Quality of Prenatal and Childhood Diet Predicts Neurodevelopmental Outcomes among Children in Mexico City

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Nutrition Measures
2.3. Neurodevelopmental Outcome Measures
2.4. Covariates
2.5. Statistical Methods
2.5.1. Nutrition Indices
2.5.2. Analytic Samples
3. Results
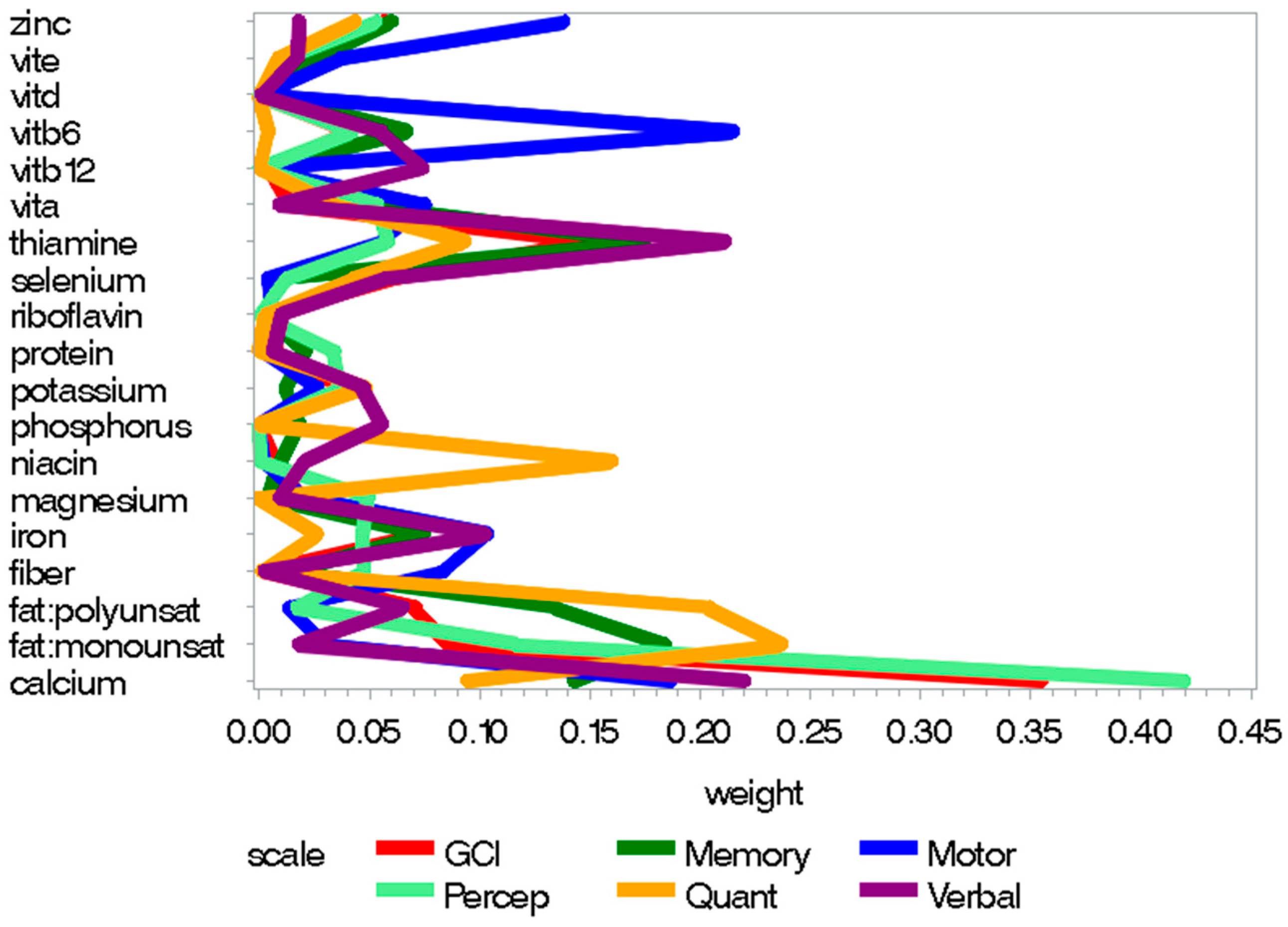
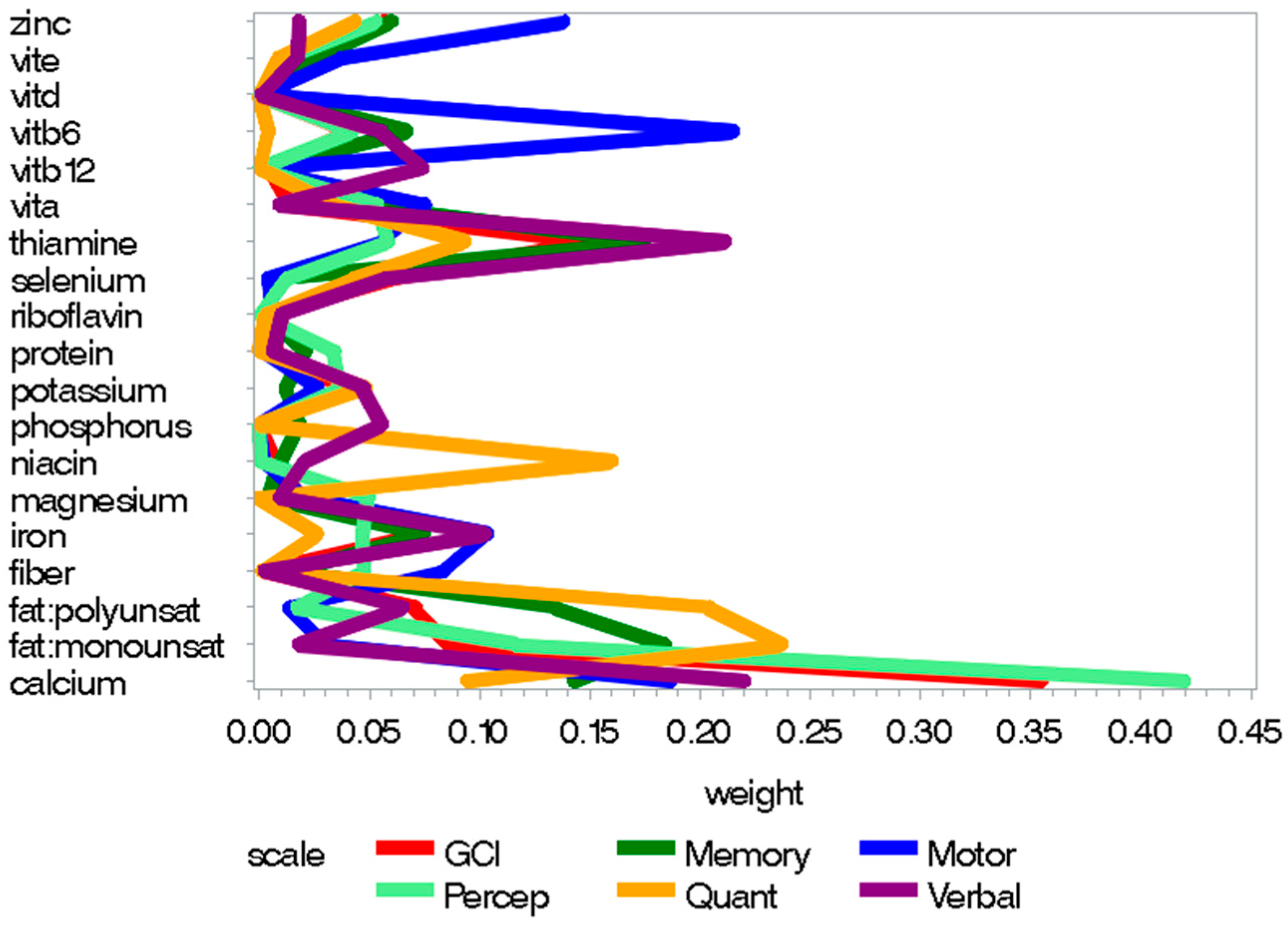
3.1. Prenatal Nutrition
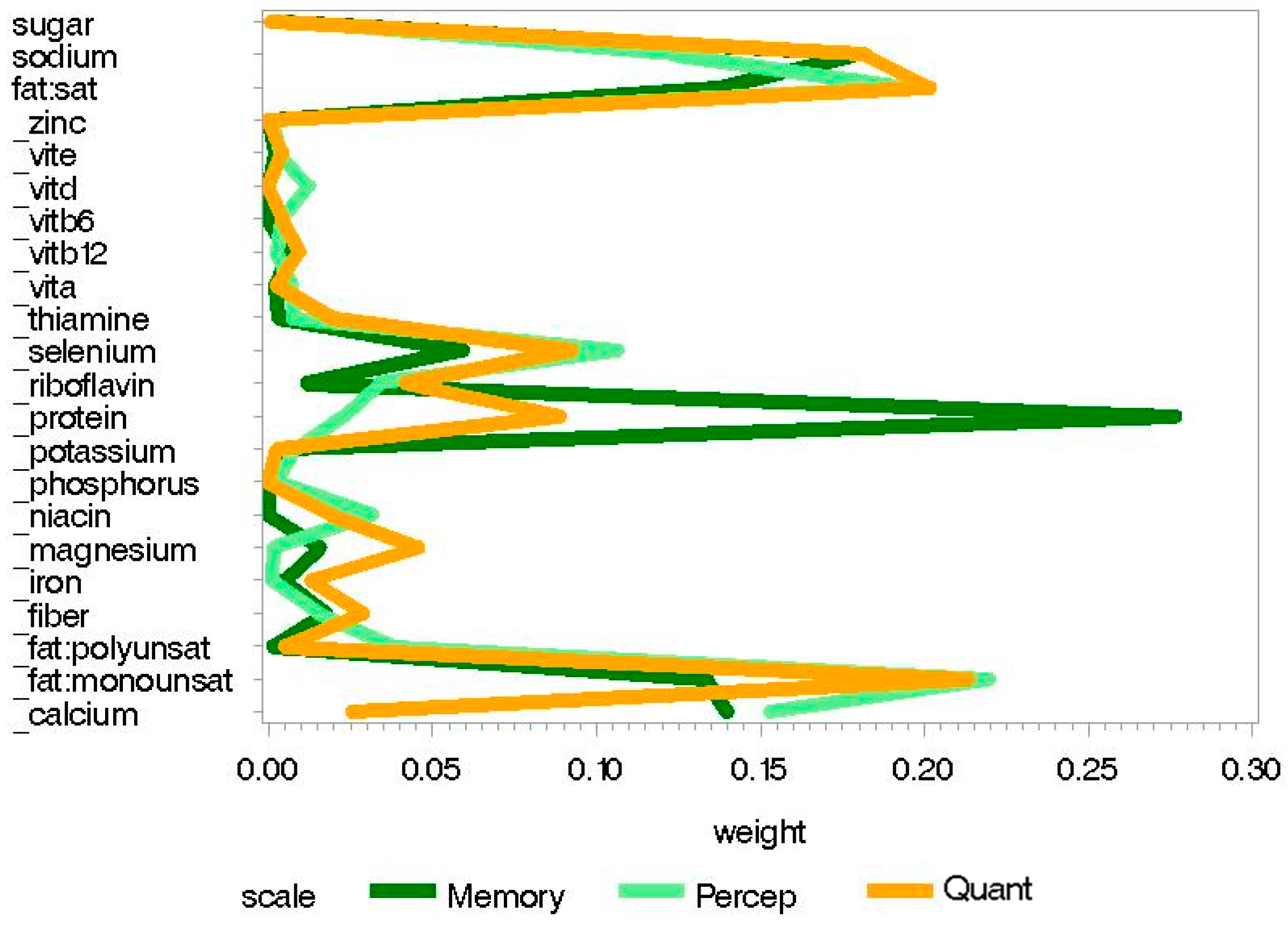
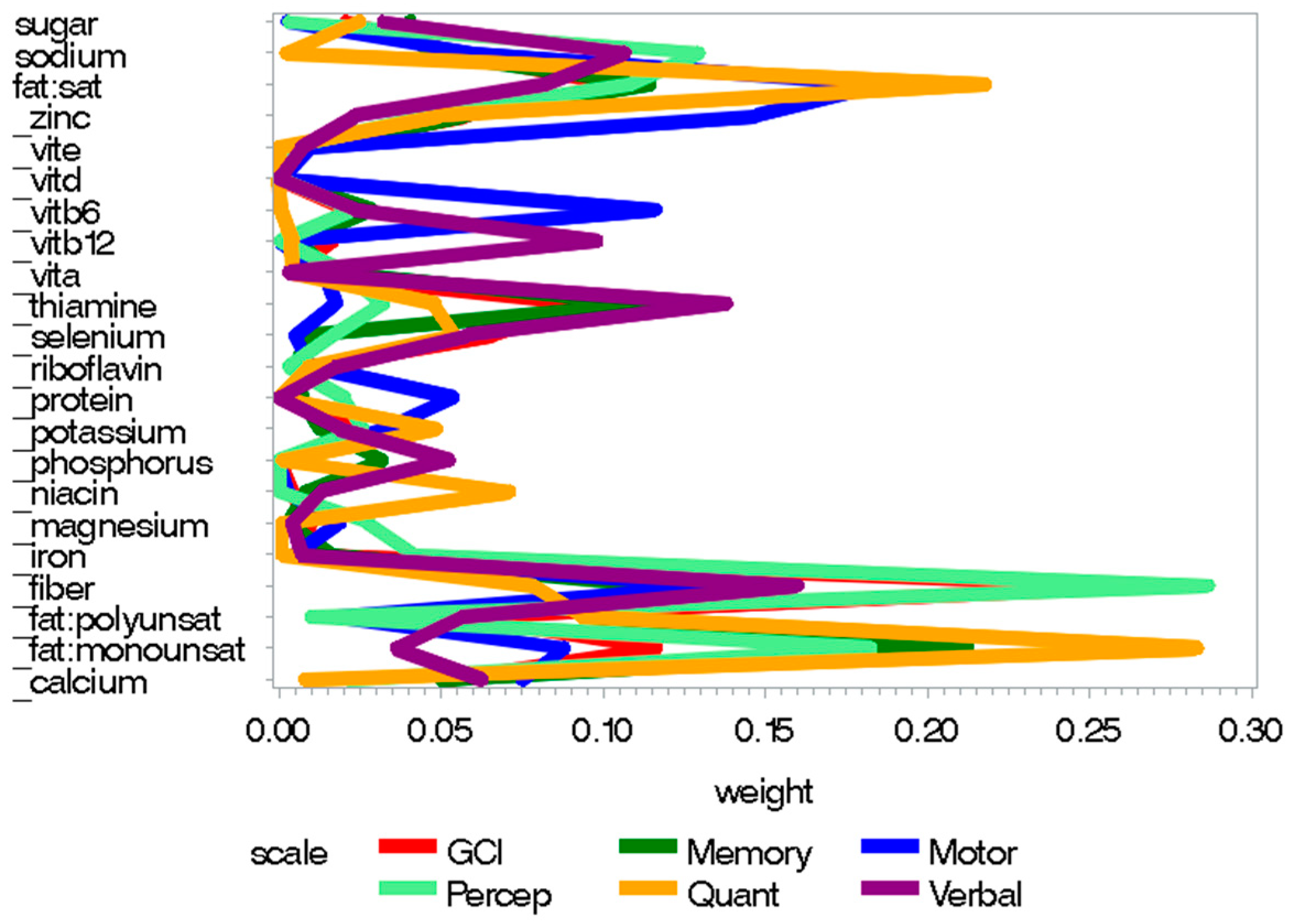
3.2. Childhood Nutrition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
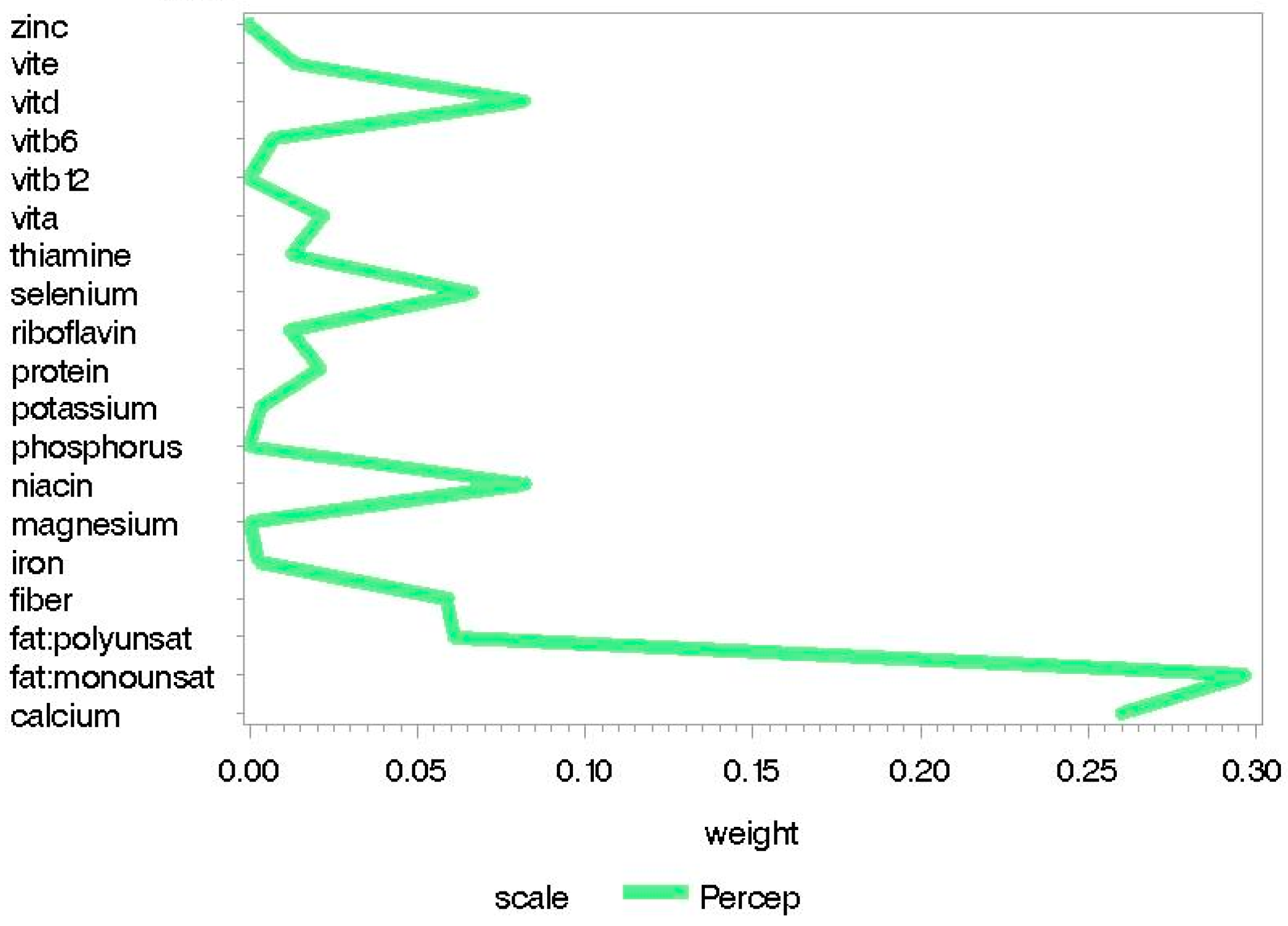
- Vite = Vitamin E
- Vitd = Vitamin D
- Vitb6 = Vitamin B6
- Vitb12 = Vitamin B12
- Vita = Vitamin A
- Fat: Polyunsat = Polyunsaturated fat
- Fat: Monounsat = Monounsaturated fat
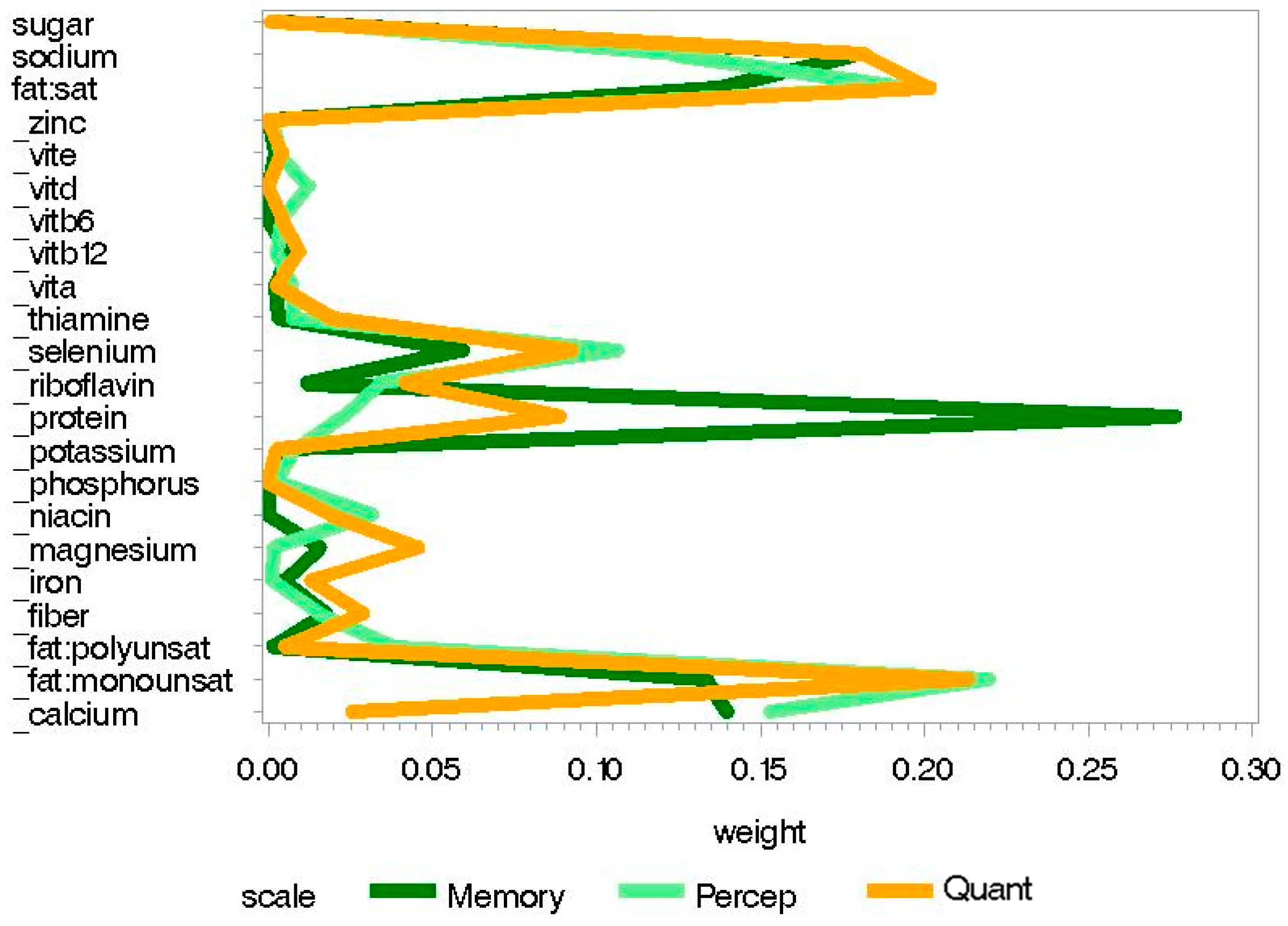
- Fat: Sat = Saturated Fat
- GCI = Global Composite Index
- Percep = Perceptual Performance
- Quan = Quantitative
- _zinc = negated value of zinc
- _vite = negated value of vitamin E
- _vitd = negated value of vitamin D
- _vitb6 = negated value of vitamin B6
- _vitb12 = negated value of vitamin B12
- _vita = negated value of vitamin A
