Factors Influencing Children’s Eating Behaviours

 ,
, 
 and
and 
Abstract
:1. Introduction
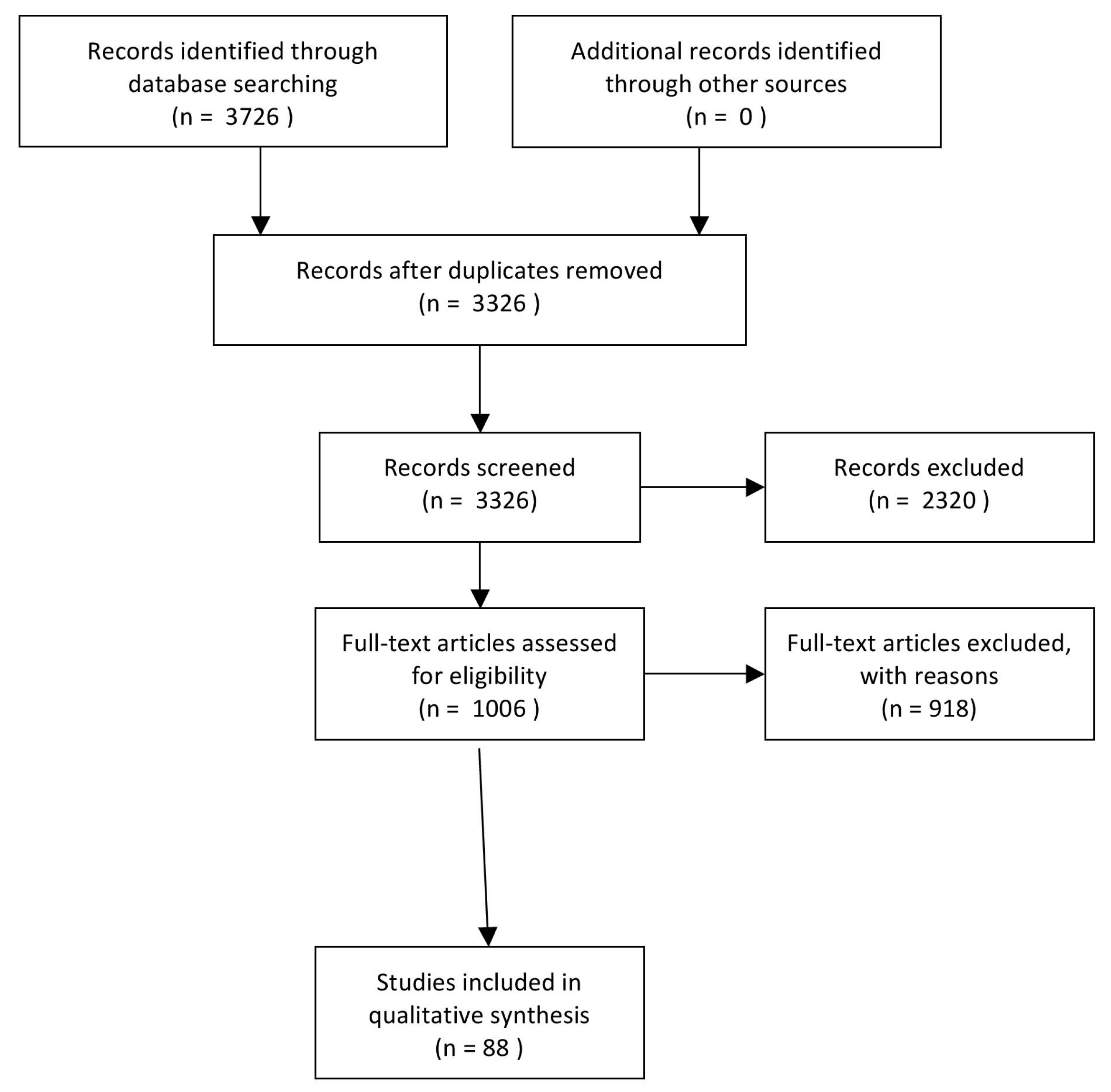
2. Methods—Literature Search Strategy
3. Family Environment
4. General Parental Influences
5. Maternal Influences
6. Paternal Influences
7. Family Meals
8. Education and Socioeconomic Status
9. Child Eating Behaviour
10. Food Preferences
11. Early Feeding Practice
12. Obesogenic Environment
13. Media Influences
14. Strategies to Improve Children’s Eating Behaviours
15. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jew, S.; Antoine, J.M.; Bourlioux, P.; Milner, J.; Tapsell, L.C.; Yang, Y.; Jones, P.J. Nutrient essentiality revisited. J. Funct. Foods 2015, 14, 203–209. [Google Scholar] [CrossRef]
- Bowen, K.J.; Sullivan, V.K.; Kris-Etherton, P.M.; Petersen, K.S. Nutrition and Cardiovascular Disease-an Update. Curr. Atheroscler. Rep. 2018, 20, 8. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.K.; Worobey, J. Early influences on the development of food preferences. Curr. Biol. 2013, 23, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.G.; Worsley, A. Why don’t they like that? And can I do anything about it? The nature and correlates of parents’ attributions and self-efficacy beliefs about preschool children’s food preferences. Appetite 2013, 66, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Cuellar, J.; Jones, D.J.; Sterrett, E. Examining Parenting in the Neighbourhood Context: A Review. J. Child Fam. Stud. 2015, 24, 195–219. [Google Scholar] [CrossRef] [PubMed]
- Montaño, Z.; Smith, J.D.; Dishion, T.J.; Shaw, D.S.; Wilson, M.N. Longitudinal relations between observed parenting behaviors and dietary quality of meals from ages 2 to 5. Appetite 2015, 87, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Finnane, J.M.; Jansen, E.; Mallan, K.M.; Daniels, L.A. Mealtime structure and responsive feeding practices are associated with less food fussiness and more food enjoyment in children. J. Nutr. Educ. Behav. 2017, 49, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, 2006–2011. [Google Scholar] [CrossRef] [PubMed]
- De Cosmi, V.; Scaglioni, S.; Agostoni, C. Early taste experience and later food choices. Nutrients. 2017, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- Niermann, C.Y.; Kremers, S.P.; Renner, B.; Woll, A. Family health climate and adolescents’ physical activity and healthy eating: A cross-sectional study with mother-father-adolescent triads. PLoS ONE 2015, 10, e0143599. [Google Scholar] [CrossRef] [PubMed]
- Vandeweghe, L.; Moens, E.; Braet, C.; Van Lippevelde, W.; Vervoort, L.; Verbeken, S. Perceived effective and feasible strategies to promote healthy eating in young children: Focus groups with parents, family child care providers and daycare assistants. BMC Public Health 2016, 16, 1045. [Google Scholar] [CrossRef] [PubMed]
- Niermann, C.; Krapf, F.; Renner, B.; Reiner, M.; Woll, A. Family health climate scale (FHC-scale): Development and validation. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Zarychta, K.; Mullan, B.; Luszczynska, A. It doesn't matter what they say, it matters how they behave: Parental influences and changes in body mass among overweight and obeseadolescents. Appetite 2016, 96, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Baumrind, D. The development of instrumental competence through socialization. In Minnesota Symposia on Child Psychology; Pick, A.D., Ed.; University of Minnesota Press: Minneapolis, MN, USA, 1973; Volume 7, pp. 3–46. [Google Scholar]
- Maccoby, E.; Martin, J. Socialization in the Context of the Family: Parent–child Interaction. In Handbook of Child Psychology: Socialization, Personality and Social Development; Hetherington, E., Ed.; Wiley: New York, NY, USA, 1983; pp. 1–101. [Google Scholar]
