
Strategic Assessment of Neighbourhood Environmental Impacts on Mental Health in the Lisbon Region (Portugal): A Strategic Focus and Assessment Framework at the Local Level



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Collection
2.3. Measure of Mental Health
2.4. Methodology for Strategic Focus on Environmental and Mental Health Assessment (SEmHA)
2.4.1. Phase I: Baseline—Understanding Neighbourhood Environmental Conditions
2.4.2. Phase II: Definition of the SEmHA Framework
3. Results
3.1. Baseline—Risks to Poor Mental Health
3.2. Strategic Focus on Neighbourhood Environmental Conditions That Influence Mental Health
3.2.1. Public Space Quality (CDF 1)
3.2.2. Physical Environment Quality (CDF 2)
3.2.3. Professional Qualification and Creation of Economic Activities (CDF 3)
3.2.4. Services and Facilities (CDF 4)
4. Discussion
4.1. Discussing the Selection of the Four Critical Decision Factors (CDF)
4.2. Discussing What Each Critical Decision Factor (CDF) Entails
4.2.1. CDF 1. Public Space Quality
4.2.2. CDF 2. Physical Environment Quality
4.2.3. CDF 3. Professional Qualification and Creation of Economic Activities
4.2.4. CDF 4. Services and Facilities
4.3. Discussing the Usefulness and Applicability of the Strategic Focus on Environmental and Mental Health Assessment (SEmHA) Framework
4.4. Strengths, Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Patel, V.; Lund, C.; Hatherill, S.; Plagerson, S.; Corrigall, J.; Funk, M.; Flisher, A.J. Mental Disorders: Equity and Social Determinants. In Equity, Social Determinants and Public Health Programs; Blas, A., Kurup, A.S., Eds.; World Health Organization: Geneva, Switzerland, 2010; pp. 115–134. [Google Scholar]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No Health without Mental Health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]
- Brown, J.; Learmonth, A.; Mackereth, C. Promoting Public Mental Health and Well-Being: Principles into Practice; Jessica Kingsley Publishers: London, UK, 2015. [Google Scholar]
- Patel, V. Acting Early: The Key to Preventing Mental Health Problems. J. R. Soc. Med. 2018, 111, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Alegría, M.; NeMoyer, A.; Falgàs Bagué, I.; Wang, Y.; Alvarez, K. Social Determinants of Mental Health: Where We Are and Where We Need to Go. Curr. Psychiatry Rep. 2018, 20, 95. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S. Space, Place and Mental Health; Ashgate: Farnham, UK, 2010; ISBN 0754673316. [Google Scholar]
- Kousoulis, A.A.; Goldie, I. A Visualization of a Socio-Ecological Model for Urban Public Mental Health Approaches. Front. Public Health 2021, 9, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Cherrie, M.; Shortt, N.; Deary, I.; Ward Thompson, C. Life Course of Place: A Longitudinal Study of Mental Health and Place. Trans. Inst. Br. Geogr. 2018, 43, 555–572. [Google Scholar] [CrossRef]
- Salanti, G.; Cipriani, A.; Furukawa, T.A.; Peter, N.; Tonia, T.; Papakonstantinou, T.; Holloway, A.; Leucht, S. An Efficient Way to Assess the Effect of COVID-19 on Mental Health in the General Population. Lancet Psychiatry 2021, 8, e14–e15. [Google Scholar] [CrossRef]
- Cave, B.; Kim, J.; Viliani, F.; Harris, P. Applying an Equity Lens to Urban Policy Measures for COVID-19 in Four Cities. Cities Health 2020, 1–5. [Google Scholar] [CrossRef]
- Campo-Arias, A.; De Mendieta, C.T. Social Determinants of Mental Health and the COVID-19 Pandemic in Low-Income and Middle-Income Countries. Lancet Glob. Health 2021, 9, e1029. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Triguero-Mas, M.; Jardim Santos, C.; Gómez-Nieto, A.; Cole, H.; Anguelovski, I.; Silva, F.M.; Baró, F. Exposure to Nature and Mental Health Outcomes during COVID-19 Lockdown. A Comparison between Portugal and Spain. Environ. Int. 2021, 154, 106664. [Google Scholar] [CrossRef]
- Barton, H. City of Well-Being. A Radical Guide to Planning; Routledge: Oxfordshire, UK, 2016. [Google Scholar]
- Un-Habitat; World Health Organization. Integrating Health in Urban and Territorial Planning: A Sourcebook; WHO: Genebra, Switzerland, 2020. [Google Scholar]
- Appelqvist-Schmidlechner, K.; Vaara, J.P.; Vasankari, T.; Häkkinen, A.; Mäntysaari, M.; Kyröläinen, H. Relationship between Different Domains of Physical Activity and Positive Mental Health among Young Adult Men. BMC Public Health 2020, 20, 1116. [Google Scholar] [CrossRef]
- Mitchell, R. Is Physical Activity in Natural Environments Better for Mental Health than Physical Activity in Other Environments? Soc. Sci. Med. 2013, 91, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Associations of Neighbourhood Greenness with Physical and Mental Health: Do Walking, Social Coherence and Local Social Interaction Explain the Relationships? J. Epidemiol. Community Health 2008, 62, e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, M.; Hashimoto, S.; Dasgupta, R. The Mediating Role of Place Attachment between Nature Connectedness and Human Well-Being: Perspectives from Japan. Sustain. Sci. 2020, 15, 849–862. [Google Scholar] [CrossRef]
- Khosravi, H.; Bahrainy, H.; Tehrani, S.O. Neighbourhood Morphology, Genuine Self-Expression and Place Attachment, the Case of Tehran Neighbourhoods. Int. J. Urban Sci. 2020, 24, 397–418. [Google Scholar] [CrossRef]
- Fischer, T.B.; Jha-Thakur, U.; Fawcett, P.; Clement, S.; Hayes, S.; Nowacki, J. Consideration of Urban Green Space in Impact Assessments for Health. Impact Assess. Proj. Apprais. 2018, 36, 32–44. [Google Scholar] [CrossRef] [Green Version]
- Loureiro, A.; Lima, J.; do Partidário, M.R.; Santana, P. Condicionantes Da Saúde Mental e Os Instrumentos de Avaliação de Impactos. In Território e Saúde Mental em Tempos de Crise; Santana, P., Ed.; Imprensa da Universidade de Coimbra: Coimbra, Portugal, 2015; pp. 11–27. [Google Scholar]
- European Union Territorial Agenda 2030. A Future for All Places. Informal Meeting of Ministers Responsible for Spatial Planning and Territorial Development and/or Territorial Cohesion; European Union: Berlin, Germany, 2020. [Google Scholar]
- Santana, P.; Almendra, R.; Pilot, E.; Doreleijers, S.; Krafft, T. Environmental Inequalities in Global Health. In Handbook of Global Health; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 1–19. [Google Scholar]
- Cave, B.; Claßen, T.; Fischer-Bonde, B.; Humboldt-Dachroeden, S.; Martín-Olmedo, P.; Mekel, O.; Pyper, R.; Silva, F.; Viliani, F.; Xiao, Y. Human Health: Ensuring a High Level of Protection. In A Reference Paper on Addressing Human Health in Environmental Impact Assessment (As per EU Directive 2011/92/EU Amended by 2014/52/EU); International Association for Impact Assessment: Washington, DC, USA, 2020. [Google Scholar]
- WHO. Health Impact Assessment: Main Concepts and Suggested Approach (Gothenburg Consensus Paper); WHO: Genea, Switzerland, 1999. [Google Scholar]
- Harris-Roxas, B.; Viliani, F.; Bond, A.; Cave, B.; Divall, M.; Furu, P.; Harris, P.; Soeberg, M.; Wernham, A.; Winkler, M. Health Impact Assessment: The State of the Art. Impact Assess. Proj. Apprais. 2012, 30, 43–52. [Google Scholar] [CrossRef]
- Partidário, M.R. Strategic Environmental Assessment Better Practice Guide Methodological Guidance for Strategic Thinking in SEA; Portuguese Environment Agency and Redes Energéticas Nacionais (REN), SA: Lisbon, Portugal, 2012. [Google Scholar]
- Partidário, M.R. Elements of an SEA Framework— Improving the Added-Value of SEA. Environ. Impact Assess. Rev. 2000, 20, 647–663. [Google Scholar] [CrossRef]
- Partidário, M.R. A Strategic Advocacy Role in SEA for Sustainability. J. Environ. Assess. Policy Manag. 2015, 17, 1550015. [Google Scholar] [CrossRef]
- Quigley, R.; den Broeder, L.; Furu, P.; Bond, A.; Cave, B.; Bos, R. Health Impact Assessment. International Best Practice Principles. Fargo USA Int. Assoc. Impact Assess. 2006, 5, 5–8. [Google Scholar]
