Serum Magnesium after Kidney Transplantation: A Systematic Review

 ,
,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
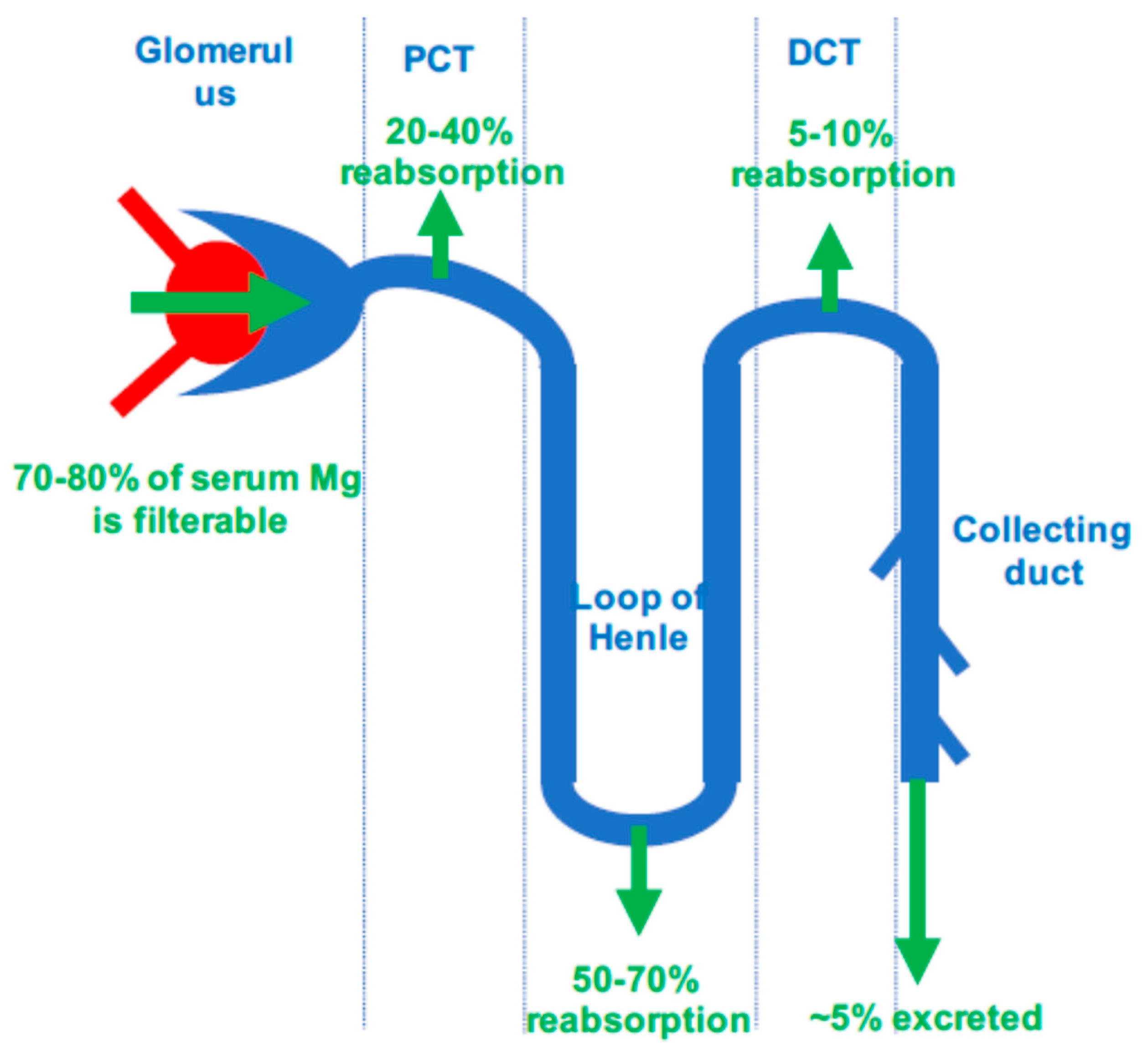
1. Magnesium: Physiology
2. Clinical Signs and Etiologies of Hypomagnesemia
3. Magnesium Status in CKD Patients
4. Magnesium and Cardiovascular Risk in CKD Patients
5. Magnesium Status after Kidney Transplantation and Relation with Graft Function
6. Serum Magnesium and New-Onset Diabetes Mellitus after Transplantation
6.1. Serum Magnesium and Diabetes Mellitus in the General Population
6.2. Serum Magnesium and New-Onset Diabetes Mellitus after Transplantation
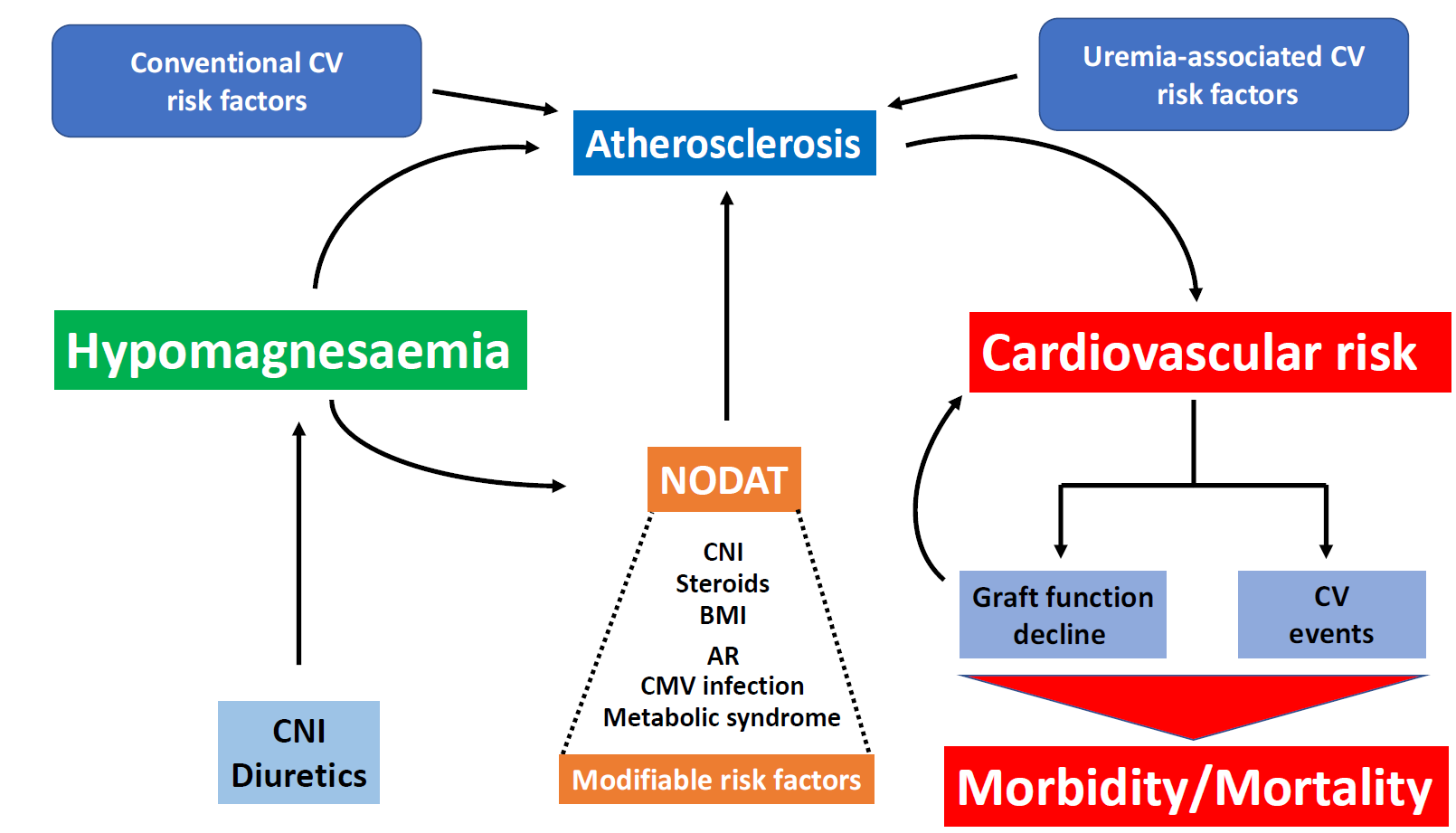
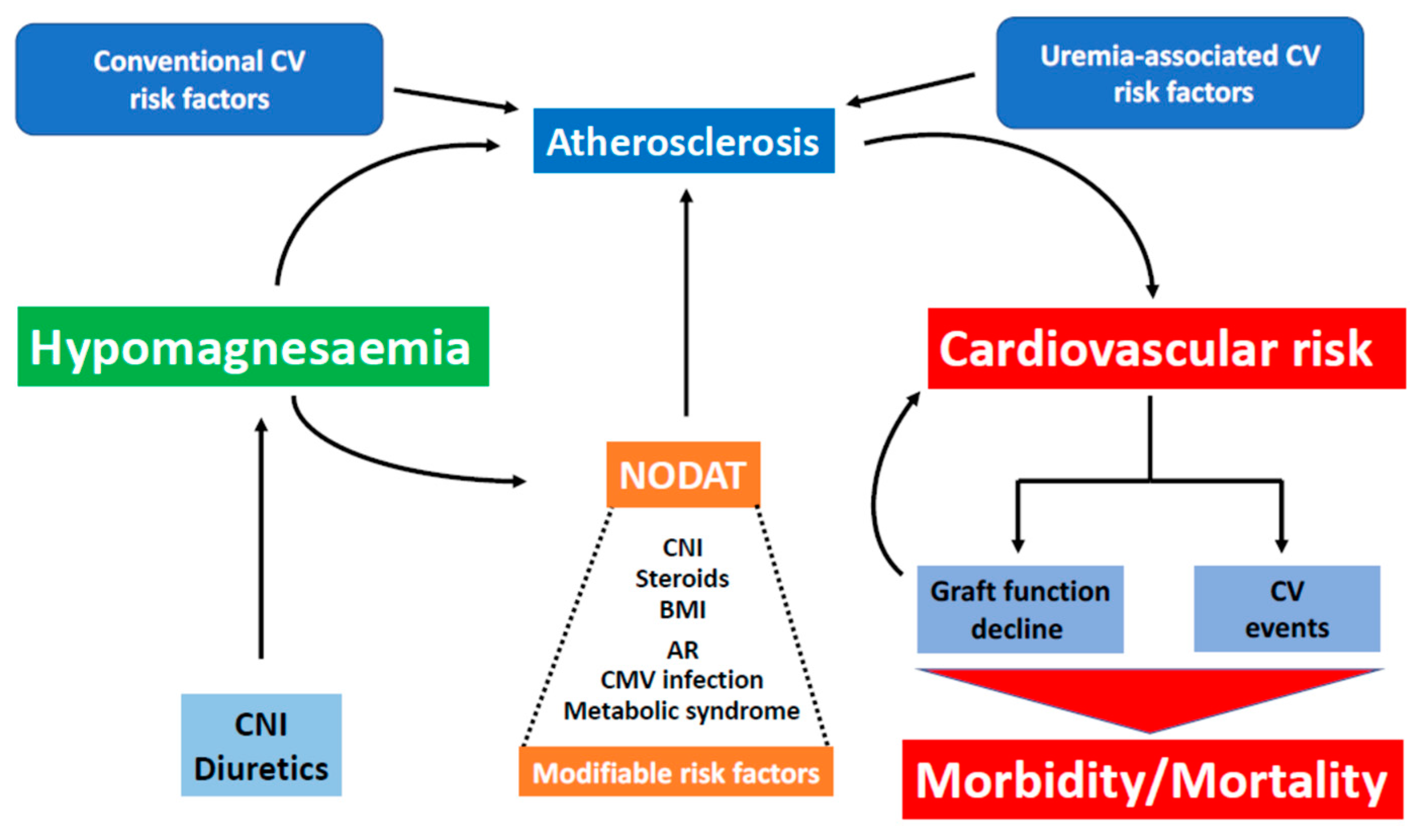
7. Magnesium Status and Cardiovascular Risk before and after Kidney Transplantation
8. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| AUC | Area under the curve |
| CKD | Chronic kidney disease |
| CNI | Calcineurin inhibitors |
| ESRD | End-stage renal disease |
| HD | Hemodialysis |
| HOMA_IR | Homeostasis model assessment-estimated insulin-resistance index |
| Mg | Magnesium |
| PD | Peritoneal dialysis |
| PTDM | Post-transplant diabetes mellitus |
| TRPM6 | Transient Receptor Potential Melastatin 6 |
References
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5, i3–i14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisinger, J.R.; Bellorín-Font, E. Magnesium and phosphorus. Lancet 1998, 352, 391–396. [Google Scholar] [CrossRef]
- Fawcett, W.J.; Haxby, E.J.; Male, D.A. Magnesium: Physiology and pharmacology. Br. J. Anaesth. 1999, 83, 302–320. [Google Scholar] [CrossRef] [PubMed]
- Tietz, N.W.; Rinker, A.D.; Morrison, S.R. When is a serum iron really a serum iron? The status of serum iron measurements. Clin. Chem. 1994, 40, 546–551. [Google Scholar] [PubMed]
- Kanbay, M.; Goldsmith, D.; Uyar, M.E.; Turgut, F.; Covic, A. Magnesium in chronic kidney disease: Challenges and opportunities. Blood Purif. 2010, 29, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.; Rodríguez, M.; Messa, P. Magnesium in chronic kidney disease Stages 3 and 4 and in dialysis patients. Clin. Kidney J. 2012, 5, i39–i51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whang, R.; Ryder, K.W. Frequency of hypomagnesemia and hypermagnesemia. Requested vs. routine. JAMA 1990, 263, 3063–3064. [Google Scholar] [CrossRef] [PubMed]
