A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation


Abstract
:1. Introduction
2. Materials and Methods
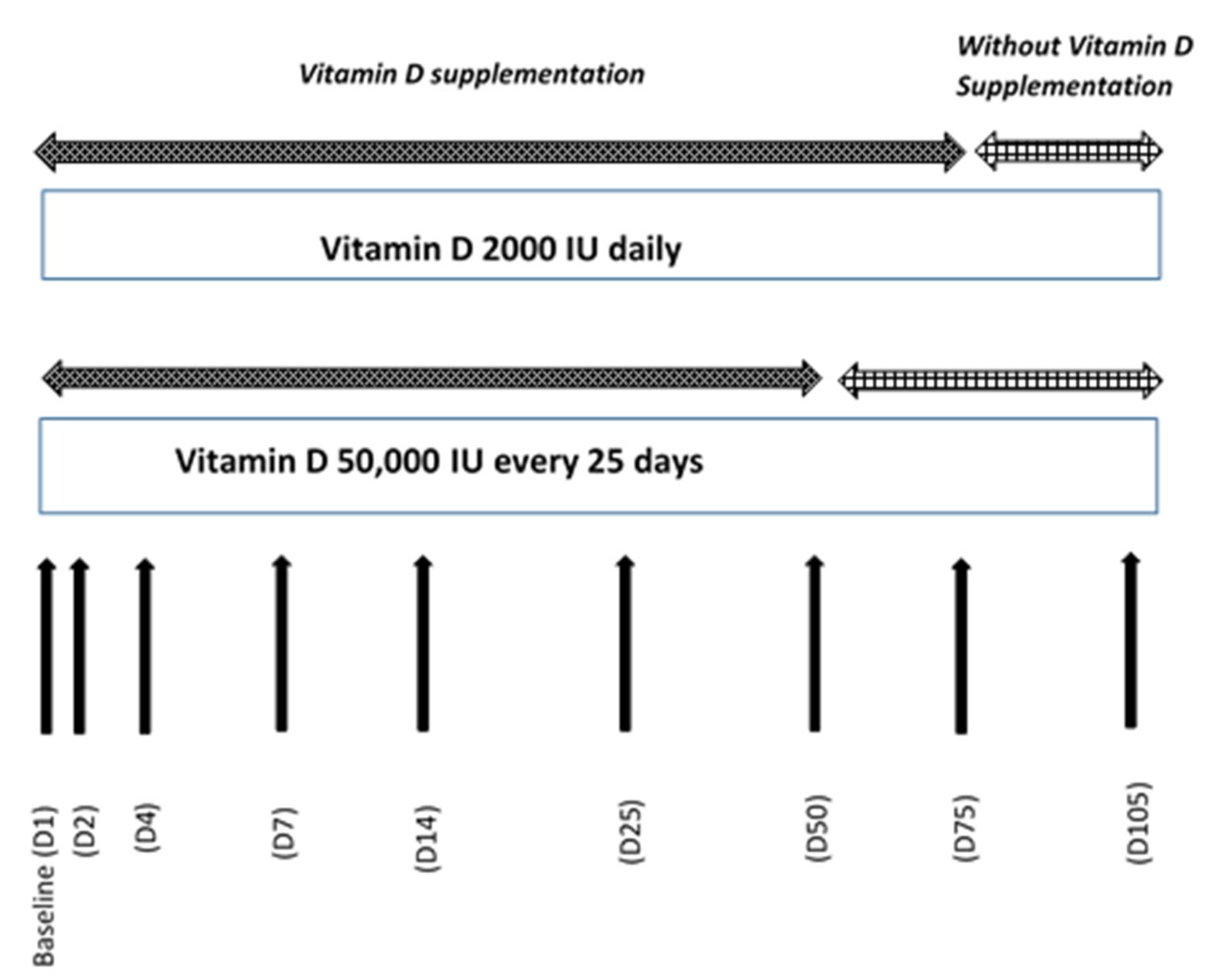
2.1. Methodology
2.2. Study Population
2.3. Laboratory Tests
2.4. Statistical Analyses
3. Results
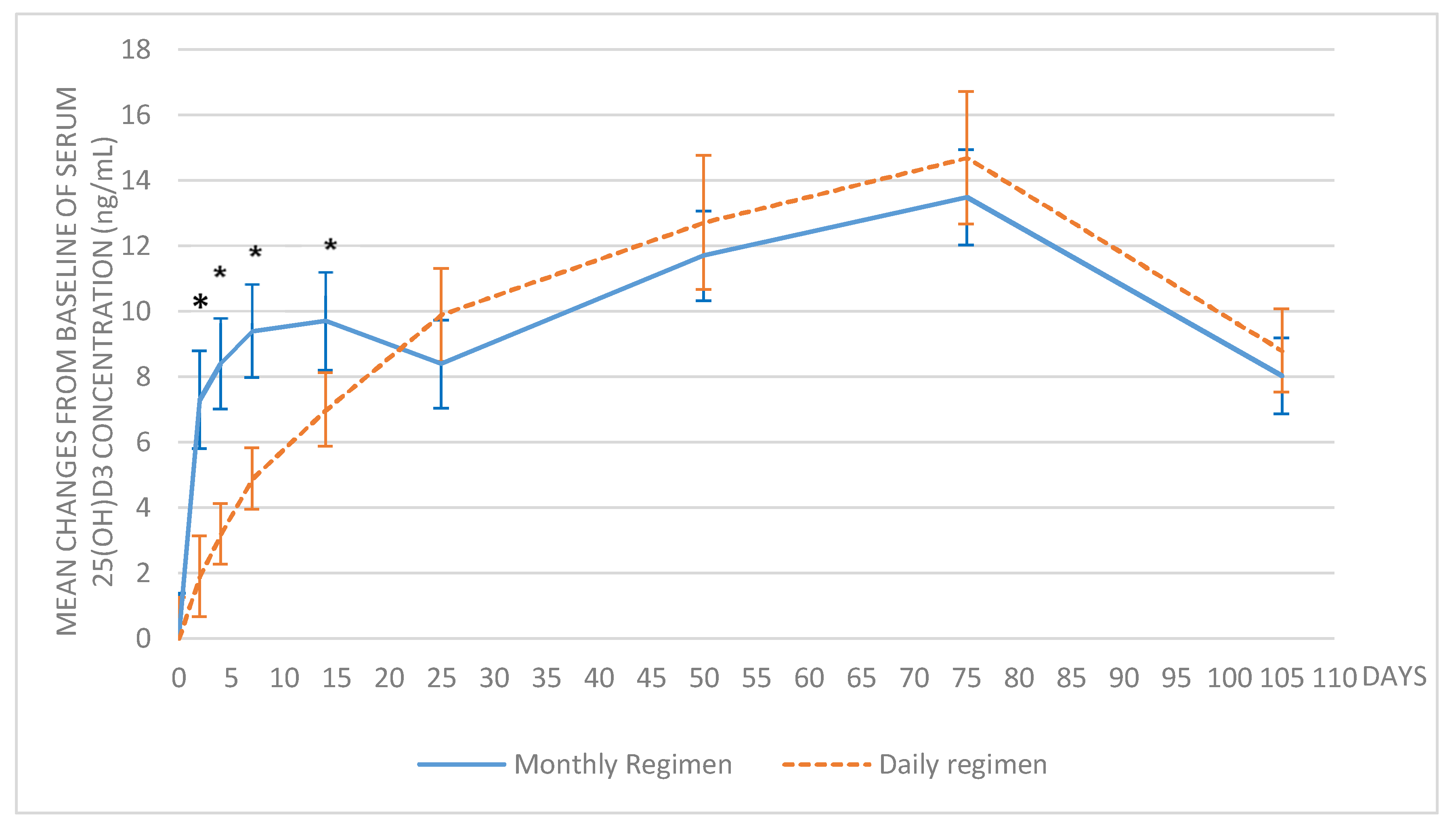
3.1. Evolution of 25(OH)D3
3.2. Evolution of 1,25(OH)2D3
3.3. Time to Definite Achievement of 25(OH)D3 Target
3.4. Safety Assessment
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Zadshir, A.; Tareen, N.; Pan, D.; Norris, K.; Martins, D. The prevalence of hypovitaminosis D among US adults: Data from the NHANES III. Ethn. Dis. 2005, 15, 97–101. [Google Scholar]
- Goodman, W.G.; London, G.; Amann, K.; Block, G.A.; Giachelli, C.; Hruska, K.A.; Ketteler, M.; Levin, A.; Massy, Z.; McCarron, D.A.; et al. Vascular calcification in chronic kidney disease. Am. J. Kidney Dis. 2004, 43, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, O.M.; Mannstadt, M.; Isakova, T.; Rauh-Hain, J.A.; Tamez, H.; Shah, A.; Smith, K.; Lee, H.; Thadhani, R.; Jüppner, H.; et al. Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N. Engl. J. Med. 2008, 359, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Isakova, T.; Xie, H.L.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutiérrez, O.M.; Steigerwalt, S.; He, J.; et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.G.; Myrtle, J.F.; Tsai, H.C.; Norman, A.W. The occurrence and biological activity of 1,25-dihydroxy-vitamin D3 in bone. J. Biol. Chem. 1972, 247, 5728–5735. [Google Scholar] [PubMed]
- Tsai, H.C.; Wong, R.G.; Norman, A.W. Subcellular localization of 1,25-dihydroxy-vitamin D3 in intestinal mucosa and correlation with increased calcium transport. J. Biol. Chem. 1972, 247, 5511–5519. [Google Scholar] [PubMed]
- Myrtle, J.F.; Norman, A.W. Vitamin D: A cholecalciferol metabolite highly active in promoting intestinal calcium transport. Science 1971, 171, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.; Farrell, C.J.L.; Pusceddu, I.; Fabregat-Cabello, N.; Cavalier, E. Assessment of vitamin D status—A changing landscape. Clin. Chem. Lab. Med. 2017, 55, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; et al. IOM committee members respond to Endocrine Society vitamin D guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Boonen, S.; Brandi, M.L.; Bruyère, O.; Cooper, C.; Kanis, J.A.; Kaufman, J.M.; Ringe, J.D.; Weryha, G.; Reginster, J.Y. Vitamin D supplementation in elderly or postmenopausal women: A 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Curr. Med. Res. Opin. 2013, 29, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Willett, W.C.; Orav, E.J.; Lips, P.; Meunier, P.J.; Lyons, R.A.; Flicker, L.; Wark, J.; Jackson, R.D.; Cauley, J.A.; et al. A pooled analysis of vitamin D dose requirements for fracture prevention. N. Engl. J. Med. 2012, 367, 40–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Kiely, M. Recommended dietary intakes for vitamin D: Where do they come from, what do they achieve and how can we meet them? J. Hum Nutr. Diet. 2014, 27, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S.; Gold, D.T. Compliance and persistence with osteoporosis medications: A critical review of the literature. Rev. Endocr. Metab. Disord. 2010, 11, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: A meta-analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef]
- Di Mauro, G.; Saggese, G. Italian Consensus on vitamin D in Infants and Children. Prev. Soc. Pediatr. 2015, 3, 154–188. [Google Scholar]
- Rabenda, V.; Mertens, R.; Fabri, V.E.; Vanoverloop, J.; Sumkay, F.; Vannecke, C.; Deswaef, A.; Verpooten, G.A.; Reginster, J.Y. Adherence to bisphosphonates therapy and hip fracture risk in osteoporotic women. Osteoporos. Int. 2008, 19, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Rabenda, V.; Hiligsmann, M.; Reginster, J.Y. Poor adherence to oral bisphosphonate treatment and its consequences: A review of the evidence. Expert. Opin. Pharmacother. 2009, 10, 2303–2315. [Google Scholar] [CrossRef] [PubMed]
- Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of daily, weekly, and monthly vitamin D3 in ethanol dosing protocols for two months in elderly hip fracture patients. J. Clin. Endocrinol. Metab. 2008, 93, 3430–3435. [Google Scholar] [CrossRef] [PubMed]
