Abstract
The key to promoting urbanization in China is to achieve urban integration of migrant peasant workers, and basic public health services may have a potential social impact on the subjective welfare of migrant peasant workers. In this paper, we use data from the China Migrants Dynamic Survey (CMDS) to study the impact of basic public health services on the urban integration of migrant peasant workers. The results show that basic public health services can significantly improve the probability of migrant peasant workers’ urban integration. The conclusions remain robust after mitigating potential endogeneity issues using the propensity score matching method (PSM), the CMP method, and robustness testing by replacing the explanatory variables with the reduced tail treatment. Further research found that the impact of basic public health services on migrant peasant workers’ urban integration is heterogeneous. The urban integration effect of basic public health services is more significant in male, high school and above, migrant peasant workers’ groups. The urban integration effect of basic public health services gradually increases with upgrading of the urban grade at the second-tier city and higher urban levels, and it also plays a vital role in the urban integration of the migrant peasant workers at the third-tier city and lower urban levels. Our findings also provide an evidence-based policy for China to promote equalizing basic public health services and a path to the urbanization of migrant peasant workers.
1. Introduction
Urbanization is an important path to modernization, and the key to promoting urbanization lies in the urban integration of hundreds of millions of migrant peasant workers in China [1,2]. One of the key reasons why China’s urbanization level lags below the world average is that migrant peasant workers have difficulties integrating into cities, and instead, migrate back and forth between urban and rural areas like “migratory birds” [3]. According to the Seventh National Population Census, there are 286 million migrant workers in China in 2020 (http://www.stats.gov.cn/tjsj/zxfb/202105/t20210510_1817176.html (accessed on 11 May 2021)), meaning there is one migrant worker for every five Chinese people. Therefore, a significant strategy for the Chinese society will be to continuously deepen reforms in several important areas, such as the social security system and the household registration system, for quite a long time [4].
Since 2009, with the deepening of China’s medical and health system reform spreading on all fronts, the national basic public health service system has been comprehensively promoted in China as an important element in new medical reform. General Secretary Xi pointed out at the 2016 National Conference on Health and Wellness that “we should unswervingly implement the prevention-oriented policy and strive to provide the people with health and wellness services throughout their life cycle”. As an important component of public services, the national basic public health service system has been tasked with bridging the health enjoyment gap between urban and rural areas and different social groups and is a necessary institutional arrangement for the Party and the government to achieve social justice in the field of health governance by restructuring social interests. The “Healthy China 2030” Plan emphasizes equalizing basic public health and family planning services for the mobile population. Since 2009, the per capita subsidy for basic public health services has gradually increased from 15 yuan to 84 yuan, and the program content has spread from 9 to 14 categories. The “14th Five-Year Plan” has taken the construction of a solid public health system and the improvement of national health promotion policies to a new level. This initiative is of great significance to enhance the accessibility of health services for migrant peasant workers in the inflow area, to enhance the competitiveness of the migrant peasant workers to integrate into cities, and ultimately, to promote high-quality development of urbanization.
Urban integration of migrant peasant workers generally refers to the process and state in which migrant peasant workers integrate into urban society and identify with their new social identity in terms of production methods, lifestyles, social psychology, and values [5,6,7,8]. Existing research on basic public health services and urban integration of migrant peasant workers in China can be divided into three main parts. First, the effectiveness of basic public health services in the field of health governance has been assessed. Since the promotion of a national basic public health service, academics have paid more attention to it. Many researchers have affirmed the positive significance of the system in the field of health governance. Moreover, relevant studies have pointed out that basic public health services have improved the health level of residents [9,10], reduced the health disparities among residents [11,12], promoted the improvement of the level of health enjoyment equalization [13,14,15], and enabled health benefits to emerge [16]. All of these advance the achievement of the WHO universal health coverage concept [17,18]. Second, the status of health service utilization among migrant peasant workers and its influencing factors have been studied. Notably, some of the literature shows that public health policies for migrant peasant workers have not been fully implemented in the inflowing areas [19]. Migrant peasant workers are more likely to suffer from health threats due to high occupational risks and poor living environments. They are prone to become a blind spot group for immunization, infectious disease prevention, and occupational health protection in inflowing areas [20]. They are also disadvantaged regarding access to conventional medical services and health insurance benefits [21]. Some scholars have further dissected the key causal factors of low utilization of public health services among migrant peasant workers in terms of health policy formulation and implementation and individual characteristic factors [22,23,24,25]. Studies on factors influencing the social integration of migrant peasant workers have mainly included household registration division [26,27], human capital characteristics [28], housing [29,30,31], and social security [32,33,34]. In terms of individual characteristics of the target population, individual characteristics such as gender, age, education level [35], household income [36], employment status [37], and mobility range [38] of migrant peasant workers also have potential impacts on their utilization of basic public health services. Third, there are studies that have discussed and assessed the urban integration of migrant peasant workers, and as compared with the previous two points, studies that have discussed and assessed the urban integration for migrant peasant workers in China are significantly lacking. Studies assessing the urban integration of migrant peasant workers have mainly been based on objective indicators such as health service utilization, labor supply, and feasible capacity [39,40,41], or single subjective welfare indicators such as economic integration, social integration, cultural integration, and psychological integration [42,43]. Fewer studies have systematically assessed the subjective welfare effects of basic public health services for migrant peasant workers.