- Pearson, N.; Atkin, A.J.; Biddle, S.J.; Gorely, T.; Edwardson, C. Parenting styles, family structure and adolescent dietary behaviour. Public Health Nutr. 2010, 13, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Kremers, S.P.; Brug, J.; de Vries, H.; Engels, R.C. Parenting style and adolescent fruit consumption. Appetite 2003, 41, 43–50. [Google Scholar] [CrossRef]
- Rhee, K.E.; Lumeng, J.C.; Appugliese, D.P.; Kaciroti, N.; Bradley, R.H. Parenting styles and overweight status in first grade. Pediatrics 2006, 117, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Russel, C.G.; Worsley, A.; Campbell, K.J. Strategies used by parents to influence their children’s food preferences. Appetite 2015, 90, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Rollins, B.Y.; Loken, E.; Savage, J.S.; Birch, L.L. Maternal controlling feeding practices and girls’ inhibitory control interact to predict changes in BMI and eating in the absence of hunger from 5 to 7 y. Am. J. Clin. Nutr. 2014, 99, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Rollins, B.Y.; Savage, J.S.; Fisher, J.O.; Birch, L.L. Alternatives to restrictive feeding practices to promote self-regulation in childhood: A developmental perspective. Pediatr. Obes. 2016, 11, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, R.L.; Mobley, A.R. Parenting styles, feeding styles, and their influence on child obesogenic behaviours and body weight. A review. Appetite 2013, 71, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.L.; Goodell, L.S.; Williams, K.; Power, T.G.; Hughes, S.O. Getting my child to eat the right amount. Mothers’ considerations when deciding how much food to offer their child at a meal. Appetite 2015, 88, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Bouhlal, S.; McBride, C.M.; Ward, D.S.; Perskya, S. Drivers of overweight mothers’ food choice behaviours depend on child gender. Appetite 2015, 84, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Bergmeier, H.; Skouteris, H.; Hetherington, M. Systematic research review of observational approaches used to evaluate mother-child mealtime interactions during preschool years. Am. J. Clin. Nutr. 2015, 101, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Palfreyman, Z.; Haycraft, E.; Meyer, C. Parental modelling of eating behaviours: Observational validation of the Parental Modelling of Eating Behaviours scale (PARM). Appetite 2015, 86, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pesh, M.H.; Appugliese, D.P.; Kaciroti, N.; Rosenblum, K.L.; Miller, A.L.; Lumeng, J.C. Maternal encouragement and discouragement: Differences by food type and child weight status. Appetite 2016, 101, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Mosli, R.H.; Miller, A.L.; Peterson, K.E.; Lumeng, J.C. Sibling feeding behaviour: Mothers as role models during mealtimes. Appetite 2015, 96, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Thullen, M.; Majee, W.; Davis, A.N. Co-parenting and feeding in early childhood: Reflections of parent dyads on how they manage the developmental stages of feeding over the first three years. Appetite 2016, 1, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Khandpur, N.; Charles, J.; Blaine, R.E.; Blake, C.; Davison, K. Diversity in fathers’ food parenting practices: A qualitative exploration within a heterogeneous sample. Appetite 2016, 101, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, A.D.; Chu, L.; Franke, T.; Kuo, A.A. Father involvement in feeding interactions with their young children. Am. J. Health Behav. 2016, 40, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, R.L.; Adamsons, K.; Foster, J.S.; Mobley, A.R. Association of fathers’ feeding practices and feeding style on preschool age children’s diet quality, eating behavior and body mass index. Appetite 2015, 89, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Le Heuzey, M.F.; Turberg-Romain, C. Nutri-Bébé Survey 2013: Behaviour of mothers and young children during feeding. Arch. Pediatr. 2015, 22, 20–29. [Google Scholar]
