Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaires
2.2. Statistical Analysis
3. Results
3.1. DH Patients with Normal Villous Architecture Compared to DH Patients with Villous Atrophy at Diagnosis
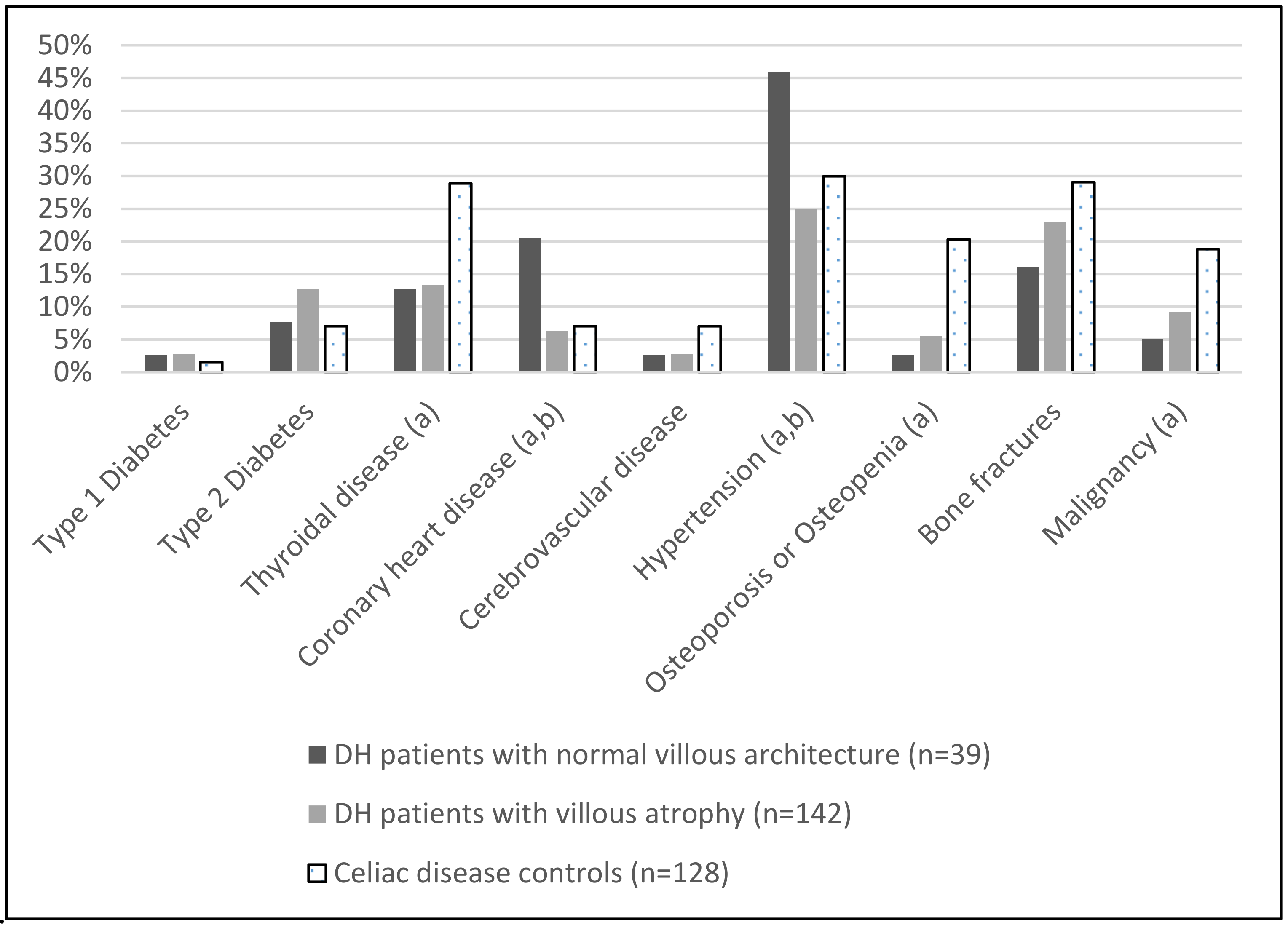
3.2. Comparisons between the DH Patients and the Classical Coeliac Disease Controls
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Salmi, T.; Hervonen, K.; Kautiainen, H.; Collin, P.; Reunala, T. Prevalence and incidence of dermatitis herpetiformis: A 40-year prospective study from Finland. Br. J. Dermatol. 2011, 165, 354–359. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Fleming, K.M.; Tata, L.J.; Card, T.R.; Crooks, C.J. Incidence and prevalence of celiac disease and dermatitis herpetiformis in the UK over two decades: Population-based study. Am. J. Gastroenterol. 2014, 109, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Bolotin, D.; Petronic-Rosic, V. Dermatitis herpetiformis: Part I. Epidemiology, pathogenesis, and clinical presentation. J. Am. Acad. Dermatol. 2011, 64, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Spurkland, A.; Ingvarsson, G.; Falk, E.; Knutsen, I.; Sollid, L.; Thorsby, E. Dermatitis herpetiformis and celiac disease are both primarily associated with the HLA-DQ (α1* 0501,(β1* 02) or the HLA-DQ (α1* 03,(β1* 0302) heterodimers. HLA 1997, 49, 29–34. [Google Scholar] [CrossRef]
- Collin, P.; Salmi, T.T.; Hervonen, K.; Kaukinen, K.; Reunala, T. Dermatitis herpetiformis: A cutaneous manifestation of coeliac disease. Ann. Med. 2017, 49, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, W.; Ehnis, T.; Bauer, M.; Donner, P.; Volta, U.; Riecken, E.O.; Schuppan, D. Identification of tissue transglutaminase as the autoantigen of celiac disease. Nat. Med. 1997, 3, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Korponay-Szabó, I.R.; Halttunen, T.; Szalai, Z.; Laurila, K.; Kiraly, R.; Kovacs, J.; Fésüs, L.; Mäki, M. In vivo targeting of intestinal and extraintestinal transglutaminase 2 by coeliac autoantibodies. Gut 2004, 53, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Salmi, T.T.; Hervonen, K.; Laurila, K.; Collin, P.; Mäki, M.; Koskinen, O.; Huhtala, H.; Kaukinen, K.; Reunala, T. Small bowel transglutaminase 2-specific IgA deposits in dermatitis herpetiformis. Acta Derm. Veneorol. 2014, 94, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, W.; Schuppan, D.; Laag, E.; Bruckner-Tuderman, L.; Reunala, T.; Kárpáti, S.; Zágoni, T.; Riecken, E.O. Antibodies to tissue transglutaminase as serologic markers in patients with dermatitis herpetiformis. J. Investig. Dermatol. 1999, 113, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Zone, J.J.; Meyer, L.J.; Petersen, M.J. Deposition of granular IgA relative to clinical lesions in dermatitis herpetiformis. Arch. Dermatol. 