1. Introduction
Vitamin D deficiency is one of the most common nutritional deficiencies in the world with approximately one billion people at risk [
1,
2]. It is on the rise in developed countries, even in Australia where there is an abundance of sunlight [
3]. Additional risk factors among newly settled refugees include veiling, dietary deficiencies, darker skin colour and unfamiliarity with the local healthcare system [
4,
5]. More specifically, in Australian children with vitamin D deficiency rickets, risk factors include dark skin and maternal veiling with 96–98% of these being children migrants or born to a migrant parent [
6,
7].
Vitamin D is involved in the regulation of several skeletal and non-skeletal functions through the action of its active metabolite, 1,25(OH)
2D. Research into non-skeletal effects of vitamin D has increased greatly in recent years [
8,
9]. Some of these associations include suppression of proliferation and differentiation of cancer cells, modulation of innate and adaptive immunity, modulation of muscle cell proliferation, improved cardiovascular health, modulation of pancreatic beta cell function and insulin sensitivity, clearance of amyloid plaques and promotion of survival, development and neuron function [
9,
10,
11,
12,
13]. Furthermore low vitamin D concentrations have been associated with increased longitudinal risk of hypertension, diabetes, cardiovascular disease and atherosclerosis [
11].
Vitamin D deficiency, whilst prevalent, is often asymptomatic. Clinical features include rickets, craniotabes, bone pain, muscle pain, hypocalcaemia seizures, delayed gross motor milestones and irritability [
14], but more likely in infants compared to older children and adolescents.
Increasing sunlight exposure within recommendations for the prevention of skin cancer is the ideal method of improving vitamin D status, but it may not be suitable or effective for refugee children due to darker skin colour, veiling and other socio-cultural factors [
15,
16,
17]. A recent international consensus paper recommends implementing national supplementation and fortification of food programmes with vitamin D and/or calcium to address the high rates of nutritional deficiency [
2,
18]. For high risk ethnic groups, vitamin D supplementation during every winter and spring has been suggested [
2].
Due to the longer periods of treatment required in this group, adherence with daily oral vitamin D supplementation is problematic and hence, depot (or “stoss”) vitamin D supplementation at larger doses in intervals of weeks or months may be a suitable alternative therapeutic option [
2,
19]. The use of high-dose depot vitamin D therapy is increasing, but there are little data on its use in children. In Australia, the experience with depot vitamin D therapy is limited.
In Western Australia (WA), the Humanitarian Entrant Health Service (HEHS) provides health assessments for all refugee and humanitarian entrants who have been resettled in the state under the Humanitarian Programs. Vitamin D assessment is conducted for all refugees who access this service. At the time of the study approximately10,000 refugees were resettled in Australia annually, with over 10% resettled in WA [
20]. Children represent about half of the resettled refugees. The main source regions for offshore refugee and humanitarian visas during the study period were Middle East, South West Asia and Africa [
20]. Vitamin D deficiency remains a common referral reason to the Princess Margaret Hospital for Children (PMH) Refugee Health Service (RHS) [
21].
The aim of this study was to compare the efficacy of daily and depot vitamin D therapy in newly settled refugees aged 0–16 years with low vitamin D levels and to analyse factors influencing the therapeutic outcome.
