations, such as with patients for whom traveling to a healthcare facility is a burden [58,59,60]. Other experiences have affected communication between clinicians. While it is helpful to have a centralized and rapidly adapting source of standardized clinical guidance, often, professional networks are the means by which guidance is distributed and accessed. This can be aided by efforts at the facility level, including setting aside time to discuss these topics at existing meetings [10].
Programs being piloted or expanded in the wake of the COVID-19 pandemic include the Regional Disaster Health Response System, the National Emerging Special Pathogen Training and Education Center, and the National Special Pathogen System of Care. The Regional Disaster Health Response System is a pilot program established in 2018 and supported by the Department of Health and Human Services, whose goal is to improve the coordination of response by hospital systems, which currently act largely independently of each other and of supporting facilities and services. If the pilot demonstration sites are successful, there are plans to expand the system nationwide [61]. The National Emerging Special Pathogen Training and Education Center, which also predates COVID-19, is receiving more support and resources to train healthcare workers and public health officials on infectious disease management [62,63]. Lastly, the recently created National Special Pathogen System of Care is intended to establish a network that can be mobilized rapidly to provide a “sustained, standardized special pathogen system of care” [63,64]. In general, efforts to better coordinate between healthcare facilities, through creation of a biodefense hospital system that allows for a cooperative relationship between hospitals with different capabilities, alongside emergency services, labs, and outpatient services, are anticipated to improve health service delivery [53].
3.2.5. Return to Work and School
Finally, as the nation emerges from a pandemic, it is important to support public health measures that allow individuals to return to work and school safely. When pandemic-related restrictions began to be lifted, numerous considerations were necessary for the safe reopening of schools and workplaces. These included upgrades to physical infrastructure, such as ventilation systems, procedural modifications such as additional testing in schools and updated paid sick leave policies in workplaces, and guidance to business owners on ways to modify their spaces to reduce disease spread [65,66].
During reopening efforts, $130 billion from the American Rescue Plan was made available to support students and safe school reopening [65]. In addition, the federal government issued recommendations and information for businesses intending to make health and safety-related changes to their infrastructure or operations [67].
3.3. Logistics
3.3.1. Surge Response
The response to the pandemic required massive logistical efforts. As waves of the pandemic moved around the nation, different parts of the country needed to handle a surge of cases at one point or another. This involved increased need for healthcare personnel, PPE, ICU beds and equipment to treat severe cases, and medications [10]. Supply shortages were exacerbated by disruptions to the global supply chain that made resources including medical equipment and PPE more expensive and more difficult to obtain [68].
In response to surges that led to shortages of ICU beds and medical equipment, various emergency measures were put into place. Hospitals postponed elective procedures, and there was movement of resources and equipment to more heavily affected regions. Temporary care facilities were built apart from hospitals to handle surges [55,69,70,71]. There were also initiatives, particularly the Arizona Surge Line, to transfer patients between hospitals [10,72]. Shortages of PPE led to the sourcing of PPE from donations and some manufacturers repurposing their manufacturing capacities to produce medical equipment [68,73]. When necessary, guidelines for decontamination and reuse of PPE, such as N95 masks, were issued [74].
The US is currently updating its procedures for surge response infrastructure, such as testing and vaccination sites, based on how they operated during the COVID-19 pandemic. This can help with more rapid mobilization and deployment during emergency responses in the future [32]. The HHS logistics and operation hub for the COVID-19 pandemic has been made into a permanent hub, named “HHS Coordination and Response Element”, or “H-CORE” [75]. The Strategic National Stockpile is being updated with additional masks, ventilators, PPE such as gloves and gowns, other hospital equipment, and COVID-19-specific supplies such as at-home tests and antiviral pills [32]. There are also efforts to improve deployment of these supplies. Most notable are plans to pre-position certain supplies at the state and local level. This reduces the distance supplies may have to travel to reach intended users, allows for more flexibility and discretion of deployment, and enables better tracking of supplies at the state and local jurisdictions during an emergency response. The Last Mile Project, a pre-positioning initiative that predates the pandemic, has been piloted in 7 cities by ASPR/HHS [53,76].
3.3.2. International Efforts
Finally, the global scope of the outbreak and the high transmissibility of the SARS-CoV-2 virus meant that the US could not act in a vacuum. The US undertook efforts to distribute supplies, including medical equipment, PPE, and vaccines, abroad, provide technical support, and build local manufacturing and healthcare service capacity. According to the State Department, over $1.5 billion through the State Department and the United States Agency for International Development (USAID) has gone or will go toward "improving public health education; protecting healthcare facilities; and increasing laboratory, disease-surveillance, and rapid-response capacity" in countries around the world [77]. The US has also donated over half a billion vaccines [78], predominantly to lower-middle-income countries, where the vaccination rate is under half that of high-income countries [79]. The Initiative for Global Vaccine Access, a program created in late 2021, was established to increase COVID-19 vaccinations and support local manufacturing capacity in coordination with national governments, especially in sub-Saharan Africa [80]. The US also joined COVAX, an international effort to distribute COVID-19 vaccines especially to low- and middle-income countries, in January 2021 [81].