- Fischer, T.B.; Matuzzi, M.; Nowacki, J. The Consideration of Health in Strategic Environmental Assessment (SEA). Environ. Impact Assess. Rev. 2010, 30, 200–210. [Google Scholar] [CrossRef]
- Fehr, R.; Viliani, F.; Nowacki, J.; Martuzzi, M. Health in Impact Assessments: Opportunities Not to Be Missed; WHO: Copenhagen, Denmark, 2014. [Google Scholar]
- Joffe, M. The Need for Strategic Health Assessment. Eur. J. Public Health 2008, 18, 439–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Pierre, L. Mental Health in the Field of Health Impact Assessment; Institut national de santé publique: Québec, QC, Canada, 2016. [Google Scholar]
- Lucyk, K.; Gilhuly, K.; Tamburrini, A.-L.; Rogerson, B. Incorporating Mental Health into Health Impact Assessment in the United States: A Systematic Review. J. Public Ment. Health 2016, 15, 150–176. [Google Scholar] [CrossRef]
- Todman, L.C.; Hricisak, L.M.; Fay, J.E.; Sherrod Taylor, J. Mental Health Impact Assessment: Population Mental Health in Englewood, Chicago, Illinois, USA. Impact Assess. Proj. Apprais. 2012, 30, 116–123. [Google Scholar] [CrossRef]
- Kumagai, Y.; Partidario, M. Lasting Community Wellbeing: Comparison of Lisbon and Tokyo. Sustain. Dev. 2019, 27, 84–95. [Google Scholar] [CrossRef] [Green Version]
- Cooke, A.; Friedli, L.; Coggins, T.; Edmonds, N.; Michaelson, J.; O’Hara, K.; Snowden, L.; Stansfield, J.; Nicola Steuer, N.; Scott-Samuel, A. Mental Well-Being Impact Assessment: A Toolkit for Well-Being; National Mental Well-Being Impact Assessment Collaborative: London, UK, 2011. [Google Scholar]
- Lalani, N. Mental Well-Being Impact Assessment: A Primer; The Wellesley Institute: Toronto, ON, Canada, 2011. [Google Scholar]
- Nowacki, J.; Martuzzi, M.; Fischer, T.B. Health and Strategic Environmental Assessment; WHO: Copenhagen, Denmark, 2009. [Google Scholar]
- De Silva, M.J. Making Mental Health an Integral Part of Sustainable Development: The Contribution of a Social Determinants Framework. Epidemiol. Psychiatr. Sci. 2015, 24, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Botezat, I.; Campion, J.; Garcia-Cubillana, P.; Guðmundsdóttir, D.; Halliday, W.; Henderson, N.; Holte, A.; Heitor Santos, M.J.; Japing, K.; Kearney, N.; et al. Mental Health in All Policies. Situation Analysis and Recommendations for Action.; European Union: Brussels, Belgium, 2017. [Google Scholar]
- Harris, P.; Sainsbury, P.; Kemp, L. The Fit between Health Impact Assessment and Public Policy: Practice Meets Theory. Soc. Sci. Med. 2014, 108, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Morrison, J.; Pons-Vigués, M.; Bécares, L.; Burström, B.; Gandarillas, A.; Domínguez-Berjón, F.; Diez, È.; Costa, G.; Ruiz, M.; Pikhart, H.; et al. Health Inequalities in European Cities: Perceptions and Beliefs among Local Policymakers. BMJ Open 2014, 4, e004454. [Google Scholar] [CrossRef] [Green Version]
- Kickbusch, I.; McCann, W.; Sherbon, T. Adelaide Revisited: From Healthy Public Policy to Health in All Policies. Health Promot. Int. 2008, 23, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Leppo, K.; Ollila, E.; Peña, S.; Wismar, M.; Cook, S. Health in All Policies. Seizing Opportunities, Implementing Policies; Ministry of Social Affairs and Health: Helsinki, Finland, 2013. [Google Scholar]
- WHO. Health in All Policies (HiAP) Framework for Country Action; WHO: Genea, Switzerland, 2014. [Google Scholar]
- Soja, E.W. Seeking Spatial Justice; University of Minnesota Press: Minnesota, MN, USA, 2015. [Google Scholar]
- Nieuwenhuijsen, M.J. COVID-19 and the City; from the Short Term to the Long Term. Environ. Res. 2020, 191, 110066. [Google Scholar] [CrossRef]
- United Nations Environment Program. Integrated Strategic Environmental Assessments in Post-Crisis Countries. In A Guidance Note for Integrating Disaster Risk Reduction and Climate Change Adaptation in Sustainable Reconstruction and Development Planning; United Nations Office for Disaster Risk Reduction: Nairobi, Kenya, 2018. [Google Scholar]
- Marmot, M.; Allen, J.; Goldblatt, P.; Herd, E.; Morrison, J. Build Back Fairer: The COVID-19 Marmot Review. The Pandemic, Socioeconomic and Health Inequalities in England; Institute of Health Equity: London, UK, 2020. [Google Scholar]
- Sarchiapone, M.; Lopez-Castroman, J.; Gramaglia, C.; Baca-Garcia, E.; Baralla, F.; Barrigón, M.L.; Bartollino, S.; Beezhold, J.; Bobes, J.; Calati, R.; et al. Increased Risk for Mental Disorders and Suicide during the COVID-19 Pandemic: Position Statement of the Section on Suicidology and Suicide Prevention of the European Psychiatric Association. Glob. Psychiatry 2021, 4, 4–19. [Google Scholar] [CrossRef]
- Green, L.; Ashton, K.; Azam, S.; Dyakova, M.; Clemens, T.; Bellis, M.A. Using Health Impact Assessment (HIA) to Understand the Wider Health and Well-Being Implications of Policy Decisions: The COVID-19 “Staying at Home and Social Distancing Policy” in Wales. BMC Public Health 2021, 21, 1456. [Google Scholar] [CrossRef] [PubMed]
- Almendra, R.; Loureiro, A.; Silva, G.; Vasconcelos, J.; Santana, P. Short-Term Impacts of Air Temperature on Hospitalizations for Mental Disorders in Lisbon. Sci. Total Environ. 2019, 647, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, A.; Santana, P.; Nunes, C.; Almendra, R. The Role of Individual and Neighborhood Characteristics on Mental Health after a Period of Economic Crisis in the Lisbon Region (Portugal): A Multilevel Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2647. [Google Scholar] [CrossRef] [Green Version]
- Santana, P.; Costa, C.; Cardoso, G.; Loureiro, A.; Ferrão, J. Suicide in Portugal: Spatial Determinants in a Context of Economic Crisis. Health Place 2015, 35, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Loureiro, A.; Costa, C.; Almendra, R.; Santana, P. The Socio-Spatial Context as a Risk Factor for Hospitalization Due to Mental Illness in the Metropolitan Areas of Portugal. Cad. Saúde Pública 2015, 31, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Antunes, A.; Azeredo-Lopes, S.; Loureiro, A.; Saraceno, B.; Caldas-de-Almeida, J.M.; Cardoso, G. Factors Associated with Involuntary Psychiatric Hospitalization in Portugal. Int. J. Ment. Health Syst. 2021, 15, 37. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Antunes, A.; Loureiro, A.; Azeredo-Lopes, S.; Saraceno, B.; Caldas-de-Almeida, J.; Cardoso, G. Factors Associated with Length of Stay and Readmission in Acute Psychiatric Inpatient Services in Portugal. Psychiatry Res. 2020, 293, 113420. [Google Scholar] [CrossRef]
- dos Santos, M.J.H.; Miguel, J.M.P. Avaliação Do Impacte de Políticas de Diferentes Sectores Na Saúde e Nos Sistemas de Saúde: Um Ponto de Situação. Rev. Port. De Saúde Pública 2009, 27, 5–17. [Google Scholar]
- de Almeida, T.C.; Heitor, M.J.; Santos, O.; Costa, A.; Virgolino, A.; Rasga, C.; Martiniano, H.; Vicente, A.; Lima, B.; Carreiras, J.; et al. SM-COVID19—Saúde Mental Em Tempos de Pandemia; Instituto Nacional de Saúde Doutor Ricardo Jorge: Lisboa, Portugal, 2020. [Google Scholar]
- Tendais, I.; Ribeiro, A.I. Espaços Verdes Urbanos e Saúde Mental Durante o Confinamento Causado Pela Covid-19. Finisterra—Rev. Port. De Geogr. 2020, 55, 183–188. [Google Scholar] [CrossRef]
- Santana, P.; Costa, C.; Marí-Dell’Olmo, M.; Gotsens, M.; Borrell, C. Mortality, Material Deprivation and Urbanization: Exploring the Social Patterns of a Metropolitan Area. Int. J. Equity Health 2015, 9, 14–55. [Google Scholar] [CrossRef] [Green Version]
- Statistics Portugal Censos 2011—Resultados Definitivos 2012. Available online: https://censos.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=156644135&PUBLICACOESmodo=2 (accessed on 18 May 2021).
