Intakes, Adequacy, and Biomarker Status of Iron, Folate, and Vitamin B12 in Māori and Non-Māori Octogenarians: Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ)


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
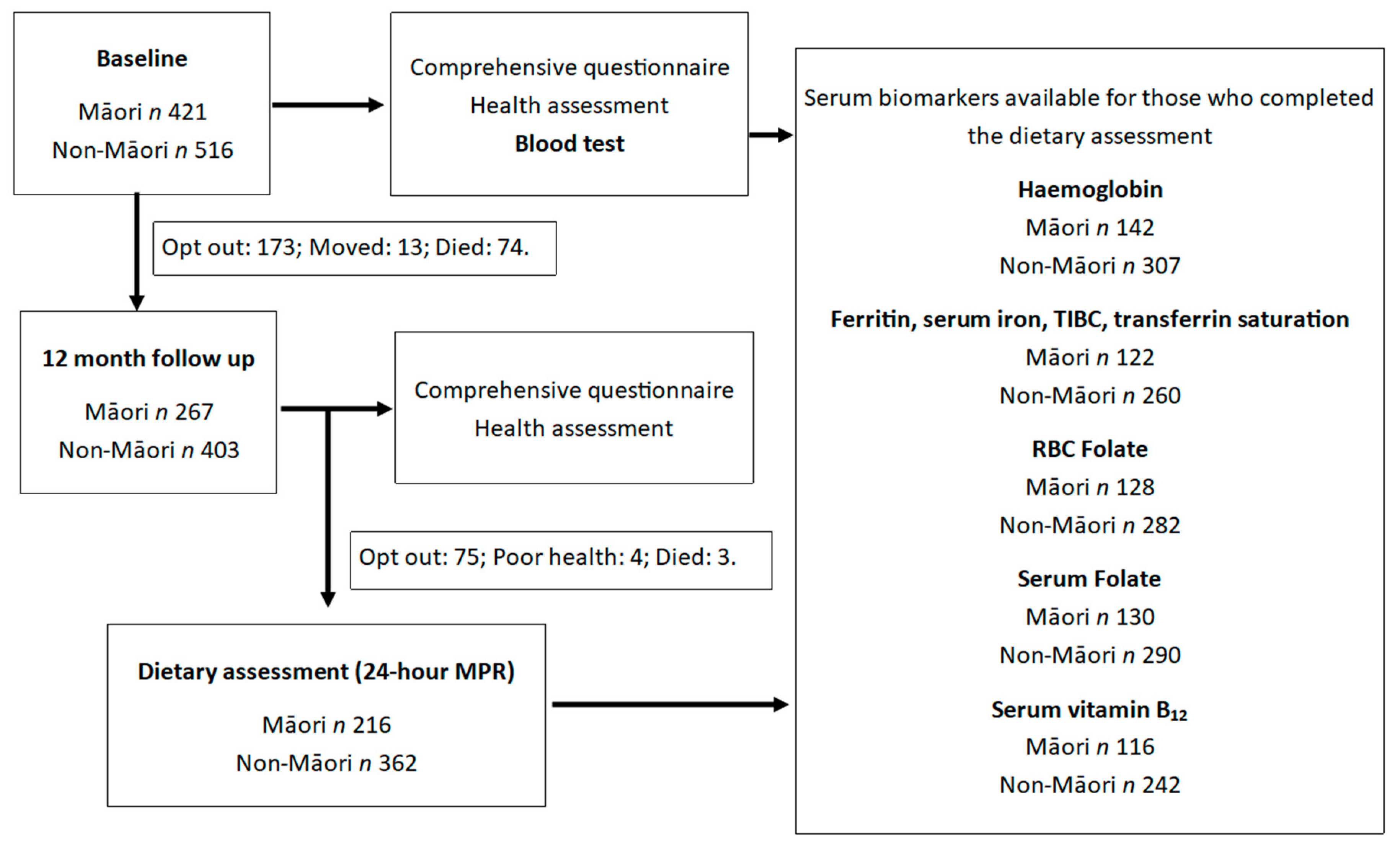
2.1. Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ)
2.2. Dietary Assessment: 24-Hour Multiple Pass Recall (MPR)
2.3. Nutritional Biomarkers
2.4. Statistical Analysis
3. Results
3.1. Māori Participants
3.2. Non-Māori Participants
3.3. Dietary Intakes and Adequacy of Iron, Folate and Vitamin B12
3.4. Biomarker Status
3.5. Top Food Contributors for Iron, Folate and Vitamin B12 Intake
3.6. Association between Dietary Intake and Biomarker Status
3.7. Risk of Iron, Folate or Vitamin B12 Deficiency by Quartiles of Dietary Intake
4. Discussion
4.1. Iron
4.2. Folate
4.3. Vitamin B12
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Statistics New Zealand, National Population Projections 2016(Base)–2068–Media Release. Available online: http://archive.stats.govt.nz/browse_for_stats/population/estimates_and_projections/NationalPopulationProjections_MR2016.aspx (accessed on 14 August 2018).