In summary, most studies have assessed the effectiveness of basic public health services in health governance or the status of health service utilization among migrant peasant workers and its influencing factors alone. Few studies have focused on the broader spillover effects of basic public health services on the social integration of migrant peasant workers. In addition, there needs to be a comprehensive indicator to measure the urban integration of migrant peasant workers in studies that specifically address this issue. A single indicator cannot comprehensively measure the multidimensional attributes of the urban integration of migrant peasant workers. Does basic public health service promote the urban integration of migrant peasant workers? This topic should be the focus of research and could be a social lens for assessing the effectiveness of basic public health services.
In this paper, we construct a comprehensive indicator of urban integration of migrant peasant workers based on the data from the China Migrants Dynamic Survey (CMDS) in 2017. By applying the least squares estimation method (OLS), propensity score matching method (PSM), and CMP methods, we study the impact of basic public health services on the urban integration of migrant peasant workers. Furthermore, the heterogeneity of these effects by gender, education level, and urban class is further explored. This study provides a new social perspective for assessing the effectiveness of basic public health services, deepens the understanding of the social spillover effects of basic public health services, and enriches the social connotation of the strategic goals of a healthy China. This study also provides theoretical references and empirical evidence for the effective utilization of the promotional effects of public health policies for migrant peasant workers at the policy level. The remainder of this paper is structured as follows: In Section 2, we describe methods; in Section 3, we report results; in Section 4, we discuss our empirical results; and in Section 5, we state our conclusions and recommendations.
2. Methods
2.1. Data Sources
The data in this paper are mainly from the 2017 data of the China Migrants Dynamic Survey (CMDS) conducted by the National Health and Wellness Commission. The CMDS is a nationwide large-scale sampling survey of floating population that has been carried out every year since 2009, covering 31 provinces (regions, cities) and Xinjiang Production and Construction Corps in China; in terms of sampling method, the CMDS mainly adopts probability proportional to size (PPS). The sample size of each province (district, city) was divided into four levels, from high to low, namely 10,000, 6000, 4000, and 2000; the survey object of this data was the floating population aged 15–59 who had live in the inflow area for more than one month and who were not registered in the district (county, city). The survey sample, in 2017, was 170,000 households. Since the research object was a rural floating population, the data cleaning process included keeping rural household registration’s in the sample and removing the samples with incomplete key variable information; finally, we obtained 107,213 individual microdata of a rural mobile population.
2.2. Variable Descriptive Statistics
2.2.1. Dependent Variable
Regarding urban integration, there have been more discussions around the connotation and extension of urban integration, and although the various discussions seem to be divergent, a consensus can be formed about the basic categories of urban integration that have been identified. These include economic integration, social integration, cultural integration, and psychological integration [42,43]. Meanwhile, psychological integration is generally considered to be the highest level of social integration. Combining with the availability of CMDS indicators, in this paper, we select five questions as proxy variables for urban integration, which are “I like the city/place I am living in now”, “I am concerned about the city/place I am living in now change”, “I would like to integrate with the locals and become one of them”, “I think the locals would like to accept me as one of them”, “I think I am already a local”; the options for all five questions were completely disagree (1 point), disagree (2 points), largely agree (3 points), and completely agree (4 points). The principal component analysis (PCA) method was used for the explained variables. A principal component analysis system automatically extracts a factor with a characteristic root greater than 1 and tests the adaptability of factor analysis. The extracted factor variance contribution rate is 60.59%, and the KMO is 0.8282; therefore, it was considered suitable for factor analysis. Meanwhile, we referred to Dong and He (2022) [40] to standardize the extracted factors to 0–100, to facilitate comparison of the independent variable coefficients, and the transformed cities were integrated into continuous variables.
2.2.2. Independent Variable
Regarding the establishment of a health record or not, when implementing basic public health programs, the establishment of a health record is considered to be a prerequisite for the provision of basic public health services [44,45,46]. According to existing practice and research, “Have you established a health record for your local area?” is used as a proxy variable for basic public health services. In the CMDS, the question options include four items, namely “yes, it is established”, “no, it is not established, and I have never heard of it”, “no, but I have heard of it”, and “I am not sure”. “Yes, established” was assigned a value of 1 and the remaining options were assigned a value of 0. Therefore, the explained variable was a binary variable.
2.2.3. Control Variable
With reference to previous relevant studies, we also controlled for other variables that could affect the social integration of migrant peasant workers, mainly including individual characteristic variables (age, age squared, gender, nationality, education level, marriage, and insurance card), occupational characteristic variables (income, unit, and industry), immigrant characteristic variables (immigrant number, immigrant time, and immigrant region), household characteristic variables (living together, land, and indemnificatory housing), and province characteristic variables.
