Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies




Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
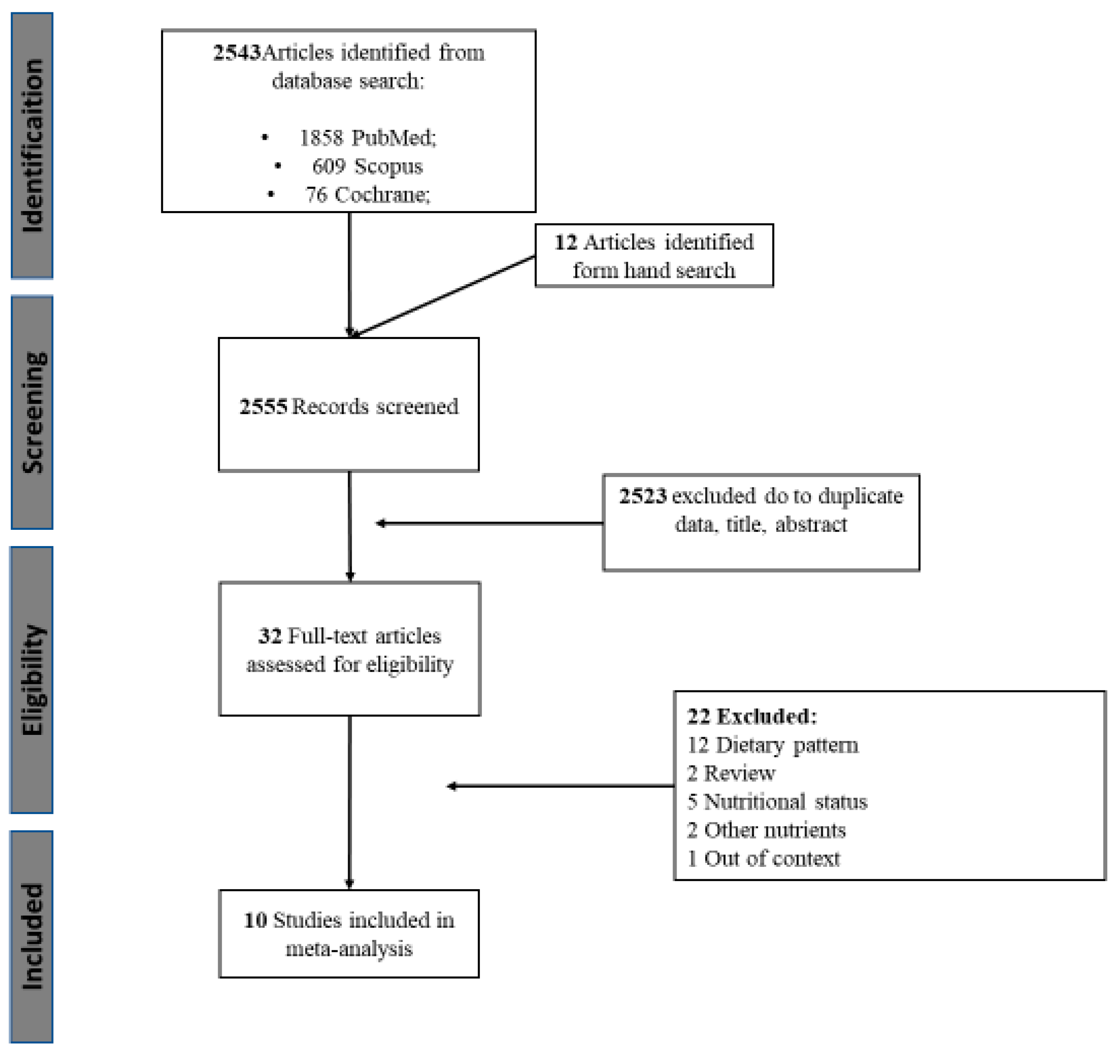
3.1. Literature Search
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
3.4. Association between Protein Intake and Frailty
3.4.1. Protein Intake and Frailty Prevalence (i.e., Cross-Sectional Studies)
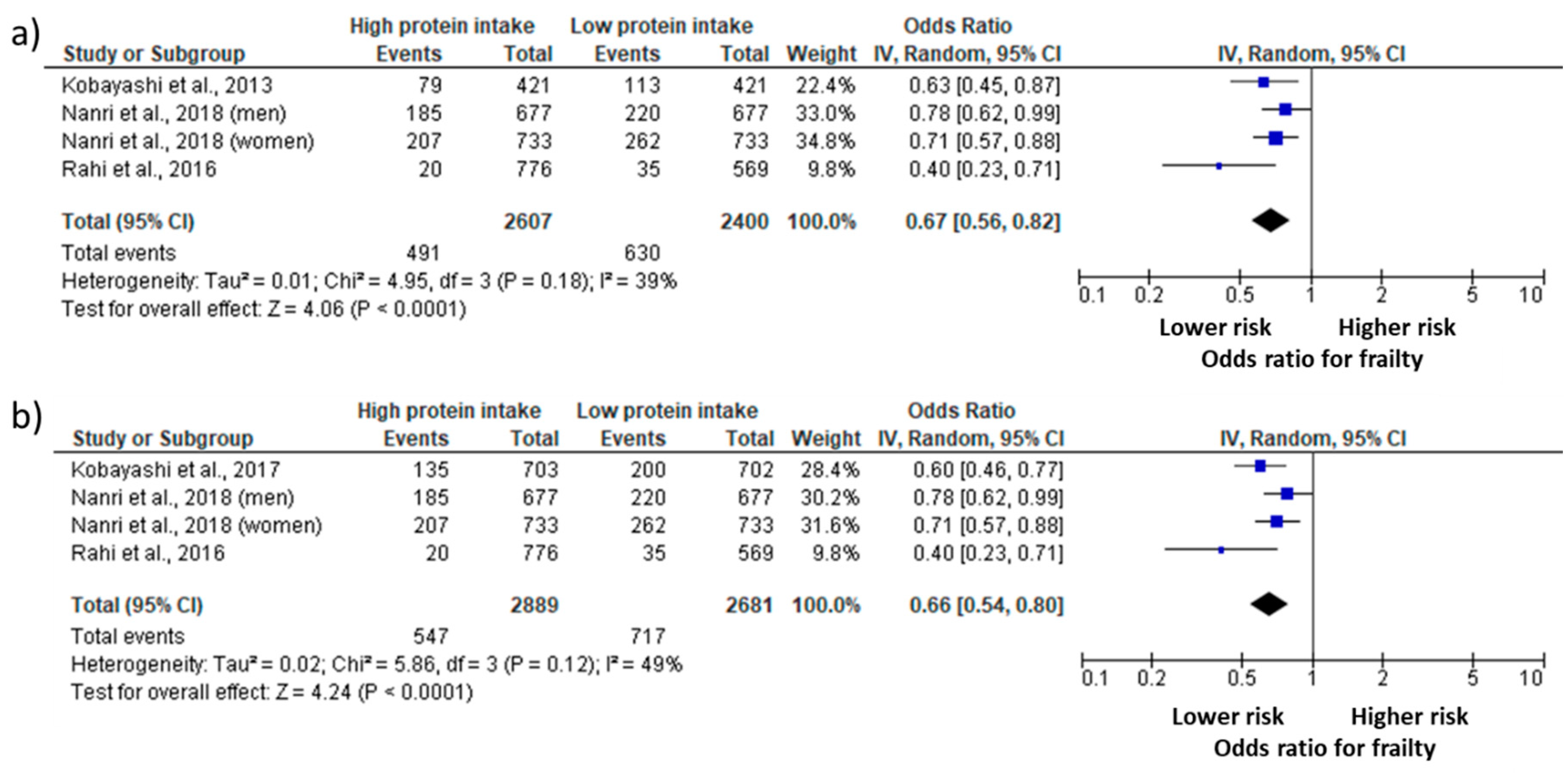
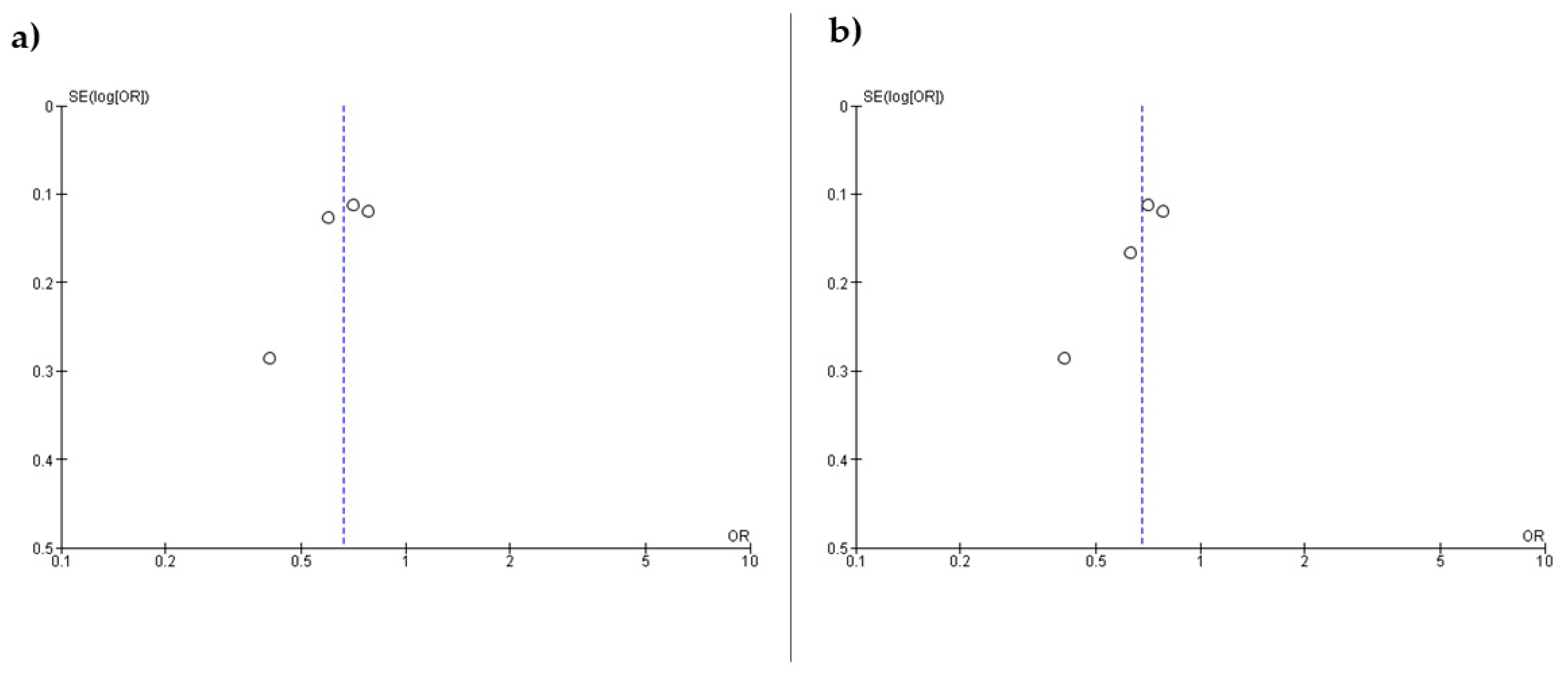
3.4.2. Protein Intake and Frailty Risk (i.e., Longitudinal Studies)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morley, J.E.; Vellas, B.; Abellan van Kan, G.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty Consensus: A Call to Action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesari, M.; Calvani, R.; Marzetti, E. Frailty in Older Persons. Clin. Geriatr. Med. 2017, 33, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Artaza-Artabe, I.; Sáez-López, P.; Sánchez-Hernández, N.; Fernández-Gutierrez, N.; Malafarina, V. The relationship between nutrition and frailty: Effects of protein intake, nutritional supplementation, vitamin D and exercise on muscle metabolism in the elderly. A systematic review. Maturitas 2016, 93, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Yannakoulia, M.; Ntanasi, E.; Anastasiou, C.A.; Scarmeas, N. Frailty and nutrition: From epidemiological and clinical evidence to potential mechanisms. Metabolism 2017, 68, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.; Bandinelli, S.; Lunenfeld, B. Frailty and the role of nutrition in older people. A review of the current literature. Acta. Biomed. 2010, 81 (Suppl. 1), 37–45. [Google Scholar] [PubMed]