- Ministry of Health. Tatau Kahukura: Māori Health Chart Book, 3rd ed.; Ministry of Health: Wellington, New Zealand, 2015.
- McElnay, C.; Marshall, B.; O’Sullivan, J.; Jones, L.; Ashworth, T.; Hicks, K.; Forrest, R.H. Nutritional risk amongst community-living Māori and non-Māori older people in Hawke’s Bay. J. Prim. Healthc. 2012, 4, 299–305. [Google Scholar]
- Wham, C.; Maxted, E.; Teh, R.; Kerse, N. Factors associated with nutrition risk in older Māori: A cross sectional study. N. Z. Med. J. 2015, 128, 1420. [Google Scholar]
- Frangos, E.; Trombetti, A.; Graf, C.E.; Lachat, V.; Samaras, N.; Vischer, U.M.; Zekry, D.; Rizzoli, R.; Herrmann, F.R. Malnutrition in Very Old Hospitalized Patients: A New Etiologic Factor of Anemia? J. Nutr. Health Aging 2016, 20, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004, 104, 2263–2268. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, B.B.; Cankurtaran, M.; Haznedaroglu, I.C.; Halil, M.; Ulger, Z.; Altun, B.; Ariogul, S. Iron deficiency can cause cognitive impairment in geriatric patients. J. Nutr. Health Aging 2012, 16, 220–224. [Google Scholar] [CrossRef]
- Mooijaart, S.P.; Gussekloo, G.; Frolich, M.; Jolles, J.; Stott, D.J.; Westendorp, R.G.J.; de Craen, A.J.M. Homocysteine, vitamin B-12, and folic acid and the risk of cognitive decline in old age: The Leiden 85-Plus Study. Am. J. Clin. Nutr. 2005, 82, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Toxqui, L.; Vaquero, M. Chronic iron deficiency as an emerging risk factor for osteoporosis: A hypothesis. Nutrients 2015, 7, 2324–2344. [Google Scholar] [CrossRef] [PubMed]
- Marian, M.; Sacks, G. Invited Review: Micronutrients and older adults. Nutr. Clin. Pract. 2009, 24, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, T.; Yalcin, A.; Atmis, V.; Cengiz, O.K.; Aras, S.; Varlı, M.; Atli, T. The prevalence of anemia, iron, vitamin B12, and folic acid deficiencies in community dwelling elderly in Ankara, Turkey. Arch. Gerontol. Geriatr. 2015, 60, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Pfisterer, K.J.; Sharratt, M.T.; Heckman, G.G.; Keller, H.H. Vitamin B12 status in older adults living in ontario long-term care homes: Prevalence and incidence of deficiency with supplementation as a protective factor. Appl. Physiol. Nutr. Metab. 2016, 41, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, D. Iron deficiency anaemia in older people: Investigation, management and treatment. Age Ageing 2002, 31, 87–91. [Google Scholar] [CrossRef] [PubMed]
- University of Otago; Ministry of Health. A Focus on Nutrition: Key findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011.
