
Improving Women’s Opportunities to Succeed in the Workplace: Addressing Workplace Policies in Support of Menstrual Health and Hygiene in Two Kenyan Factories



Abstract
:1. Introduction
1.1. Background
1.2. Study Aims
2. Materials and Methods
2.1. Population and Setting
- Medium- or large-sized enterprise (100+ employees) in the formal sector, with multiple places of business/operations and a fixed/permanent workplace;
- Urban or peri-urban location;
- Minimum of 50 female employees per workplace;
- Majority of the female workforce has completed no more than secondary school and is not in professional/managerial positions;
- The workplace has accessible, single-sex toilets with adequate water supply; and
- The workplace does not have existing programs addressing menstrual hygiene management or women’s economic empowerment initiatives.
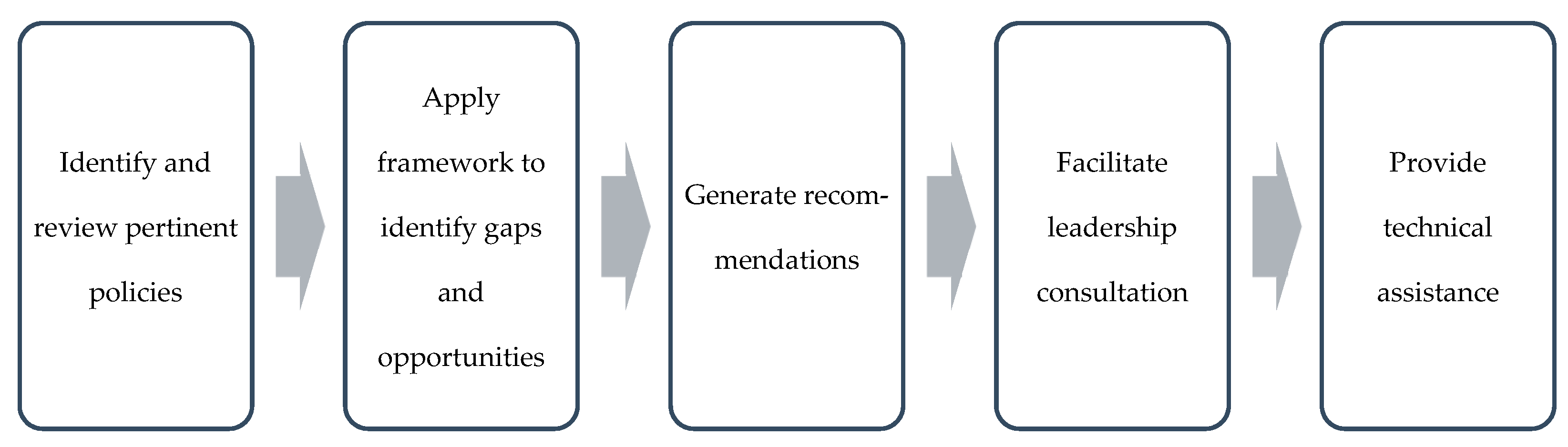
2.2. Policy Review Process
3. Results
3.1. Workplace 1
- Intentionally support menstruating women through the provision of necessary supplies.
- Provide menstrual products;
- Equip the first aid provider with painkillers at all times;
- Ensure weekly waste pick up to adhere to international hygiene protocols of menstrual waste removal; and
- Provide break time and rest areas.
- Cultivate a working environment and supervisory approach that is supported and less harsh.
- Implement the existing Supervisor’s Code of Conduct: “Exercise compassion when an employee is unwell, has personal issues, and needs time to resolve these issues”;
- Incorporate MHH-supportive language into the Supervisor’s Code of Conduct;
- Sponsor a supervisor training session about workplace support for employees who menstruate;
- Incorporate MHH-friendly content into orientation for new supervisors; and
- Alter supervisor job description to include: “Supervisors are expected to treat employees’ health-related concerns with respect”.
- Remove barriers that prevent women from accessing toilets as needed.
- Increase the number of toilets available to women (25:1 women toilet ratio);
- Tile toilet floors and walls to reduce drying time after cleaning; and
- Increase the hours available for women to access toilets.
- Ensure that new employees fully understand all workplace policies, including their rights and provisions as menstruating employees.
- Compile HR policies into a single employee handbook, including a signed acknowledgment of understanding by new hires;
- Prioritize in-person (1:1 or small group) meeting with new hires to thoroughly orient them to all employment policies; and
- Discuss MHH accommodations clearly with new hires and invite questions (destigmatize the topic).