- Nichols, C.G.; Ho, K.; Hebert, S. Mg(2+)-dependent inward rectification of ROMK1 potassium channels expressed in Xenopus oocytes. J. Physiol. (Lond.) 1994, 476, 399–409. [Google Scholar] [CrossRef]
- Agus, Z.S.; Kelepouris, E.; Dukes, I.; Morad, M. Cytosolic magnesium modulates calcium channel activity in mammalian ventricular cells. Am. J. Physiol. 1989, 256, C452–C455. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, N.; Mori, M. An analysis of hypermagnesemia and hypomagnesemia. Jpn. J. Med. 1990, 29, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Kafka, H.; Langevin, L.; Armstrong, P.W. Serum magnesium and potassium in acute myocardial infarction. Influence on ventricular arrhythmias. Arch. Intern. Med. 1987, 147, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Aglio, L.S.; Stanford, G.G.; Maddi, R.; Boyd, J.L.; Nussbaum, S.; Chernow, B. Hypomagnesemia is common following cardiac surgery. J. Cardiothorac. Vasc. Anesth. 1991, 5, 201–208. [Google Scholar] [CrossRef]
- England, M.R.; Gordon, G.; Salem, M.; Chernow, B. Magnesium administration and dysrhythmias after cardiac surgery. A placebo-controlled, double-blind, randomized trial. JAMA 1992, 268, 2395–2402. [Google Scholar] [CrossRef] [PubMed]
- Agus, Z.S. Hypomagnesemia. J. Am. Soc. Nephrol. 1999, 10, 1616–1622. [Google Scholar] [PubMed]
- Truttmann, A.C.; Faraone, R.; Von Vigier, R.O.; Nuoffer, J.M.; Pfister, R.; Bianchetti, M.G. Maintenance hemodialysis and circulating ionized magnesium. Nephron 2002, 92, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Blumenkrantz, M.J.; Kopple, J.D.; Moran, J.K.; Coburn, J.W. Metabolic balance studies and dietary protein requirements in patients undergoing continuous ambulatory peritoneal dialysis. Kidney Int. 1982, 21, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum magnesium concentration is a significant predictor of mortality in maintenance hemodialysis patients. Magnes. Res. 2007, 20, 237–244. [Google Scholar] [PubMed]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Meema, H.E.; Oreopoulos, D.G.; Rapoport, A. Serum magnesium level and arterial calcification in end-stage renal disease. Kidney Int. 1987, 32, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E.; Okuno, S.; Kitatani, K.; Tsuchida, T.; Yamakawa, T.; Shioi, A.; Inaba, M.; Nishizawa, Y. Significant association between the presence of peripheral vascular calcification and lower serum magnesium in hemodialysis patients. Clin. Nephrol. 