As mentioned earlier, the sample size for the data used in this paper was 107,213. And Table 1 shows in this sample size, 27,419 had established health records (approximately 25.57%) and 79,794 had not established health records (approximately 74.43%). The mean value of urban integration was higher and significantly different (p < 0.01) in the group with established health records as compared with the group without established health records, although this only reflects statistical differences, and the relationship between basic public health services and social integration of migrant peasant workers still needs to be discussed in empirical studies. In addition, differences existed in personal characteristic variables, occupational characteristic variables, mobility characteristic variables, and household characteristic variables.

Table 1.
Statistical description of the variables.
2.3. Model Setting
2.3.1. Baseline Model—OLS Model
Considering that the explanatory variables are continuous variables, the least squares linear model was chosen to examine the impact of basic public health services on the urban integration of migrant peasant workers, and we constructed the following empirical analysis model:
In Equation (1) above, is the urban integration of t migrant peasant workers; is the core explanatory variable; represent the control variables; refer to the intercept terms; and represent the effect coefficients of the core explanatory variables and each control variable, respectively; are the random disturbance terms.
2.3.2. Correcting for Measurable Selective Bias—Propensity Score Matching (PSM)
In general, mobile populations receive basic public health care based on their own health status considerations, thus, the potential selective bias problem arising from this study. Referring to existing practices, in this paper, we used PSM to construct a counterfactual framework for analysis. Specifically, the treatment group average treatment effect (ATT) of this study assessing basic public health services and social integration of rural mobile populations can be expressed as follows:
where is the propensity score value, and is an observable confounding variable that is largely consistent with the baseline regression model control variables. The dummy variable indicates whether the rural mobile population has a health record.
2.3.3. Endogeneity Discussion
In this paper, we used the conditional mixed process (CMP) method for the analysis. Instrumental variables need to be included in the model. Valid instrumental variables should satisfy both correlation and exogeneity, where correlation requires that the instrumental variable is related to the independent variable and exogeneity requires that the instrumental variable does not directly affect the dependent. The specific choices are presented later in the paper.
3. Results
3.1. Baseline Result
Table 2 reports the regression results based on the OLS model. In particular, Column 1 controls only for the core explanatory variables, Columns 2, 3, 4, and 5 gradually increase individual characteristic variables, occupational characteristic variables, mobility characteristic variables, and household characteristic variables, and column 6 controls for province effects.
Table 2.
Baseline regression results.
Specifically, the regression results in the Column 1 show that the establishment of health records has a significant positive impact on the urban integration of migrant peasant workers. The conclusion is significant at the level of 1%, indicating that the enjoyment of basic public health services has a positive impact on the urban integration of migrant peasant workers. The extracted factor of the dependent variable urban integration is normalized to 0~100; therefore, the coefficient 4.169 means that the establishment of health records will improve the urban integration level of migrant peasant workers by 4.169 points.
In terms of control variables, this is largely in line with theoretical expectations. Specifically: (1) As compared with women, men are more likely to have higher levels of urban integration; in terms of education, as compared with the education level of primary school and below, migrant peasant workers with education levels of university and above, high school, and junior high school have higher levels of social integration; migrant peasant workers who have established social security cards have higher levels of social integration. (2) As income rises, migrant peasant workers have higher levels of social integration. (3) The social integration of migrant peasant workers is higher the fewer cities they move to and the longer they move, and the social integration of rural migrants who move across cities and counties within cities is higher as compared with those who move across provinces. (4) The number of people living together, having land in hometown, and living in indemnificatory housing also increases the level of urban integration. In addition, the average VIF value is 4.72, which is less than 10; therefore, it can be considered that there is no multicollinearity in the selection of control variables in this paper (It is not shown due to the limited space and can be obtained from the author if necessary).
3.2. Propensity Score Matching Method
The key to the PSM approach is to compare the mean difference in social integration of the rural mobile population in the treatment and control groups based on a matched sample. However, before using this method, a balance test should be carried out to ensure that there is no significant systematic difference in the explanatory variables between the two groups [47]. The estimation results are shown in Table 3. Before matching, the pseudo R2 is 0.091 and the LR test corresponded to a p-value of 0.000, which was significant at the 1% level, with a mean and median standardized bias of 8.7% and 8.1%, respectively. After matching, the pseudo R2 decreased significantly and was not higher than 0.001, and the results of the LR test were not statistically insignificant, with the mean and median of standardized bias below 0.7%. The above results indicate that matching significantly weakens the systematic differences in the explanatory variables and basically achieves the effect similar to a randomized test, that is, the matching process is successful.
Table 3.
Results of the balance test.
In this paper, we also draw the probability distribution diagram of the tendency scores of the treatment group and the control group before and after matching to ensure the matching quality (Figure 1). The overlap interval between the two groups of samples before matching is narrow and the difference in probability distribution is very significant, while the two groups of samples after matching have a larger range of overlap interval and the difference in probability distribution is significantly weaker, which indicates that the proportion of effective samples is reduced less after matching and the matching quality is higher.