- Fayet-Moore, F.; Kim, J.; Sritharan, N.; Petocz, P. Impact of breakfast skipping and breakfast choice on the nutrient intake and body mass index of Australian children. Nutrients 2016, 8, 487. [Google Scholar] [CrossRef] [PubMed]
- Fink, S.K.; Racine, E.F.; Mueffelmann, R.E.; Petocz, P. Family meals and diet quality among children and adolescents in North Carolina. J. Nutr. Educ. Behav. 2014, 46, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Jaworowska, A.; Blackham, T.; Davies, I.G.; Stevenson, L. Nutritional challenges and health implications of takeaway and fast food. Nutr. Rev. 2013, 71, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Suglia, S.F.; Shelton, R.C.; Hsiao, A.; Wang, Y.C.; Rundle, A.; Link, B.G. Why the Neighborhood Social Environment is Critical in Obesity Prevention. J. Urban Health 2016, 93, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Schrempft, S.; van Jaarsveld, C.H.M.; Fisher, A.; Fildes, A.; Wardle, J. Maternal characteristics associated with the obesogenic quality of the home environment in early childhood. Appetite 2016, 107, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Griffiths, P.; Biddle, S.J.H.; Johnston, J.P.; McGeorge, S.; Haycraft, E. Clustering and correlates of screen-time and eating behaviours among young adolescents. BMC Public Health 2017, 17, 533. [Google Scholar] [CrossRef] [PubMed]
- Khalsa, A.S.; Kharofa, R.; Ollberding, N.J.; Bishop, L.; Copeland, K.A. Attainment of ‘5-2-1-0’ obesity recommendations in preschool-aged children. Prev. Med. Rep. 2017, 8, 79–87. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, A.; Kubena, K.; Tolle, G.; Dean, W.; Kim, M.J.; Jan, J.S.; Anding, J. Determinants of children’s use of and time spent in fast-food and full service restaurants. J. Nutr. Educ. Behav. 2011, 43, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, L.M.; Haynie, D.L.; Liu, D.; Chaurasia, A.; Gee, B.; Li, K.; Iannotti, R.J.; Simons-Morton, B. Trajectories of eating behaviors in a nationally representative cohort of U.S. adolescents during the transition to young adulthood. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.E.; Norris, M.L.; Obeid, N.; Fu, M.; Weinstangel, H.; Sampson, M. Systematic review of the effects of family meal frequency on psychosocial outcomes in youth. Can. Fam. Physician 2015, 61, 96–106. [Google Scholar]
- Fulkerson, J.A.; Loth, K.; Bruening, M.; Berge, J.; Eisenberg, M.E.; Neumark-Sztainer, D. Time 2 tlk 2nite: Use of electronic media by adolescents during family meals and associations with demographic characteristics, family characteristics, and foods served. J. Acad. Nutr. Diet. 2014, 114, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.N.; Banda, J.A.; Hale, L.; Lu, A.S.; Fleming-Milici, F.; Calvert, S.L.; Wartella, E. Screen Media Exposure and Obesity in Children and Adolescents. Pediatrics 2017, 140, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Lanfer, A.; Gwozdz, W.; Olafsdottir, S.; Eiben, G.; Moreno, L.A.; Santaliestra-Pasías, A.M.; Kovács, E.; Barba, G.; Loit, H.M.; et al. Television habits in relation to overweight, diet and taste preferences in European children: The IDEFICS study. Eur. J. Epidemiol. 