- Refrain from penalizing employees who face routine health challenges related to menstruation.
- Allow paid time off if an employee is unwell due to menstruation;
- Consider leave without a doctor’s note (maximum of 1 day); and
- Train supervisors to recognize that many employees face menstruation-related complications, encouraging supportive supervision.
3.2. Workplace 2
- Consider the Labor Relations Act of Kenya, and provide all employees with opportunities for representation.
- Revisit the rationale behind contract versus permanent employee classification;
- Consider employees’ rights to join a trade union; and
- Consider employees’ right to participate in the election of officials/representatives or to vie for a union position.
- Consider revising the paid sick leave policy so that its application is equitable across all employee levels.
- Apply the 30-days-per-year allowance across all employees;
- Allow paid time off if an employee is unwell due to menstruation;
- Consider leave without a doctor’s note (maximum 1 day); and
- Recognize that many employees face menstruation-related complications.
- Adopt additional HR policies.
- Equal employment opportunity/non-discrimination;
- Supervisor code of conduct; and
- Anti-harassment and bullying policy, including reporting mechanism.
- Ensure that new employees fully understand all workplace policies, including their rights and provisions as menstruating employees.
- Compile HR policies into a single employee handbook, including a signed acknowledgment of understanding by new hires;
- Prioritize in-person (1:1 or small group) meeting with new hires to thoroughly orient them to all employment policies; and
- Discuss MHH accommodations clearly with new hires and invite questions (destigmatize the topic).
- Promote women in management and supervisory roles to improve supervisor support for menstruating employees and grow women’s representation in decision-making channels (also affecting MHH).
- Consider setting targets at the managerial level; and
- Build a strategy around promoting women in leadership positions.
4. Discussion
4.1. Limitations of Study
4.2. Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Policy development
- How are policies drafted? Who is present/involved in policy development?
- Who has the authority to make changes?
- Who is responsible for enforcement/implementation?
- What is the review process for company policies?
- Policy application
- Do policies on disciplinary procedures apply to employees or to those who are not in management only? [Probe for disciplinary procedures for senior employees]
- Does the policy on pregnancy apply to all categories of employees?
- Are there other policies that do not apply to all categories of employees?
- Policy dissemination
- How are policies communicated to employees?
- How are supervisors informed/trained on the supervisors’ manual and supervisors code of conduct?
- Policy implementation
- What measures are in place to actively advance women’s leadership as provided in the Gender Equality and Women’s Empowerment Policy?
- How is the piece-rate-compensation policy and overtime policy, which commit to paying workers at government’s minimum wage or higher, provides no more than 40 h a week work and to pay workers 1.5 times the regular rate for all hours worked in excess of 45 h in a workweek implemented?
- Given that senior managers are responsible for handling complaints, how are complaints against senior managers handled?
- What happens if an employee feels unfairly evaluated?
- Policy contradictions
- How is the sick leave policy implemented? [Probe for discrepancies between what exists in policy and the reality of workers having to take unpaid leave for illness]
- How can you explain the contradictions in anti-harassment policy and the reality of the work culture, i.e., harassment as a way to meet targets and lack of compassion as indicated by women during FGDs?
- Representation
- How are worker representatives selected? How are employees involved in selection of worker representatives? If they are not involved, why not? [Probe for why management appoints worker representatives]
- Promoting MHH
- Are there widespread or recognized company practices and/or guidelines that are not written in policies (less formalized)? [specific to MHH]
- What recommendations would you make to promote adequate MHH in the workplace?