1996, 132, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Sárdy, M.; Kárpáti, S.; Merkl, B.; Paulsson, M.; Smyth, N. Epidermal transglutaminase (TGase3) is the autoantigen of dermatitis herpetiformis. J. Exp. Med. 2002, 195, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Marietta, E.V.; Camilleri, M.J.; Castro, L.A.; Krause, P.K.; Pittelkow, M.R.; Murray, J.A. Transglutaminase autoantibodies in dermatitis herpetiformis and celiac sprue. J. Investig. Dermatol. 2008, 128, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Hull, C.M.; Liddle, M.; Hansen, N.; Meyer, L.; Schmidt, L.; Taylor, T.; Jaskowski, T.; Hill, H.; Zone, J. Elevation of IgA anti-epidermal transglutaminase antibodies in dermatitis herpetiformis. Br. J. Dermatol. 2008, 159, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Salmi, T.T.; Kurppa, K.; Hervonen, K.; Laurila, K.; Collin, P.; Huhtala, H.; Saavalainen, P.; Sievänen, H.; Reunala, T.; Kaukinen, K. Serum transglutaminase 3 antibodies correlate with age at celiac disease diagnosis. Dig. Liver Dis. 2016, 48, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Marks, J.; Shuster, S.; Watson, A. Small-bowel changes in dermatitis herpetiformis. Lancet 1966, 288, 1280–1282. [Google Scholar] [CrossRef]
- Mansikka, E.; Hervonen, K.; Salmi, T.T.; Kautiainen, H.; Kaukinen, K.; Collin, P.; Reunala, T. The decreasing prevalence of severe villous atrophy in dermatitis herpetiformis: A 45-year experience in 393 patients. J. Clin. Gastroenterol. 2017, 51, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Kárpáti, S. Dermatitis herpetiformis: Close to unravelling a disease. J. Dermatol. Sci. 2004, 34, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Zone, J.J. Skin manifestations of celiac disease. Gastroenterology 2005, 128, S87–S91. [Google Scholar] [CrossRef] [PubMed]
- Fry, L.; Riches, D.; Seah, P.; Hoffbrand, A. Clearance of skin lesions in dermatitis herpetiformis after gluten withdrawal. Lancet 1973, 301, 288–291. [Google Scholar] [CrossRef]
- Kaplan, R.P.; Callen, J.P. Dermatitis herpetiformis: Autoimmune disease associations. Clin. Dermatol. 1991, 9, 347–360. [Google Scholar] [CrossRef]
- Hervonen, K.; Viljamaa, M.; Collin, P.; Knip, M.; Reunala, T. The occurrence of type 1 diabetes in patients with dermatitis herpetiformis and their first-degree relatives. Br. J. Dermatol. 2004, 150, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.; Magazzù, G.; Greco, L. Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. Gastroenterology 1999, 117, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Viljamaa, M.; Kaukinen, K.; Pukkala, E.; Hervonen, K.; Reunala, T.; Collin, P. Malignancies and mortality in patients with coeliac disease and dermatitis herpetiformis: 30-year population-based study. Dig. Liver Dis. 2006, 38, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Hervonen, K.; Vornanen, M.; Kautiainen, H.; Collin, P.; Reunala, T. Lymphoma in patients with dermatitis herpetiformis and their first-degree relatives. Br. J. Dermatol. 