- Den Elzen, W.P.J.; de Craen, A.J.M.; Wiegerinck, E.T.; Westendorp, R.G.J.; Swinkels, D.W.; Gussekloo, J. Plasma hepcidin levels and anemia in old age. The Leiden 85-Plus Study. Haematologica 2012, 98, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, T.J.; Venn, B.J.; Skeaff, C.M.; Williams, S.M. Serum vitamin B12 concentrations and atrophic gastritis in older new zealanders. Eur. J. Clin. Nutr. 2004, 59, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, N.; Mathers, J.C.; Adamson, A.J.; Martin-Ruiz, C.; Seal, C.J.; Jagger, C.; Hill, T.R. Intakes of Folate and Vitamin B12 and Biomarkers of Status in the Very Old: The Newcastle 85+ Study. Nutrients 2016, 8, 604. [Google Scholar] [CrossRef] [PubMed]
- Kassarjian, Z.; Russell, R.M. Hypochlorhydria: A factor in nutrition. Annu. Rev. Nutr. 1989, 9, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.M. Factors in Aging that Effect the Bioavailability of Nutrients. J. Nutr. 2001, 131, 1359–1361. [Google Scholar] [CrossRef] [PubMed]
- Stover, P.J. Vitamin B12 and older adults. Curr. Opin Clin. Nutr. Metab. Care 2010, 13, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Causes of vitamin B12 and folate deficiency. Food Nutr. Bull. 2008, 29, S20–S34. [Google Scholar] [CrossRef] [PubMed]
- Lombardi-Boccia, G.; Martinez-Dominguez, B.; Aguzzi, A. Total heme and non-heme iron in raw and cooked meats. J. Food Sci. 2002, 67, 1738–1741. [Google Scholar] [CrossRef]
- Pourkhalili, A.; Mirlohi, M.; Rahimi, E. Heme iron content in lamb meat is differentially altered upon boiling, grilling, or frying as assessed by four distinct analytical methods. Sci. World J. 2013, 2013, 374030. [Google Scholar] [CrossRef] [PubMed]
- Gille, D.; Schmid, A. Vitamin B12 in meat and dairy products. Nutr. Rev. 2015, 73, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Zinck, J.W.; de Groh, M.; MacFarlane, A.J. Genetic modifiers of folate, vitamin B-12, and homocysteine status in a cross-sectional study of the canadian population. Am. J. Clin. Nutr. 2015, 101, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Fairweather-Tait, S.J.; Teucher, B. Iron and calcium bioavailability of fortified foods and dietary supplements. Nutr. Rev. 2002, 60, 360–367. [Google Scholar] [CrossRef] [PubMed]
- López, M.A.A.; Martos, F.C. Iron availability: An updated review. Int. J. Food Sci. Nutr. 2004, 55, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Chernoff, R. Geriatric Nutrition; Jones & Bartlett Learning LLC.: Barlington, MA, USA, 2013. [Google Scholar]
- Ovesen, L.; Schroll, M.; Milman, N.; Pedersen, A.N. Iron status in 358 apparently healthy 80-year-old danish men and women: Relation to food composition and dietary and supplemental iron intake. Ann. Hematol. 2004, 83, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Chen, J. Association between dietary folate-rich food intake and folate status of elderly Taiwanese. Asia Pac. J. Clin. Nutr. 2005, 14, 244–249. [Google Scholar] [PubMed]
- Jackson, J.; Williams, R.; McEvoy, M.; MacDonald-Wicks, L.; Patterson, A. Is higher consumption of animal flesh foods associated with better iron status among adults in developed countries? A systematic review. Nutrients 2016, 8, 89. [Google Scholar] [CrossRef] [PubMed]
- Hayman, K.J.; Kerse, N.; Dyall, L.; Kepa, M.; Teh, R.; Wham, C.; Clair, V.W.-S.; Wiles, J.; Keeling, S.; Connolly, M.J.; et al. Life and living in advanced age: A cohort study in new zealand -te puāwaitanga o nga tapuwae kia ora tonu, lilacs nz: Study protocol. BMC Geriatr. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Dyall, L.; Kepa, M.; Hayman, K.; Teh, R.; Moyes, S.; Broad, J.B.; Kerse, N. Engagement and recruitment of māori and non-māori people of advanced age to LiLACS Nz. Aust. N. Z. J. Public Health 2013, 37, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Adamson, A.J. Nutrition in advanced age: Dietary assessment in the Newcastle 85+ study. Eur. J. Clin. Nutr. 2009, 63, 6–18. [Google Scholar] [CrossRef] [PubMed]
- Wham, C.; Maxted, E.; Dyall, L.; Teh, R.; Kerse, N. Korero Te Kai O Te Rangatira: Nutritional Wellbeing of Māori at the Pinnacle of Life. Nutr. Diet. 2012, 69, 213–216. [Google Scholar] [CrossRef]
- Hopkins, C.G. A Research Institute for New Zealand. Nature 1920, 104, 442. [Google Scholar]
- NHMRC. Nutrient Reference Values for Australia and New Zealand: Including Recommended Dietary Intakes; National Health and Medical Research Council: Canberra, ACT, Australia; Ministry of Health: Wellington, New Zealand, 2006.