References
- International Labour Office. WASH@Work: A Self-Training Handbook; ILO: Geneva, Switzerland, 2016. [Google Scholar]
- USAID. Menstrual Hygiene Management in the Workplace Action Research: Final Activity Report; USAID: Washington, DC, USA, 2022. [Google Scholar]
- Hennegan, J.; Winkler, I.T.; Bobel, C.; Keiser, D.; Hampton, J.; Larsson, G.; Chandra-Mouli, V.; Plesons, M.; Mahon, T. Menstrual Health: A Definition for Policy, Practice, and Research. Sex. Reprod. Health Matters 2021, 29, 1911618. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Chandraratna, S.; Cavill, S.; Mahon, T.; Phillips-Howard, P. Managing Menstruation in the Workplace: An Overlooked Issue in Low- and Middle-Income Countries. Int. J. Equity Health 2016, 15, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- USAID. Menstrual Hygiene Management and Women’s Economic Empowerment: A Review of Existing Evidence; USAID: Washington, DC, USA, 2019. [Google Scholar]
- Rajaraman, D.; Travasso, S.M.; Heymann, S.J. A Qualitative Study of Access to Sanitation amongst Low-Income Working Women in Bangalore, India. J. Water Sanit. Hyg. Dev. 2013, 3, 432–440. [Google Scholar] [CrossRef]
- BSR. Investing in Women for a Better World; Business for Social Responsibility (BSR): San Francisco, CA, USA, 2010. [Google Scholar]
- Speak Up Africa. Knowledge, Attitudes and Practices Pertaining to Menstrual Hygiene Management in Suburban Areas in the Dakar Region: Case Study of the Departments of Pikine and Guediawaye; Speak Up Africa: Dakar, Senegal, 2017. [Google Scholar]
- Spelman, L.; Cookson, T. The Impact of Periods: Promoting Menstrual Health Is Critical to Women’s Economic Empowerment around the World; Economic Development; Stanford Social Innovation Review (SSIR): Stanford, CA, USA, 2017; p. 3. [Google Scholar]
- USAID. Menstrual Hygiene Management in the Workplace Action Research: Kenya Inception Report; USAID: Washington, DC, USA, 2020. [Google Scholar]
- Geertz, A.; Iyer, L.; Kasen, P.; Mazzola, F.; Peterson, K. An Opportunity to Address Menstrual Health and Gender Equity; FSG: Washington, DC, USA, 2016. [Google Scholar]
- Bhattacharya, S. Menstruation at Work: Why We Must Have Period-Equipped Workplaces in the 21st Century; TheaCare, 2019. Available online: https://drive.google.com/file/d/1v8B6TEApqKv7WE_DZjp57j2u9R7frooz/view?fbclid=IwAR1gRO_-ER2VEoqZw7bPAj6MuIewWvgGGSyY6TMKINHPUq0KuZmCyz4CCrY&usp=embed_facebook (accessed on 3 August 2021).
- CARE Canada. The Tough Stuff-Managing Menstruation; CARE Canada: Ottawa, ON, Canada, 2018. [Google Scholar]
- Columbia University; IRC. A Toolkit for Integrating Menstrual Hygiene Management (MHM) into Humanitarian Response; Columbia University, IRC: New York, NY, USA, 2017. [Google Scholar]
- House, S.; Mahon, T.; Cavill, S. Menstrual Hygiene Matters: A Resource for Improving Menstrual Hygiene around the World; WaterAid: London, UK, 2012; p. 354. [Google Scholar]
- Nepal Red Cross Society. Menstrual Hygiene Friendly Workplace; Nepal Red Cross Society: Kathmandu, Nepal, 2017. [Google Scholar]
- RTI International; Hartmann, M.; Krishnan, S.; Rowe, B.; Hossain, A.; Elledge, M. Gender-Responsive Sanitation Solutions in Urban India; RTI Press: Research Triangle Park, NC, USA, 2015. [Google Scholar]
- Ministry of Health. Kenya Menstrual Hygiene Management Policy 2019–2030; Government of Kenya: Nairobi, Kenya, 2019.
- USAID. Engendering Utilities: Integrating Gender into Workplace Policies; USAID Engendering Industries: Washington, DC, USA, 2021.
- The Republic of Kenya. Labour Relations Act; The Republic of Kenya: Nairobi, Kenya, 2007.
- WaterAid; WSUP; UNICEF. Female-Friendly Public and Community Toilets: A Guide for Planners and Decision Makers; WaterAid: Melbourne, VIC, Australia, 2018. [Google Scholar]
- The Republic of Kenya. The Constitution of Kenya; The Republic of Kenya: Nairobi, Kenya, 2010.