2007, 68, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Turgut, F.; Kanbay, M.; Metin, M.R.; Uz, E.; Akcay, A.; Covic, A. Magnesium supplementation helps to improve carotid intima media thickness in patients on hemodialysis. Int. Urol. Nephrol. 2008, 40, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Schmaderer, C.; Braunisch, M.C.; Suttmann, Y.; Lorenz, G.; Pham, D.; Haller, B.; Angermann, S.; Matschkal, J.; Renders, L.; Baumann, M.; et al. Reduced Mortality in Maintenance Haemodialysis Patients on High versus Low Dialysate Magnesium: A Pilot Study. Nutrients 2017, 9, 926. [Google Scholar] [CrossRef] [PubMed]
- Margreiter, R. European Tacrolimus vs. Ciclosporin Microemulsion Renal Transplantation Study Group Efficacy and safety of tacrolimus compared with ciclosporin microemulsion in renal transplantation: A randomised multicentre study. Lancet 2002, 359, 741–746. [Google Scholar] [CrossRef]
- Ledeganck, K.J.; De Winter, B.Y.; Van den Driessche, A.; Jürgens, A.; Bosmans, J.-L.; Couttenye, M.M.; Verpooten, G.A. Magnesium loss in cyclosporine-treated patients is related to renal epidermal growth factor downregulation. Nephrol. Dial. Transplant. 2014, 29, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Nijenhuis, T.; Hoenderop, J.G.J.; Bindels, R.J.M. Downregulation of Ca(2+) and Mg(2+) transport proteins in the kidney explains tacrolimus (FK506)-induced hypercalciuria and hypomagnesemia. J. Am. Soc. Nephrol. 2004, 15, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, C.A.; de Bragança, A.C.; Shimizu, M.H.M.; Sanches, T.R.; Fortes, M.A.Z.; Giorgi, R.R.; Andrade, L.; Seguro, A.C. Rosiglitazone prevents sirolimus-induced hypomagnesemia, hypokalemia, and downregulation of NKCC2 protein expression. Am. J. Physiol. Renal Physiol. 2009, 297, F916–F922. [Google Scholar] [PubMed]
- Andoh, T.F.; Burdmann, E.A.; Fransechini, N.; Houghton, D.C.; Bennett, W.M. Comparison of acute rapamycin nephrotoxicity with cyclosporine and FK506. Kidney Int. 1996, 50, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W. Hypomagnesaemia in kidney transplantation. Transplant. Rev. 2015, 29, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.H.; Vaziri, N.D.; Martin, D.C.; Choi, S.; Alikhani, S. Hypomagnesemia and renal magnesium wasting in renal transplant recipients receiving cyclosporine. Am. J. Med. 1987, 83, 693–699. [Google Scholar] [CrossRef]