- _thiamine = negated value of thiamine
- _selenium = negated value of selenium
- _riboflavin = negated value of riboflavin
- _protein = negated value of protein
- _potassium = negated value of potassium
- _phosphorus = negated value of phosphorus
- _niacin = negated value of niacin
- _magnesium = negated value of magnesium
- _iron = negated value of iron
- _fiber = negated value of fiber
- _fat: Polyunsat = negated value of polyunsaturated fat
- _fat: Monounsat = negated value of monounsaturated fat
- _calcium = negated value of calcium
- Adj = Adjusted
References
- Yang, X.; Bao, Y.; Fu, H.; Li, L.; Ren, T.; Yu, X. Selenium protects neonates against neurotoxicity from prenatal exposure to manganese. PLoS ONE 2014, 9, e86611. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr. Bull. 2008, 29, S126–S131. [Google Scholar] [CrossRef] [PubMed]
- Fattal-Valevski, A.; Azouri-Fattal, I.; Greenstein, Y.J.; Guindy, M.; Blau, A.; Zelnik, N. Delayed language development due to infantile thiamine deficiency. Dev. Med. Child Neurol. 2009, 51, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, P.; Tong, S.L.; Hao, J.H.; Tao, R.X.; Huang, K.; Hu, W.B.; Zhou, Q.F.; Jiang, X.M.; Tao, F.B. Cord blood vitamin D and neurocognitive development are nonlinearly related in toddlers. J. Nutr. 2015, 145, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Murray-Kolb, L.E.; Khatry, S.K.; Katz, J.; Schaefer, B.A.; Cole, P.M.; Leclerq, S.C.; Tielsch, J.M. Prenatal micronutrient supplementation and intellectual and motor function in early school-aged children in nepal. JAMA 2010, 304, 2716–2723. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, X.; Fu, H.; Li, L.; Ren, T. Different levels of prenatal zinc and selenium had different effects on neonatal neurobehavioral development. Neurotoxicology 2013, 37, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K. Nutrition and the developing brain: Nutrient priorities and measurement. Am. J. Clin. Nutr. 2007, 85, S614–S620. [Google Scholar]
- Gonzalez, H.F.; Visentin, S. Micronutrients and neurodevelopment: An update. Arch. Argent. Pediatr. 2016, 114, 570–575. [Google Scholar] [PubMed]
- Hou, N.; Ren, L.; Gong, M.; Bi, Y.; Gu, Y.; Dong, Z.; Liu, Y.; Chen, J.; Li, T. Vitamin A deficiency impairs spatial learning and memory: The mechanism of abnormal CBP-dependent histone acetylation regulated by retinoic acid receptor alpha. Mol. Neurobiol. 