- Guite, H.F.; Clark, C.; Ackrill, G. The Impact of the Physical and Urban Environment on Mental Well-Being. Public Health 2006, 120, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Takano, T. Urban Residential Environments and Senior Citizens’ Longevity in Megacity Areas: The Importance of Walkable Green Spaces. J. Epidemiol. Community Health 2002, 56, 913–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gary, T.L.; Stark, S.A.; LaVeist, T.A. Neighborhood Characteristics and Mental Health among African Americans and Whites Living in a Racially Integrated Urban Community. Health Place 2007, 13, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, A.J.; Salmon, C.; Balasubramaniam, P.; Parsons, J.; Singh, G.; Jabbar, A.; Zaidi, Q.; Scott, A.; Nisenbaum, R.; Dunn, J.; et al. Are Residents of Downtown Toronto Influenced by Their Urban Neighbourhoods? Using Concept Mapping to Examine Neighbourhood Characteristics and Their Perceived Impact on Self-Rated Mental Well-Being. Int. J. Health Geogr. 2012, 11, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitley, R.; Prince, M. Fear of Crime, Mobility and Mental Health in Inner-City London, UK. Soc. Sci. Med. 2005, 61, 1678–1688. [Google Scholar] [CrossRef] [PubMed]
- Cromley, E.K.; Wilson-Genderson, M.; Pruchno, R.A. Neighborhood Characteristics and Depressive Symptoms of Older People: Local Spatial Analyses. Soc. Sci. Med. 2012, 75, 2307–2316. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Genderson, M.; Pruchno, R. Effects of Neighborhood Violence and Perceptions of Neighborhood Safety on Depressive Symptoms of Older Adults. Soc. Sci. Med. 2013, 85, 43–49. [Google Scholar] [CrossRef]
- Semenza, J.C.; Krishnasamy, P.V. Design of a Health-Promoting Neighborhood Intervention. Health Promot. Pract. 2007, 8, 243–256. [Google Scholar] [CrossRef]
- Araya, R.; Montgomery, A.; Rojas, G.; Fritsch, R.; Solis, J.; Signorelli, A.; Lewis, G. Common Mental Disorders and the Built Environment in Santiago, Chile. Br. J. Psychiatry J. Ment. Sci. 2007, 190, 394–401. [Google Scholar] [CrossRef]
- Thomas, H.; Weaver, N.; Patterson, J.; Jones, P.; Bell, T.; Playle, R.; Dunstan, F.; Palmer, S.; Lewis, G.; Araya, R. Mental Health and Quality of Residential Environment. Br. J. Psychiatry J. Ment. Sci. 2007, 191, 500–505. [Google Scholar] [CrossRef] [Green Version]
- Gatersleben, B.; Uzzell, D. Affective Appraisals of the Daily Commute. Environ. Behav. 2007, 39, 416–431. [Google Scholar] [CrossRef] [Green Version]
- Wener, R.E.; Evans, G.W. Comparing Stress of Car and Train Commuters. Transp. Res. Part F Traffic Psychol. Behav. 2011, 14, 111–116. [Google Scholar] [CrossRef]
- Preston, J.; Rajé, F. Accessibility, Mobility and Transport-Related Social Exclusion. J. Transp. Geogr. 2007, 15, 151–160. [Google Scholar] [CrossRef]
- Stanley, J.K.; Hensher, D.A.; Stanley, J.R.; Vella-Brodrick, D. Mobility, Social Exclusion and Well-Being: Exploring the Links. Transp. Res. Part A Policy Pract. 2011, 45, 789–801. [Google Scholar] [CrossRef]
- Annerstedt, M.; Ostergren, P.-O.; Björk, J.; Grahn, P.; Skärbäck, E.; Währborg, P. Green Qualities in the Neighbourhood and Mental Health—Results from a Longitudinal Cohort Study in Southern Sweden. BMC Public Health 2012, 12, 337. [Google Scholar] [CrossRef] [Green Version]
- Dalgard, O.S.; Mykletun, A.; Rognerud, M.; Johansen, R.; Zahl, P.H. Education, Sense of Mastery and Mental Health: Results from a Nation Wide Health Monitoring Study in Norway. BMC Psychiatry 2007, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Araya, R. Education and Income: Which Is More Important for Mental Health? J. Epidemiol. Community Health 2003, 57, 501–505. [Google Scholar] [CrossRef] [Green Version]
- Breslin, F.C.; Mustard, C. Factors Influencing the Impact of Unemployment on Mental Health among Young and Older Adults in a Longitudinal, Population-Based Survey. Scand. J. Work. Environ. Health 2003, 29, 5–14. [Google Scholar] [CrossRef]
- Comino, E.J.; Harris, E.; Chey, T.; Manicavasagar, V.; Penrose Wall, J.; Powell Davies, G.; Harris, M.F. Relationship between Mental Health Disorders and Unemployment Status in Australian Adults. Aust. N. Z. J. Psychiatry 2003, 37, 230–235. [Google Scholar] [CrossRef]
- Artazcoz, L.; Benach, J.; Borrell, C.; Cortès, I. Unemployment and Mental Health: Understanding the Interactions among Gender, Family Roles, and Social Class. Am. J. Public Health 2004, 94, 82–88. [Google Scholar] [CrossRef]
- Fone, D.L.; Dunstan, F. Mental Health, Places and People: A Multilevel Analysis of Economic Inactivity and Social Deprivation. Health Place 2006, 12, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Benzeval, M.; Stansfeld, S. Psychological Distress after Employment Transitions: The Role of Subjective Financial Position as a Mediator. J. Epidemiol. Community Health 2007, 61, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Córdoba-Doña, J.A.; San Sebastián, M.; Escolar-Pujolar, A.; Martínez-Faure, J.E.; Gustafsson, P.E. Economic Crisis and Suicidal Behaviour: The Role of Unemployment, Sex and Age in Andalusia, Southern Spain. Int. J. Equity Health 2014, 13, 55. [Google Scholar] [CrossRef] [PubMed]
- Hämmig, O.; Bauer, G.F. The Social Gradient in Work and Health: A Cross-Sectional Study Exploring the Relationship between Working Conditions and Health Inequalities. BMC Public Health 2013, 13, 1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, K.; Frech, A.; Carlson, D.L. Marital Status and Mental Health. In A Handbook for the Study of Mental Health; Scheid, T.L., Brown, T.N., Eds.; Cambridge University Press: Cambridge, UK, 2012; pp. 306–320. [Google Scholar]
- Lindström, M.; Rosvall, M. Marital Status, Social Capital, Economic Stress, and Mental Health: A Population-Based Study. Soc. Sci. J. 2012, 49, 339–342. [Google Scholar] [CrossRef] [Green Version]
