Field Testing of the Use of Intake24—An Online 24-Hour Dietary Recall System

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
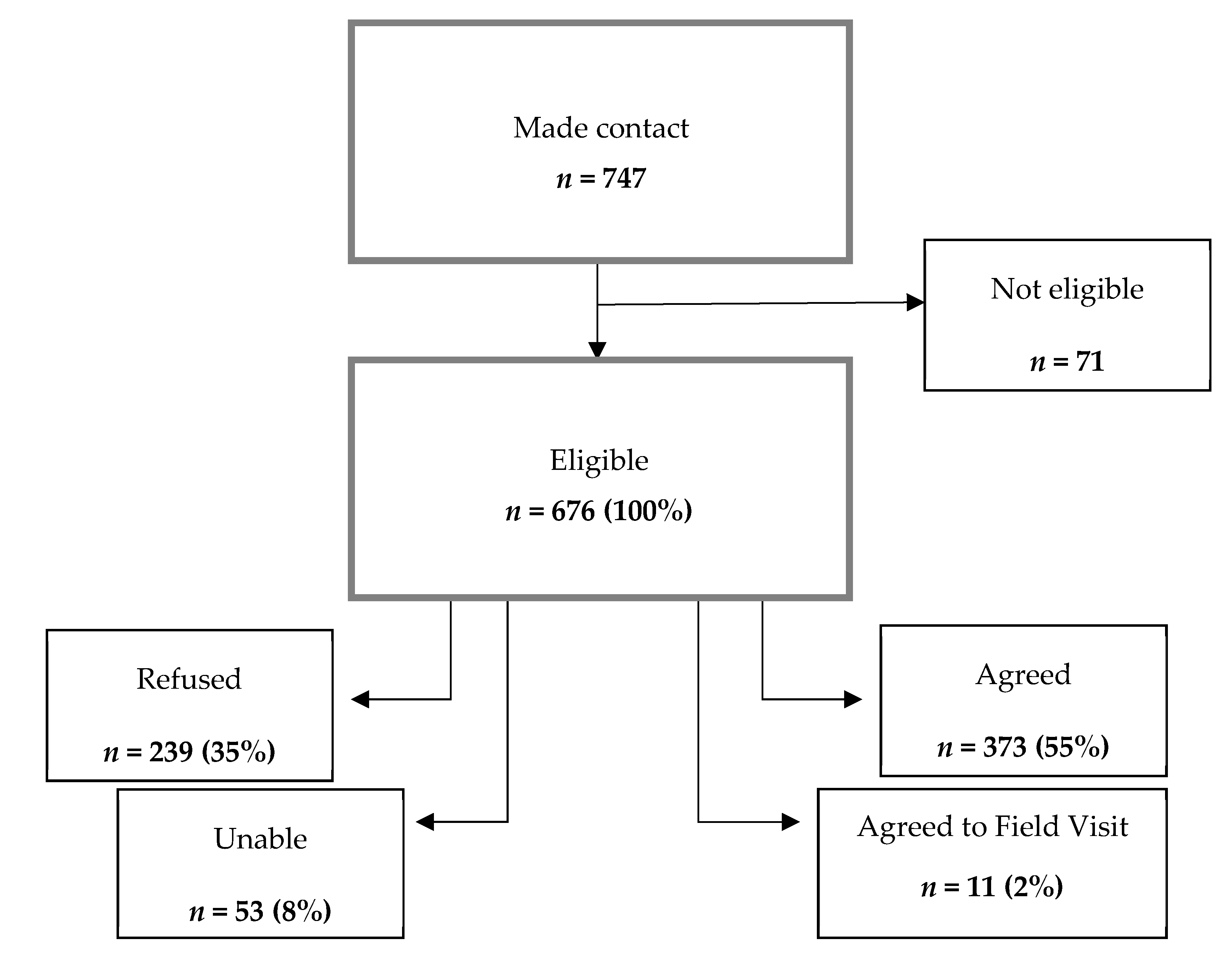
3.1. Participant Response
3.2. Demographics of Those Who Completed a Recall
3.3. Number of Recalls Completed
3.4. Technology Use
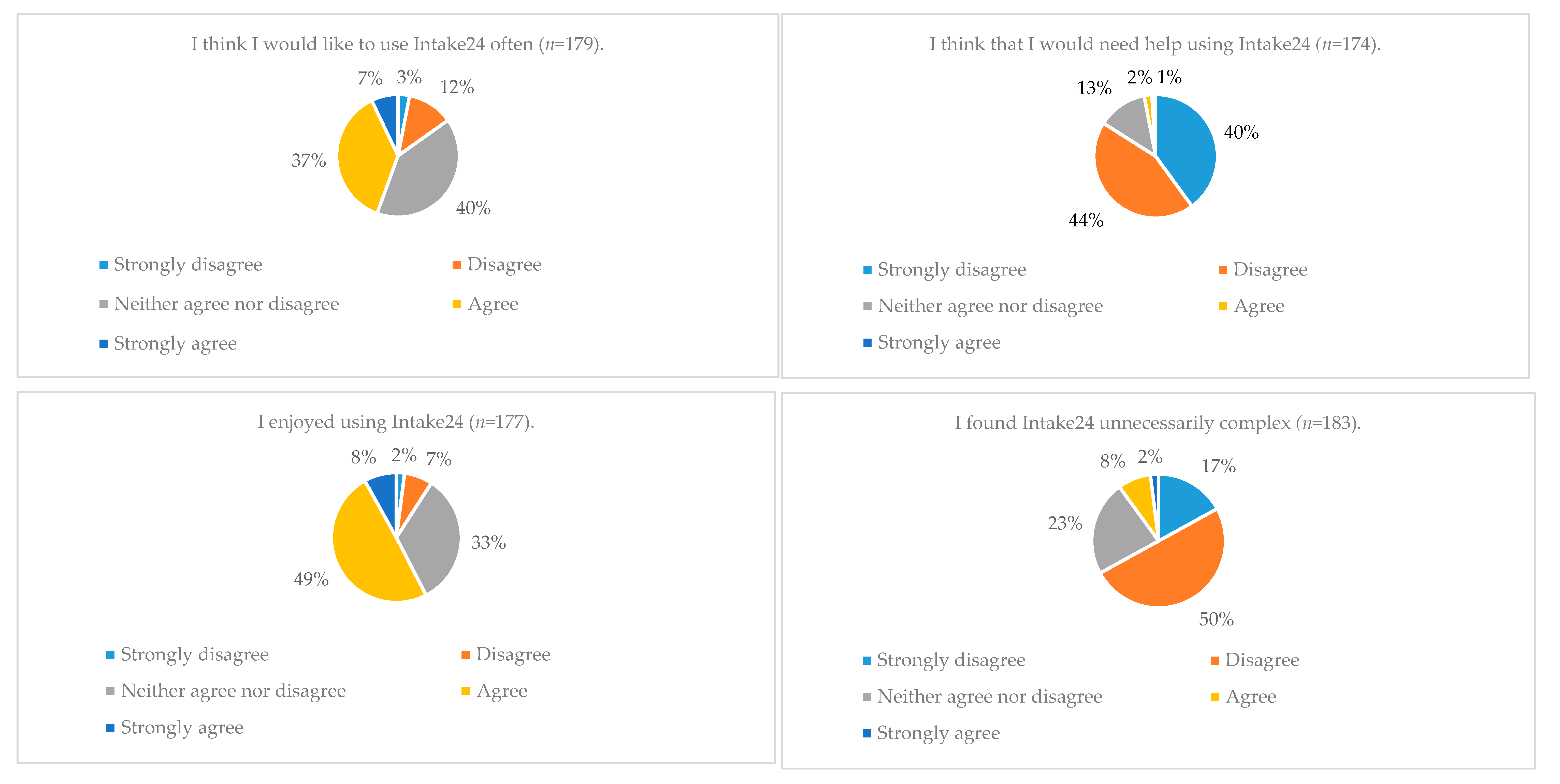
3.5. All Participant Feedback on Intake24
3.6. Feedback from Those Completing Fewer than four Recalls
3.7. Timings of Recalls
3.8. Help Requests
4. Discussion
4.1. Response and Reminders
4.2. Usability and Developments
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Obesity Observatory, Review of Dietary Assessment Methods in Public Health. 2010. Available online: http://webarchive.nationalarchives.gov.uk/20170110165944/https://www.noo.org.uk/NOO_pub/briefing_papers (accessed on 24 September 2018).