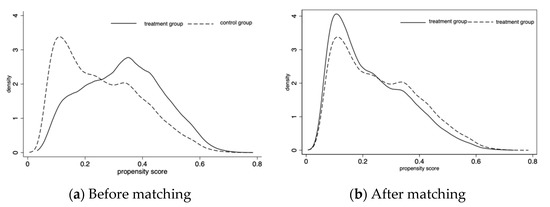
Figure 1.
Probability distribution of propensity score values for the treatment and control groups, before and after matching.
Finally, the ATT measurement results of the two groups of samples after matching are shown in Table 4. It can be seen that the measurement results of the four matching methods have some differences in the numerical level, but the differences are small, and are highly consistent in direction and significance. This also confirms, again, that basic public health services will indeed improve the social integration level of migrant peasant workers.
Table 4.
Estimation results of PSM, IPW, and IPWRA methods (ATT).
3.3. Endogenous Discussion
Considering the potential endogenous problems, the results of the basic regression model may still be biased, and therefore, it is necessary to add instrumental variables. Effective instrumental variables should meet the requirements of relevance and exogenous. Among them, relevance requires that instrumental variables are related to whether the rural floating population has established records, and exogenous requires that instrumental variables cannot directly affect the urban integration of the rural floating population. It has been pointed out that, when studying micro individuals, a tool variable can be used the interpretation at a higher level (such as county level, community level, village level, etc.) [48]. Therefore, in this study, we use the proportion of migrant peasant workers with health records established at the county level as a tool variable. Specifically, subtract the number of migrant peasant workers in the sample from the number of files in the districts and counties where they live as the numerator, subtract the total number of migrant peasant workers in the districts and counties where they live as the denominator, and divide the numerator by the denominator to obtain the instrumental variables used. The reason for meeting the relevant conditions is that the individual’s filing decision will be affected by the surrounding filing situation, and the reason for meeting the exogenous conditions is that the filing situation of other migrant peasant workers in the migrant peasant workers own district and county will not have a direct impact on their own social integration, and therefore, this instrumental variable (IV) meets the requirements of both relevance and exogenous, that is, the IV is related to the core explanatory variable, but not directly related to the explained variable.
According to Table 5, the regression results of the first stage of the CMP method show that the impact of the establishment of health records on the social integration of rural mobile population at the district and county level is statistically significant at the 1% level, which is consistent with the expectation, indicating that the instrumental variable satisfies the correlation condition. Further, the regression results of the second stage show that the establishment of health records has a statistically significant positive effect on the social integration of migrant peasant workers at the 5% level, after controlling for possible endogeneity bias, again validating the finding that the use of basic public health services contributes to the social integration of migrant peasant workers. Meanwhile, the endogeneity parameter atanhrho_12 is statistically insignificant, which indicates that there is no serious endogeneity problem in the baseline model of this paper.
Table 5.
Results of treatment effects model estimation.
3.4. Robust Tests
To further test the robustness of the analysis results, we perform robustness tests by replacing the explanatory variables with the reduced tail treatment. As shown in Table 6, the core explanatory variables in Columns 1 to 2 are replaced by the willingness to settle down and the willingness to stay in the city. The analysis results still support the significant positive effect of access to basic public health services on the urban integration of migrant peasant workers.
Table 6.
Robustness tests.
Columns 3 and 4 shrunk the tail of urban integration by 0.5% and 2.5% respectively. The regression results are also similar to the benchmark results in terms of significance and coefficient, further confirming the robustness of the regression results.
4. Discussion
As mentioned earlier, the abovementioned studies confirmed that basic public health services can significantly improve the probability of migrant peasant workers’ urban integration. Considering that the previous findings are only averaged across the whole sample, they do not consider the group heterogeneity of access to basic public health services on the social integration of migrant peasant workers. Next, we group the migrant peasant workers along three dimensions: gender, education, and region, and use the method of subsample regression and full-sample interaction terms to obtain more detailed and in-depth research conclusions.
4.1. Heterogeneity by Gender and Education Attainment
As shown in Table 7, in general, the establishment of health records has a positive impact on the urban integration of migrant peasant workers, whether grouped by gender or by education level. Specifically, in terms of gender, the subsample estimates show that the impact of health records on the urban integration of male migrant peasant workers is more obvious than that of female migrant peasant workers, with coefficients of 3.185 and 2.956, respectively. Using “health records × gender” further shows that basic public health services have a greater impact on men.
Table 7.
Heterogeneity of gender and education attainment.
The results of the subsample regression on education show that the establishment of health records has a more significant impact on the urban integration of migrant peasant workers with “high school and above”, and the estimation results using “health records × education” further confirmed that the effect of health records (i.e., basic public health services) still needs to be based on a certain amount of human capital.