4. Discussion
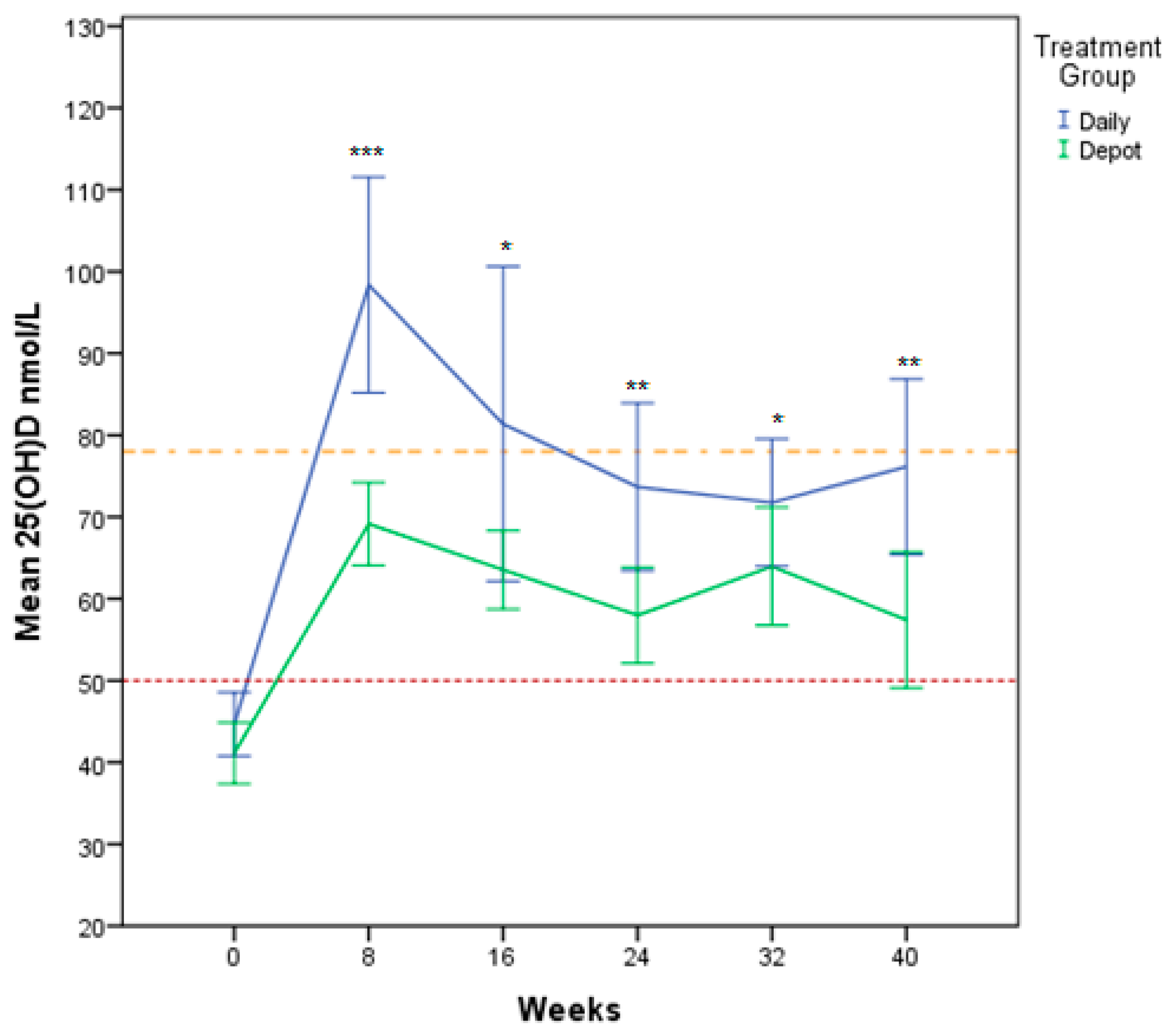
This is a randomised controlled clinical trial comparing the outcome of daily versus depot vitamin D supplementation in a group of newly-settled refugee children and adolescents in Western Australia. Participants on both daily and depot regimens achieved vitamin D sufficiency (
Figure 3). The therapeutic outcome was influenced by time, sun exposure score, calcium and treatment group. Studies looking at vitamin D status in recently arrived immigrants confirm similar patterns with highest prevalence of vitamin D deficiency in Middle Eastern populations [
30,
31]. This is of growing global importance in the context of the ongoing Syrian refugee crisis and resettlement health challenges internationally.