- Stevens, R.B.; Lane, J.T.; Boerner, B.P.; Miles, C.D.; Rigley, T.H.; Sandoz, J.P.; Nielsen, K.J.; Skorupa, J.Y.; Skorupa, A.J.; Kaplan, B.; Wrenshall, L.E. Single-dose rATG induction at renal transplantation: Superior renal function and glucoregulation with less hypomagnesemia: RATGS minimizes glucose dysregulation. Clin. Transplant. 2012, 26, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Van de Cauter, J.; Sennesael, J.; Haentjens, P. Long-term evolution of the mineral metabolism after renal transplantation: A prospective, single-center cohort study. Transplant. Proc. 2011, 43, 3470–3475. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, N.; Santana, A.; Guerra, J.; Neves, M.; Nascimento, C.; Gonçalves, J.; da Costa, A.G. Serum Magnesium and Related Factors in Long-Term Renal Transplant Recipients: An Observational Study. Transplant. Proc. 2017, 49, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Holzmacher, R.; Kendziorski, C.; Michael Hofman, R.; Jaffery, J.; Becker, B.; Djamali, A. Low serum magnesium is associated with decreased graft survival in patients with chronic cyclosporin nephrotoxicity. Nephrol. Dial. Transplant. 2005, 20, 1456–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, K.; Nakatani, T.; Asai, T.; Yamanaka, S.; Tamada, S.; Tashiro, K.; Kim, S.; Okamura, M.; Iwao, H. Role of hypomagnesemia in chronic cyclosporine nephropathy. Transplantation 2002, 73, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Zhou, J.; Chen, B.C.; Zhang, X.; Zhou, H.M.; Du, D.F.; Chang, S.; Chen, Z.K. Magnesium supplementation prevents chronic cyclosporine nephrotoxicity via adjusting nitric oxide synthase activity. Transplant. Proc. 2005, 37, 1892–1895. [Google Scholar] [CrossRef] [PubMed]
- Asai, T.; Nakatani, T.; Yamanaka, S.; Tamada, S.; Kishimoto, T.; Tashiro, K.; Nakao, T.; Okamura, M.; Kim, S.; Iwao, H.; et al. Magnesium supplementation prevents experimental chronic cyclosporine a nephrotoxicity via renin-angiotensin system independent mechanism. Transplantation 2002, 74, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Asai, T.; Nakatani, T.; Tamada, S.; Kuwabara, N.; Yamanaka, S.; Tashiro, K.; Nakao, T.; Komiya, T.; Okamura, M.; Kim, S.; et al. Activation of transcription factors AP-1 and NF-kappaB in chronic cyclosporine A nephrotoxicity: Role in beneficial effects of magnesium supplementation. Transplantation 2003, 75, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.-C.T.; Pham, P.-M.T.; Pham, S.V.; Miller, J.M.; Pham, P.