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s Dietary Intake Data System. J. Food Compos. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- Liu, B.; Young, H.; Crowe, F.L.; Benson, V.S.; Spencer, E.A.; Key, T.J.; Appleby, P.N.; Beral, V. Development and evaluation of the Oxford WebQ, a low-cost, web-based method for assessment of previous 24 h dietary intakes in large-scale prospective studies. Public Health Nutr. 2011, 14, 1998–2005. [Google Scholar] [CrossRef] [Green Version]
- Carroll, R.J.; Midthune, D.; Subar, A.F.; Shumakovich, M.; Freedman, L.S.; Thompson, F.E.; Kipnis, V. Taking advantage of the strengths of 2 different dietary assessment instruments to improve intake estimates for nutritional epidemiology. Am. J. Epidemiol. 2012, 175, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Albar, S.A.; Morris, M.A.; Mulla, U.Z.; Hancock, N.; Evans, C.E.; Alwan, N.A.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S. Development of a UK Online 24-h Dietary Assessment Tool: Myfood24. Nutrients 2015, 7, 4016–4032. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; Mcnutt, S.; et al. The Automated Self-Administered 24-h Dietary Recall (ASA24): A Resource for Researchers, Clinicians, and Educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Covents, M.; Sichert-Hellert, W.; Alvira, J.M.F.; Le Donne, C.; De Henauw, S.; De Vriendt, T.; Phillipp, M.K.; Béghin, L.; Manios, Y.; et al. Development and evaluation of a self-administered computerized 24-h dietary recall method for adolescents in europe. Int. J. Obes. 2008, 32, S26–S34. [Google Scholar] [CrossRef] [PubMed]
- Smithers, G.; Gregory, J.R.; Bates, C.J.; Prentice, A.; Jackson, L.V.; Wenlock, R. The National Diet and Nutrition Survey: Young people aged 4–18 years. Nutr. Bull. 2000, 25, 105–111. [Google Scholar] [CrossRef]
- Foster, E.; O’Keeffe, M.; Matthews, J.N.; Mathers, J.C.; Nelson, M.; Barton, K.L.; Wrieden, W.L.; Adamson, A.J. Children’s estimates of food portion size: The effect of timing of dietary interview on the accuracy of children’s portion size estimates. Br. J. Nutr. 2008, 99, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.; Hawkins, A.; Stamp, E.; Adamson, A.J. Development and validation of an interactive portion size assessment system (IPSAS). Proc. Nutr. Soc. 2010, 69, E430. [Google Scholar] [CrossRef]
- Simpson, E.; Bradley, J.; Poliakov, I.; Jackson, D.; Olivier, P.; Adamson, A.J. Iterative Development of an Online Dietary Recall Tool: INTAKE24. Nutrients 2017, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.; Simpson, E.; Poliakov, I.; Matthews, J.N.; Olivier, P.; Adamson, A.J.; Foster, E. Comparison of INTAKE24 (an Online 24-h Dietary Recall Tool) with Interviewer-Led 24-h Recall in 11–24 Year-Old. Nutrients 2016, 8, 358. [Google Scholar] [CrossRef] [PubMed]
- The Scottish Government. Scottish Index of Multiple Deprivation 2013. Available online: http://www.scotland.gov.uk/Topics/Statistics/SIMD (accessed on 26 September 2018).
- Office for National Statistics. Statistical Bulletin: Internet Access—Households and Individuals. 2014. Available online: http://www.ons.gov.uk/ons/dcp171778_373584.pdf (accessed on 26 September 2018).
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Page, P.; Nicholson, S. National Diet and Nutrition Survey Rolling Programme (NDNS RP) Results from Years 1–4 (combined) for Scotland (2008/09-2011/12). Available online: https://www.foodstandards.gov.scot/downloads/NDNS_Y1-4_Scotland_report_FULL_TEXT_MASTER_DOC_FINAL_FOR_REPUBLICATION__JUNE_2017.pdf (accessed on 26 September 2018).
- Hollis, J.L.; Craig, L.C.A.; Whybrow, S.; Clark, H.; Kyle, J.A.M.; McNeill, G. Assessing the relative validity of the Scottish Collaborative Group FFQ for measuring dietary intake in adults. Public Health Nutr. 2017, 20, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.I.; Ekholm, O.; Kristensen, P.L.; Larsen, F.B.; Vinding, A.L.; Glumer, C.; Juel, K. The effect of multiple reminders on response patterns in a Danish health survey. Eur. J. Public Health 2015, 25, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Tolonen, H.; Aistrich, A.; Borodulin, K. Increasing health examination survey participation rates by SMS reminders and flexible examination times. Scand J. Public Health 2014, 42, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Breen, C.L.; Shakeshaft, A.P.; Doran, C.M.; Sanson-Fisher, R.W.; Mattick, R.P. Cost-effectiveness of follow-up contact for a postal survey: A randomised controlled trial. Aust. N. Z. J. Public Health 2010, 34, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS-A Quick and Dirty Usability Scale. Available online: https://www.usability.gov/how-to-and-tools/methods/system-usability-scale.html (accessed on 25 October 2018).