- Wham, C.; Teh, R.; Moyes, S.A.; Rolleston, A.; Muru-Lanning, M.; Hayman, K.; Adamson, A.; Kerse, N. Macronutrient intake in advanced age: Te puāwaitanga o ngā tapuwae kia ora tonu, life and living in advanced age: A cohort study in new zealand (LiLACS Nz). Columbia J. Nutr. 2016, 116, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- WHO; CDC. Assessing the Iron Status of Populations; World Health Organisation & Centers for Disease Control and Prevention: Geneva, Switzerland, 2007. [Google Scholar]
- Mahan, W.L.K.; Escott-Stump, S. Krause’s Food, Nutrition & Diet Therapy, 9th ed.; W. B. Saunders Company: Philadelphia, PA, USA, 1996; 1194p. [Google Scholar]
- De Benoist, B. Conclusions of a who technical consultation on folate and vitamin B12 deficiencies. Food Nutr. Bull. 2008, 29, S238–S244. [Google Scholar] [CrossRef] [PubMed]
- University of Otago; Ministry of Health. Methodology Report for the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011.
- Looker, A.C. Prevalence of iron deficiency in the United States. JAMA 1997, 277, 973–976. [Google Scholar] [CrossRef] [PubMed]
- Babaei, M.; Shafiei, S.; Bijani, A.; Heidari, B.; Hosseyni, S.R.; Vakili Sadeghi, M. Ability of serum ferritin to diagnose iron deficiency anemia in an elderly cohort. Braz. J. Hematol. Hemother. 2017, 39, 223–228. [Google Scholar]
- Fairweather-Tait, S.J. Iron status in the elderly. Mech. Ageing Dev. 2014, 136–137, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.W.; Cho, W.R.; Park, K.H.; Choi, I.K.; Seo, J.H.; Kim, B.S.; Shin, S.W.; Kim, Y.H.; Kim, J.S.; Lee, J. The cutoff value of serum ferritin for the diagnosis of iron deficiency in community-residing older persons. Ann. Hematol. 2005, 84, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Doyle, W.; Crawley, H.; Robert, H.; Bates, C.J. Iron deficiency in older people: Interactions between food and nutrient intakes with biochemical measures of iron; further analysis of the national diet and nutrition survey of people aged 65 years and over. Eur. J. Clin. Nutr. 1999, 53, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Milman, N.; Ingerslev, J.; Graudal, N. Serum ferritin and iron status in a population of “healthy” 85-year-old individuals. Scan. J. Clin. Lab. Investig. 1990, 50, 77–83. [Google Scholar] [CrossRef]
- WHO. Iron Deficiency Anaemia: Assessment, Prevention and Control; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- Hurrell, R.; Egli, I. Iron bioavailability and dietary reference values. Am. J. Clin. Nutr. 2010, 91, 1461S–1467S. [Google Scholar] [CrossRef] [PubMed]
- Garry, P.J.; Hunt, W.C.; Baumgartner, R.N. Effects of iron intake on iron stores in elderly men and women: Longitudinal and cross-sectional results. J. Am. Coll. Nutr. 2000, 19, 262–269. [Google Scholar] [CrossRef] [PubMed]