2015, 51, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.E.; Cheong, H.K.; Ha, E.H.; Kim, B.N.; Ha, M.; Kim, Y.; Hong, Y.C.; Park, H.; Oh, S.Y. Maternal blood manganese and early neurodevelopment: The mothers and children’s environmental health (MOCEH) study. Environ. Health Perspect. 2015, 123, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Uauy, R.; Dangour, A.D. Nutrition in brain development and aging: Role of essential fatty acids. Nutr. Rev. 2006, 64, S24–S33. [Google Scholar] [CrossRef] [PubMed]
- Clandinin, M.T.; Van Aerde, J.E.; Merkel, K.L.; Harris, C.L.; Springer, M.A.; Hansen, J.W.; Diersen-Schade, D.A. Growth and development of preterm infants fed infant formulas containing docosahexaenoic acid and arachidonic acid. J. Pediatr. 2005, 146, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.E.; Walden, R.V.; Gargus, R.A.; Tucker, R.; McKinley, L.; Mance, M.; Nye, J.; Vohr, B.R. First-week protein and energy intakes are associated with 18-month developmental outcomes in extremely low birth weight infants. Pediatrics 2009, 123, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Keen, C.L.; Uriu-Adams, J.Y.; Skalny, A.; Grabeklis, A.; Grabeklis, S.; Green, K.; Yevtushok, L.; Wertelecki, W.W.; Chambers, C.D. The plausibility of maternal nutritional status being a contributing factor to the risk for fetal alcohol spectrum disorders: The potential influence of zinc status as an example. Biofactors 2010, 36, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Risbud, R.D.; Chambers, C.D.; Thomas, J.D. Dietary nutrient intake in school-aged children with heavy prenatal alcohol exposure. Alcohol. Clin. Exp. Res. 2016, 40, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.; Aguirre, J.; Serrano, L. Alimentacio’n de Obreros Y Sus Familias; Publicacio’n l61; Divisio’n de Nutricio’n de Comunidad INNSZ/Instituto Nacional de Salud Pu’blica: Cuernavaca, Mexico, 1983. [Google Scholar]
- Hernandez-Avila, M.; Romieu, I.; Parra, S.; Hernandez-Avila, J.; Madrigal, H.; Willett, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico city. Salud Publ. Mex. 1998, 40, 133–140. [Google Scholar] [CrossRef]
- USDA. Dietary Supplement Fact Sheets. Available online: https://ods.od.nih.gov/factsheets/list-all/ (accessed on 5 July 2018).