{kind=link}
{kind=link}
| Reasons | Answers Obtained (n = 99) | |
|---|---|---|
| n = | % | |
| No internet access | 41 | 41 |
| No devices linked to internet | 28 | 28 |
| Not comfortable/competent using computers/tablets/smart phones | 24 | 24 |
| Going away or in hospital during fieldwork | 3 | 3 |
| Age | 3 | 3 |
| Demographic | Eligible (n = 676) 1 | Agreed (n = 384) 1 | |||
|---|---|---|---|---|---|
| n = | % | n = | % | ||
| Gender | Male | 343 | 51 | 203 | 53 |
| Female | 333 | 49 | 181 | 47 | |
| Age Group | 11–16 years | 151 | 22 | 123 | 32 |
| 17–24 years | 121 | 18 | 81 | 21 | |
| 25–64 years | 183 | 27 | 120 | 31 | |
| 65+ years | 221 | 33 | 60 | 16 | |
| Body mass index (BMI) classification | Under weight | 7 | 1 | 6 | 2 |
| Healthy weight | 255 | 38 | 165 | 47 | |
| Over weight | 195 | 29 | 110 | 31 | |
| Obese | 126 | 19 | 59 | 17 | |
| Morbidly obese | 24 | 4 | 14 | 4 | |
| Scottish Index of Multiple Deprivation (SIMD) Quintiles | 1 (Most deprived) | 174 | 26 | 86 | 22 |
| 2 | 111 | 16 | 64 | 17 | |
| 3 | 136 | 20 | 81 | 21 | |
| 4 | 126 | 19 | 76 | 20 | |
| 5 (Least deprived) | 129 | 19 | 77 | 20 | |
| Number of Recalls | Eligible (n = 676) | Agreed (n = 384) | ||
|---|---|---|---|---|
| n = | % | n = | % | |
| 0 | 446 | 66.0 | 154 | 40.1 |
| 4+ | 132 | 19.5 | 132 | 34.4 |
| Any | 230 | 34.0 | 230 | 59.9 |
| Number of Recalls | Male (n = 203) | Female (n = 181) | |||||
|---|---|---|---|---|---|---|---|
| n = | % | CI | n = | % | CI | p Value | |
| 0 | 83 | 40.9 | 34.3–47.8 | 71 | 39.2 | 32.4–46.6 | 0.741 |
| 4+ | 70 | 34.5 | 28.2–41.3 | 62 | 34.3 | 27.7–41.5 | 0.963 |
| Any | 120 | 59.1 | 52.2–65.7 | 110 | 60.8 | 53.4–67.6 | 0.741 |
| Number of Recalls | Age Group (Years) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 11–16 (n = 123) | 17–24 (n = 81) | 25–64 (n = 120) | 65+ (n = 60) | p Value | |||||||||
| n = | % | CI | n = | % | CI | n = | % | CI | n = | % | CI | ||
| 0 | 54 | 43.9 | 35.4–52.8 | 26 | 32.1 | 22.8–43.0 | 46 | 38.3 | 30.0–47.4 | 28 | 46.7 | 34.5–59.3 | 0.256 |
| 4+ | 40 | 32.5 | 24.8–41.3 | 32 | 39.5 | 29.5–50.5 | 41 | 34.2 | 26.2–43.1 | 19 | 31.7 | 21.2–44.5 | 0.726 |
| Any | 69 | 56.1 | 47.2–64.6 | 55 | 67.9 | 57.0–77.2 | 74 | 61.7 | 52.6–70.0 | 32 | 53.3 | 40.7–65.5 | 0.256 |
| Number of Recalls | SIMD Quintile | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (Most Deprived) (n = 86) | 2 (n = 64) | 3 (n = 81) | 4 (n = 76) | 5 (Least Deprived) (n = 77) | p Value | |||||||||||
| n = | % | CI | n = | % | CI | n = | % | CI | n = | % | CI | n = | % | CI | ||
| 0 | 44 | 51.2 | 40.7–61.6 | 30 | 46.9 | 35.0–59.1 | 32 | 39.5 | 29.5–50.5 | 28 | 36.8 | 26.8–48.2 | 20 | 26.0 | 17.4–36.9 | 0.019 * |
| 4+ | 22 | 25.6 | 17.4–35.9 | 22 | 34.4 | 23.8–46.8 | 30 | 37.0 | 27.2–48.1 | 26 | 34.2 | 27.2–48.1 | 32 | 41.6 | 31.1–52.9 | 0.305 |