2005, 152, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Dimenäs, E.; Carlsson, G.; Glise, H.; Israelsson, B.; Wiklund, I. Relevance of norm values as part of the documentation of quality of life instruments for use in upper gastrointestinal disease. Scand. J. Gastroenterol. 1996, 31, 8–13. [Google Scholar] [CrossRef]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Ciacci, C.; Green, P.H.; Kaukinen, K.; Korponay-Szabo, I.R.; Kurppa, K.; Murray, J.A.; Lundin, K.E.A.; Maki, M.J.; Popp, A. Outcome measures in coeliac disease trials: The Tampere recommendations. Gut 2018. [Google Scholar] [CrossRef] [PubMed]
- Hindryckx, P.; Levesque, B.G.; Holvoet, T.; Durand, S.; Tang, C.-M.; Parker, C.; Khanna, R.; Shackelton, L.M.; D’haens, G.; Sandborn, W.J. Disease activity indices in coeliac disease: Systematic review and recommendations for clinical trials. Gut 2016, 67, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Roos, S.; Kärner, A.; Hallert, C. Psychological well-being of adult coeliac patients treated for 10 years. Dig. Liver Dis. 2006, 38, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Viljamaa, M.; Collin, P.; Huhtala, H.; Sievänen, H.; Mäki, M.; Kaukinen, K. Is coeliac disease screening in risk groups justified? A fourteen-year follow-up with special focus on compliance and quality of life. Aliment. Pharmacol. Ther. 2005, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Svensson, M.; Tholstrup, J.; Hultberg, B. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Aliment. Pharmacol. Ther. 2009, 29, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Khan, G. Dermatology life quality index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Fry, L.; Keir, P.; McMinn, R.; Cowan, J.; Hoffbrand, A. Small-intestinal structure and function and haematological changes in dermatitis herpetiformis. Lancet 1967, 290, 729–734. [Google Scholar] [CrossRef]
- Mansikka, E.; Salmi, T.; Kaukinen, K.; Collin, P.; Huhtala, H.; Reunala, T.; Hervonen, K. Diagnostic delay in dermatitis herpetiformis in a high-prevalence area. Acta Derm. Venereol. 2018, 98, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Fry, L.; Leonard, J.; Swain, F.; Tucker, W.; Haffenden, G.; Ring, N.; McMinn, R. Long term follow-up of dermatitis herpetiformis with and without dietary gluten withdrawal. Br. J. Dermatol. 1982, 107, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Gawkrodger, D.; Blackwell, J.; Gilmour, H.; Rifkind, E.; Heading, R.; Barnetson, R. Dermatitis herpetiformis: Diagnosis, diet and demography. Gut 1984, 25, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Hervonen, K.; Alakoski, A.; Salmi, T.; Helakorpi, S.; Kautiainen, H.; Kaukinen, K.; Pukkala, E.; Collin, P.; Reunala, T. Reduced mortality in dermatitis herpetiformis: A population-based study of 476 patients. Br. J. Dermatol. 