This finding has been verified in some studies [35,49], which implies differences in the urban integration of basic public health services for migrant peasant workers by gender and education level. Male, higher educated migrant peasant workers, tend to be more integrated into the city. The possible reason for this is that there are differences in the ability and level of utilization of public health services by individuals [50]. Male, higher educated, migrant peasant workers are better able to understand the rules of health service utilization and have some ability to pay. Basic public health services promote the health of such migrant peasant workers, increasing their urban integration level. This finding provides a valuable reference for the territorial government to carry out a precise supply of public health service programs by groups and stages.
4.2. Urban Hierarchical Heterogeneity
It has been noted that with the rise of the scale and grade of the city, the higher “the gold content” of public services and the better the basic public health services provided, but also with increasing difficulty of urban integration. Therefore, we further investigate the heterogeneous impact of the establishment of health records at different urban levels on the urban integration of migrant peasant workers(Table 8). In general, the establishment of health records has a positive effect on the urban integration of migrant peasant workers at all urban classes; further, from this perspective, the coefficient of each urban level is similar, among which the coefficients of megacity, third-tier city and lower urban leves, and first-tier city are more than 3.000, and that of second-tier city is slightly lower, 2.896. The regression results are all significant at the level of 1%. The interactive regression results further show that the urban integration of migrant peasant workers at each urban level has a small difference.
Table 8.
Heterogeneity of urban classes.
This result differs from most previous studies [51,52,53,54]. Earlier studies have suggested that the acceptance of migrant peasant workers varies considerably across different classes of cities. More specifically, most migrant peasant workers will still be rejected by developed cities and “forced” to move to less developed second-tier and third-tier cities. However, the latter is also likely unpopular with migrant peasant workers due to a lack of resources. On the one hand, the urban integration effect of basic public health services on a rural floating population is gradually enhanced with the improvement of urban level from the perspective of the second-tier city and higher urban levels. On the other hand, basic public health services can also play a strong urban integration effect at the third-tier city and lower urban levels. Our findings constitute a significant policy implication for strengthening basic public health services in counties to promote local urbanization.
The homogeneous migrant peasant workers may face different integration problems depending on their city class which, therefore, profoundly impacts the citizenship paths of different classes of cities; however, the policy of basic public health services contributes to the quality of people-oriented urbanization under the development pressure of cities and the comprehensive attractiveness of small and medium-sized cities for migrant peasant workers to settle in. Basic public health services have a good spillover effect on promoting high-level and quality urbanization in China.
5. Conclusions and Policy Recommendations
5.1. Conclusions
In this paper, we construct a comprehensive indicator of urban integration of migrant peasant workers based on the data from the China Migrants Dynamic Survey (CMDS) in 2017. By applying the least squares estimation method (OLS), propensity score matching method (PSM), and CMP methods, we study the impact of basic public health services on the urban integration of migrant peasant workers. Furthermore, the heterogeneity of these effects by gender, education level, and urban class are further explored. The study finds that: (1) Basic public health services can significantly increase the probability of migrant peasant workers, and the findings still hold after adding the main control variables, and province dummy variables. (2) Exploring for gender and education heterogeneity finds that basic public health services exert stronger effects on urban integration effects for migrant peasant workers of men with high school and above education. (3) The urban integration effect of basic public health services increases with urban class at the second-tier city and higher urban levels, and also has a stronger effect on the urban integration of migrant peasant workers at the third-tier city and lower urban levels.
5.2. Suggestions
5.2.1. Leveraging the Systemic Spillover Effects of the National Basic Public Health Service
The contribution of the national basic public health service to the social integration of the migrant peasant workers reveals the strong institutional spillover effects of the system. In the long run, it has significantly contributed to the improvement of social governance and the quality of social construction, greatly extending the connotations and extensions of the system for assessing its effectiveness. Therefore, it is necessary to continue to deepen and optimize the national basic public health service provision system. The protection of basic public health services for migrant peasant workers should be strengthened and the system should be deeply linked with basic livelihood projects such as the housing and education security, to form a linkage and integration with basic livelihood projects and to respond to the livelihood concerns and demands of the migrant population.
5.2.2. Enhancing Equity and Accessibility of Basic Public Health Services for Migrant Peasant Workers
On 12 July 2022, China’s National Development and Reform Commission issued the Implementation Plan for the New Type of Urbanization for the 14th Five-Year Plan. It addresses that it will continue to promote the urbanization of the migrant peasant workers and it emphasizes the continuous improvement of institutional mechanisms and policy systems. Among them, improving the mechanism for providing basic public services in urban areas, steadily increasing the number and level of basic public services available to the non-resident population in the inflow areas, and promoting full coverage of basic public services for the resident population in urban areas highlight the important role of basic public health services in realizing the citizenship of the migrant peasant workers. The data in this paper show that the rate of health record construction among the rural migrant population is about one quarter, and that the coverage of basic public health services for the migrant peasant workers should be continuously expanded in order to continue to bring its effects into play.