- Bourges, H. Tablas de Composicio’n de Alimentos. “50 Aniversario Instituto Nacional de la Nutricio’n”; Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán: Cuernavaca, Mexico, 1996. [Google Scholar]
- Rodriguez-Ramirez, S.; Mundo-Rosas, V.; Jimenez-Aguilar, A.; Shamah-Levy, T. Methodology for the analysis of dietary data from the Mexican national health and nutrition survey 2006. Salud Publ. Mex. 2009, 51 (Suppl. 4), S523–S529. [Google Scholar] [CrossRef]
- McCarthy, D. Manual for the Mccarthy Scales of Children’s Abilities; Psychological Corp: New York, NY, USA, 1972. [Google Scholar]
- McCarthy, D. Escalas Mccarthy de Aptitudes Y Psicomotricidad Para Niños. Available online: http://www.pearsonclinical.es/producto/63/msca-escalas-mccarthy-de-aptitudes-y-psicomotricidad-para-ninos (accessed on 5 July 2018).
- Kaufman, A.S.; Kaufman, N.L. Clinical Evaluation of Young Children with the McCarthy Scales; Allyn and Bacon: Needham Heights, MA, USA, 1977. [Google Scholar]
- Carrasco, A.V. The AMAI System of Classifying Households by Socio-Economic Level: The Experience of Mexico and Its Comparison with Brazil and Argentina. In Proceedings of the Latin American Conference, Sao Paulo, Brazil, May 2002; Available online: http://archive.is/vT30#selection-693.0-695.11 (accessed on 5 July 2018).
- Caldwell, B.; Bradley, R. Home Observation for Measurement of the Environment: Administration Manual; Arizona State University: Tempe, AZ, USA, 2003. [Google Scholar]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. J. Agric. Biol. Environ. Stat. 2015, 20, 100–120. [Google Scholar] [CrossRef]
- USDA. 2015–2020 Dietary Guidelines for Americans, 8th ed. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 5 July 2018).
- Ramirez-Silva, I.; Jimenez-Aguilar, A.; Valenzuela-Bravo, D.; Martinez-Tapia, B.; Rodriguez-Ramirez, S.; Gaona-Pineda, E.B.; Angulo-Estrada, S.; Shamah-Levy, T. Methodology for estimating dietary data from the semi-quantitative food frequency questionnaire of the Mexican national health and nutrition survey 2012. Salud Publ. Mex. 2016, 58, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Torsvik, I.K.; Ueland, P.M.; Markestad, T.; Midttun, O.; Bjorke Monsen, A.L. Motor development related to duration of exclusive breastfeeding, B vitamin status and B12 supplementation in infants with a birth weight between 2000–3000 g, results from a randomized intervention trial. BMC Pediatr. 2015, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.; Mougan, I. Fatty acid composition of human brain phospholipids during normal development. J Neurochem. 1998, 71, 2528–2533. [Google Scholar] [CrossRef] [PubMed]
- Statovci, D.; Aguilera, M.; MacSharry, J.; Melgar, S. The impact of western diet and nutrients on the microbiota and immune response at mucosal interfaces. Front. Immunol. 2017, 8, 838. [Google Scholar] [PubMed]
- Ettinger, A.S.; Lamadrid-Figueroa, H.; Tellez-Rojo, M.M.; Mercado-Garcia, A.; Peterson, K.E.; Schwartz, J.; Hu, H.; Hernandez-Avila, M. Effect of calcium supplementation on blood lead levels in pregnancy: A randomized placebo-controlled trial. Environ. Health Perspect. 2009, 117, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, C. Calcium signaling and the development of specific neuronal connections. Prog. Brain Res. 2009, 175, 443–452. [Google Scholar] [PubMed]