2012, 167, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Tio, M.; Cox, M.; Eslick, G. Meta-analysis: Coeliac disease and the risk of all-cause mortality, any malignancy and lymphoid malignancy. Aliment. Pharmacol. Ther. 2012, 35, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Reunala, T.; Collin, P. Diseases associated with dermatitis herpetiformis. Br. J. Dermatol. 1997, 136, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Krishnareddy, S.; Lewis, S.K.; Green, P.H. Dermatitis herpetiformis: Clinical presentations are independent of manifestations of celiac disease. Am. J. Clin. Dermatol. 2014, 15, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Pasternack, C.; Kaukinen, K.; Kurppa, K.; Mäki, M.; Collin, P.; Reunala, T.; Huhtala, H.; Salmi, T. Quality of life and gastrointestinal symptoms in long-term treated dermatitis herpetiformis patients: A cross-sectional study in Finland. Am. J. Clin. Dermatol. 2015, 16, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Salmi, T.T.; Collin, P.; Korponay-Szabo, I.R.; Laurila, K.; Partanen, J.; Huhtala, H.; Kiraly, R.; Lorand, L.; Reunala, T.; Mäki, M. Endomysial antibody-negative coeliac disease: Clinical characteristics and intestinal autoantibody deposits. Gut 2006, 55, 1746–1753. [Google Scholar] [CrossRef] [PubMed]
- Vivas, S.; De Morales, J.M.R.; Fernandez, M.; Hernando, M.; Herrero, B.; Casqueiro, J.; Gutierrez, S. Age-related clinical, serological, and histopathological features of celiac disease. Am. J. Gastroenterol. 2008, 103, 2360. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| DH Patients | CD Controls (n = 248) | p-Value * | ||
|---|---|---|---|---|
| With Normal Villous Architecture (n = 98) | With Villous Atrophy (n = 254) | |||
| Females; n (%) | 50 (51) | 125 (49) | 193 (78) | <0.001 |
| Age at diagnosis; median (range) | 52 (3–84) | 37 (4–78) | 42 (7–75) | <0.001 a |
| Coeliac autoantibodies 1 present in the serum at diagnosis; n (%) | 28/72 (39) | 139/191 (73) | 124/148 (84) | <0.001 a |
| Haemoglobin level at diagnosis 2, g/L; median (Q1–Q3) 3 | 138 (128–148) | 136 (129–146) | 130 (121–140) | 0.057 |
| Dapsone treatment used; n (%) | 75/93 (81) | 191/243 (79) | - | - |
| Duration of dapsone treatment, months; median (range) | 36 (5–324) | 24 (2–384) | - | - |
| DH Patients | CD Controls (n = 128) | p-Value * | ||
|---|---|---|---|---|
| With Normal Villous Architecture (n = 39) | With Villous Atrophy (n = 142) | |||
| Females; n (%) | 18 (46) | 67 (47) | 104 (81) | <0.001 |
| Follow-up time, years; median (range) | 20 (1–44) | 23 (1–42) | 18 (6–43) | 0.003 |
| Age; median (range) | 68 (52–85) | 61 (18–96) | 65 (34–85) | <0.001 a |
| BMI, kg/m2; median (range) | 25 (19–37) | 25 (16–38) | 26 (15–46) | 0.772 |
| Strict adherence to GFD, no dietary lapses; n (%) | 30 (77) | 101 (71) | 107 (84) | 0.170 b |