The transparency and processes of some of these international efforts has been scrutinized; for example, there has been criticism of where ventilator donations were sent toward the beginning of the pandemic. A government audit identified an unprecedented reduction of input from USAID in decisions about ventilator allocation, with USAID analyses largely disregarded by the National Security Council [82]. Other efforts have been more effective, with USAID support helping increase vaccination rates and vaccine administration infrastructure in multiple sub-Saharan African nations [83].
4. Discussion
4.1. Human Resources
With respect to the challenge of human resources, one of the most pressing issues during the COVID-19 pandemic response centers on persistent healthcare personnel shortages at all levels within the health care system, ranging from nursing and other healthcare providers to maintenance and support staff. Redoubling efforts by which the number of personnel can be augmented through additional training, development of new training resources, and cross-training are important considerations. Use of non-clinical staff serving in less technical roles to reduce the strain on clinical staff should likewise be considered. Additionally, the importance of maintaining updated and accurate numbers of healthcare workers available to fulfill certain roles cannot be overstated, particularly during periods of surge. Support of frontline workers by taking care of everyday needs such as childcare and food can reduce burdens that may contribute to burnout, as can institutional responsiveness to healthcare workers’ concerns.
4.2. Health Service Delivery
Availability of testing and surveillance remain a cornerstone of COVID-19 response. The development and distribution of accessible, low-cost, fast, and accurate testing should be a priority during any infectious disease outbreak, with its benefits in reducing disease spread and informing about the progression of an outbreak. While such testing is now readily available, this was not always the case through the early stages of the pandemic. Individuals seeking testing increased strain on healthcare systems due to unnecessary hospital visits. Actions taken during the COVID-19 pandemic have demonstrated ways for governments to make testing accessible such as setting up mass sites, and providing materials directly to households. The US increased its testing manufacturing capacity during the COVID-19 pandemic and is anticipated to continue investing in this capacity. In addition, there are plans to add at-home tests to national emergency stockpiles. Other surveillance-related efforts should continue to be developed. Sequencing data, with the US now capable of sequencing tens of thousands of isolates per week, can provide early warning of new variants, which is particularly important with fast-changing viral pathogens such as SARS-CoV-2. Situational awareness maintained via surveillance data collected at all governmental levels should remain consistent, accessible, transparent and readily interpretable.
Recognition of healthcare disparities is readily acknowledged; yet implementing measures to effectively address issues ranging from health literacy to access to care remains daunting. Gaps in the collection of demographic information that could identify the presence and scope of disparities can be used to inform data collection standards going forward.
In the age of social media, the extensive impact of misinformation will certainly be a topic that deserves attention. Clear, non-conflicting communication from trusted, authoritative sources in the face of uncertainty must be coupled with channels to receive feedback on the effectiveness of communication strategies [84], as well as robust campaigns to actively debunk misinformation.
Many clinical questions remain regarding the origins and continued evolution of the virus as well as ways this will impact the course of the pandemic. Characteristics of those affected by long COVID remain to be fully elucidated and the demand for research on long COVID has been drawing increasing attention. Growing evidence suggests that autoimmune responses may play an important role in long COVID, while the impacts over time on the health of the population remain to be seen [85].
4.3. Logistics Systems
The challenges of COVID-19 surges have highlighted the importance of flexibility and mobility within the health system. Keeping personnel and equipment mobile so they can be rapidly deployed to areas of need, as well as systems to transfer patients from overburdened facilities to ones better positioned to address their needs, are measures that can help the health system and healthcare personnel better handle surges. Flexibility is also a consideration with supplies, alongside volume and variety. In addition to stockpiling more and different types of PPE, medical equipment, antivirals, tests, and other supplies, the ability to get them to healthcare facilities, healthcare workers, and the general public quickly is critical.
Finally, the international scope of this pandemic has demonstrated the fact that variants continue to arise around the world and spread globally. In addition to humanitarian objectives, mitigating the spread of the virus abroad could reduce the emergence of new variants, as well as reduce the risk of imported cases. In the future, the US should continue to foster distribution of supplies and provide support abroad as part of its response to a public health emergency. However, care should be taken to ensure that these decisions are based on public health principles and expertise.
4.4. Limitations and Future Directions
While a comprehensive effort was made to identify major contributions to the US response to COVID-19 pandemic pertaining to human resources, health service delivery, and logistics, certain pertinent resources may not have been identified or included due to the inherent breadth of the topic. The search included strictly publicly available sources and documents; accordingly, those with restrictions or not released externally were not considered. As the pandemic continues, the longer-term impacts of various responses on post-pandemic health emergency and Disaster Risk Management remain to be fully determined.