2012, 27, 705–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, E.; Edmunds, L.; Dennison, B. Positive effects of family dinner are undone by television viewing. J. Am. Diet. Assoc. 2007, 107, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Pyper, E.; Harrington D Manson, H. The impact of different types of parental support behaviours on child physical activity, healthy eating, and screen time: A cross-sectional study. BMC Public Health 2016, 16, 568. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, L.; Ek, A.; Nyman, J.; Marcus, C.; Ulijaszek, S.; Nowicka, P. Low granparental social support combined with low parental socioeconomic status is closely associated with obesity in preschool-aged children: A pilot study. Pediatr. Obes. 2016, 11, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Van Ansem, W.J.C.; Schrijvers, C.T.; Rodenburg, G.; van de Mheen, D. Maternal educational level and children's healthy eating behaviour: Role of the home food environment (cross-sectional results from the INPACT study). Int. J. Behav. Nutr. Phys. Act. 2014, 11, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, X.; Kong, K.L.; Eiden, R.D.; Sharma, N.N.; Xie, C. Sociodemographic differences and infant dietary patterns. Pediatrics 2014, 134, 1387–1398. [Google Scholar] [CrossRef] [PubMed]
- Non, A.L.; Román, J.C.; Gross, C.L.; Gilman, S.E.; Loucks, E.B.; Buka, S.L.; Kubzansky, L.D. Early childhood social disadvantage is associated with poor health behaviours in adulthood. Ann. Hum. Biol. 2016, 4, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Park, S.M.; Oh, K.W. The impact of nutritional policy on socioeconomic disparity in the unhealthy food intake among Korean adolescents. Appetite 2013, 71, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Tao, S.; Yu, L.; Gao, W.; Xue, W. Food preferences, personality and parental rearing styles: Analysis of factors influencing health of left-behind children. Qual. Life Res. 2016, 25, 2921–2929. [Google Scholar] [CrossRef] [PubMed]
- Emmett, P.M.; R Jones, L.R. Diet, growth, and obesity development throughout childhood in the Avon Longitudinal Study of Parents and Children. Nutr. Rev. 2015, 73, 175–206. [Google Scholar] [CrossRef] [PubMed]
- Fildes, A.; van Jaarsveld, C.H.M.; Llewellyn, C.; Wardle, J.; Fisher, A. Parental control over feeding in infancy. Influence of infant weight, appetite and feeding method. Appetite. 2015, 1, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrow, C.V.; Haycraft, E.; Blissett, J.M. Teaching our children when to eat: How parental feeding practices inform the development of emotional eating: A longitudinal experimental design. Am. J. Clin. Nutr. 2015, 101, 908–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derks, I.P.; Tiemeier, H.; Sijbrands, E.J.; Nicholson, J.M.; Voortman, T.; Verhulst, F.C.; Jaddoe, V.W.; Jansen, P.W. Testing the direction of effects between child body composition and restrictive feeding practices: Results from a population-based cohort. Am. J. Clin. Nutr. 2017, 106, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Cooke, L.; Fildes, A. The impact of flavour exposure in utero and during milk feeding on food acceptance at weaning and beyond. Appetite 2011, 57, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F. Intense sweeteners, appetite for the sweet taste, and relationship to weight management. Curr. Obes. Rep. 2015, 4, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Hong, G.; Matsuyam, Y. Association of oral fat sensitivity with body mass index, taste preference, and eating habits in healthy Japanese young adults. Tohoku J. Exp. Med. 2016, 238, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Hetherington, M.M.; Schwartz, C.; Madrelle, J.; Croden, F.; Nekitsing, C.; Vereijken, C.M.J.L.; Weenen, H. A step-by-step introduction to vegetables at the beginning of complementary feeding. The effects of early and repeated exposure. Appetite 2015, 84, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Gahagan, S. The development of eating behavior-biology and context. J. Dev. Behav. Pediatr. 