5.2.3. Promote Basic Public Health Services to Migrant Peasant Workers by Combining Differences in Characteristics and Taking Multiple Measures
The incentive effects of basic public health services on a rural floating population with different characteristics varies, and the benefit of basic public health services to a rural floating population should be promoted in light of the individual characteristics and urban level of the rural floating population, for example, to enhance the benefit of basic public health services for groups with higher education levels and positive externalities of urban integration at the third-tier city and lower urban levels, and to promote basic public health. For example, basic public health services have been strengthened for the more educated groups and the positive externalities of urban integration at the third-tier city and lower urban levels, and basic public health services have been promoted to facilitate local urbanization. At the same time, community and community strengths are being strengthened. On the one hand, primary health care workers are regarded as the gatekeepers of residents’ health, and gatekeeping means not only providing a certain level of medical and health services, but more importantly, beyond medical and health services, community doctors and residents should jointly build a life world around health governance, in which they interact to form a joint construction of a good state of health. Because of the mobile nature of the mobile population, it is all the more necessary to strengthen the community-based construction of this system, to strengthen the social connection between community doctors and the mobile population, and to develop adequate information exchange through effective communication, and therefore, improve the level of health promotion for the mobile population and help them achieve higher quality social integration. On the other hand, it is necessary to improve the quality of health education, promote health literacy promotion campaigns on all fronts, and take various measures to attract the participation of both the resident population and the mobile population (especially the rural mobile population), and therefore, foster the power of the community in health governance through social cooperation.
With industrialization and urbanization in China, migrant peasant workers gradually become the main part of new urban citizens. The new urbanization strategy with the migrant peasant workers as the core will be the inevitable path of China’s economic and social development. However, the migrant peasant workers are vulnerable in China’s urbanization process, facing the dilemma of semi-urbanization of “economic acceptance and social exclusion”. The research has substantial policy implications. First, basic public health services help to increase the probability of urban integration of migrant peasant workers. Second, there are differences in the urban integration level of migrant peasant workers by gender and education level. Finally, basic public health services weaken social exclusion, contributing to the quality of people-oriented urbanization under the development pressure of large cities and the comprehensive attractiveness of small- and medium-sized cities for migrant peasant workers to settle in. Basic public health services have improved the spillover effect on the orderly promotion of high-quality urbanization in China.
Author Contributions
Conceptualization, formal analysis, visualization, writing—review and editing, Y.Y.; project administration, supervision, writing—review and editing, D.G.; methodology, formal analysis, writing—original draft, R.L.; methodology, formal analysis, writing—review and editing, H.D. All authors have read and agreed to the published version of the manuscript.
Funding
The Student Scientific Research Training Program of the School of Agricultural Economics and Rural Development of Renmin University of China (No. 22A10) and the 2022 Ali Fresh Water Project of AliResearch (Research on the Coupling Development of China’s Digital Economy and Rural Revitalization, No. 3).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data included in the paper are open access data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Li, Y.N. Migrant workers, the new demographic dividend and the human capital revolution. Reform 2018, 6, 5–12. (In Chinese) [Google Scholar]
- Zheng, S.; Song, Z.; Sun, W. Do Affordable Housing Programs Facilitate Migrants’ Social Integration in Chinese Cities? Cities 2020, 96, 102449. [Google Scholar] [CrossRef]
- Q, L.; C, F.L.; Lu, H.Y.; Qian, W.R. A study on the influence of urban people’s "identity" on the transfer of rural residential land use rights—A survey based on farm households in Wenzhou, Zhejiang. Agric. Technol. Econ. 2019, 8, 40–52. (In Chinese) [Google Scholar]