Beyond the US, other countries faced similar challenges, including shortage of healthcare workers and healthcare worker attrition, shortages of PPE and other supplies, and COVID-19-related misinformation. Lower income nations faced additional burdens, such as loss of healthcare personnel to recruitment from higher income nations, fewer resources such as PPE and equipment to treat severe cases, and less infrastructure for vaccine and medical countermeasure development and production [86,87,88,89].
Responses have been less generalizable than challenges. Short term responses and more systematic changes alike have varied widely, even between geographically proximate countries, as a result of a diverse array of factors both medical and non-medical, including differences in healthcare systems, social, political, and cultural considerations, infrastructure, demographics, and biomedical research capacity. These difficulties in generalization suggest that a comparison with a more global scope of public health responses to COVID-19 and changes to public health systems would be a rich topic of study.
In addition, it will be important going forward to evaluate the ongoing impact of changes made and programs initiated as a result of lessons learned during the COVID-19 pandemic. For example, the initiatives regarding healthcare worker mental health supported by American Rescue Plan Act funds can be compared, such as through qualitative interviews with healthcare worker participants, to give an idea of what initiatives are effective. As another example, supply pre-positioning programs can be evaluated to see whether resources are reaching frontline facilities faster.
5. Conclusions
Challenges faced by the US during the COVID-19 pandemic have highlighted ways that the nation’s health system can prepare for and improve its response during future outbreaks. Major areas of improvement include increasing the numbers and flexibility of healthcare personnel, as well as the supplies and equipment needed to treat patients and keep themselves safe. The importance of fast and accessible testing, and the benefits of rapid development and deployment of vaccines, have been shown. Various considerations surround information delivery to combat misinformation, communicate clinical guidance, conduct effective surveillance, and identify disparities in infection rates and healthcare access. Coordination between hospital systems can help take varying capabilities and capacities into account during a response. Lastly, support of outbreak control and vaccination efforts abroad are important considerations of a US pandemic response. Some changes as a result of challenges identified are already being implemented, and continuing to do so will strengthen the health system in anticipation of future emergency responses.
Author Contributions
Conceptualization, E.B.H.; Data curation, A.P.C., B.H. and E.B.H.; Funding acquisition, E.B.H.; Investigation, A.P.C., B.H. and E.B.H.; Methodology, A.P.C. and E.B.H.; Project administration, E.B.H.; Resources, E.B.H.; Supervision, E.B.H.; Visualization, A.P.C. and E.B.H.; Writing—original draft, A.P.C. and E.B.H.; Writing—review & editing, A.P.C., B.H. and E.B.H. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the World Health Organization Kobe Centre for Health Development (WKC-HEDRM-K21001) in collaboration with the Department of Public Health and Health Policy, Graduate School of Biomedical and Health Sciences, Hiroshima University, Japan.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to gratefully acknowledge Tatsuhiko Kubo, and Chimed Ochir Odgerel, from the Department of Public Health and Health Policy, Graduate School of Biomedical and Health Sciences, Hiroshima University and the World Health Organization Kobe Centre for Health Development for reviewing and providing feedback on early iterations of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- COVID Data Tracker. Centers for Disease Control and Prevention. 28 July 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 2 August 2022).
- Laboratory-Confirmed COVID-19-Associated Hospitalizations. COVID-NET, Centers for Disease Control and Prevention. 23 July 2022. Available online: https://gis.cdc.gov/grasp/covidnet/covid19_5.html (accessed on 2 August 2022).
- World Health Organization. Health Emergency and Disaster Risk Management Framework. 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/326106/9789241516181-eng.pdf (accessed on 2 August 2022).
- Aitsi-Selmi, A.; Murray, V.; Heymann, D.; McCloskey, B.; Azhar, E.I.; Petersen, E.; Zumla, A.; Dar, O. Reducing risks to health and wellbeing at mass gatherings: The role of the Sendai Framework for Disaster Risk Reduction. Int. J. Infect. Dis. 2016, 47, 101–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; American Hospital Association. AHA Letter Re: Challenges Facing America’s Health Care Workforce as the U.S. Enters Third Year of COVID-19 Pandemic. 1 March 2022. Available online: https://www.aha.org/lettercomment/2022-03-01-aha-provides-information-congress-re-challenges-facing-americas-health (accessed on 6 April 2022).
- Office of the Assistant Secretary for Planning and Evaluation. Impact of the COVID-19 Pandemic on the Hospital and Outpatient Clinician Workforce: Challenges and Policy Responses. (Issue Brief No. HP-2022-13). U.S. Department of Health and Human Services. 3 March 2022. Available online: https://aspe.hhs.gov/sites/default/files/documents/9cc72124abd9ea25d58a22c7692dccb6/aspe-covid-workforce-report.pdf (accessed on 2 August 2022).