-T.T. Hypomagnesemia in Patients with Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiger, H.; Wanner, C. Magnesium in disease. Clin. Kidney J. 2012, 5, i25–i38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, P.C.T.; Pham, P.M.T.; Pham, P.a.T.; Pham, S.V.; Pham, H.V.; Miller, J.M.; Yanagawa, N.; Pham, P.T.T. Lower serum magnesium levels are associated with more rapid decline of renal function in patients with diabetes mellitus type 2. Clin. Nephrol. 2005, 63, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Ridaura, R.; Willett, W.C.; Rimm, E.B.; Liu, S.; Stampfer, M.J.; Manson, J.E.; Hu, F.B. Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care 2004, 27, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Manson, J.E.; Buring, J.E.; Liu, S. Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 2004, 27, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose-response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Kao, W.H.; Folsom, A.R.; Nieto, F.J.; Mo, J.P.; Watson, R.L.; Brancati, F.L. Serum and dietary magnesium and the risk for type 2 diabetes mellitus: The Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 1999, 159, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Nadler, J.L.; Buchanan, T.; Natarajan, R.; Antonipillai, I.; Bergman, R.; Rude, R. Magnesium deficiency produces insulin resistance and increased thromboxane synthesis. Hypertension 1993, 21, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W.; Vanholder, R. Hypomagnesaemia, the kidney and the vessels. Nephrol. Dial. Transplant. 2012, 27, 4003–4010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Moran, M.; Guerrero-Romero, F. Oral Magnesium Supplementation Improves Insulin Sensitivity and Metabolic Control in Type 2 Diabetic Subjects: A randomized double-blind controlled trial. Diabetes Care 2003, 26, 1147–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.; Matas, A.J. Diabetes mellitus after kidney transplantation in the United States. Am. J. Transplant. 2003, 3, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Augusto, J.-F.; Subra, J.-F.; Duveau, A.; Rakotonjanahary, J.; Dussaussoy, C.; Picquet, J.; Croue, A.; Villemain, F.; Onno, C.; Sayegh, J. Relation between Pretransplant Magnesemia and the Risk of New Onset Diabetes After Transplantation within the First Year of Kidney Transplantation. Transplantation 2014, 97, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.J.; Fourlanos, S.; Hjelmesaeth, J.; Colman, P.G.; Cohney, S.J. New-onset diabetes after kidney transplantation-changes and challenges. Am. J. Transplant. 