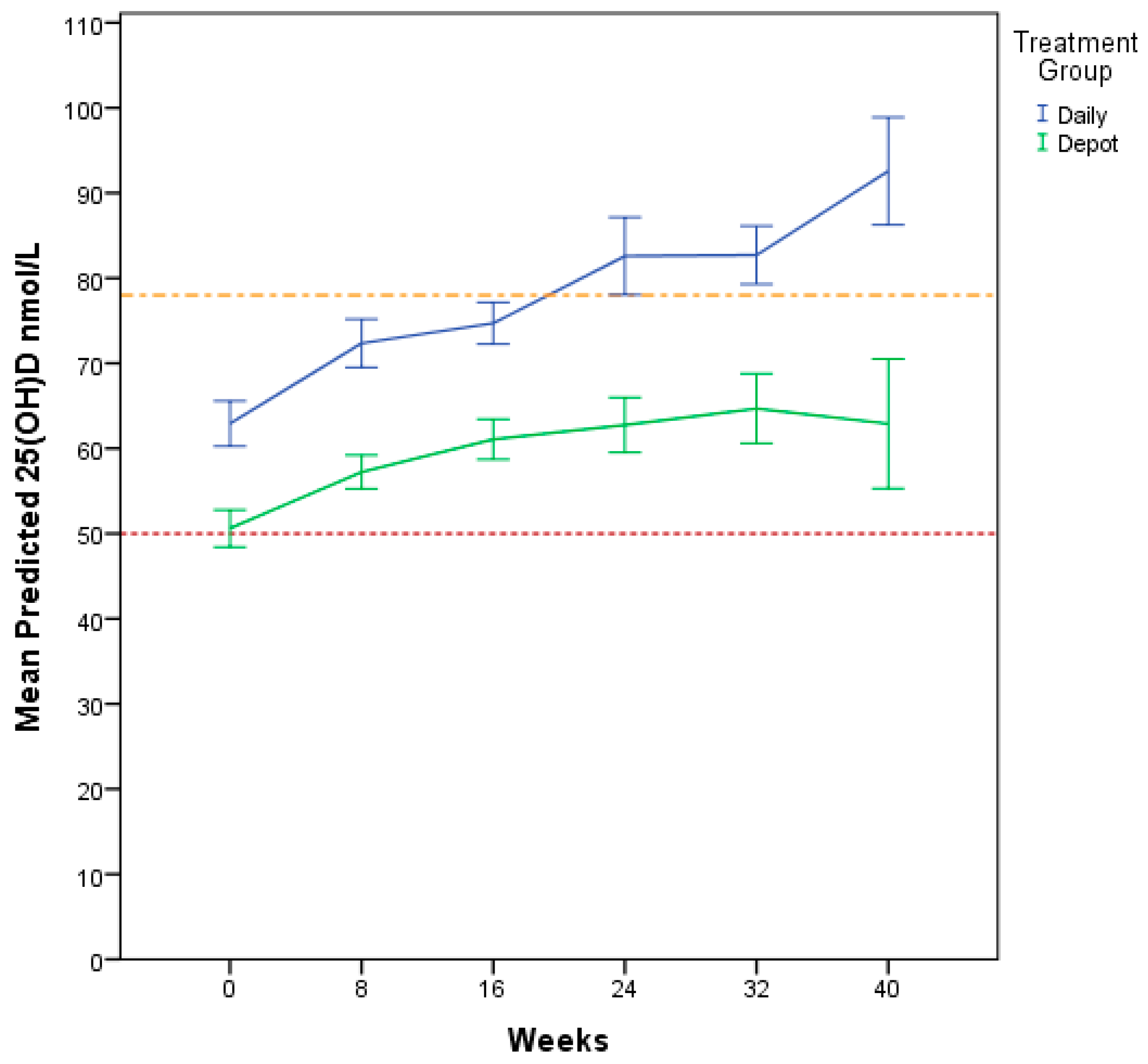
Our study demonstrated statistical difference between treatment groups for 25(OH)D at all follow up time points with higher serum levels for the daily group. Predictive modelling controlling for other determining factors supported this relationship, indicating that daily treatment was 1.5 times more likely to improve and maintain vitamin D levels. The drop in vitamin D levels for the daily treatment group after eight weeks is most likely related to a lack of adherence to treatment. With longer duration of treatment, it is possible that only the most dedicated participants showing high adherence to daily treatment regimen are remaining. This consistent decline could be due to a change in patient behaviour resulting from their involvement in a study known as the “Hawthorne effect” [
32,
33,
34]. It is also possible that this outcome was affected by the fact that the depot dose chosen was slightly lower than the potential cumulative dose for the daily doses i.e., the 5000 IU/day group would have had 280,000 IU cumulative dose (5000 IU/day × 56 days) between visits compared to the 200,000 IU given as a single depot dose. Similarly, the 2500 IU/day group received 140,000 IU cumulative dose (2500 IU × 56 days) between visits compared to the 100,000 IU given as a depot dose. We were conservative with the calculation of the depot dose as we could not include an early follow up to analyse for peak values post depot administration. A second rationale was that this would allow compensating for non-adherence in the daily group. Importantly, the study demonstrates that even with treatment at the relatively lower depot vitamin D dose, 25(OH)D levels were sufficient. For the maintenance phase, the depot dose was higher than the potential sum of the daily doses (35,000 versus 22,400 IU). This regimen allowed further stabilisation of 25 OHD levels.
Several studies have used depot or stoss therapy or daily treatment to treat vitamin D deficiency. Many of the studies are adult studies but there are increasing numbers of studies in children (