- Fadel, L.; Stone, W.; Anderson, M.; Benincasa, R. As Hospitals Lose Revenue, More Than a Million Health Care Workers Lose Jobs. NPR. 8 May 2020. Available online: https://www.npr.org/2020/05/08/852435761/as-hospitals-lose-revenue-thousands-of-health-care-workers-face-furloughs-layoff (accessed on 2 August 2022).
- Staff Shortages. Centers for Disease Control and Prevention. 21 January 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/mitigating-staff-shortages.html (accessed on 2 August 2022).
- Begun, J.W.; Jiang, H.J. Health Care Management During COVID-19: Insights from Complexity Science. NEJM Catal. Innov. Care Deliv. 2020, 1, 1–12. [Google Scholar] [CrossRef]
- McAfee, M.; Pedersen, C.; Kim, D.; Hawkins, S.; Redman, M. Doctors, Nurses from Across the US Step Up to Help NYC on the Coronavirus Front Lines. ABC News. 10 April 2020. Available online: https://abcnews.go.com/US/doctors-nurses-us-step-nyc-coronavirus-front-lines/story?id=70049109 (accessed on 2 August 2022).
- NYC Health + Hospitals/Coney Island Welcomes, U.S. Department of Defense Medical Team. NYC Health + Hospitals. 24 January 2022. Available online: https://www.nychealthandhospitals.org/pressrelease/coney-island-hospital-welcomes-military-medical-team/ (accessed on 2 August 2022).
- U.S. Army North Public Affairs. Military Hospital Support to Fema Begins in Five States, Navajo Nation, Expands Elsewhere. U.S. Northern Command. 21 January 2022. Available online: https://www.northcom.mil/Newsroom/News/Article/Article/2907587/military-hospital-support-to-fema-begins-in-five-states-navajo-nation-expands-e/ (accessed on 2 August 2022).
- Pollack, R.; American Hospital Association. Hospital Workforce Shortage Crisis Demands Immediate Action. American Hospital Association. Available online: https://www.aha.org/lettercomment/2022-01-27-hospital-workforce-shortage-crisis-demands-immediate-action (accessed on 2 August 2022).
- COVID-19 Contact Tracing. Coursera. Available online: https://www.coursera.org/learn/covid-19-contact-tracing (accessed on 2 August 2022).
- Connley, C. States Are Hiring Thousands of Coronavirus Contact Tracers—Here’s What to Know about the Job. CNBC. 21 May 2020. Available online: https://www.cnbc.com/2020/05/21/what-is-a-coronavirus-contact-tracer-and-how-to-get-hired-as-one.html (accessed on 2 August 2022).
- Connecticut COVID-19 Response. Volunteer to Support Your Community. 2022. Available online: https://portal.ct.gov/Coronavirus/Information-For/Volunteers (accessed on 2 August 2022).
- Opportunities for Medical and Non-Medical Volunteers. City of Chicago. 2022. Available online: https://www.chicago.gov/city/en/sites/covid19-vaccine/home/for-volunteers.html (accessed on 2 August 2022).
- Hancock, S.C. Perspective: An Inside Look at a Rural Hospital Preparing for the Wave. The Kansas Leadership Center Journal. 6 April 2020. Available online: https://klcjournal.com/inside-rural-hospital-covid-19/ (accessed on 2 August 2022).
- Davis, J. Episode 2—The Silver Lining: COVID-19 Care Teams and Cross-Training. American Association of Critical-Care Nurses. 4 June 2020. Available online: https://www.aacn.org/clinical-resources/covid-19/podcast-series/the-silver-lining (accessed on 2 August 2022).
- U.S. Department of Health and Human Services. Health Misinformation. Available online: https://www.hhs.gov/surgeongeneral/priorities/health-misinformation/index.html (accessed on 2 August 2022).
- Prasad, K.; McLoughlin, C.; Stillman, M.; Poplau, S.; Goelz, E.; Taylor, S.; Nankivil, N.; Brown, R.; Linzer, M.; Cappelucci, K.; et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: A national cross-sectional survey study. eClinicalMedicine 2021, 35, 100879. [Google Scholar] [CrossRef] [PubMed]
- Byhoff, E.; Paulus, J.K.; Guardado, R.; Zubiago, J.; Wurcel, A.G. Healthcare workers’ perspectives on coronavirus testing availability: A cross sectional survey. BMC Health Serv. Res. 2021, 21, 719. [Google Scholar] [CrossRef] [PubMed]
- Additional Background: Sweeping Regulatory Changes to Help U.S. Healthcare System Address COVID-19 Patient Surge. 30 March 2020. Available online: https://www.cms.gov/newsroom/fact-sheets/additional-backgroundsweeping-regulatory-changes-help-us-healthcare-system-address-covid-19-patient (accessed on 2 August 2022).
- U.S. Department of Health and Human Services. Biden-Harris Administration Awards $103 Million in American Rescue Plan Funds to Reduce Burnout and Promote Mental Health and Wellness Among Health Care Workforce. 20 January 2022. Available online: https://www.hhs.gov/about/news/2022/01/20/biden-harris-administration-awards-103-million-american-rescue-plan-funds-reduce-burnout-promote-mental-health-wellness-among-health-care-workforce.html (accessed on 2 August 2022).