- Neher, E.; Sakaba, T. Multiple roles of calcium ions in the regulation of neurotransmitter release. Neuron 2008, 59, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Kališnik, M.; Zorc-Pleskovič, R.; Pajer, Z.; Pavlin, K. The effect of chronic hypercalcemia or hypocalcemia on the follicular and parafollicular cells in rat thyroid gland. Am. J. Anat. 1990, 189, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.Z.; Sargent, J.D.; Larsen, P.R.; Waisbren, S.E.; Haddow, J.E.; Mitchell, M.L. Relation of severity of maternal hypothyroidism to cognitive development of offspring. J. Med. Screen. 2001, 8, 18–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, R.O.; Hu, H.; Silverman, E.K.; Tsaih, S.W.; Schwartz, J.; Bellinger, D.; Palazuelos, E.; Weiss, S.T.; Hernandez-Avila, M. Apolipoprotein E genotype predicts 24-month bayley scales infant development score. Pediatr. Res. 2003, 54, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Bennet, A.M.; Di Angelantonio, E.; Ye, Z.; Wensley, F.; Dahlin, A.; Ahlbom, A.; Keavney, B.; Collins, R.; Wiman, B.; de Faire, U.; et al. Association of apolipoprotein E genotypes with lipid levels and coronary risk. JAMA 2007, 298, 1300–1311. [Google Scholar] [CrossRef] [PubMed]
- Fernando, W.M.; Martins, I.J.; Goozee, K.G.; Brennan, C.S.; Jayasena, V.; Martins, R.N. The role of dietary coconut for the prevention and treatment of alzheimer’s disease: Potential mechanisms of action. Br. J. Nutr. 2015, 114, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Boris, M.; Mandel, F.S. Foods and additives are common causes of the attention deficit hyperactive disorder in children. Ann. Allergy 1994, 72, 462–468. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Third Trimester Nutrition Sample (n = 65) | 4–6 Year-Old Cross-Sectional Sample (n = 329) | Entire Cohort (n = 948) 1,2 | |
|---|---|---|---|
| Mother’s age at enrollment (years), mean (SD) | 28.42 (6.06) | 27.77 (5.57) | 27.66 (5.48) |
| Maternal Education, n (%) | |||
| <Secondary school | 25 (39%) | 129 (39%) | 385 (41%) |
| Secondary school | 21 (32%) | 118 (36%) | 334 (35%) |
| >Secondary school | 19 (29%) | 82 (25%) | 229 (24%) |
| SES index, n (%) | |||
| Low | 28 (43%) | 172 (52%) | 486 (51%) |
| Medium | 31 (48%) | 125 (38%) | 356 (38%) |
| High | 6 (9%) | 32 (10%) | 106 (11%) |
| Sex of child, n (%) | |||
| Male | 33 (51%) | 186 (57%) | 498 (53%) |
| Female | 32 (49%) | 143 (43%) | 450 (47%) |
| Child’s birthweight (kg), mean (SD) | 3.10 (0.40) | 3.12 (0.43) | 3.04 (0.49) |
| Gestational age at birth (weeks), mean (SD) | 38.28 (1.49) | 38.49 (1.62) | 38.24 (1.96) |
| HOME Score at 24 months, mean (SD) | 33.45 (4.72) | 31.91 (5.41) | 31.72 (5.42) |
| McCarthy Scales, mean (SD) | |||
| Memory | 46.20 (7.23) | 47.01 (8.15) | 47.06 (8.35) |
| Quantitative | 45.66 (7.98) | 46.10 (9.19) | 45.92 (9.44) |
| Motor | 44.42 (9.85) | 44.47 (8.67) | 44.44 (8.61) |
| Perception | 52.83 (7.71) | 51.96 (7.57) | 51.71 (7.94) |
| Verbal | 48.91 (8.59) | 49.87 (8.97) | 49.81 (8.97) |
| GCI | 99.20 (12.52) | 99.78 (12.86) | 99.55 (13.19) |
| Nutrition Component | Prenatal Nutrition (n = 65) | 4–6 Year-Old Nutrition (n = 329) | ||||||
|---|---|---|---|---|---|---|---|---|
| Dietary 1 Intake Reference for Pregnancy | Tolerable Upper Level | Food and Supplement Intake | Child 2 Dietary Intake Reference1 | Tolerable Upper Level | Food Intake 3 | |||
| Mean (SD) | Range | Mean (SD) | Range | |||||
| Kilocalories | 2295.6 (852.2) | 872.5–4839.6 | 1447.3 (356.2) | 642.9–2417.06 | ||||
| Protein, g | 71 | 74.6 (26.1) | 30.2–153.4 | 19 | 47.6 (12.5) | 20.0–82.5 | ||
| Zinc, mg | 11 | 40 | 13.9 (10.0) | 3.5–43.4 | 5 | 12 | 6.3 (1.9) | 1.8–15.4 |
| Vitamin A, mcg RAE | 770 | 3000 | 1016.8 (923.5) | 332.9–7009.4 | 400 | 900 | 492.8 (227.9) | 73.3–1383.5 |
| Vitamin E, mg | 15 | 1000 | 11.2 (4.3) | 3.8–22.4 | 7 | 300 | 5.8 (2.6) | 0.8–15.6 |
| Vitamin D, IU | 600 | 107.8 (159.4) | 1.8–1019.4 | 600 | 43.1 (51.4) | 1.3–389.2 | ||
| Vitamin B6, mg | 1.9 | 100 | 2.0 (0.8) | 0.6–4.7 | 0.6 | 40 | 1.1 (0.4) | 0.3–3.7 |
| Vitamin B12, mcg | 2.6 | 4.4 (3.4) | 0.8–27.9 | 1.2 mcg | 2.4 (1.3) | 0.5–11.9 | ||
| Thiamine, mg | 1.4 | 14.2 (33.0) | 0.5–103.9 | 0.6 | 0.8 (0.2) | 0.2–1.9 | ||
| Selenium, mcg | 60 | 400 | 45.6 (25.5) | 11.4–149.3 | 30 | 150 | 23.1 (11.0) | 4.8–86.3 |