- Cannuscio, C.C.; Weiss, E.E.; Asch, D.A. The Contribution of Urban Foodways to Health Disparities. J. Urban Health 2010, 87, 381–393. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.-C.; Matthews, S.A. The Role of Social and Built Environments in Predicting Self-Rated Stress: A Multilevel Analysis in Philadelphia. Health Place 2010, 16, 803–810. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.; Taylor, K.; Wheatley Price, S. Debt and Distress: Evaluating the Psychological Cost of Credit. J. Econ. Psychol. 2005, 26, 642–663. [Google Scholar] [CrossRef]
- Lee, S.; Guo, W.J.; Tsang, A.; Mak, A.D.P.; Wu, J.; Ng, K.L.; Kwok, K. Evidence for the 2008 Economic Crisis Exacerbating Depression in Hong Kong. J. Affect. Disord. 2010, 126, 125–133. [Google Scholar] [CrossRef]
- Gili, M.; Roca, M.; Basu, S.; McKee, M.; Stuckler, D. The Mental Health Risks of Economic Crisis in Spain: Evidence from Primary Care Centres, 2006 and 2010. Eur. J. Public Health 2013, 23, 103–108. [Google Scholar] [CrossRef]
- Zhang, J.X.; Ho, S.C.; Woo, J. Assessing Mental Health and Its Association with Income and Resource Utilization in Old-Old Chinese in Hong Kong. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2005, 13, 236–243. [Google Scholar] [CrossRef]
- Sundquist, K.; Ahlen, H. Neighbourhood Income and Mental Health: A Multilevel Follow-up Study of Psychiatric Hospital Admissions among 4.5 Million Women and Men. Health Place 2006, 12, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Fone, D.; Dunstan, F.; Williams, G.; Lloyd, K.; Palmer, S. Places, People and Mental Health: A Multilevel Analysis of Economic Inactivity. Soc. Sci. Med. 2007, 64, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Orpana, H.; Lemyre, L.; Gravel, R. Income and Psychological Distress: The Role of the Social Environment. Stat. Can. Health Rep. 2009, 20, 1–8. [Google Scholar]
- Fukuda, Y.; Hiyoshi, A. Influences of Income and Employment on Psychological Distress and Depression Treatment in Japanese Adults. Environ. Health Prev. Med. 2012, 17, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, R.; Sherwood, P.R. Physical and Mental Health Effects of Family Caregiving. AJN Am. J. Nurs. 2008, 108, 23–27. [Google Scholar] [CrossRef]
- Myer, L.; Stein, D.J.; Grimsrud, A.; Seedat, S.; Williams, D.R. Social Determinants of Psychological Distress in a Nationally-Representative Sample of South African Adults. Soc. Sci. Med. 2008, 66, 1828–1840. [Google Scholar] [CrossRef] [Green Version]
- Fone, D.; Dunstan, F.; Lloyd, K.; Williams, G.; Watkins, J.; Palmer, S. Does Social Cohesion Modify the Association between Area Income Deprivation and Mental Health? A Multilevel Analysis. Int. J. Epidemiol. 2007, 36, 338–345. [Google Scholar] [CrossRef] [Green Version]
- Fone, D.; Dunstan, F.; John, A.; Lloyd, K. Associations between Common Mental Disorders and the Mental Illness Needs Index in Community Settings. Multilevel Analysis. Br. J. Psychiatry J. Ment. Sci. 2007, 191, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Rios, R.; Aiken, L.S.; Zautra, A.J. Neighborhood Contexts and the Mediating Role of Neighborhood Social Cohesion on Health and Psychological Distress among Hispanic and Non-Hispanic Residents. Ann. Behav. Med. 2012, 43, 50–61. [Google Scholar] [CrossRef]
- Lee, M.A. Neighborhood Residential Segregation and Mental Health: A Multilevel Analysis on Hispanic Americans in Chicago. Soc. Sci. Med. 2009, 68, 1975–1984. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, A.; Moreira-Almeida, A.; Menezes, P.; Vallada, H.; Scazufca, M. Investigating the Role Played by Social Support in the Association between Religiosity and Mental Health in Low Income Older Adults: Results from the São Paulo Ageing & Health Study (SPAH). Rev. Bras. De Psiquiatr. 2010, 33, 157–164. [Google Scholar]
- Tsai, J.; Thompson, E. Impact of Social Discrimination, Job Concerns, and Social Support on Filipino Immigrant Worker Mental Health and Substance Use. Am. J. Ind. Med. 2013, 56, 1082–1094. [Google Scholar] [CrossRef] [PubMed]
- Quinn, N.; Biggs, H. Creating Partnerships to Improve Community Mental Health and Well-Being in an Area of High Deprivation: Lessons from a Study with Highrise Flat Residents in East Glasgow. J. Public Ment. Health 2010, 9, 16–21. [Google Scholar] [CrossRef]
- Poblete, F.; Sapag, J.; Bossert, T. Capital Social y Salud Mental En Comunidades Urbanas de Nivel Socioeconómico Bajo, En Santiago, Chile. Nuevas Formas de Entender La Relación Comunidad-Salud. Rev. Méd. Chile 2008, 136, 230–239. [Google Scholar] [CrossRef]
- Hamano, T.; Fujisawa, Y.; Ishida, Y.; Subramanian, S.V.; Kawachi, I.; Shiwaku, K. Social Capital and Mental Health in Japan: A Multilevel Analysis. PLoS ONE 2010, 5, e13214. [Google Scholar] [CrossRef]
- Ferreira, P.L.; Noronha Ferreira, L.; Nobre Pereira, L. Medidas Sumário Física e Mental de Estado de Saúde Para a População Portuguesa. Rev. Port. Saude Publica 2012, 30, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med. Care 1992, 6, 473–483. [Google Scholar] [CrossRef]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B. SF-36 Health Survey Manual and Interpretation Guide; The Health Institute, New England Medical Center: Boston, UK, 1993; Volume 1, ISBN 1891810065. [Google Scholar]
- Partidário, M.R. Strategic Thinking for Sustainability in SEA. In Handbook on Strategic Environmental Assessment; Fischer, T., Gonzalez, A., Eds.; Edward Elgar Research Handbooks of Impact Assessment Series: Cheltenham, UK, 2021; pp. 41–57. [Google Scholar]
- WHO; Calouste Gulbenkian Foundation. Social Determinants of Mental Health; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Barton, H.; Thompson, S.; Burgess, S.; Grant, M. (Eds.) The Routledge Handbook of Planning for Health and Well-Being. In Shaping a Sustainable and Healthy Future; Routledge: Oxfordshire, UK, 2015. [Google Scholar]
- Villeneau, L.; Morris, D.; Parkman, S.; Wolf, J.; McCulloch, A. On Your Doorstep: Community Organisations and Mental Health; Sainsbury: London, UK, 2001. [Google Scholar]
- Korkeila, J.; Lehtinen, V.; Bijl, R.; Dalgard, O.-S.; Kovess, V.; Morgan, A.; Salize, H.J. Review Article: Establishing a Set of Mental Health Indicators for Europe. Scand. J. Public Health 2003, 31, 451–459. [Google Scholar] [CrossRef]