- Harry, E.M.; Carlasare, L.E.; Sinsky, C.A.; Brown, R.L.; Goelz, E.; Nankivil, N.; Linzer, M. Childcare Stress, Burnout, and Intent to Reduce Hours or Leave the Job During the COVID-19 Pandemic Among US Health Care Workers. JAMA Netw. Open 2022, 5, e2221776. [Google Scholar] [CrossRef] [PubMed]
- Berg, S. Half of Health Workers Report Burnout Amid COVID-19. American Medical Association. 20 July 2021. Available online: https://www.ama-assn.org/practice-management/physician-health/half-health-workers-report-burnout-amid-covid-19 (accessed on 2 August 2022).
- Yong, E. Why Health-care Workers are Quitting in Droves. The Atlantic. 16 November 2021. Available online: https://www.theatlantic.com/health/archive/2021/11/the-mass-exodus-of-americas-health-care-workers/620713/ (accessed on 2 August 2022).
- Kelly, J. New Survey Shows That Up To 47% Of U.S. Healthcare Workers Plan to Leave Their Positions By 2025. Forbes. 19 April 2022. Available online: https://www.forbes.com/sites/jackkelly/2022/04/19/new-survey-shows-that-up-to-47-of-us-healthcare-workers-plan-to-leave-their-positions-by-2025/?sh=4acd8d9e395b (accessed on 2 August 2022).
- Berlin, G.; Lapointe, M.; Murphy, M. Surveyed Nurses Consider Leaving Direct Patient Care at Elevated Rates. McKinsey. 17 February 2022. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/surveyed-nurses-consider-leaving-direct-patient-care-at-elevated-rates (accessed on 2 August 2022).
- Sinsky, C.A.; Brown, R.L.; Stillman, M.J.; Linzer, M. COVID-Related Stress and Work Intentions in a Sample of US Health Care Workers. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- The White House. National COVID-19 Preparedness Plan. March 2022. Available online: https://www.whitehouse.gov/covidplan/ (accessed on 6 April 2022).
- Centers for Disease Control and Prevention. CDC’s COVID-19 Data Improvement. 29 October 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/data-improvements.html (accessed on 2 August 2022).
- U.S. Department of Health and Human Services. Community-Based Testing Sites for COVID-19. 24 January 2022. Available online: https://www.hhs.gov/coronavirus/community-based-testing-sites/index.html (accessed on 2 August 2022).
- Centers for Disease Control and Prevention. Waterborne Disease & Outbreak Surveillance Reporting. 21 March 2022. Available online: https://www.cdc.gov/healthywater/surveillance/wastewater-surveillance/wastewater-surveillance.html (accessed on 2 August 2022).
- Centers for Disease Control and Prevention. COVID-19: Specific Groups of People. 25 March 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html (accessed on 2 August 2022).
- US Department of Health and Human Services. CDC Found Ways to Use Data to Understand and Address COVID-19 Health Disparities, Despite Challenges with Existing Data. July 2022. Available online: https://oig.hhs.gov/oei/reports/OEI-05-20-00540.pdf (accessed on 24 November 2022).
- Cohen, J. Unveiling ‘Warp Speed’, the White House’s America-First Push for a Coronavirus Vaccine. ScienceInsider. 12 May 2020. Available online: https://www.science.org/content/article/unveiling-warp-speed-white-house-s-america-first-push-coronavirus-vaccine (accessed on 2 August 2022).
- National Institutes of Health. Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV). Available online: https://www.nih.gov/research-training/medical-research-initiatives/activ (accessed on 2 August 2022).
- CDC. COVID-19 Vaccinations in the United States. 16 November 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-additional-dose-totalpop (accessed on 24 November 2022).
- MN Department of Health. COVID-19 Vaccine Phases and Planning. 9 May 2022. Available online: https://www.health.state.mn.us/diseases/coronavirus/vaccine/plan.html (accessed on 2 August 2022).
- Centers for Disease Control and Prevention. A Guide for Community Partners: Increasing COVID-19 Vaccine Uptake among Members of Racial and Ethnic Minority Communities. 6 April 2021. Available online: https://www.cdc.gov/vaccines/covid-19/downloads/guide-community-partners.pdf (accessed on 2 August 2022).
- Perez-Stable, E. Overcoming Racial Disparities in Vaccine Hesitancy and Access. Briefings—Foreign Press Centers, U.S. Department of State. 2021. Available online: https://www.state.gov/briefings-foreign-press-centers/overcoming-racial-disparities-in-vaccine-hesitancy-and-access/ (accessed on 2 August 2022).