- Zhu, Y.L. Land dependency effect and semi-urbanization facts: A revision and empirical test of the Todaro model. Ind. Econ. Rev. 2018, 9, 140–153. (In Chinese) [Google Scholar]
- Li, H. On Construction of Rural Migrant Workers’ Social Integration Indicator System—An Empirical Analysis on Surveyed Data in 2016 Based on Structural Equation Modeling. Des. Eng. 2021, 76–90. [Google Scholar]
- Yang, J. A Study on Social Integration and Happiness Index of Migrant Workers in the Construction of Harmonious Society. J. Fujian Prov. Social. Coll. 2008, 4, 107–109. (In Chinese) [Google Scholar]
- Lv, K. Discusses the main obstacles to the citizenship of “migrant workers”. J. Party Sch. CPC Chengdu Munic. Comm. (Philos. Soc. Sci.) 2004, 2, 45–47. (In Chinese) [Google Scholar]
- Durkheim, E. The Division of Labor in Society; Free Press: New York, NY, USA, 1933. [Google Scholar]
- Wang, Z.H.; Yang, J.X.; Chen, X.; Li, X.N.; Xie, P.P.; Liu, W.Q.; Liu, J.Q. Evaluation on Implementation Effect of National Basic Public Health Service Project. China Health Econ. 2018, 10, 63–66. (In Chinese) [Google Scholar]
- Li, Y.; Dou, D. The influence of medical insurance on the use of basic public health services for the floating population: The mediating effect of social integration. Int. J. Equity Health 2022, 1, 1–7. [Google Scholar] [CrossRef]
- Zhang, Z.J.; Miao, Y.Q. Analysis on the Contribution of Primary Public Health Service on Public Health Disparity. China J. Popul. Sci. 2020, 1, 78–89+127–128. (In Chinese) [Google Scholar]
- Luo, J. Non-equalization and Administrative Obstacles of the Basic Public Services of Urban and Rurual: A System Analytical Frame. Urban Stud. 2010, 2, 151–153. (In Chinese) [Google Scholar]
- Harold, A.; Victor, L. Household Responses to Public Health Services: Cost and Quality Tradeoffs. World Bank Res. Obs. 1996, 1, 3–22. [Google Scholar]
- Wang, W.; Ren, R. The Connotation and Implementing Strategies of Equalization of Basic Public Health Services. Med. Philos. (Humanist. Soc. Med. Ed.) 2010, 6, 58–60. (In Chinese) [Google Scholar]
- Pan, Y.T.; Lian, Z.W.; Liao, Z.R.; Zhao, P.Y.; You, L.L.; Liu, Y.L. Implementation effects of National Basic Public Health Service Project: A review. China J. Public Health 2020, 3, 441–445. (In Chinese) [Google Scholar]
- Liu, Z.Y.; Xiao, Y.; Zhao, K.; Liu, A.Z. Implementation progress and effect of National Essential Public Health. China J. Public Health 2019, 6, 657–664. (In Chinese) [Google Scholar]
- Wei, W.; Wang, X.H.; Luo, Y.F. Evaluation of the Implementation Effect of National Basic Public Health Service Project. China Prim. Health Care 2013, 10, 1–2+5. (In Chinese) [Google Scholar]
- You, L.L.; Zhao, J.H.; Chen, X.Y.; Yang, L.H.; Liu, M.C.; Pan, Y.T.; Zhang, S.Q.; Liu, Y.L. Progress and Achievements of the Implementation of National Essential Public Health Services Programs over the Past Decade. China Gen. Pract. 2022, 26, 3209–3220. (In Chinese) [Google Scholar]
- Wang, J.; Zheng, J.; Wang, P.; Qi, L. Migration and health in China: Addressing the gap between policy goals and reality in health services for the migrant population. Public Adm. Rev. 2014, 7, 29–45+182–183. (In Chinese) [Google Scholar]
- Gransow, B. Body as Armor: Health Risks and Health Consciousness among Rural Migrants in Urban China. Hefte 2010, 38, 9–27. [Google Scholar]
- Keung Wong, D.F.; Li, C.Y.; Song, H.X. Rural Migrant Workers in Urban China: Living a Marginalised Life. Int. J. Soc. Welf. 2007, 16, 32–40. [Google Scholar] [CrossRef]
- Chen, Q.L.; Ge, R. The impact of individual characteristics on public service utilization—A review of studies based on public health services. Labor Econ. Res. 2018, 6, 116–127. (In Chinese) [Google Scholar]
- Derose, K.P.; Escarce, J.J.; Lurie, N. Immigrants and Health Care: Sources of Vulnerability. Health Aff. 2007, 26, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, R. Reconstructing Citizenship in a Global Economy: How Restricting Immigrants from Welfare Undermines Social Rights for U.S. Citizens. J. Soc. Soc. Soc. Welf. 2010, 37, 63. [Google Scholar]
- Drinkwater, S.; Robinson, C. Welfare Participation by Immigrants in the UK. Int. J. Manpow. 2013, 34, 100–102. [Google Scholar] [CrossRef]
- Ren, Y.; Wu, M.L. Social Integration of Floating Population in Urban China:A Literature Review. Popul. Res. 2006, 3, 87–94. (In Chinese) [Google Scholar]
- Sun, Y.; Jia, Z. The social integration among the floating population of china in 2012. China J. Drug Depend. 2016, 5, 440–448. (In Chinese) [Google Scholar]
- Wang, X.F.; Zhang, X.F. Research of the Influence of Migrant Scope and Employment Identity and Household Registration on Migrant Integration into Urban Society in Northeast China. Popul. J. 2019, 2, 43–53. (In Chinese) [Google Scholar]
- Dorvil, H.; Morin, P.; Beaulieu, A.; Robert, D. Housing as a social integration factor for people classified as mentally ill. Hous. Stud. 2005, 3, 497–519. [Google Scholar] [CrossRef]