- Takacs, I.; Toth, B.E.; Szekeres, L.; Szabo, B.; Bakos, B.; Lakatos, P. Randomized clinical trial to comparing efficacy of daily, weekly and monthly administration of vitamin D3. Endocrine 2016, 55, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Chel, V.; Wijnhoven, H.A.; Smit, J.H.; Ooms, M.; Lips, P. Efficacy of different doses and time intervals of oral vitamin D supplementation with or without calcium in elderly nursing home residents. Osteoporos. Int. 2008, 19, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Cavalier, E.; Lukas, P.; Crine, Y.; Peeters, S.; Carlisi, A.; Le Goff, C.; Gadisseur, R.; Delanaye, P.; Souberbielle, J.C. Evaluation of automated immunoassays for 25(OH)-vitamin D determination in different critical populations before and after standardization of the assays. Clin. Chim. Acta 2014, 431, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Gemar, D.; Engelke, J.; Gangnon, R.; Ramamurthy, R.; Krueger, D.; Drezner, M.K. Evaluation of ergocalciferol or cholecalciferol dosing 1600 IU daily or 50000 IU monthly in older adults. J. Clin. Endocrinol. Metab. 2011, 96, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Courbebaisse, M.; Thervet, E.; Souberbielle, J.C.; Zuber, J.; Eladari, D.; Martinez, F.; Mamzer-Bruneel, M.F.; Urena, P.; Legendre, C.; Friedlander, G.; et al. Effects of vitamin D supplementation on the calcium-phosphate balance in renal transplant patients. Kidney Int. 2009, 75, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, E.; Mascia, M.L.; Cipriani, C.; Fassino, V.; Mazzei, F.; D’erasmo, E.; Carnevale, V.; Scillitani, A.; Minisola, S. Short and long-term variations in serum calciotropic hormones after a single very large dose of ergocalciferol (vitamin D2) or cholecalciferol (vitamin D3) in the elderly. J. Clin. Endocrinol. Metab. 2008, 93, 3015–3020. [Google Scholar] [CrossRef] [PubMed]
- Bacon, C.J.; Gamble, G.D.; Horne, A.M.; Scott, M.A.; Reid, I.R. High-dose oral vitamin D3 supplementation in the elderly. Osteoporos. Int. 2009, 20, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Cavalier, E.; Faché, W.; Souberbielle, J.C. A randomised, double-blinded, placebo-controlled, parallel study of vitamin D3 supplementation with different schemes based on multiples of 25,000 IU doses. Int. J. Endocrinol. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 30, 1815–1822. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Monthly Regimen n = 30 | Daily Regimen n = 30 | ||
|---|---|---|---|
| Age (years) | |||
| Mean ± SD | 29.8 ± 9.5 | 29.4 ± 7.7 | |
| [min–max] | [19.0–53.0] | [19.0–44.0] | |
| Gender | |||
| Male | N (%) | 9 (30%) | 13 (43.33%) |