- Hennegan, J.; Kibira, S.P.S.; Exum, N.G.; Schwab, K.J.; Makumbi, F.E.; Bukenya, J. ‘I Do What a Woman Should Do’: A Grounded Theory Study of Women’s Menstrual Experiences at Work in Mukono District, Uganda. BMJ Glob. Health 2020, 5, e003433. [Google Scholar] [CrossRef] [PubMed]
- Hennegan, J.; Bukenya, J.N.; Makumbi, F.E.; Nakamya, P.; Exum, N.; Schwab, K.J.; Kibira, S.P.S. Menstrual Health Challenges in the Workplace and Consequences for Women’s Work and Wellbeing: A Cross-Sectional Survey in Mukono, Uganda. SocArXiv 2021. [Google Scholar] [CrossRef]
- Hennegan, J.; OlaOlorun, F.M.; Oumarou, S.; Alzouma, S.; Guiella, G.; Omoluabi, E.; Schwab, K.J. School and Work Absenteeism Due to Menstruation in Three West African Countries: Findings from PMA2020 Surveys. Sex. Reprod. Health Matters 2021, 29, 1915940. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.; Yoon, J.; Kim, J.-H.; Yoo, J.; Sorensen, G.; Kim, S.-S. Working Alone, Limited Restroom Accessibility, and Poor Menstrual Health Among Cosmetics Saleswomen in South Korea. New Solut. J. Environ. Occup. Health Policy 2022, 10482911221083666. [Google Scholar] [CrossRef] [PubMed]
- Phillips-Howard, P.A. What’s the Bleeding Problem: Menstrual Health and Living with a Disability. Lancet Reg. Health West. Pac. 2022, 19, 100349. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type of Policy | Details |
|---|---|
| Leave policies (particularly sick leave) | Noting which employee classifications qualify for leave (and which do not) and whether employees qualify upon hire or after a certain length of employment |
| Occupational health and safety policy | Detailing workplace approaches to ensure the health and safety of employees |
| Employee wellness policy | Policies that document ways in which the workplace addresses wellness and well-being for employees (may overlap with Occupational Health and Safety Policy) |
| Non-discrimination or equal employment opportunity policy | Documentation of how the workplace addresses hiring practices, with specific focus on equal opportunities and non-discrimination |
| Anti-harassment policy | Documentation of the standard operating procedures for reporting and responding to harassment in the workplace, including details of a company-sponsored, accessible grievance and complaints mechanism |
| Employee classification information | Documentation about the types of employment contracts (full-time, short-term, etc.) and associated benefits or entitlements |
| Union or employee associations | Descriptions of these associations, including requirements for membership and serving as representatives, as well as terms of any existing Collective Bargaining Agreements |
| Expectations of supervisors | Documentation of a supervisor manual, training for supervisors, etc. |
| Policy with language about periodic breaks | Documentation of toilet breaks and who monitors break time, etc. |
| Performance management | Description of appraisals, including how performance is measured, how promotions are determined, etc. |
| New employee induction | Documentation for new employees outlining benefits, breaks allowed, etc., including induction or new hire training provisions by the employer |
| Number | Question |
|---|---|
| 1 | On what date was the policy instated? |
| 2 | Does the policy apply to all employee categories or only some? |
| 3 | Does the policy benefit menstruating and non-menstruating employees differently? Is this intentional? |
| 4 | Does the policy place undue burden on employees who menstruate? How? |
| 5 | What are the potential unintended consequences of this policy, as pertaining to menstruation? |
| 6 | How does the policy align with national legislation/policy? |
| 7 | Does the policy present an opportunity to promote adequate MHH in the workplace (i.e., recommendations)? How? |
| 8 | Based on the analysis of this policy, what are some preliminary recommendations that can be made to promote adequate MHH in the workplace? |
| 9 | What clarifications are needed from the HR Manager? List. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fry, W.; Njagi, J.W.; Houck, F.; Avni, M.; Krishna, A. Improving Women’s Opportunities to Succeed in the Workplace: Addressing Workplace Policies in Support of Menstrual Health and Hygiene in Two Kenyan Factories. Sustainability 2022, 14, 4521. https://doi.org/10.3390/su14084521
Fry W, Njagi JW, Houck F, Avni M, Krishna A. Improving Women’s Opportunities to Succeed in the Workplace: Addressing Workplace Policies in Support of Menstrual Health and Hygiene in Two Kenyan Factories. Sustainability. 2022; 14(8):4521. https://doi.org/10.3390/su14084521
Chicago/Turabian StyleFry, Whitney, Joan W. Njagi, Frances Houck, Michal Avni, and Aditi Krishna. 2022. "Improving Women’s Opportunities to Succeed in the Workplace: Addressing Workplace Policies in Support of Menstrual Health and Hygiene in Two Kenyan Factories" Sustainability 14, no. 8: 4521. https://doi.org/10.3390/su14084521
APA StyleFry, W., Njagi, J. W., Houck, F., Avni, M., & Krishna, A. (2022). Improving Women’s Opportunities to Succeed in the Workplace: Addressing Workplace Policies in Support of Menstrual Health and Hygiene in Two Kenyan Factories. Sustainability, 14(8), 4521. https://doi.org/10.3390/su14084521