Supplementary Table S1), but study/trial designs are significantly heterogenous, making direct comparisons difficult. Importantly the variability in vitamin D replacement regimens with respect to formulation (Ergocalciferol, (vitamin D2) or Cholecalciferol (vitamin D3)), dosing (low dose 1000–5000 IU or depot 150,000–600,000 IU), frequency (daily, weekly/bi-weekly and stat/intermittent) and different routes of delivery (intramuscular or oral) may influence generalisability of results to other clinical settings.
The majority of the trials in children have used single high doses of vitamin D [
35,
36,
37,
38,
39,
40] or compared different doses or duration of depot preparations [
41,
42,
43,
44,
45,
46,
47,
48,
49,
50] for treatment. There are only limited numbers of trials comparing low dose daily against intermittent depot vitamin D therapy [
51,
52,
53,
54,
55,
56,
57,
58]. Studies using depot vitamin D treatment in children suggest that high-dose repletion approaches are safe and effective. Various combinations of high doses have been used including 600,000 IU vitamin D2 [
36], 60,000 IU vitamin D3 weekly for 4–8 weeks [
41], intermittent 50,000 IU to 300,000 IU 1–3 monthly over 12 months [
59], 600,000 IU single dose versus 60,000 IU weekly over eight weeks [
46], 45,000 IU weekly for two months [
57], 100,000 IU bimonthly (total three doses) during winter [
60] and were reported to be effective with no hypercalcaemia, hypercalcuria or nephrocalcinosis observed. Cesur et al. [
45] compared depot vitamin D doses of 150,000 IU, 300,000 IU and 600,000 IU to treat vitamin D deficiency rickets in children 3–36 months of age and showed no differences in the improvement of rickets between the different doses, but two of the 300,000 IU group (
n = 16) and six of the 600,000 IU group (
n = 16) developed hypercalcaemia. In our cohort asymptomatic hypercalcaemia was seen in only one child in the daily arm at eight weeks. Similarly, hypercalcaemia and/or hypercalciuria has been reported when 300,000 IU or 600,000 IU of an oral depot solution is used [
47,
61]. Severe hypercalcaemia was not seen in a cohort of 987 infants supplemented 400 IU to 1200 IU daily at 6 and 12 months [
62]. Interestingly, in a study by Vijayakumar and Meenu [
46] comparing effectiveness of 600,000 IU stat versus 60,000 IU weekly oral dosing in children with nutritional rickets; calcium supplementation was administered to all children for 12 months without any demonstrated increased risk of hypercalcaemia.