- EFSA NDA Panel. Scientific opinion on dietary reference values for folate. EFSA J. 2015, 12, 3893. [Google Scholar]
- Green, R. Indicators for assessing folate and vitamin B-12 status and for monitoring the efficacy of intervention strategies. Am. J. Clin. Nutr. 2011, 94, 666S–672S. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, I.A.; van Dusseldorp, M.; West, C.E.; Steegers-Theunissen, R.P. Bioavailability and bioefficacy of folate and folic acid in man. Nutr. Res. Rev. 2001, 14, 267–294. [Google Scholar] [CrossRef] [PubMed]
- Holmes, B.; Roberts, C. The Influence of Social and Physical Factors and Out-of-Home Eating on Food Consumption and Nutrient Intake in the Materially Deprived Older UK Population; Kings College London: London, UK, 2009. [Google Scholar]
- Caudill, M.A. Folate bioavailability: Implications for establishing dietary recommendations and optimizing status. Am. J. Clin. Nutr. 2010, 91, 1455S–1460S. [Google Scholar] [CrossRef] [PubMed]
- Devalia, V.; Hamilton, M.S.; Molloy, A.M. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Columbia J. Haematol. 2014, 166, 496–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doets, E.L.; de Groot, L. Chapter 42—Vitamin B12 Requirements in Older Adults. In Molecular Basis of Nutrition and Aging; Mocchegiani, E., Ed.; Academic Press: San Diego, CA, USA, 2016; pp. 599–607. [Google Scholar]
- Allen, L.H. How common is vitamin B-12 deficiency? Am. J. Clin. Nutr. 2009, 89, 693S–696S. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, F.; Samman, S. Vitamin B12 in Health and Disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef] [PubMed]
- De Silva, N.; Davis, B. Iron, B12 and folate. Medicine 2013, 41, 204–207. [Google Scholar] [CrossRef]
- Wong, C. Vitamin B12 deficiency in the elderly: Is it worth screening? Kong Kong Méd. J. 2015, 21, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Nexo, E.; Hoffmann-Lucke, E. Holotranscobalamin, a marker of vitamin B-12 status: Analytical aspects and clinical utility. Am. J. Clin. Nutr. 2011, 94, 359S–365S. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzoglou, A.; Oulhaj, A.; Smith, A.D.; Nurk, E.; Drevon, C.A.; Ueland, P.M.; Vollset, S.E.; Tell, G.S.; Refsum, H. Determinants of plasma methylmalonic acid in a large population: Implications for assessment of vitamin B12 status. Clin. Chem. 2009, 55, 2198–2206. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.D. Metabolic vitamin B12 deficiency: A missed opportunity to prevent dementia and stroke. Nutr. Res. 2016, 36, 109–116. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Māori | Non-Māori | |||||
|---|---|---|---|---|---|---|---|