| Any | 42 | 48.8 | 38.4–59.3 | 34 | 53.1 | 40.9–65.0 | 49 | 60.5 | 49.5–70.5 | 48 | 63.2 | 51.8–73.2 | 57 | 74.0 | 63.1–82.6 | 0.19 * |
| Number of Recalls | BMI Classification | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Under-Weight (n = 6) | Healthy Weight (n = 165) | Over-Weight (n = 110) | Obese (n = 59) | Morbidly Obese (n = 14) | p Value | |||||||||||
| n = | % | CI | n = | % | CI | n = | % | CI | n = | % | CI | n = | % | CI | ||
| 0 | 3 | 50.0 | 16.7–83.3 | 59 | 35.8 | 28.8–43.4 | 48 | 43.6 | 34.7–53.1 | 27 | 45.8 | 33.5–58.5 | 5 | 35.7 | 15.6–62.5 | 0.564 |
| 4+ | 3 | 50.0 | 16.7–83.3 | 65 | 39.4 | 32.2–47.1 | 35 | 31.8 | 23.8–41.1 | 16 | 27.1 | 17.3–39.8 | 4 | 28.6 | 11.1–56.2 | 0.374 |
| Any | 3 | 50.0 | 16.7–83.3 | 106 | 64.2 | 56.6–71.2 | 62 | 56.4 | 46.9–65.3 | 32 | 54.2 | 41.5–66.5 | 9 | 64.3 | 37.5–84.4 | 0.564 |
| Sentiment | n = 72 | % |
|---|---|---|
| Negative | 11 | 15 |
| Neutral | 24 | 33 |
| Positive | 29 | 40 |
| Mixed | 8 | 11 |
| Reason Given | Number of Responses (n = 57) | % 1 |
|---|---|---|
| Thought I had fully completed the survey | 16 | 28 |
| Don’t remember seeing any more emails | 10 | 18 |
| Opened the email too late to complete for allocated day | 10 | 18 |
| Did not receive any more emails | 7 | 12 |
| Away/Holiday/No (or problems with) Internet access 1 | 5 | 9 |
| Didn’t enjoy doing it | 3 | 5 |
| Unable to access the website | 2 | 4 |
| It took too long | 1 | 2 |
| Lost interest | 1 | 2 |
| Could access the website but was unable to log on | 1 | 2 |
| Had enough after completing 1, 2 or 3 recalls | 1 | 2 |
| Changed mind about taking part | 0 | 0 |
| Didn’t like that it was online | 0 | 0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowland, M.K.; Adamson, A.J.; Poliakov, I.; Bradley, J.; Simpson, E.; Olivier, P.; Foster, E. Field Testing of the Use of Intake24—An Online 24-Hour Dietary Recall System. Nutrients 2018, 10, 1690. https://doi.org/10.3390/nu10111690
Rowland MK, Adamson AJ, Poliakov I, Bradley J, Simpson E, Olivier P, Foster E. Field Testing of the Use of Intake24—An Online 24-Hour Dietary Recall System. Nutrients. 2018; 10(11):1690. https://doi.org/10.3390/nu10111690
Chicago/Turabian StyleRowland, Maisie K., Ashley J. Adamson, Ivan Poliakov, Jennifer Bradley, Emma Simpson, Patrick Olivier, and Emma Foster. 2018. "Field Testing of the Use of Intake24—An Online 24-Hour Dietary Recall System" Nutrients 10, no. 11: 1690. https://doi.org/10.3390/nu10111690
APA StyleRowland, M. K., Adamson, A. J., Poliakov, I., Bradley, J., Simpson, E., Olivier, P., & Foster, E. (2018). Field Testing of the Use of Intake24—An Online 24-Hour Dietary Recall System. Nutrients, 10(11), 1690. https://doi.org/10.3390/nu10111690