Some literature exists exploring safety and efficacy of comparative treatment regimens. Specifically, daily treatment (2000 IU D3 for six weeks [
51,
55,
56], 2000 IU D2 [
55,
56] and 20 days [
52], 400 IU D3 or 2000 IU D3 for two months then 1000 IU D3 daily over 12 months [
57]) against depot treatment (50,000 IU D2 weekly for six weeks [
55,
56], 150,000 IU D3 [
51] and 600,000 IU D3 [
52], 45,000 IU D3 weekly for two months then 400 IU D3 daily [
57]). Vitamin D level post treatment in depot therapy groups were significantly higher compared to daily vitamin D treatment groups [
51,
52]. No difference was seen in the other two studies [
55,
56]. Talaat et al. [
57], randomised clinically asymptomatic vitamin D deficient children aged 2 to 18 years into three different vitamin D3 replacement regimens: 400 IU daily or 45,000 IU weekly for two months then 400 IU daily or 2000 IU daily for three months then 1000 IU daily for a period of 12 months with assessment at the 4 and 12 month time points. No dosing adjustments were made to vitamin D therapy at follow up assessment. Similar to our study, daily replacement therapy was the best therapeutic regimen in maintaining sufficient vitamin D levels.
A recent global consensus statement on nutritional rickets [
2] defines vitamin D toxicity as hypercalcaemia and 25(OH)D >250 nmol/L with hypercalciuria and suppressed PTH. These cases are regarded as being rare and usually asymptomatic, limited data exists exploring toxic doses of vitamin D [
63]. In infants and young children, toxicity has been reported after dosage in the range of 240,000 IU to 4,500,000 IU [
63]. Only one participant in our study, receiving daily supplementation, had hypervitaminosis D and hypercalcaemia of 2.70 mmol/L but remained asymptomatic. We ensured the participant was being given the correct dose and not excess supplementation. Unfortunately, a renal ultrasound was not performed; levels normalised on repeat testing at 14 weeks.
Studies looking at safety of depot vitamin D therapy have not reported significant evidence of hypercalcaemia or renal nephrocalcinosis, but follow-up periods were predominantly <8 weeks. Compared to our study, relatively higher doses of depot treatment [
52] were used and in two of the studies, vitamin D2 rather than vitamin D3 was used. Our cohort provides longitudinal data to 40 weeks, which is a key strength of this study. Talaat et al. [
57] reported calcium and hypercalciuria at 4 months and found up to 1.5% of cases hypercalciuria in the daily replacement group and no reported hypercalcaemia in any of the participants. It is postulated that daily or weekly therapy are more physiological and effective with less adverse effects compared to depot therapy [
22,
64]. However, depot therapy is a preferred option when adherence to therapy is uncertain [
2].
None of our participants had clinical signs of rickets; routine radiological imaging was not undertaken. Similarly, in a study by Jain et al. [
65], none of the 98 infants (aged 2.5–3.5 months) with 25(OH)D <25 nmol/L showed any clinical signs of rickets. Studies by Ladhani et al. [
66], Gordon et al. [
67] and Perez-Rossello [
68] included radiological assessment in addition to clinical assessment in children with vitamin D deficiency and reported radiological changes in 32.5% (all clinically asymptomatic) to 70% (no mention of clinical evidence of rickets) of the children with vitamin D deficiency. Given the varying aetiology and prevalence of rickets in infants, children and adolescents with vitamin D deficiency, clinical signs alone are not adequate for screening and diagnosis. The role of ALP as a screening parameter for vitamin D deficiency is controversial. ALP is an enzyme found in all body tissues, including osteoblasts where it is a marker for bone formation. It is especially utilised as a bone marker due to being cost effective. Whilst levels of ALP have been noted to raise during vitamin D deficiency, thought to be due to regeneration of bone tissue, it is not a suitable marker for children due to its wide distribution and increase during skeletal growth [
69,
70]. ALP levels vary according to age, race and gender, making it difficult to associate vitamin D deficiency with ALP levels alone [
71,
72,
73,
74]. In our study clinical findings and ALP were not reliable markers of vitamin D deficiency in line with other studies [
70]. We did not measure bone specific ALP, which has been shown to be a reliable marker [
18]. Population-based screening with serum 25(OH)D, ALP and radiographs is not recommended [
2]. However, testing serum 25(OH)D in at risk populations can be considered.