2012, 12, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Mazali, F.C.; Lalli, C.A.; Alves-Filho, G.; Mazzali, M. Posttransplant diabetes mellitus: Incidence and risk factors. Transplant. Proc. 2008, 40, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Maes, B.D.; Kuypers, D.; Messiaen, T.; Evenepoel, P.; Mathieu, C.; Coosemans, W.; Pirenne, J.; Vanrenterghem, Y.F.C. Posttransplantation Diabetes Mellitus in Fk-506-Treated Renal Transplant Recipients: Analysis of Incidence and Risk Factors. Transplantation 2001, 72, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Van Biesen, W.; Verbeke, F.; De Bacquer, D.; Peeters, P.; Vanholder, R. Posttransplantation hypomagnesemia and its relation with immunosuppression as predictors of new-onset diabetes after transplantation. Am. J. Transplant. 2009, 9, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Famure, O.; Li, Y.; Kim, S.J. Hypomagnesemia and the Risk of New-Onset Diabetes Mellitus after Kidney Transplantation. J. Am. Soc. Nephrol. 2016, 27, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Hayes, W.; Boyle, S.; Carroll, A.; Bockenhauer, D.; Marks, S.D. Hypomagnesemia and increased risk of new-onset diabetes mellitus after transplantation in pediatric renal transplant recipients. Pediatr. Nephrol. 2017, 32, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Chanchlani, R.; Joseph Kim, S.; Kim, E.D.; Banh, T.; Borges, K.; Vasilevska-Ristovska, J.; Li, Y.; Ng, V.; Dipchand, A.I.; Solomon, M.; et al. Incidence of hyperglycemia and diabetes and association with electrolyte abnormalities in pediatric solid organ transplant recipients. Nephrol. Dial. Transplant. 2017, 32, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Osorio, J.M.; Bravo, J.; Pérez, A.; Ferreyra, C.; Osuna, A. Magnesemia in Renal Transplant Recipients: Relation With Immunosuppression and Posttransplant Diabetes. Transplant. Proc. 2010, 42, 2910–2913. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.; Rodrigo, E.; Piñera, C.; Robledo, C.; Palomar, R.; Gómez-Alamillo, C.; González-Cotorruelo, J.; Arias, M. Elevated serum gamma-glutamyltransferase and hypomagnesemia are not related with new-onset diabetes after transplantation. Transplant. Proc. 2010, 42, 2914–2916. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Desideri, F.; Geerts, A.; Van Vlierberghe, H.; Berrevoet, F.; Rogiers, X.; Troisi, R.; de Hemptinne, B.; Vanholder, R.; Colle, I. Hypomagnesemia and the risk of new-onset diabetes after liver transplantation. Liver Transplant. 2010, 16, 1278–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Laecke, S.; Nagler, E.V.; Taes, Y.; Van Biesen, W.; Peeters, P.; Vanholder, R. The effect of magnesium supplements on early post-transplantation glucose metabolism: A randomized controlled trial. Transpl. Int. 2014, 27, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Van Laecke, S.; Caluwe, R.; Huybrechts, I.; Nagler, E.V.; Vanholder, R.; Peeters, P.; Van Vlem, B.; Van Biesen, W. Effect of Magnesium Supplements on Insulin Secretion After Kidney Transplantation: A Randomized Controlled Trial. Ann. Transplant. 2017, 22, 524–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Fructuoso, A.I.; Santín Cantero, J.M.; Pérez Flores, I.; Valero San Cecilio, R.; Calvo Romero, N.; Vilalta Casas, R. Changes in magnesium and potassium homeostasis after conversion from a calcineurin inhibitor regimen to an mTOR inhibitor-based regimen. Transplant. Proc. 2010, 42, 3047–3049. [Google Scholar] [CrossRef] [PubMed]
- Murakami, N.; Riella, L.V.; Funakoshi, T. Risk of metabolic complications in kidney transplantation after conversion to mTOR inhibitor: A systematic review and meta-analysis. Am. J. Transplant. 2014, 14, 2317–2327. [Google Scholar] [CrossRef] [PubMed]
- Grimbert, P.; Thaunat, O. mTOR inhibitors and risk of chronic antibody-mediated rejection after kidney transplantation: Where are we now? Transpl. Int. 2017, 30, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Kumar, P.; Reisin, E.; Ramcharan, T. Kidney Transplantation: The Evolving Challenges. Am. J. Med. Sci. 2004, 328, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.M.; Malpuech-Brugère, C.; Zimowska, W.; Rayssiguier, Y.; Mazur, A. Low magnesium promotes endothelial cell dysfunction: Implications for atherosclerosis, inflammation and thrombosis. Biochim. Biophys. Acta 2004, 1689, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Paravicini, T.M.; Yogi, A.; Mazur, A.; Touyz, R.M. Dysregulation of Vascular TRPM7 and Annexin-1 is Associated with Endothelial Dysfunction in Inherited Hypomagnesemia. Hypertension 2009, 53, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Liao, F.; Folsom, A.R.; Brancati, F.L. Is low magnesium concentration a risk factor for coronary heart disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 1998, 136, 480–490. [Google Scholar] [CrossRef]