- Jones, M.; Khader, K.; Branch-Elliman, W. Estimated Impact of the US COVID-19 Vaccination Campaign—Getting to 94% of Deaths Prevented. JAMA Netw. Open 2022, 5, e2220391. [Google Scholar] [CrossRef] [PubMed]
- Schneider, E.C.; Shah, A.; Sah, P.; Moghadas, S.M.; Vilches, T.; Galvania, A. The U.S. COVID-19 Vaccination Program at One Year: How Many Deaths and Hospitalizations Were Averted? The Commonwealth Fund. 14 December 2021. Available online: https://www.commonwealthfund.org/publications/issue-briefs/2021/dec/us-covid-19-vaccination-program-one-year-how-many-deaths-and (accessed on 2 August 2022).
- Holder, J. Tracking Coronavirus Vaccinations around the World. The New York Times. 21 November 2022. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (accessed on 24 November 2022).
- Kriss, J.L.; Hung, M.-C.; Srivastav, A.; Black, C.L.; Lindley, M.C.; Lee, J.T.; Koppaka, R.; Tsai, Y.; Lu, P.-J.; Yankey, D.; et al. COVID-19 Vaccination Coverage, by Race and Ethnicity—National Immunization Survey Adult COVID Module, United States, December 2020–November 2021. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 757–763. [Google Scholar] [CrossRef]
- King, W.C.; Rubinstein, M.; Reinhart, A.; Mejia, R. Time trends, factors associated with, and reasons for COVID-19 vaccine hesitancy: A massive online survey of US adults from January–May 2021. PLoS ONE 2021, 16, e0260731. [Google Scholar] [CrossRef]
- AAFP. Four Reasons for COVID-19 Vaccine Hesitancy among Health care Workers, and Ways to Counter Them. 27 April 2021. Available online: https://www.aafp.org/pubs/fpm/blogs/inpractice/entry/countering_vaccine_hesitancy.html (accessed on 2 August 2022).
- Newport, P. Vaccine Hesitancy and U.S. Public Opinion. Gallup. 30 July 2021. Available online: https://news.gallup.com/opinion/polling-matters/352976/vaccine-hesitancy-public-opinion.aspx (accessed on 2 August 2022).
- World Health Organization. Infodemic. Available online: https://www.who.int/health-topics/infodemic#tab=tab_1 (accessed on 2 August 2022).
- U.S. Department of Health and Human Services. COVID-19 Concerns and Opportunities for Healthcare Leadership. September 2022. Available online: https://files.asprtracie.hhs.gov/documents/covid-19-concerns-and-opportunities-for-healthcare-leadership.pdf (accessed on 6 April 2022).
- Biodefense in Crisis: Immediate Action Needed to Address National Vulnerabilities. Bipartisan Commission on Biodefense. March 2021. Available online: https://biodefensecommission.org/wp-content/uploads/2021/03/Indicators-Report_final7_070221_web.pdf (accessed on 6 April 2022).
- Berlin, G.; Singhal, S.; Lapointe, M.; Schulz, J. Challenges Emerge for the US Healthcare System as COVID-19 Cases Rise. McKinsey & Company. 25 November 2020. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/challenges-emerge-for-the-us-healthcare-system-as-covid-19-cases-rise (accessed on 6 April 2022).
- Centers for Medicare & Medicaid Services. CMS Adult Elective Surgery and Procedures Recommendations. 7 April 2020. Available online: https://www.cms.gov/files/document/covid-elective-surgery-recommendations.pdf (accessed on 2 August 2022).
- Centers for Medicare & Medicaid Services. Non-Emergent, Elective Medical Services, and Treatment Recommendations. 7 April 2020. Available online: https://www.cms.gov/files/document/cms-non-emergent-elective-medical-recommendations.pdf (accessed on 2 August 2022).
- Goldman, B. Stanford Medicine to Enroll 900 in NIH-Funded long-COVID Study. Stanford Medicine News Center. 22 November 2021. Available online: https://med.stanford.edu/news/all-news/2021/11/long-covid-research-initiative.html (accessed on 2 August 2022).
- Weiner, S. What Happens to Telemedicine after COVID-19? AAMC News. 21 October 2021. Available online: https://www.aamc.org/news-insights/what-happens-telemedicine-after-covid-19 (accessed on 2 August 2022).
- U.S. Department of Health and Human Services. Telehealth Policy Changes after the COVID-19 Public Health Emergency. 29 June 2022. Available online: https://telehealth.hhs.gov/providers/policy-changes-during-the-covid-19-public-health-emergency/policy-changes-after-the-covid-19-public-health-emergency/ (accessed on 2 August 2022).
- Bestsennyy, O.; Gilbert, G.; Harris, A.; Rost, J. Telehealth: A quarter-trillion-dollar post-COVID-19 reality? McKinsey & Company. 9 July 2021. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality (accessed on 2 August 2022).
- Administration for Strategic Preparedness & Response, U.S. Department of Health and Human Services. Regional Disaster Health Response System. Available online: https://aspr.hhs.gov/RDHRS/Pages/default.aspx (accessed on 2 August 2022).