Depot therapy has been proposed as an alternative to daily therapy to improve the therapeutic outcome. In the Global Consensus paper daily therapy was preferred over depot therapy acknowledging that depot therapy may be more practical in certain situations such as non-adherence to treatment [
2]. An important factor in the context is that depot therapy can be administered under supervision in clinic. A successful example for this strategy is “directly observed therapy for treating tuberculosis” [
75]. Depot utilisation in more vulnerable clinical cohorts (e.g., young children, adolescents, limited English proficiency or itinerant populations) also needs consideration.
Significant predictors of 25(OH)D serum levels were time, treatment group, calcium and sun exposure score. Gender, age, season and country of refuge/origin did not significantly influence the treatment effectiveness depending on chosen cut-off points. A significant positive change in sun exposure scores at each of the follow up visits was observed in the daily treatment group compared to the depot group, with statistically significant group differences at 24, 32 and 40 weeks. It is likely that taking daily treatment is a reminder of need for sun exposure as opposed to depot treatment. A positive association between sun exposure and 25(OH)D3 levels has been confirmed in a few studies by Jones et al. [
26,
76], although this association became non-significant once adjusted for number of sports played [
26]. Unfortunately, in our study, sport participation information was not obtained.
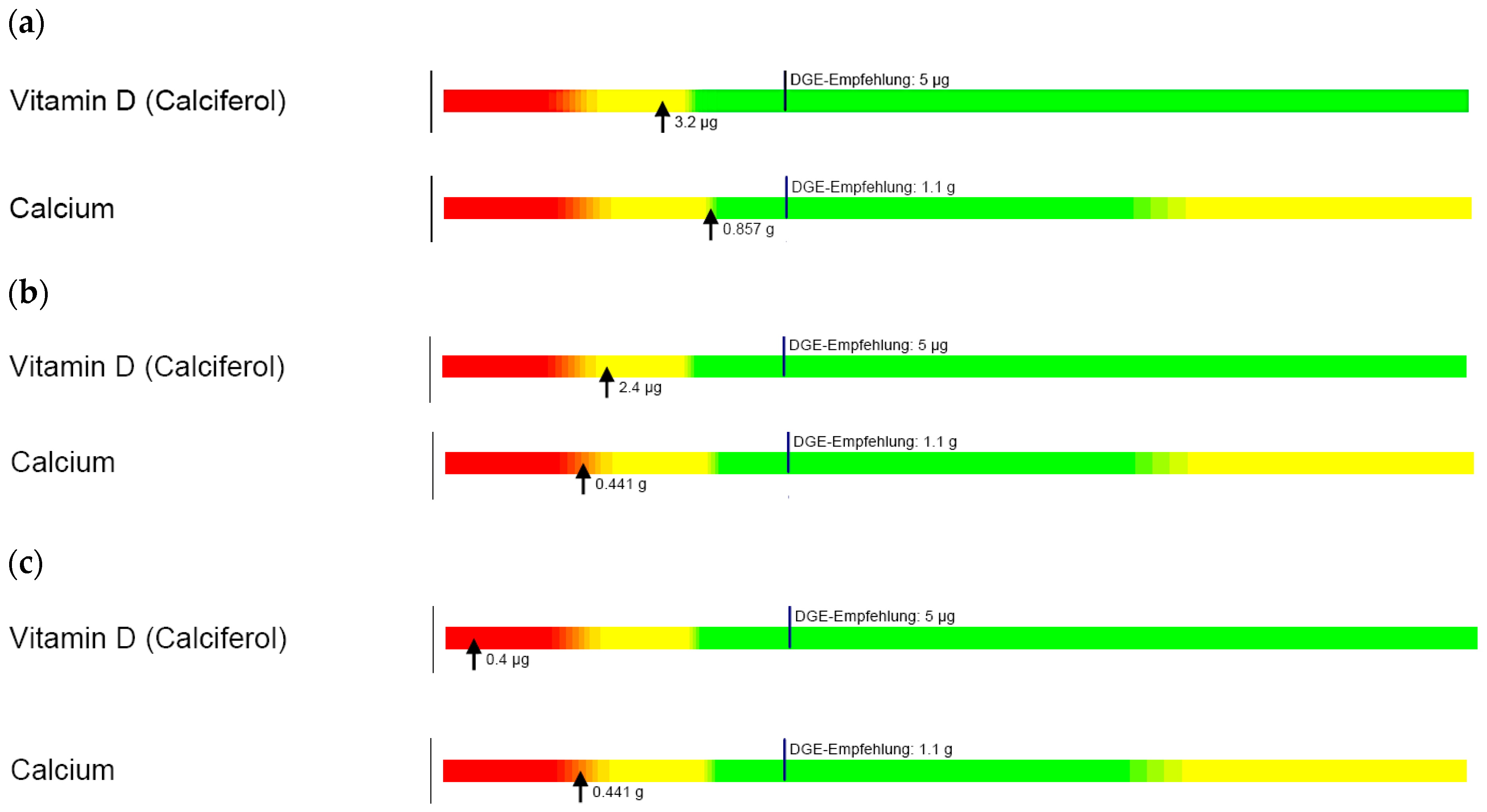
Dietary analysis confirmed that traditional diets of all families, regardless of ethnic background, were deficient in calcium and vitamin D. Newly settled migrants and refugees are often in poor health due to prolonged periods in their country of origin or refuge before entering Australia [
5,
77]. Once in Australia, unfamiliarity with local produce, food insecurity, accessibility, limited health literacy, language barriers and acculturation (e.g., consumption of high-fat, high-calorie fast foods) can further influence suboptimal nutrition [
5,
77,
78,
79]. Our data demonstrate the importance of nutritional assessment for refugee children and provision of culturally appropriate health and nutrition education to allow families to familiarise themselves with local produce and foods and optimise nutritional intake in keeping with age-appropriate recommendations [
79].