| Total | Men | Women | Total | Men | Women | ||
| Number of participants, n (%) * | 216 | 92 (43%) | 124 (57%) | 362 | 172 (48%) | 190 (52%) | |
| Age (years) 1 | 83 (81, 85) | 82 (81, 85) | 84 (81, 86) | 86 (85, 86) | 86 (85, 86) | 86 (85, 86) | |
| Medications used 2 | None | 36 (17%) | 15 (16%) | 21 (17%) | 14 (4%) | 9 (5%) | 5 (3%) |
| 1–3 | 35 (15%) | 14 (15%) | 21 (17%) | 53 (15%) | 29 (17%) | 24 (13%) | |
| 4–6 | 68 (31%) | 29 (32%) | 39 (31%) | 120 (33%) | 60 (35%) | 60 (32%) | |
| 7–9 | 44 (20%) | 21 (23%) | 23 (19%) | 97 (27%) | 40 (23%) | 57 (30%) | |
| 10+ | 33 (15%) | 13 (14%) | 20 (16%) | 78 (22%) | 34 (20%) | 44 (23%) | |
| Types of Medications used | Antacids | 3 (1%) | 3 (3%) | 0 | 3 (1%) | 1 (1%) | 2 (1%) |
| H2RAs | 0 | 0 | 0 | 4 (1%) | 1 (1%) | 3 (2%) | |
| PPIs | 61 (28%) | 29 (32%) | 32 (26%) | 118 (33%) | 50 (29%) | 68 (36%) | |
| NSAIDs | 18 (8%) | 6 (7%) | 11 (9%) | 69 (19%) | 26 (15%) | 43 (23%) | |
| Dietary supplements 3 | None | 161 (75%) | 72 (78%) | 89 (72%) | 217 (60%) | 120 (70%) | 97 (51%) |
| Supplements used | 55 (25%) | 20 (22%) | 35 (28%) | 145 (40%) | 52 (30%) | 93 (49%) | |
| Māori | p-Value ◊ | Non-Māori | p-Value ¥ | p-Value Ethnic * | |||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Men | Women | Total | Men | Women | ||||
| Energy Intake (MJ) 1 | 6.4 (5.2, 8.2) | 7.5 (6.1, 9.1) | 6.0 (4.8, 7.2) | <0.001 | 7.1 (5.8, 8.7) | 7.9 (6.7, 9.6) | 6.3 (5.3, 7.5) | <0.001 | <0.001 |
| Iron | |||||||||
| Intake (mg/day) 1 | 9.7 (7.1, 13.1) | 11.2 (7.8, 14.4) | 8.9 (6.7, 11.9) | - | 10.6 (8.1, 13.3) | 11.6 (9.9, 14.3) | 9.3 (7.1, 11.7) | - | - |
| Intake per 1 MJ (mg) | 1.47 | 1.43 | 1.54 | 0.376 | 1.44 | 1.44 | 1.42 | 0.692 | 0.391 |
| <EAR (n, %) a | 25 (12%) | 11 (12%) | 14 (11%) | - | 18 (5%) | 3 (2%) | 15 (8%) | - | - |
| Hemoglobin (g/L) 1 | 137 (128, 144) | 137 (126, 146) | 134 (127, 143) | 0.197 | 136 (126, 143) | 138 (127, 144) | 129 (123, 138) | <0.001 | 0.167 |
| Hb <125 g/L (men); or <118 g/L (women) | 15 (7%) | 10 (11%) | 5 (4%) | - | 45 (12%) | 28 (16%) | 17 (9%) | - | - |
| Ferritin 1 | 188 (94, 340) | 257 (127, 369) | 172 (84, 304) | 0.015 | 122 (77, 224) | 179 (97, 361) | 107 (71, 178) | <0.001 | 0.002 |
| <12 (µg/L) | 0 | 0 | 0 | 1 (1%) | 1 (1%) | 0 | |||
| Serum iron (µmol/L) 1 | 15 (11, 18) | 14 (11, 17) | 15 (12, 20) | 0.544 | 15 (12,18) | 18 (12, 19) | 15 (12,17) | 0.146 | 0.882 |
| <10 µmol/L | 8 (4%) | 3 (3%) | 5 (4%) | - | 18 (5%) | 8 (5%) | 10 (5%) | - | - |
| TIBC (µmol/L) 1 | 57 (52, 65) | 56 (51, 62) | 57 (52, 67) | 0.015 | 56 (50, 63) | 52 (48, 57) | 57 (53, 65) | <0.001 | 0.080 |
| >71 µmol/L | 10 (5%) | 2 (2%) | 8 (7%) | - | 9 (3%) | 5 (3%) | 4 (2%) | - | - |
| Tf-sat (%) 1 | 28 (21, 34) | 28 (22, 35) | 28 (21, 35) | 0.545 | 28 (22, 34) | 32 (24, 39) | 26 (22, 32) | 0.001 | 0.544 |