- Lemanski, C. The impact of residential desegregation on social integration: Evidence from a South African neighbourhood. Geoforum 2006, 3, 417–435. [Google Scholar] [CrossRef]
- Wang, Z.C.; Guo, M.R.; Deng, J.N. Can Indemnificatory Housing Promote the Integration of Floating Population? Reform Econ. Syst. 2020, 1, 176–181. (In Chinese) [Google Scholar]
- Katrougalos, G.S. The privatisation of social insurance and its effect on social integration. Eur. J. Soc. Sec. 2007, 1, 79–95. [Google Scholar] [CrossRef]
- Shi, Z.L.; Shi, N. The Analysis of the Social Security of Migrant Workers and Their Integration into Urban Society. Popul. Dev. 2014, 2, 33–43. (In Chinese) [Google Scholar]
- Lu, C.; Wang, J.X.; Fan, H.L. Health insurance and social integration of migrant population: Evidence from commercial insurance. Insur. Stud. 2018, 2, 42–52. (In Chinese) [Google Scholar]
- Smith, J.P. Assimilation across the Latino Generations. Am. Econ. Rev. 2003, 93, 315–319. [Google Scholar] [CrossRef]
- Algan, Y.; Dustmann, C.; Glitz, A.; Manning, A. The Economic Situation of First and Second-Generation Immigrants in France, Germany and the United Kingdom; Oxford University Press: Oxford, UK, 2010; ISBN 0013-0133. [Google Scholar]
- Guo, J.; Shao, F.; Fan, H.; Xue, L.P.; Wu, Y.Q. Analysis of basic public health service accessibility and influencing factors of mobile population. China Health Policy Res. 2016, 9, 75–82. (In Chinese) [Google Scholar]
- Hamermesh, D.S.; Trejo, S.J. How Do Immigrants Spend Their Time? The Process of Assimilation. J. Popul. Econ. 2013, 26, 507. [Google Scholar] [CrossRef]
- Meng, Y.Y.; Han, J.Q. The impact of medical insurance system on health service utilization of mobile population. China Popul. Sci. 2019, 110–120+128. (In Chinese) [Google Scholar]
- Deng, R. Health equity accessibility and urban labor supply of migrant workers—Evidence from dynamic monitoring of the mobile population. China Rural. Econ. 2019, 4, 92–110. (In Chinese) [Google Scholar]
- Zhu, Z.K.; Zheng, Y.X.; Leng, C.X.; Tao, J.P. Urban public health services and the viability of migrant workers—Empirical evidence from a dynamic monitoring survey of China’s mobile population. Econ. Rev. 2020, 3, 54–68. (In Chinese) [Google Scholar]
- Yang, J.H. Research on the Assimilation of the Floating Population in China. Soc. Sci. China 2015, 2, 61–79+203–204. (In Chinese) [Google Scholar]
- Dong, Y.X.; He, X.B. Employment Mode and Urban Integration of Floating Youth: An Empirical Analysis Based on the Differentiation Effect of Food and Housing. China Youth Study 2022, 7, 48–55. (In Chinese) [Google Scholar]
- Ren, J.; Jiang, Q.C.; Shi, X. The Impact of Accessing to Urban Basic Health Services on the Willingness of Agricultural Migrants to Stay in Cities. Popul. Dev. 2020, 4, 14–25. (In Chinese) [Google Scholar]
- Yuan, H.B.; Deng, H.L. The impact of basic public health services on the health of floating population—Empirical analysis based on CMDS2018 data. Soc. Sci. 2021, 8, 104–107+112. (In Chinese) [Google Scholar]
- Zhou, Z.; Jiang, Y.; Wu, H.; Jiang, F.; Yu, Z. The Age of Mobility: Can Equalization of Public Health Services Alleviate the Poverty of Migrant Workers? Int. J. Environ. Res. Public Health 2022, 19, 13342. [Google Scholar] [CrossRef]
- Sianesi, B. Making Advanced Statistical Software Freely Available to Practitioners. Nucl. Instrum. Methods Phys. Res. 2004, 10, 693–698. [Google Scholar]
- Zhu, Z.K. A study of the "crowding out" effect of excessive labor on migrant workers’ social participation: Empirical evidence from a survey on the dynamics of China’s migrant population. China Rural. Obs. 2020, 5, 108–130. [Google Scholar]
- Deng, R. How does the accessibility of health services affect the subjective quality of life of migrant workers?—Evidence based on a thematic survey on health focus areas of migrant populations. China Rural Surv. 2022, 2, 165–184. (In Chinese) [Google Scholar]
- Qin, L.J.; Chen, B. Analysis of the impact of medical insurance on urban integration of migrant workers. Manag. World 2014, 91–99. (In Chinese) [Google Scholar]
- Wang, C.G. A study on the "semi-urbanization" of the rural migrant population. Sociol. Res. 2006, 5, 107–122+244. (In Chinese) [Google Scholar]
- Wang, C.G. The relationship between social identity and urban-rural integration among the new generation of rural migrants. Sociol. Res. 2001, 3, 63–76. (In Chinese) [Google Scholar]
- Tan, J. Research on migrant population in the context of new urbanization: Scope changes, practice review and evolutionary directions. South. Econ. 2021, 8, 102–111. (In Chinese) [Google Scholar]
- Li, P.L.; T, F. An intergenerational comparison of social integration of migrant workers in China. Society 2012, 32, 1–24. (In Chinese) [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).