- Lahtinen, E.; Lehtinen, V.; Riikonen, E.; Ahonen, J. (Eds.) Framework for Promoting Mental Health in Europe; STAKES National Research and Development Center for Welfare and Health Ministery of Social Affairs and Health: Hamina, Finland, 1999; ISBN 951-33-0823-5. [Google Scholar]
- Parkinson, J. Establishing National Mental Health and Well-being Indicators for Scotland. J. Public Ment. Health 2006, 5, 42–48. [Google Scholar] [CrossRef]
- Parkinson, J. Establishing a Core Set of National, Sustainable Mental Health Indicators for Adults in Scotland: Final Report.; NHS Health Scotland: Glasgow, Scotland, 2007. [Google Scholar]
- Orpana, H.; Vachon, J.; Dykxhoorn, J.; McRae, L.; Jayaraman, G. Monitoring Positive Mental Health and Its Determinants in Canada: The Development of the Positive Mental Health Surveillance Indicator Framework. Health Promot. Chronic Dis. Prev. Can. 2016, 36, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajrasoulih, A.; del Rio, V.; Francis, J.; Edmondson, J. Urban Form and Mental Wellbeing: Scoping a Theoretical Framework for Action. J. Urban Des. Ment. Health 2018, 5, 1–10. [Google Scholar]
- King, J. Air Pollution, Mental Health, and Implications for Urban Design: A Review. J. Urban Des. Ment. Health 2018, 4, 1–6. [Google Scholar]
- Baranyi, G. Neighbourhood Conditions and Mental Health: Time and Space over the Life Course; The University of Edinburgh: Edinburgh, Scotland, 2017. [Google Scholar]
- Mair, C.; Diez Roux, A.V.; Galea, S. Are Neighbourhood Characteristics Associated with Depressive Symptoms? A Review of Evidence. J. Epidemiol. Community Health 2008, 62, 940–946. [Google Scholar] [PubMed]
- McCormack, G.R.; Shiell, A. In Search of Causality: A Systematic Review of the Relationship between the Built Environment and Physical Activity among Adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Santana, P.; Santos, R.; Costa, C.; Roque, N.; Loureiro, A. Crime Impacts of Urban Design. TRIA 2010, 5, 39–48. [Google Scholar]
- Baranyi, G.; Di Marco, M.H.; Russ, T.C.; Dibben, C.; Pearce, J. The Impact of Neighbourhood Crime on Mental Health: A Systematic Review and Meta-Analysis. Soc. Sci. Med. 2021, 282, 114106. [Google Scholar] [CrossRef]
- Beyer, F.R.; Ker, K. Street Lighting for Preventing Road Traffic Injuries. Cochrane Database Syst. Rev. 2009, 21, 1–57. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, T.; Ward Thompson, C.; Alves, S. Associations between Neighborhood Open Space Attributes and Quality of Life for Older People in Britain. Environ. Behav. 2009, 41, 3–12. [Google Scholar] [CrossRef]
- Annear, M.; Keeling, S.; Wilkinson, T.; Cushman, G.; Gidlow, B.; Hopkins, H. Environmental Influences on Healthy and Active Ageing: A Systematic Review. Ageing Soc. 2014, 34, 590–622. [Google Scholar] [CrossRef]
- Gascon, M.; Mas, M.T.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental Health Benefits of Long-Term Exposure to Residential Green and Blue Spaces: A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calogiuri, G.; Chroni, S. The Impact of the Natural Environment on the Promotion of Active Living: An Integrative Systematic Review. BMC Public Health 2014, 14, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.C.K.; Maheswaran, R. The Health Benefits of Urban Green Spaces: A Review of the Evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Myron, R.; Stansfeld, S.; Candy, B. A Systematic Review of the Evidence on the Effect of the Built and Physical Environment on Mental Health. J. Public Ment. Health 2007, 6, 14–27. [Google Scholar] [CrossRef]
- Foster, S.; Giles-Corti, B.; Knuiman, M. Does Fear of Crime Discourage Walkers? A Social-Ecological Exploration of Fear As a Deterrent to Walking. Environ. Behav. 2014, 46, 698–717. [Google Scholar] [CrossRef]
- Davison, K.K.; Lawson, C.T. Do Attributes in the Physical Environment Influence Children’s Physical Activity? A Review of the Literature. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Dunton, G.F.; Kaplan, J.; Wolch, J.; Jerrett, M.; Reynolds, K.D. Physical Environmental Correlates of Childhood Obesity: A Systematic Review. Obes. Rev. 2009, 10, 393–402. [Google Scholar] [CrossRef] [Green Version]
- Hunter, R.F.; Christian, H.; Veitch, J.; Astell-Burt, T.; Hipp, J.A.; Schipperijn, J. The Impact of Interventions to Promote Physical Activity in Urban Green Space: A Systematic Review and Recommendations for Future Research. Soc. Sci. Med. 2015, 124, 246–256. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.R.; Petitot, C. Ageing and Urbanization: Can Cities Be Designed to Foster Active Ageing? Public Health Rev. 2010, 32, 427–450. [Google Scholar] [CrossRef] [Green Version]
- Francis, J.; Giles-Corti, B.; Wood, L.; Knuiman, M. Creating Sense of Community: The Role of Public Space. J. Environ. Psychol. 2012, 32, 401–409. [Google Scholar] [CrossRef]
- Francis, J.; Wood, L.J.; Knuiman, M.; Giles-Corti, B. Quality or Quantity? Exploring the Relationship between Public Open Space Attributes and Mental Health in Perth, Western Australia. Soc. Sci. Med. 2012, 74, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Nieuwenhuijsen, M.J. Urban Greenspace, Transportation, and Health. In International Encyclopedia of Transportation; Elsevier: Amsterdam, The Netherlands, 2021; pp. 327–334. [Google Scholar]
- BC Centre for Disease Control. Healthy Built Environment Linkages Toolkit: Making the Links between Design, Planning and Health, Version 2.0; Provincial Health Services Authority: Vancouver, BC, Canada, 2018. [Google Scholar]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Owen, N.; Giles-Corti, B. Public Open Space, Physical Activity, Urban Design and Public Health: Concepts, Methods and Research Agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, A.; McGaw-Césaire, J.; Petrokofsky, C. Spatial Planning for Health: An Evidence Resource for Planning and Designing Healthier Places; Public Health England: London, UK, 2017. [Google Scholar]
- Department of Health—UK Government. Making It Happen:A Guide to Delivering Mental Health Promotion; Department of Health-UK Government: London, UK, 2001.