| Number of long-term illnesses; median (range) | 1 (0–7) | 1 (0–14) | 2 (0–9) | <0.001 |
| Number of prescription medications used; median (range) | 2 (0–11) | 1 (0–18) | 3 (0–16) | 0.078 |
| Uses statin medication; n (%) | 14 (36) | 21 (15) | 15 (12) | 0.001 c |
| Uses antihypertensive medication; n (%) | 20 (51) | 50 (35) | 49 (38) | 0.188 |
| Uses proton pump inhibitor medication; n (%) | 5 (13) | 16 (11) | 16 (13) | 0.938 |
| Number of over-the-counter medications used; median (range) | 0 (0–5) | 1 (0–7) | 2 (0–7) | <0.001 |
| Number of children born; median (range) | 2 (0–5) | 2 (0–6) | 2 (0–5) | 0.497 |
| First-degree relatives with DH or CD; n (%) | 13 (33) | 53 (37) | 55 (43) | 0.464 |
| DH Patients | CD Controls (n = 128) | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|
| With Normal Villous Architecture (n = 39) | With Villous Atrophy (n = 142) | |||||||
| PGWB | median | (Q1–Q3) | median | (Q1–Q3) | median | (Q1–Q3) | ||
| Total | 110 | (99–116) | 110 | (101–117) | 106 | (96–117) | 0.200 | |
| Anxiety | 26 | (23–27) | 26 | (23–27) | 25 | (23–28) | 0.891 | |
| Depression | 17 | (16–18) | 17 | (16–18) | 17 | (15–18) | 0.587 | |
| Well-being | 18 | (16–20) | 18 | (16–20) | 18 | (16–20) | 0.279 | |
| Self-control | 16 | (15–17) | 16 | (15–17) | 16 | (14–17) | 0.295 | |
| General health | 13 | (12–15) | 14 | (12–16) | 13 | (11–15) | 0.022 | |
| Vitality | 20 | (17–21) | 19 | (17–21) | 18 | (16–20) | 0.104 | |
| GSRS | median | (Q1–Q3) | median | (Q1–Q3) | median | (Q1–Q3) | ||
| Total | 1.6 | (1.3–2.0) | 1.7 | (1.3–2.3) | 2.1 | (1.5–4.2) | <0.001 | |
| Diarrhoea | 1.0 | (1.0–1.7) | 1.3 | (1.0–2.3) | 1.7 | (1.0–2.7) | 0.006 | |
| Indigestion | 1.8 | (1.5–2.5) | 2.0 | (1.5–2.5) | 2.0 | (1.5–3.0) | 0.227 | |
| Constipation | 1.7 | (1.0–2.3) | 1.7 | (1.0–2.3) | 1.7 | (1.0–2.4) | 0.482 | |
| Pain | 1.3 | (1.0–1.7) | 1.7 | (1.0–2.0) | 1.7 | (1.3–2.3) | 0.007 | |
| Reflux | 1.0 | (1.0–1.5) | 1.0 | (1.0–2.0) | 1.5 | (1.0–2.0) | 0.084 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansikka, E.; Hervonen, K.; Kaukinen, K.; Collin, P.; Huhtala, H.; Reunala, T.; Salmi, T. Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis. Nutrients 2018, 10, 641. https://doi.org/10.3390/nu10050641
Mansikka E, Hervonen K, Kaukinen K, Collin P, Huhtala H, Reunala T, Salmi T. Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis. Nutrients. 2018; 10(5):641. https://doi.org/10.3390/nu10050641
Chicago/Turabian StyleMansikka, Eriika, Kaisa Hervonen, Katri Kaukinen, Pekka Collin, Heini Huhtala, Timo Reunala, and Teea Salmi. 2018. "Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis" Nutrients 10, no. 5: 641. https://doi.org/10.3390/nu10050641
APA StyleMansikka, E., Hervonen, K., Kaukinen, K., Collin, P., Huhtala, H., Reunala, T., & Salmi, T. (2018). Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis. Nutrients, 10(5), 641. https://doi.org/10.3390/nu10050641