| Female | N (%) | 21 (70%) | 17 (56.67%) |
| BMI (kg/m2) | Mean ± SD | 22.0 ± 2.1 | 21.9 ± 1.9 |
| [min–max] | [18.2–25.0] | [18.3–25.0] |
| Daily Regimen (Mean ± SD) | Monthly Regimen (Mean ± SD) | |
|---|---|---|
| ALBUMIN (g/L) | ||
| Baseline | 46.7 ± 2.5 | 46.9 ± 2.3 |
| Day 105 | 46.6 ± 2.4 | 46.1 ± 2.4 |
| Change (Day 105—Baseline) * | −0.1 ± 2.3 | −0.8 ± 2.3 |
| CREATININE (mg/dL) | ||
| Baseline | 0.8 ± 0.2 | 0.8 ± 0.1 |
| Day 105 | 0.8 ± 0.2 | 0.9 ± 0.1 |
| Change (Day 105—Baseline) * | −0.0 ± 0.1 | 0.0 ± 0.1 |
| PHOSPHATES (mmol/L) | ||
| Baseline | 1.0 ± 0.2 | 1.1 ± 0.2 |
| Day 105 | 1.0 ± 0.2 | 1.1 ± 0.2 |
| Change (Day 105—Baseline) * | 0.0 ± 0.1 | 0.0 ± 0.2 |
| ALKALINE PHOSPHATASE (IU/L) | ||
| Baseline | 57.0 ± 17.5 | 58.7 ± 16.2 |
| Day 105 | 57.6 ± 17.7 | 58.4 ± 16.9 |
| Change (Day 105—Baseline) * | 0.6 ± 7.6 | −0.3 ± 5.0 |
| CORRECTED CALCIUM (mmol/L) | ||
| Baseline | 2.2 ± 0.1 | 2.2 ± 0.1 |
| Day 105 | 2.2 ± 0.1 | 2.2 ± 0.1 |
| Change (Day 105—Baseline) * | −0.0 ± 0.1 | −0.0 ± 0.1 |
| PTH (ng/L) | ||
| Baseline | 18.2 ± 6.0 | 22.3 ± 10.7 |
| Day 105 | 16.5 ± 6.1 | 20.0 ± 9.0 |
| Change (Day 105—Baseline) * | −1.6 ± 4.8 | −2.3 ± 9.1 |
| FGF23 (pg/mL) | ||
| Baseline | 51.9 ± 16.4 | 57.3 ± 16.3 |
| Day 105 | 63.0 ± 18.8 | 63.6 ± 14.3 |
| Change (Day 105—Baseline) * | 11.1 ± 14.8 | 6.3 ± 15.9 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Niet, S.; Coffiner, M.; Da Silva, S.; Jandrain, B.; Souberbielle, J.-C.; Cavalier, E. A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation. Nutrients 2018, 10, 659. https://doi.org/10.3390/nu10060659
De Niet S, Coffiner M, Da Silva S, Jandrain B, Souberbielle J-C, Cavalier E. A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation. Nutrients. 2018; 10(6):659. https://doi.org/10.3390/nu10060659
Chicago/Turabian StyleDe Niet, Sophie, Monte Coffiner, Stéphanie Da Silva, Bernard Jandrain, Jean-Claude Souberbielle, and Etienne Cavalier. 2018. "A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation" Nutrients 10, no. 6: 659. https://doi.org/10.3390/nu10060659
APA StyleDe Niet, S., Coffiner, M., Da Silva, S., Jandrain, B., Souberbielle, J.-C., & Cavalier, E. (2018). A Randomized Study to Compare a Monthly to a Daily Administration of Vitamin D3 Supplementation. Nutrients, 10(6), 659. https://doi.org/10.3390/nu10060659