| <15% | 10 (5%) | 4 (4%) | 6 (5%) | - | 21 (6%) | 10 (6%) | 11 (6%) | - | - |
| Folate | |||||||||
| Intake (µg/d) 1 | 279 (191, 393) | 298 (205, 391) | 268 (186, 397) | - | 313 (224, 447) | 341 (253, 479) | 290 (202, 407) | - | - |
| Intake per 1 MJ (µg) | 42.15 | 36.78 | 44.37 | 0.019 | 44.31 | 42.22 | 45.61 | 0.304 | 0.417 |
| <EAR (n, %) b | 125 (58%) | 53 (58%) | 72 (58%) | - | 186 (51%) | 74 (43%) | 112 (59%) | - | - |
| Serum folate (nmol/L) 2 | 18 (16–20) | 18 (16–20) | 19 (17–21) | 0.110 | 19 (17–20) | 17 (14–20) | 19 (16–21) | 0.480 | 0.430 |
| <6.7 nmol/L | 0 | 0 | 0 | - | 6 (2%) | 3 (2%) | 3 (2%) | - | - |
| RBC folate (nmol/L) 2 | 338 (302–379) | 333 (298–372) | 338 (315–363) | 0.635 | 336 (317–357) | 322 (261–398) | 348 (303, 401) | 0.866 | 0.228 |
| <317 nmol/L | 58 (27%) | 22 (24%) | 26 (29%) | - | 111 (31%) | 54 (31%) | 57 (30%) | - | |
| Vitamin B12 | |||||||||
| Intake (µg/d) 1 | 3.0 (1.9, 4.4) | 3.4 (2.5, 5.1) | 2.7 (1.7, 3.9) | - | 3.03 (2.1, 4.2) | 3.6 (2.4, 4.8) | 2.6 (1.8, 3.6) | - | - |
| Intake per 1 MJ (µg) | 0.46 | 0.48 | 0.45 | 0.198 | 0.43 | 0.45 | 0.42 | 0.370 | 0.038 |
| <EAR (n, %) c | 55 (26%) | 12 (13%) | 43 (37%) | - | 78 (22%) | 21 (12%) | 57 (30%) | - | - |
| Serum B12 (pmol/L) 2 | 261 (227–299) | 212 (188–239) | 229 (209–251) | 0.359 | 222 (207–239) | 253 (196–363) | 265 (224–315) | 0.770 | 0.026 |
| <148 pmol/L | 15 (7%) | 6 (7%) | 9 (7%) | - | 34 (9%) | 19 (11%) | 15 (8%) | - | - |
| Māori | Non-Māori | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| Iron | Cereals (18%) | Cereals (17%) | Cereals (19%) | Cereals (15%) |
| Bread (12%) | Bread (15%) | Bread (14%) | Bread (15%) | |
| Beef and veal (8%) | Vegetables (8%) | Beef and veal (9%) | Vegetables (9%) | |
| Folate | Cereals (20%) | Cereals (18%) | Cereals (19%) | Vegetables (16%) |
| Vegetables (15%) | Bread (16%) | Bread (16%) | Bread (15%) | |
| Bread (14%) | Vegetables (16%) | Vegetables (14%) | Cereals (14%) | |
| Vitamin B12 | Milk (20%) | Milk (24%) | Milk (23%) | Milk (24%) |
| Beef and veal (17%) | Fish and seafood (16%) | Beef and veal (21%) | Beef and veal (16%) | |
| Fish and seafood (16%) | Beef and veal (15%) | Fish and seafood (12%) | Fish and seafood (9%) | |
| Māori | Non-Māori | |||||||
|---|---|---|---|---|---|---|---|---|
| Ron Intake (mg/day) | Model 1 (Unadjusted) | Model 2 (Adjusted) * | Model 1 (Unadjusted) | Model 2 (Adjusted) * | ||||
| (n = 8) | p | p | (n = 18) | p | p | |||
| <7.75 | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref.) | - |
| 7.75–10.42 | 0.43 (0.04, 4.39) | 0.478 | 0.41 (0.04, 4.34) | 0.458 | 0.63 (0.16, 2.45) | 0.500 | 0.82 (0.19, 3.60) | 0.789 |