2012, 33, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Harris, G.; Mason, S. Are There Sensitive Periods for Food Acceptance in Infancy? Curr. Nutr. Rep. 2017, 6, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Cole, N.C.; An, R.; Lee, S.Y.; Donovan, S.M. Correlates of picky eating and food neophobia in young children: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 516–532. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. The role of food experiences during early childhood in food pleasure learning. Appetite 2016, 104, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Moschonis, G.; Oliveira, A.; de Lauzon-Guillain, B.; Manios, Y.; Xepapadaki, P.; Lopes, C.; Moreira, P.; Charles, M.A.; Emmett, P. The influence of early feeding practices on healthy diet variety score among pre-school children in four European birth cohorts. Public Health Nutr. 2015, 18, 1774–1784. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Hirota, Y. Feeding practices in early life and later intake of fruit and vegetables among Japanese toddlers: The Osaka Maternal and Child Health Study. Public Health Nutr. 2015, 3, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.K. Does Breastfeeding Shape Food Preferences? Links to Obesity. Ann. Nutr. Metab. 2017, 3, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Morison, B.J.; Taylor, R.W.; Haszard, J.J.; Schramm, C.J.; Erickson, L.W.; Fangupo, L.J.; Fleming, E.A.; Luciano, A.; Heath, A.M. How different are baby-led weaning and conventional complementary feeding? A cross-sectional study of infants aged 6–8 months. BMJ Open 2016, 6, e010665. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Lee, M. Maternal control of child feeding during the weaning period: Differences between mothers following a baby-led or standard weaning approach. Matern. Child Health J. 2011, 15, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.; Heath, A.L.; Williams, S.M.; Cameron, S.L.; Fleming, E.A.; Taylor, B.J.; Wheeler, B.J.; Gibson, R.S.; Taylor, R.W. Baby-Led Introduction to SolidS (BLISS) study: A randomised controlled trial of a baby-led approach to complementary feeding. BMC Pediatr. 2015, 15, 179. [Google Scholar] [CrossRef] [PubMed]
- Maslin, K.; Dean, T.; Arshad, S.H.; Venter, C. Fussy eating and feeding difficulties in infants and toddlers consuming a cows' milk exclusion diet. Pediatr. Allergy Immunol. 2015, 26, 503–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonntag, D.; Schneider, S.; Mdege, N.; Ali, S.; Schmidt, B. Beyond Food Promotion: A Systematic Review on the Influence of the Food Industry on Obesity-Related Dietary Behaviour among Children. Nutrients 2015, 7, 8565–8576. [Google Scholar] [CrossRef] [PubMed]
- Oldham-Cooper, R.E.; Wilkinson, L.L.; Hardman, C.A.; Rogers, P.J.; Brunstrom, J.M. Presenting a food in multiple smaller units increases expected satiety. Appetite 2017, 118, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Crino, M.; Herrera, A.M.M.; Ananthapavan, J.; Wu, J.H.Y.; Neal, B.; Lee, Y.Y.; Zheng, M.; Lal, A.; Sacks, G. Modelled Cost-Effectiveness of a Package Size Cap and a Kilojoule Reduction Intervention to Reduce Energy Intake from Sugar-Sweetened Beverages in Australia. Nutrients 2017, 9, 983. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal feeding practices predict weight gain and obesogenic eating behaviours in young children: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2013, 18, 10–24. [Google Scholar]