- Russell, H.; Killoran, A. Public Health and Regeneration: Making the Links; Health Education: London, UK, 2000; ISBN 0752118048. [Google Scholar]
- Vert, C.; Sánchez-Benavides, G.; Martínez, D.; Gotsens, X.; Gramunt, N.; Cirach, M.; Molinuevo, J.L.; Sunyer, J.; Nieuwenhuijsen, M.J.; Crous-Bou, M.; et al. Effect of Long-Term Exposure to Air Pollution on Anxiety and Depression in Adults: A Cross-Sectional Study. Int. J. Hyg. Environ. Health 2017, 220, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- South, E.C.; Hohl, B.C.; Kondo, M.C.; MacDonald, J.M.; Branas, C.C. Effect of Greening Vacant Land on Mental Health of Community-Dwelling Adults. JAMA Netw. Open 2018, 1, e180298. [Google Scholar] [CrossRef] [Green Version]
- Mair, C.; Diez Roux, A.V.; Morenoff, J.D. Neighborhood Stressors and Social Support as Predictors of Depressive Symptoms in the Chicago Community Adult Health Study. Health Place 2010, 16, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Garvin, E.; Branas, C.; Keddem, S.; Sellman, J.; Cannuscio, C. More Than Just An Eyesore: Local Insights And Solutions on Vacant Land And Urban Health. J. Urban Health 2013, 90, 412–426. [Google Scholar] [CrossRef] [Green Version]
- Woodward, A.; Samet, J. Active Transport: Exercise Trumps Air Pollution, Almost Always. Prev. Med. 2016, 87, 237–238. [Google Scholar] [CrossRef]
- Elliott, I. Poverty and Mental Health: A Review to Inform the Joseph Rowntree Foundation’s Anti-Poverty Strategy; Mental Health Foundation: London, UK, 2016. [Google Scholar]
- Hyde, M.; Phillipson, C. How Can Lifelong Learning, Including Continuous Training within the Labour Market, Be Enabled and Who Will Pay for This? Looking Forward to 2025 and 2040 How Might This Evolve? Foresight, Government Office for Science: London, UK, 2015. [Google Scholar]
- UNESCO Institute for Lifelong Learning. Learning Cities and the SDGs: A Guide to Action; UNESCO Institute for Lifelong Learning: Hamburgo, Germany, 2017. [Google Scholar]
- Zajacova, A.; Lawrence, E.M. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu. Rev. Public Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [Green Version]
- Motoyama, Y.; Wiens, J. Guidelines for Local and State Governments to Promote Entrepreneurship; Kauffman Foundation Research Series on City, Metro, and Regional Entrepreneurship: Kansas City, MO, USA, 2015. [Google Scholar]
- Srinivas, H. The Role of Local Governments in Fostering Business Partnerships for Environmental Sustainability. GDRC Res. Output 2016, E-076, 1–8. [Google Scholar]
- Hatak, I.; Zhou, H. Health as Human Capital in Entrepreneurship: Individual, Extension, and Substitution Effects on Entrepreneurial Success. Entrep. Theory Pract. 2021, 45, 18–42. [Google Scholar] [CrossRef] [Green Version]
- Leyden, K.M.; Goldberg, A.; Michelbach, P. Understanding the Pursuit of Happiness in Ten Major Cities. Urban Aff. Rev. 2011, 47, 861–888. [Google Scholar] [CrossRef]
- McCrea, R.; Shyy, T.K.; Stimson, R. What Is the Strength of the Link between Objective and Subjective Indicators of Urban Quality of Life? Appl. Res. Qual. Life 2006, 1, 79–96. [Google Scholar] [CrossRef]
- Menec, V.H.; Brown, C.L.; Newall, N.E.G.; Nowicki, S. How Important Is Having Amenities Within Walking Distance to Middle-Aged and Older Adults, and Does the Perceived Importance Relate to Walking? J. Aging Health 2016, 28, 546–567. [Google Scholar] [CrossRef] [PubMed]
- Fraser, S.D.S.; Lock, K. Cycling for Transport and Public Health: A Systematic Review of the Effect of the Environment on Cycling. Eur. J. Public Health 2011, 21, 738–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padeiro, M. Comparing Alternative Methods to Measuring Pedestrian Access to Community Pharmacies. Health Serv. Outcomes Res. Methodol. 2018, 18, 1–16. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.M. Importance of Proximity to Resources, Social Support, Transportation and Neighborhood Security for Mobility and Social Participation in Older Adults: Results from a Scoping Study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing Walking. Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Bull, F.; Knuiman, M.; McCormack, G.; Van Niel, K.; Timperio, A.; Christian, H.; Foster, S.; Divitini, M.; Middleton, N.; et al. The Influence of Urban Design on Neighbourhood Walking Following Residential Relocation: Longitudinal Results from the RESIDE Study. Soc. Sci. Med. 2013, 77, 20–30. [Google Scholar] [CrossRef] [Green Version]
- Koohsari, M.J.; Kaczynski, A.T.; Giles-Corti, B.; Karakiewicz, J.A. Effects of Access to Public Open Spaces on Walking: Is Proximity Enough? Landsc. Urban Plan. 2013, 117, 92–99. [Google Scholar] [CrossRef]
- Boulange, C.; Gunn, L.; Giles-Corti, B.; Mavoa, S.; Pettit, C.; Badland, H. Examining Associations between Urban Design Attributes and Transport Mode Choice for Walking, Cycling, Public Transport and Private Motor Vehicle Trips. J. Transp. Health 2017, 6, 155–166. [Google Scholar] [CrossRef]
- Lee, K.; Fernandes, F.; Ng, M.; Reznikov, V.-E.; Poos, M. Urban Design and Mental Health in Toronto, Canada: A City Case Study. J. Urban Des. Ment. Health 2020, 6, 1–12. [Google Scholar]
- Freeman, H. Mental Health and the Environment; Freeman, H., Ed.; Churchill Livingstone: London, UK, 1984. [Google Scholar]
- Dalgard, O.S.; Tambs, K. Urban Environment and Mental Health. A Longitudinal Study. Br. J. Psychiatry 1997, 171, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Melis, G.; Gelormino, E.; Marra, G.; Ferracin, E.; Costa, G. The Effects of the Urban Built Environment on Mental Health: A Cohort Study in a Large Northern Italian City. Int. J. Environ. Res. Public Health 2015, 12, 14898–14915. [Google Scholar] [CrossRef]
- Boyko, C.T.; Cooper, R. Density and Mental Wellbeing. In Wellbeing; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2014; pp. 1–22. [Google Scholar]
- Harris-Roxas, B.; Simpson, S.; Harris, L. Equity Focused Health Impact Assessment: A Literature Review; Centre for Health Equity Training Research and Evaluation: Sidney, Australia, 2004. [Google Scholar]
- Steptoe, A.; Di Gessa, G. Mental Health and Social Interactions of Older People with Physical Disabilities in England during the COVID-19 Pandemic: A Longitudinal Cohort Study. Lancet Public Health 2021, 6, e365–e373. [Google Scholar] [CrossRef]
- da Conceição, V.; Rothes, I.; Gusmão, R.; Barros, H. Depression and Anxiety before and during the COVID-19 Lockdown: A Longitudinal Cohort Study with University Students. medRxiv 2021. [Google Scholar] [CrossRef]
- Cherrie, M.; Curtis, S.; Baranyi, G.; Cunningham, N.; Dibben, C.; Bambra, C.; Pearce, J. A Data Linkage Study of the Effects of the Great Recession and Austerity on Antidepressant Prescription Usage. Eur. J. Public Health 2021, 31, 297–303. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The Outbreak of COVID-19 Coronavirus and Its Impact on Global Mental Health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Bert, F.; Scaioli, G.; Gualano, M.R.; Siliquini, R. How Can We Bring Public Health in All Policies? Strategies for Healthy Societies. J. Public Health Res. 2015, 4, 393. [Google Scholar] [CrossRef] [Green Version]
- Partidario, M.R. Transforming the Capacity of Impact Assessment to Address Persistent Global Problems. Impact Assess. Proj. Apprais. 2020, 38, 146–150. [Google Scholar] [CrossRef]