- Hashimoto, T.; Hara, A.; Ohkubo, T.; Kikuya, M.; Shintani, Y.; Metoki, H.; Inoue, R.; Asayama, K.; Kanno, A.; Nakashita, M.; et al. Serum Magnesium, Ambulatory Blood Pressure, and Carotid Artery Alteration: The Ohasama Study. Am. J. Hypertens. 2010, 23, 1292–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisters, K.; Gremmler, B.; Hausberg, M. Magnesium and arterial stiffness. Hypertension 2006, 47, e3. [Google Scholar] [CrossRef] [PubMed]
- Shechter, M.; Sharir, M.; Labrador, M.J.; Forrester, J.; Silver, B.; Bairey Merz, C.N. Oral magnesium therapy improves endothelial function in patients with coronary artery disease. Circulation 2000, 102, 2353–2358. [Google Scholar] [CrossRef] [PubMed]
- Massy, Z.A.; Drüeke, T.B. Magnesium and outcomes in patients with chronic kidney disease: Focus on vascular calcification, atherosclerosis and survival. Clin. Kidney J. 2012, 5, i52–i61. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Steiner, R.W. A trial of oral magnesium supplementation in renal transplant recipients receiving cyclosporine. Transplant. Proc. 1998, 30, 4317–4319. [Google Scholar] [CrossRef]
- Van Laecke, S.; Maréchal, C.; Verbeke, F.; Peeters, P.; Van Biesen, W.; Devuyst, O.; Jadoul, M.; Vanholder, R. The relation between hypomagnesaemia and vascular stiffness in renal transplant recipients. Nephrol. Dial. Transplant. 2011, 26, 2362–2369. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garnier, A.-S.; Duveau, A.; Planchais, M.; Subra, J.-F.; Sayegh, J.; Augusto, J.-F. Serum Magnesium after Kidney Transplantation: A Systematic Review. Nutrients 2018, 10, 729. https://doi.org/10.3390/nu10060729
Garnier A-S, Duveau A, Planchais M, Subra J-F, Sayegh J, Augusto J-F. Serum Magnesium after Kidney Transplantation: A Systematic Review. Nutrients. 2018; 10(6):729. https://doi.org/10.3390/nu10060729
Chicago/Turabian StyleGarnier, Anne-Sophie, Agnès Duveau, Martin Planchais, Jean-François Subra, Johnny Sayegh, and Jean-François Augusto. 2018. "Serum Magnesium after Kidney Transplantation: A Systematic Review" Nutrients 10, no. 6: 729. https://doi.org/10.3390/nu10060729
APA StyleGarnier, A.-S., Duveau, A., Planchais, M., Subra, J.-F., Sayegh, J., & Augusto, J.-F. (2018). Serum Magnesium after Kidney Transplantation: A Systematic Review. Nutrients, 10(6), 729. https://doi.org/10.3390/nu10060729