- Savage, J.S.; Birch, L.L.; Marini, M.; Anzman-Frasca, S. Paul IM Effect of the INSIGHT Responsive Parenting Intervention on Rapid Infant Weight Gain and Overweight Status at Age 1 Year: A Randomized Clinical Trial. JAMA Pediatr. 2016, 170, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Dalton, M.A.; Longacre, M.R.; Drake, K.M.; Cleveland, L.P.; Harris, J.L.; Hendricks, K.; Titus, L.J. Child-targeted fast-food television advertising exposure is linked with fast-food intake among pre-school children. Public Health Nutr. 2017, 20, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; French, S. Food Advertising and Marketing Directed at Children and Adolescents in the US. Int. J. Behav. Nutr. Phys. Act. 2004, 1, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovács, E.; Hunsberger, M.; Reisch, L.; Gwozdz, W.; Eiben, G.; De Bourdeaudhuij, I.; Russo, P.; Veidebaum, T.; Hadjigeorgiou, C.; Sieri, S.; et al. Adherence to combined lifestyle factors and their contribution to obesity in the IDEFICS study. Obes. Rev. 2015, 16, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Inhulsen, M.M.; Mérelle, S.Y.; Renders, C.M. Parental feeding styles, young children’s fruit, vegetable, water and sugar-sweetened beverage consumption, and the moderating role of maternal education and ethnic background. Public Health Nutr. 2017, 20, 2124–2133. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Bennett, C.; Fogel, A.; Harris, G.; Higgs, S. Parental modelling and prompting effects on acceptance of a novel fruit in 2-4-year-old children are dependent on children's food responsiveness. Br. J. Nutr. 2016, 115, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Van Ansem, W.J.; Schrijvers, C.T.; Rodenburg, G.; van de Mheen, D. Children’s snack consumption: Role of parents, peers and child snack-purchasing behaviour. Results from the INPACT study. Eur. J. Public Health 2015, 25, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Majee, W.; Thullen, M.J.; Davis, A.N.; Sethi, T.K. Influences on Infant Feeding: Perceptions of Mother-Father Parent Dyads. MCN Am. J. Matern. Child Nurs. 2017, 42, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Stifter, C.A.; Anzman-Frasca, S.; Birch, L.L.; Voegtline, K. Parent use of food to soothe infant/toddler distress and child weight status. An exploratory study. Appetite 2011, 57, 693–699. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Strategy | Practices |
|---|---|
| Covert control |
|
| Avoid the use of food rewards |
|
| Promoting self-regulation |
|
| Authoritative parenting style |
|
| Family meals |
|
| Parent’s focused intervention |
|
| Family environment |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. https://doi.org/10.3390/nu10060706
Scaglioni S, De Cosmi V, Ciappolino V, Parazzini F, Brambilla P, Agostoni C. Factors Influencing Children’s Eating Behaviours. Nutrients. 2018; 10(6):706. https://doi.org/10.3390/nu10060706
Chicago/Turabian StyleScaglioni, Silvia, Valentina De Cosmi, Valentina Ciappolino, Fabio Parazzini, Paolo Brambilla, and Carlo Agostoni. 2018. "Factors Influencing Children’s Eating Behaviours" Nutrients 10, no. 6: 706. https://doi.org/10.3390/nu10060706
APA StyleScaglioni, S., De Cosmi, V., Ciappolino, V., Parazzini, F., Brambilla, P., & Agostoni, C. (2018). Factors Influencing Children’s Eating Behaviours. Nutrients, 10(6), 706. https://doi.org/10.3390/nu10060706