- Mehta, A.; Lowe, J.; Mukherjee, V. To Prepare For The Next Pandemic, Build A National Care Delivery Network By Leveraging Existing Systems. Health Affairs. 15 October 2021. Available online: https://www.healthaffairs.org/do/10.1377/forefront.20211014.312600 (accessed on 2 December 2022).
- Administration for Strategic Preparedness & Response, U.S. Department of Health and Human Services. National Emerging Special Pathogens Training and Education Center: Mission, Vision & Goals. Available online: https://netec.org/nsps/mission-goals/ (accessed on 2 August 2022).
- Administration for Strategic Preparedness & Response, U.S. Department of Health and Human Services. National Special Pathogen System of Care (NSPS) Strategy Summary. 18 June 2021. Available online: https://netec.org/wp-content/uploads/2021/12/NETEC_NSPS-Strategy-Summary-1.pdf (accessed on 2 August 2022).
- U.S. Department of Education. U.S. Department of Education Approves Maryland’s Plan for Use of American Rescue Plan Funds to Support K-12 Schools and Students, Distributes Remaining More Than $651 Million to State. 14 October 2021. Available online: https://www.ed.gov/news/press-releases/us-department-education-approves-marylands-plan-use-american-rescue-plan-funds-support-k-12-schools-and-students-distributes-remaining-more-651-million-state (accessed on 2 August 2022).
- Miller, C.C. A Key to Returning to Normal Is Paid Sick Leave, Democrats Say. The New York Times. 20 February 2022. Available online: https://www.nytimes.com/2022/02/21/upshot/paid-leave-covid-democrats.html (accessed on 2 August 2022).
- The White House. Biden Administration Launches Effort to Improve Ventilation and Reduce the Spread of COVID-19 in Buildings. 17 March 2022. Available online: https://www.whitehouse.gov/briefing-room/statements-releases/2022/03/17/fact-sheet-biden-administration-launches-effort-to-improve-ventilation-and-reduce-the-spread-of-covid-19-in-buildings/ (accessed on 2 August 2022).
- World Bank Group. COVID-19 and the Global Supply Chains for Medical Supplies. Available online: https://www.globalfinancingfacility.org/sites/gff_new/files/documents/COVID-19-Supply-Chain-ENGLISH.pdf (accessed on 2 August 2022).
- Aboulenein, A. Overwhelmed by Omicron Surge, U.S. Hospitals Delay Surgeries. Reuters. 7 January 2022. Available online: https://www.reuters.com/world/us/overwhelmed-by-omicron-surge-us-hospitals-delay-surgeries-2022-01-07/ (accessed on 2 August 2022).
- Dwyer, C. ‘This Is A Big Deal’: New York Hails Ventilator Deliveries from China and Oregon. NPR. 4 April 2020. Available online: https://www.npr.org/sections/coronavirus-live-updates/2020/04/04/827314791/this-is-a-big-deal-new-york-hails-ventilator-deliveries-from-china-and-oregon (accessed on 2 August 2022).
- Donnelly, C. Field Hospitals Return to Some States As COVID-19 Pushes Hospitals to Breaking Point. NPR. 31 January 2021. Available online: https://www.npr.org/2021/01/31/962528974/field-hospitals-return-to-some-states-as-covid-19-pushes-hospitals-to-breaking-p (accessed on 2 August 2022).
- The Arizona Surgeline. Available online: https://www.azdhs.gov/covid19/documents/healthcare-providers-surge-line/faqs-for-healthcare-facilities-providers.pdf (accessed on 2 August 2022).
- Robinson, D. The Companies Repurposing Manufacturing to Make Key Medical Kit during COVID-19 Pandemic. NS Medical Devices. 1 April 2020. Available online: https://www.nsmedicaldevices.com/analysis/companies-ventilators-shortage-coronavirus/ (accessed on 2 August 2022).
- Centers for Disease Control and Prevention. Decontamination & Reuse of N95 Respirators. 19 October 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html (accessed on 2 August 2022).
- Administration for Strategic Preparedness & Response, U.S. Department of Health and Human Services. H-CORE: HHS Coordination Operations and Response Element. Available online: https://aspr.hhs.gov/h-core/Pages/Default.aspx (accessed on 2 August 2022).
- Office of the Assistant Secretary for Preparedness and Response; U.S. Department of Health and Human Services. The Last Mile: A Pilot Project. 3 April 2019. Available online: https://www.phe.gov/Preparedness/planning/last-mile/Pages/default.aspx (accessed on 2 August 2022).
- U.S. Department of State. Foreign Assistance for Coronavirus (COVID-19). Available online: https://www.state.gov/foreign-assistance-for-coronavirus-covid-19/ (accessed on 2 August 2022).
- Power, S. Marking Delivery of Half a Billion U.S.-Donated COVID-19 Vaccines. Office of Press Relations, USAID. 17 March 2022. Available online: https://www.usaid.gov/news-information/press-releases/mar-17-2022-marking-delivery-half-billion-us-donated-covid-19-vaccines (accessed on 2 August 2022).