| Riboflavin, mg | 1.4 | 2.5 (1.7) | 0.6–7.6 | 0.6 | 1.0 (0.4) | 0.2–2.7 | ||
| Potassium, mg | 4700 | 3189.8 (1419.2) | 852.3–9421.4 | 3800 | 1580.1 (621.9) | 398.1–4369.2 | ||
| Phosphorus, mg | 700 | 3500 | 1334.0 (485.6) | 440.5–2363.7 | 500 | 3000 | 893.8 (313.6) | 219.5–1916.7 |
| Niacin, mg | 18 | 35 | 15.2 (5.5) | 6.0–29.6 | 8 | 15 | 9.3 (3.2) | 2.4–21.7 |
| Magnesium, mg | 350–360 | 350 | 330.0 (137.1) | 85.4–778.9 | 130 | 110 | 178.3 (57.4) | 51.5–394.9 |
| Iron, mg | 27 | 45 | 54.1 (28.4) | 6.8–153.2 | 10 | 40 | 8.4 (3.0) | 2.8–20.2 |
| Fiber, g | 28 | 22.0 (9.7) | 5.1–54.3 | 16.8–19.6 | 11.3 (5.1) | 3.0–45.1 | ||
| Calcium, mg | 1000 | 2500 | 1460.8 (559.1) | 387.7–3064.2 | 1000 | 2500 | 937.1 (353.0) | 170.0–2237.0 |
| Monounsaturated fat, g | 21.1 (9.8) | 6.2–55.4 | 13.6 (5.2) | 2.5–36.5 | ||||
| Polyunsaturated fat, g | 15.5 | 11.3 (5.2) | 2.5–24.2 | 10 | 6.7 (3.1) | 1.4–28.6 | ||
| Saturated fat, mg | 28.6 (13.2) | 9.6–64.9 | 17.9 (9.0) | 1.9–54.0 | ||||
| Sugar, g | 38.5 (44.9) | 4.7–237.5 | 31.7 (23.8) | 1.0–179.9 | ||||
| Sodium, mg | 1500 | 2300 | 2241.9 (844.4) | 861.4–4820.2 | 1200 | 1900 | 1605.4 (546.7) | 581.4–3733.6 |
| Carbohydrates, g | 175 | 337.7 (165.6) | 97.3–1008.7 | 130 | 198.9 (57.4) | 81.6–421.2 | ||
| McCarthy Scale | Good Nutrition Index | Poor Nutrition Index | ||||
|---|---|---|---|---|---|---|
| WQS Beta | 95% CI | p Value | WQS Beta | 95% CI | p Value | |
| Memory | 2.56 | 0.99, 4.13 | 0.001 | −3.55 | −5.71, −1.38 | 0.001 |
| Quantitative | 1.78 | 0.11, 3.44 | 0.037 | −3.39 | −6.02, −0.76 | 0.012 |
| Motor | 2.84 | 1.11, 4.57 | 0.001 | −4.36 | −6.76, −1.96 | <0.001 |
| Perception | 1.64 | 0.33, 2.96 | 0.015 | −2.75 | −4.77, −0.72 | 0.008 |
| Verbal | 2.75 | 1.44, 4.06 | <0.001 | −3.71 | −5.46, −1.96 | <0.001 |
| GCI | 3.54 | 1.62, 5.45 | <0.001 | −4.69 | −7.28, −2.10 | <0.001 |
| McCarthy Scale | Good Nutrition Index | Poor Nutrition Index | ||||
|---|---|---|---|---|---|---|
| WQS Beta | 95% CI | p Value | WQS Beta | 95% CI | p Value | |
| Memory | 0.66 | −0.03, 1.35 | 0.059 | −1.44 | −2.59, −0.30 | 0.014 |
| Quantitative | 0.44 | −0.45, 1.32 | 0.335 | −1.74 | −3.27, −0.20 | 0.026 |
| Motor | 0.70 | −0.18, 1.57 | 0.120 | −1.18 | −2.49, 0.13 | 0.078 |
| Perception | 0.81 | 0.01, 1.61 | 0.048 | −1.88 | −3.17, −0.58 | 0.004 |
| Verbal | 0.66 | −0.13, 1.45 | 0.102 | −0.73 | −1.64, 0.18 | 0.115 |
| GCI | 0.92 | −0.27, 2.11 | 0.131 | −1.77 | −3.66, 0.11 | 0.066 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malin, A.J.; Busgang, S.A.; Cantoral, A.J.; Svensson, K.; Orjuela, M.A.; Pantic, I.; Schnaas, L.; Oken, E.; Baccarelli, A.A.; Téllez-Rojo, M.M.; et al. Quality of Prenatal and Childhood Diet Predicts Neurodevelopmental Outcomes among Children in Mexico City. Nutrients 2018, 10, 1093. https://doi.org/10.3390/nu10081093
Malin AJ, Busgang SA, Cantoral AJ, Svensson K, Orjuela MA, Pantic I, Schnaas L, Oken E, Baccarelli AA, Téllez-Rojo MM, et al. Quality of Prenatal and Childhood Diet Predicts Neurodevelopmental Outcomes among Children in Mexico City. Nutrients. 2018; 10(8):1093. https://doi.org/10.3390/nu10081093
Chicago/Turabian StyleMalin, Ashley J., Stefanie A. Busgang, Alejandra J. Cantoral, Katherine Svensson, Manuela A. Orjuela, Ivan Pantic, Lourdes Schnaas, Emily Oken, Andrea A. Baccarelli, Martha M. Téllez-Rojo, and et al. 2018. "Quality of Prenatal and Childhood Diet Predicts Neurodevelopmental Outcomes among Children in Mexico City" Nutrients 10, no. 8: 1093. https://doi.org/10.3390/nu10081093
APA StyleMalin, A. J., Busgang, S. A., Cantoral, A. J., Svensson, K., Orjuela, M. A., Pantic, I., Schnaas, L., Oken, E., Baccarelli, A. A., Téllez-Rojo, M. M., Wright, R. O., & Gennings, C. (2018). Quality of Prenatal and Childhood Diet Predicts Neurodevelopmental Outcomes among Children in Mexico City. Nutrients, 10(8), 1093. https://doi.org/10.3390/nu10081093