There were limitations to this study design. This study focussed on prospective longitudinal follow up of vitamin D treatment using different treatment modes. As such, one limitation is the lack of data regarding potential vitamin D toxicity at the end of the initial two weeks following depot treatment as there was no follow up at this time point.
It should be noted that the study was underpowered statistically at 40 weeks for the daily group, although statistical significance was still shown, suggesting sufficient power. Post study design and implementation, it was decided to analyse four categories of Vitamin D, hence the Chi square analysis is likely underpowered for detecting significant group differences, but data suggests that there is a difference between treatment groups and Vitamin D categories that should be further explored in future research studies.
Loss to follow-up was significant, however engagement through the paediatric RHS facilitated longitudinal follow-up, particularly in a mobile and predominantly non-English proficient cohort. No comparative international data currently exist beyond a period post-treatment; our data provide important evidence to improve this gap in knowledge. Importantly, sample selection bias was negated by the recruitment through the centralised refugee screening service.
Different study preparations of vitamin D solutions were utilised; the daily regimen arm received a commercially available preparation whilst the depot D3 therapy was prepared by the Clinical Trials Pharmacy. The depot solution required refrigeration and any precipitation may have altered the concentration of the solution, although precautions were in place in the study protocol with respect to time for warming prior to administration. Consequently, the solution half-lives of the solutions may have differed however the high number of participants and long duration of the study is likely to have reduced this variability.
Compliance with the daily vitamin D supplementation was assessed by parental report via interpreters, but formal review of bottles was not undertaken. Similarly, a degree of recall bias may have influenced sun exposure reporting and dietary questionnaires. Interestingly, vitamin D intoxication was only noted in the daily treatment group at the scheduled visits. It can be speculated that this risk of overdosing on daily therapy needs to be considered as a factor in favour of depot therapy when depot therapy under supervision represents a safe alternative.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}