- KFF. Tracking U.S. COVID-19 Vaccine Donations. 22 September 2021. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/tracking-u-s-covid-19-vaccine-donations/ (accessed on 24 November 2022).
- Office of Press Relations, USAID. USAID Announces Initiative for Global Vaccine Access (Global VAX) to Accelerate Vaccine Access and Delivery Assistance Around the World. 6 December 2021. Available online: https://www.usaid.gov/news-information/press-releases/dec-6-2021-usaid-announces-initiative-global-vaccine-access-global-vax (accessed on 2 August 2022).
- Rouw, A.; Kates, J.; Michaud, J.; Wexler, A. COVAX and the United States. KFF. 18 February 2021. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/covax-and-the-united-states/ (accessed on 2 August 2022).
- Office of Inspector General. USAID Had Limited Control Over COVID-19 Ventilator Donations, Differing from Its Customary Response to Public Health Emergencies. U.S. Agency for International Development. 24 February 2021. Available online: https://oig.usaid.gov/sites/default/files/2021-02/4-936-21-002-P_0.pdf (accessed on 2 August 2022).
- USAID. COVID-19—Sub-Saharan Africa: Fact Sheet #4. 31 March 2022. Available online: https://www.usaid.gov/sites/default/files/documents/Regional_Fact_Sheet_4_-_SSA.pdf (accessed on 2 August 2022).
- Overton, D.; Ramkeesoon, S.A.; Kirkpatrick, K.; Byron, A.; Pak, E.S. Lessons from the COVID-19 Crisis on Executing Communications and Engagement at the Community Level During a Health Crisis. National Academies. 7 December 2021. Available online: https://www.nationalacademies.org/news/2021/12/lessons-from-covid-19-on-executing-communications-and-engagement-at-the-community-level-during-a-health-crisis (accessed on 24 November 2022).
- NIH. Autoimmune Response Found in Many with COVID-19. 28 September 2021. Available online: https://www.nih.gov/news-events/nih-research-matters/autoimmune-response-found-many-covid-19 (accessed on 24 November 2022).
- Poon, Y.-S.R.; Lin, Y.P.; Griffiths, P.; Yong, K.K.; Seah, B.; Liaw, S.Y. A global overview of healthcare workers’ turnover intention amid COVID-19 pandemic: A systematic review with future directions. Hum. Resour. Health 2022, 20, 70. [Google Scholar] [CrossRef] [PubMed]
- Nebehay, S. Global Shortage of Nurses Set to Grow as Pandemic Enters Third Year-Group. Reuters. 10 December 2021. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/global-shortage-nurses-set-grow-pandemic-enters-third-year-group-2021-12-10/ (accessed on 24 November 2022).
- Tessema, G.A.; Kinfu, Y.; Dachew, B.A.; Tesema, A.G.; Assefa, Y.; Alene, K.A.; Aregay, A.F.; Ayalew, M.B.; Bezabhe, W.M.; Bali, A.G.; et al. The COVID-19 pandemic and healthcare systems in Africa: A scoping review of preparedness, impact and response. BMJ Glob. Health 2021, 6, e007179. [Google Scholar] [CrossRef]
- Siwakoti, S.; Yadav, K.; Thange, I.; Bariletto, N.; Zanotti, L.; Ghoneim, A.; Shapiro, J.N. Localized Misinformation in a Global Pandemic: Report on COVID-19 Narratives around the World. Empirical Studies of Conflict. 2021. Available online: https://esoc.princeton.edu/publications/localized-misinformation-global-pandemic-report-covid-19-narratives-around-world (accessed on 24 November 2022).
Figure 1.
Analytic framework of United States-based COVID-19 pandemic response.

{kind=link}
Table 1.
Domains and Key Takeaway Impacts.
| Domain | Key Takeaway Impacts |
|---|---|
| Human Resources |
|
| Health Service Delivery |
|
| Logistics |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, A.P.; Hansoti, B.; Hsu, E.B. The COVID-19 Pandemic Response and Its Impact on Post-Pandemic Health Emergency and Disaster Risk Management in the United States. Sustainability 2022, 14, 16301. https://doi.org/10.3390/su142316301
AMA Style
Chen AP, Hansoti B, Hsu EB. The COVID-19 Pandemic Response and Its Impact on Post-Pandemic Health Emergency and Disaster Risk Management in the United States. Sustainability. 2022; 14(23):16301. https://doi.org/10.3390/su142316301
Chicago/Turabian StyleChen, Allison P., Bhakti Hansoti, and Edbert B. Hsu. 2022. "The COVID-19 Pandemic Response and Its Impact on Post-Pandemic Health Emergency and Disaster Risk Management in the United States" Sustainability 14, no. 23: 16301. https://doi.org/10.3390/su142316301
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.