- Public Health England. Health Impact Assessment in Spatial Planning. In A Guide for Local Authority Public Health and Planning Teams; Public Health England: London, UK, 2020. [Google Scholar]
- Dunstan, F.; Fone, D.L.; Glickman, M.; Palmer, S. Objectively Measured Residential Environment and Self-Reported Health: A Multilevel Analysis of UK Census Data. PLoS ONE 2013, 8, e69045. [Google Scholar] [CrossRef]
- Rega, C.; Baldizzone, G. Public Participation in Strategic Environmental Assessment: A Practitioners’ Perspective. Environ. Impact Assess. Rev. 2015, 50, 105–115. [Google Scholar] [CrossRef]
- Freitas, Â.; Rodrigues, T.C.; Santana, P. Assessing Urban Health Inequities through a Multidimensional and Participatory Framework: Evidence from the EURO-HEALTHY Project. J. Urban Health 2020, 97, 857–875. [Google Scholar] [CrossRef] [PubMed]
- Jokela, M. Are Neighborhood Health Associations Causal? A 10-Year Prospective Cohort Study With Repeated Measurements. Am. J. Epidemiol. 2014, 180, 776–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDaid, S.; Kousoulis, A. Tackling Social Inequalities to Reduce Mental Health Problems: How Everyone Can Flourish Equally; Mental Health Foundation: UK, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lisbon | Amadora | Oeiras | Mafra | |
|---|---|---|---|---|
| Population density (inhab./km2) 2020 | 5093.4 | 7799.8 | 3875.0 | 292.5 |
| Population variation (%) 1991–2011 | −17.5 | −3.8 | 13.7 | 75.4 |
| Population under 15 years old (%) 2020 | 16.9 | 15.8 | 15.1 | 16.1 |
| Elderly living alone (%) 2011 | 15.0 | 10.8 | 10.6 | 7.8 |
| Population of foreign nationality (%) 2011 | 5.8 | 10.2 | 5.4 | 4.8 |
| Unemployment rate (%) 2011 | 11.8 | 15.0 | 10.8 | 9.1 |
| School leavers rate (%) 2011 | 1.8 | 2.7 | 1.2 | 1.4 |
| Population with higher education (%) 2011 | 33.6 | 16.3 | 33.4 | 17.4 |
| Overcrowded living quarters (%) 2011 | 12.1 | 17.7 | 11.4 | 9.9 |
| Population living in small areas with high material deprivation (%) 2001 [63] | 9.6 | 19.34 | 0.0 | 9.4 |
| Neighbourhood Environmental Characteristics and Scientific Literature References (Association with Mental Health) | Survey Categories | ||
|---|---|---|---|
| Physical and built environment | Satisfaction with residence area [65,66,67,68,69,70,71,72] | Health facilities and services | Not satisfied; Satisfied |
| Educational facilities and services | Not satisfied; Satisfied | ||
| Sports facilities and services | Not satisfied; Satisfied | ||
| Cultural facilities and services | Not satisfied; Satisfied | ||
| Associative and community facilities (e.g., associations, recreation centres, clubs) | Not satisfied; Satisfied | ||
| Public transport facilities and services | Not satisfied; Satisfied | ||
| Parking | Not satisfied; Satisfied | ||
| Outdoor leisure facilities and services | Not satisfied; Satisfied | ||
| Local commerce | Not satisfied; Satisfied | ||
| Safety | Not satisfied; Satisfied | ||
| Environmental Quality [73,74] | Indoor noise levels (at home) | Not satisfied; Satisfied | |
| Outdoor noise levels | Not satisfied; Satisfied | ||
| Outdoor air quality | Not satisfied; Satisfied | ||
| Urban cleanliness (e.g., garbage collection) | Not satisfied; Satisfied | ||
| Mobility and Transports [75,76,77,78] | Type of transport used for commuting | Motorized; non-motorized | |
| Private motorized; Not motorized or public | |||
| Average travel time for daily commuting | <20 min; ≥20 min | ||
| Green Spaces [17,79] | Use | Yes; No | |
| Proximity to residence | Use of the nearest green space; Not using the nearest green space | ||
| Frequency of use | Monthly or less; Weekly; Daily | ||
| Usefulness of the existence near the residence | Yes; No | ||
| Socioeconomic environment | Education [80,81] | ≤12 years; >12 years | |
| Labour [82,83,84,85,86,87,88] | Professional status | Unemployed; Employed; Student; Retired; Homemaker | |
| Type of profession | Manual worker; Non manual worker; Unqualified manual worker | ||
| Unemployment in the last three years | Yes; No | ||
| Unemployed in the family | Yes; No | ||
| Satisfaction with the job offer in the area of residence | Not satisfied; Satisfied | ||
| Marital status [89,90] | Single; Married; Divorced; Widow(er) | ||
| Household and surrounding financial situation [91,92,93,94,95] | Difficulty in paying expenses | Difficulty in paying expenses; Able to pay current expenses only; Able to save money | |
| Concern about expenses | More concerned with expenses; Less concerned with expenses | ||
| Main expense of thehousehold budget | Health expenses; Education expenses; Housing expenses | ||
| Family member, friend, neighbour with difficulty paying expenses | Yes; No | ||
| Household income [96,97,98,99,100] | ≤500 €; >500 € | ||
| Dependent persons [101] | Dependent children; Other dependents; No dependents | ||
| Social and cultural interaction environment | Sense of belonging and identity [102,103] | Like living in the neighbourhood | Like; Dislike |
| Residence time in the neighbourhood | ≤5 years; >5 years | ||
| Family and community relational support [102,104,105,106,107,108] | Relationship with neighbours | Bad/without relation; Good relation | |
| Financial support | Neighbours; Family and Friends; Bank; Social Solidarity Institutions; Nobody | ||
| Emotional support | Neighbours; Family and Friends; Health Professionals; Social Solidarity Institutions; Nobody | ||
| Isolation [109] | Living alone | Yes; No | |
| Trust in public institutions [110,111] | Voting in the last municipal elections | Yes; No | |
| Voting in the last parliamentary elections | Yes; No | ||
| Variables | Categories | n | % |
|---|---|---|---|
| Gender | Female | 573 | 53.8% |
| Male | 493 | 46.2% | |
| Age group | 18–29 | 172 | 16.1% |
| 30–44 | 319 | 29.9% | |
| 45–59 | 246 | 23.1% | |
| 60–74 | 202 | 19.0% | |
| ≥75 | 127 | 11.9% | |
| Educational level | ≤12 years | 770 | 72.2% |
| >12 years | 296 | 27.8% | |
| Mental health | Good mental health (score > 50) | 715 | 67.1% |
| Poor mental health (score ≤ 50) | 351 | 32.9% | |
| Household Income | ≤700 € | 403 | 37.8% |
| 701 €–1200 € | 281 | 26.4% | |
| 1201 €–2000 € | 229 | 21.5% | |
| >2000 € | 153 | 14.4% |
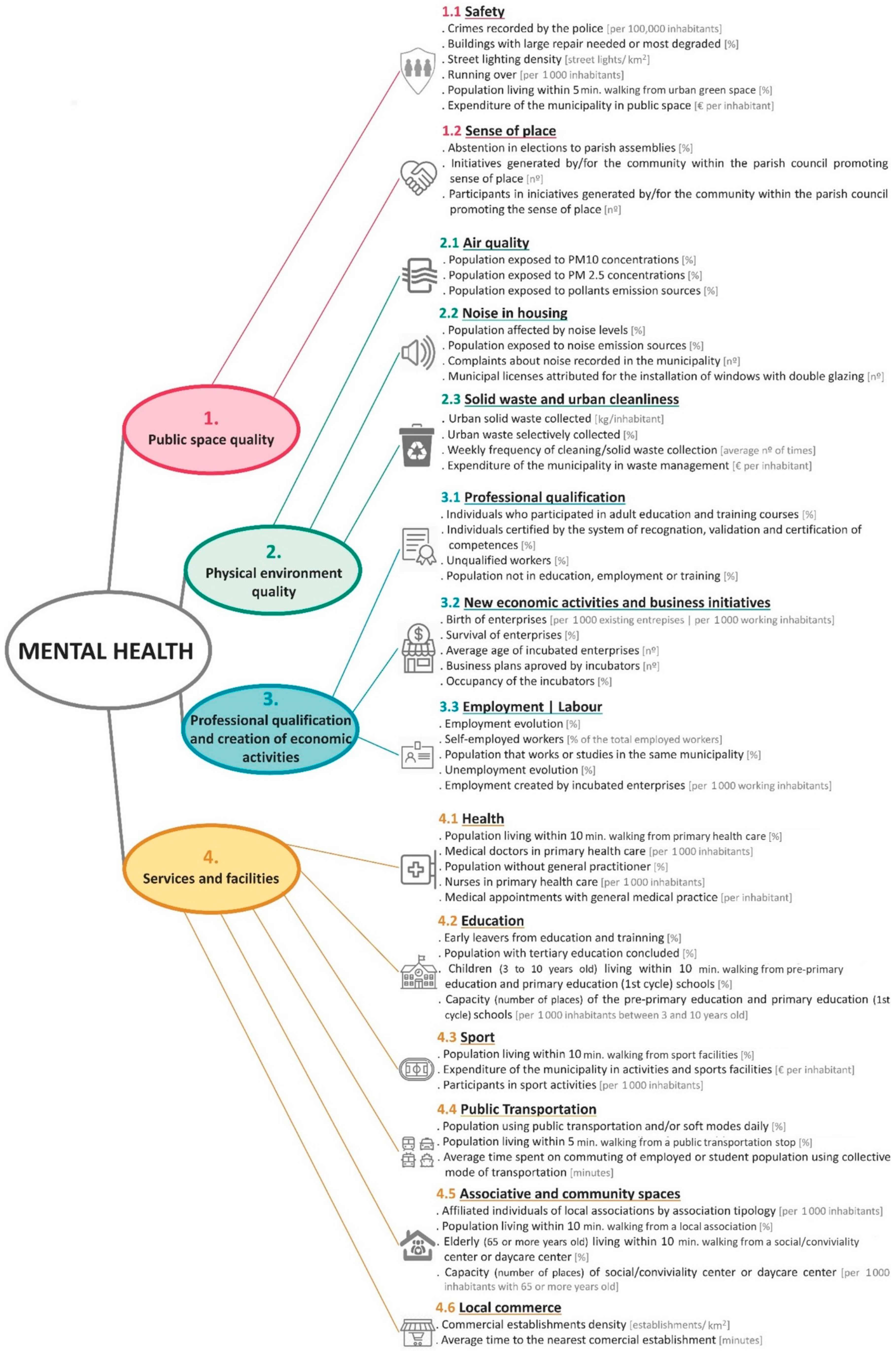
| Critical Decision Factors (CDF) | Assessment Criteria (AC) | Indicators | Units |
|---|---|---|---|
| 1. Public space quality Access, characteristics and elements of public space that ensure opportunities to make healthy choices, promoting
| 1.1 Safety Assessment of the quality and functionality of public space, considering the elements of the space that promote feelings of security, namely the presence of urban furniture, lighting, maintenance and cleanliness of the space, the interior/exterior relationship of buildings, among other characteristics. | Crimes recorded by the police: pickpocketing, robbery on public roads, theft of vehicles, burglary, theft in establishments | Per 100,000 inhabitants |
| Buildings with large repair needed or most degraded | % | ||
| Street lighting density | Streetlights/km2 | ||
| Running over | Per 1000 inhabitants | ||
| Resident population living within 5 min. walking distance of urban green space | % | ||
| Expenditure of the municipality on public space | € per inhabitant | ||