| 10.43–13.27 | 0.75 (0.12, 4.80) | 0.769 | 0.59 (0.08, 4.58) | 0.617 | 0.29 (0.06, 1.58) | 0.153 | 0.49 (0.07, 3.32) | 0.465 |
| >13.27 | 1.11 (0.17, 7.20) | 0.912 | 0.76 (0.07, 8.41) | 0.820 | 1.17 (0.35, 3.90) | 0.802 | 2.33 (0.46, 11.9) | 0.311 |
| Folate Intake (µg/day) | Model 1 (Unadjusted) | Model 2 (Adjusted) ¥ | Model 1 (Unadjusted) | Model 2 (Adjusted) ¥ | ||||
| (n = 58) | p | p | (n = 111) | p | p | |||
| <215 | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref.) | - |
| 215–304 | 0.16 (0.06, 0.47) | 0.001 | 0.16 (0.05, 0.47) | 0.001 | 0.91 (0.45, 1.81) | 0.781 | 0.90 (0.44, 1.86) | 0.774 |
| 305–440 | 0.19 (0.06, 0.55) | 0.002 | 0.13 (0.04, 0.43) | 0.001 | 0.61 (0.31, 1.23) | 0.166 | 0.60 (0.27, 1.31) | 0.201 |
| >440 | 0.10 (0.03, 0.32) | <0.001 | 0.06 (0.01, 0.34) | 0.001 | 0.45 (0.22, 0.91) | 0.027 | 0.59 (0.20, 1.69) | 0.325 |
| Vitamin B12 Intake (µg/day) | Model 1 (Unadjusted) | Model 2 (Adjusted) ◊ | Model 1 (Unadjusted) | Model 2 (Adjusted) ◊ | ||||
| (n = 15) | p | p | (n = 34) | p | p | |||
| <2.07 | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref.) | - | 1.00 (ref) | - |
| 2.07–3.03 | 0.46 (0.08, 2.60) | 0.378 | 0.39 (0.07, 2.28) | 0.293 | 1.61 (0.56, 4.67) | 0.379 | 1.41 (0.47, 4.21) | 0.536 |
| 3.04–4.24 | 0.77 (0.18, 3.21) | 0.717 | 0.57 (0.12, 2.65) | 0.472 | 1.70 (0.58, 5.03) | 0.338 | 1.33 (0.41, 4.29) | 0.639 |
| >4.24 | 0.62 (0.15, 2.56) | 0.508 | 0.41 (0.08, 2.14) | 0.293 | 1.21 (0.38, 3.87) | 0.743 | 0.89 (0.24, 3.31) | 0.862 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillay, D.; Wham, C.; Moyes, S.; Muru-Lanning, M.; Teh, R.; Kerse, N. Intakes, Adequacy, and Biomarker Status of Iron, Folate, and Vitamin B12 in Māori and Non-Māori Octogenarians: Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Nutrients 2018, 10, 1090. https://doi.org/10.3390/nu10081090
Pillay D, Wham C, Moyes S, Muru-Lanning M, Teh R, Kerse N. Intakes, Adequacy, and Biomarker Status of Iron, Folate, and Vitamin B12 in Māori and Non-Māori Octogenarians: Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Nutrients. 2018; 10(8):1090. https://doi.org/10.3390/nu10081090
Chicago/Turabian StylePillay, Danika, Carol Wham, Simon Moyes, Marama Muru-Lanning, Ruth Teh, and Ngaire Kerse. 2018. "Intakes, Adequacy, and Biomarker Status of Iron, Folate, and Vitamin B12 in Māori and Non-Māori Octogenarians: Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ)" Nutrients 10, no. 8: 1090. https://doi.org/10.3390/nu10081090
APA StylePillay, D., Wham, C., Moyes, S., Muru-Lanning, M., Teh, R., & Kerse, N. (2018). Intakes, Adequacy, and Biomarker Status of Iron, Folate, and Vitamin B12 in Māori and Non-Māori Octogenarians: Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Nutrients, 10(8), 1090. https://doi.org/10.3390/nu10081090