| 1.2 Sense of place Assessment of the contribution of the sense of place to social interaction, generation of feelings of common identity and belonging to the community, relationships of trust, help and cooperation and combating social isolation, recognizing proximity networks, as well as community responsibilities for the quality of public space and its heritage/patrimonial elements. | Abstention in elections to parish assemblies | % | |
| Initiatives generated by/for the community within the parish council promoting sense of place | N° | ||
| Participants in initiatives generated by/for the community within the parish council promoting sense of place | N° | ||
| 2. Physical environment quality Characteristics and elements of the physical and natural environment that support human life, such as:
| 2.1 Air quality Assessment of air quality, namely levels of pollutants from traffic, industries and works. | Resident population exposed to PM10 concentrations | % |
| Resident population exposed to PM2.5 concentrations | % | ||
| Population exposed to pollutants emission sources | % | ||
| 2.2 Noise in housing Assessment of outdoor noise levels, that are perceived indoor particularly from traffic, construction sites and the neighbourhood. | Resident population affected by noise levels | % | |
| Population exposed to noise emission sources | % | ||
| Complaints about noise recorded in the municipality | N° | ||
| Municipal licenses attributed for the installation of windows with double glazing | N° | ||
| 2.3 Solid waste and urban cleanliness Assessment of the cleanliness of public space, namely the management of solid urban waste and works. | Urban solid waste collected | kg/inhabitants | |
| Urban waste selectively collected | % | ||
| Weekly frequency of cleaning/solid waste collection | Average n° of times | ||
| Expenditure of the municipality on waste management | € per inhabitant | ||
| 3. Professional qualification and creation of economic activities Training opportunities and qualification of individuals and local economic dynamics, including:
| 3.1 Professional qualification Assessment of initiatives for lifelong learning. | Individuals (18 and over) who participated in adult education and training courses | % |
| Individuals (18 and over) certified by the system of recognition, validation and certification of competences | % | ||
| Unqualified workers | % | ||
| Resident population not in education, employment, or training | % | ||
| 3.2 New economic activities and business initiatives Assessment of the capacity to attract new investments and economic activities to the territory, including conditions for the generation of business initiatives (e.g., incubators, start-ups) and the capacity to host/install these initiatives in the territory. | Birth of enterprises | % | |
| Survival of enterprises | % | ||
| Average age of incubated enterprises | N° | ||
| Business plans approved by incubators | N° | ||
| Occupancy of the incubators | % | ||
| 3.3 Employment|Labour Assessment of job creation and maintenance in the territory. | Employment evolution | % | |
| Self-employed workers | % | ||
| Resident population that works or studies in the same municipality | % | ||
| Unemployment evolution | % | ||
| Employment created by incubated enterprises | % | ||
| 4. Services and facilities Offer, access and quality of services and facilities supporting community activities | 4.1 Health Assessment of the offer, access and quality of health services and facilities, namely the walking proximity to the residence. | Population living within 10 min. walking distance to primary health care | % |
| Medical doctors in primary health care | Per 1000 inhabitants | ||
| Resident population without general practitioner/family doctor | % | ||
| Nurses in primary health care | Per 1000 inhabitants | ||
| Medical appointments with general medical practice and family medicine | Per inhabitant | ||
| 4.2 Education Assessment of the offer, access and quality of education services and facilities, namely the walking proximity to the residence. | Early leavers from education and training | % | |
| Population with tertiary education concluded | % | ||
| Children (3 to 10 years old) living within 10 min. walking from pre-primary education and primary education (1st cycle) schools | % | ||
| Capacity (number of places) of the pre-primary education and primary education (1st cycle) schools | Per 1000 inhabitants between 3 and 10 years old | ||
| 4.3 Sport Assessment of the offer, access and quality of services and sports facilities, considering their contribution to the practice of physical exercise and active social life. | Population living within 10 min. walking distance to sports facilities | % | |
| Expenditure of the municipality on activities and sports facilities | € per inhabitant | ||
| Participants in sport activities | Per 1000 inhabitants | ||
| 4.4 Public Transport Assessment of the offer, access and quality of public transport services and facilities, valuing the functional proximity and the complementarity of transport systems (e.g., smooth mobility). | Population using public transportation and/or active (soft) modes daily | % | |
| Population living within 5 min. walking distance to a public transportation stop | % | ||
| Average time spent commuting of employed or student resident population using collective mode of transport | Minutes | ||
| 4.5 Associative and community spaces Assessment of the offer, access and quality of the associative/community spaces, namely those that encourage involvement in the community/society, combating social isolation and loneliness. | Affiliated individuals of local associations by association typology | Per 1000 inhabitants | |
| Population living within 10 min. walking distance to a local association | % | ||
| Elderly (65 or over) living within 5 min. walking distance to social/conviviality centre or daycare centre | % | ||
| Capacity (number of places) of social/conviviality centre or daycare centre | Per 1000 inhabitants with 65 or more years old | ||
| 4.6 Local commerce Assessment of the offer and access to trade services, namely the walking proximity to the residence and its integration into mixed land use. | Commercial establishments density | Establishments /km2 | |
| Average time to nearest commercial establishments | Minutes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loureiro, A.; Partidário, M.d.R.; Santana, P. Strategic Assessment of Neighbourhood Environmental Impacts on Mental Health in the Lisbon Region (Portugal): A Strategic Focus and Assessment Framework at the Local Level. Sustainability 2022, 14, 1547. https://doi.org/10.3390/su14031547
Loureiro A, Partidário MdR, Santana P. Strategic Assessment of Neighbourhood Environmental Impacts on Mental Health in the Lisbon Region (Portugal): A Strategic Focus and Assessment Framework at the Local Level. Sustainability. 2022; 14(3):1547. https://doi.org/10.3390/su14031547
Chicago/Turabian StyleLoureiro, Adriana, Maria do Rosário Partidário, and Paula Santana. 2022. "Strategic Assessment of Neighbourhood Environmental Impacts on Mental Health in the Lisbon Region (Portugal): A Strategic Focus and Assessment Framework at the Local Level" Sustainability 14, no. 3: 1547. https://doi.org/10.3390/su14031547