- Phillips, S.M. The science of muscle hypertrophy: Making dietary protein count. Proc. Nutr. Soc. 2011, 70, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Stokes, T.; Hector, A.J.; Morton, R.W.; McGlory, C.; Phillips, S.M. Recent Perspectives Regarding the Role of Dietary Protein for the Promotion of Muscle Hypertrophy with Resistance Exercise Training. Nutrients 2018, 10, 180. [Google Scholar] [CrossRef] [PubMed]
- Tipton, K.D.; Phillips, S.M. Dietary Protein for Muscle Hypertrophy. In Nestle Nutrition Institute Workshop Series; Karger Publishers: Basel, Switzerland, 2013; Volume 76, pp. 73–84. [Google Scholar]
- Robinson, S.M.; Reginster, J.Y.; Rizzoli, R.; Shaw, S.C.; Kanis, J.A.; Bautmans, I.; Bischoff-Ferrari, H.; Bruyere, O.; Cesari, M.; Dawson-Hughes, B.; et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin. Nutr. 2018, 37, 1121–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. Aging is associated with diminished accretion of muscle proteins after the ingestion of a small bolus of essential amino acids. Am. J. Clin. Nutr. 2005, 82, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. A high proportion of leucine is required for optimal stimulation of the rate of muscle protein synthesis by essential amino acids in the elderly. Am. J. Physiol. Metab. 2006, 291, E381–E387. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H. Nutrition for Sarcopenia. J. Clin. Med. Res. 2015, 7, 926–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, S.M. Current Concepts and Unresolved Questions in Dietary Protein Requirements and Supplements in Adults. Front. Nutr. 2017, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Rue, A.; Koehler, K.M.; Wayne, S.J.; Chiulli, S.J.; Haaland, K.Y.; Garry, P.J. Nutritional status and cognitive functioning in a normally aging sample: A 6-year reassessment. Am. J. Clin. Nutr. 1997, 65, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.O.; Roberts, L.A.; Geda, Y.E.; Cha, R.H.; Pankratz, V.S.; O’Connor, H.M.; Knopman, D.S.; Petersen, R.C. Relative Intake of Macronutrients Impacts Risk of Mild Cognitive Impairment or Dementia. J. Alzheimer’s Dis. 2012, 32, 329–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, F.; Charlton, K.; Walton, K.; McMahon, A.-T. Role of dietary protein and thiamine intakes on cognitive function in healthy older people: A systematic review. Nutrients 2015, 7, 2415–2439. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe, I. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Green, S.; Higgins, J. Cochrane handbook for systematic reviews of interventions. 2005. [Google Scholar]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low nutrient intake is an essential component of frailty in older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S. High protein intake is associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2013, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Suga, H.; Sasaki, S. Diet with a combination of high protein and high total antioxidant capacity is strongly associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2017, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but not amount of protein intake is associated with frailty: A cross-sectional investigation in the region of Nurnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [PubMed]
- Shikany, J.M.; Barrett-Connor, E.; Ensrud, K.E.; Cawthon, P.M.; Lewis, C.E.; Dam, T.-T.L.; Shannon, J.; Redden, D.T. Macronutrients, diet quality, and frailty in older men. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Rahi, B.; Colombet, Z.; Gonzalez-Colaco Harmand, M.; Dartigues, J.-F.; Boirie, Y.; Letenneur, L.; Feart, C. Higher Protein but Not Energy Intake Is Associated with a Lower Prevalence of Frailty Among Community-Dwelling Older Adults in the French Three-City Cohort. J. Am. Med. Dir. Assoc. 2016, 17, 672.e7–672.e11. [Google Scholar] [CrossRef] [PubMed]
- Nanri, H.; Yamada, Y.; Yoshida, T.; Okabe, Y.; Nozawa, Y.; Itoi, A.; Yoshimura, E.; Watanabe, Y.; Yamaguchi, M.; Yokoyama, K.; et al. Sex Difference in the Association Between Protein Intake and Frailty: Assessed Using the Kihon Checklist Indexes Among Older Adults. J. Am. Med. Dir. Assoc. 2018, 19, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Lacroix, A.Z.; Neuhouser, M.L.; Huang, Y.; Tinker, L.; Woods, N.; Michael, Y.; Curb, J.D.; Prentice, R.L. Protein intake and incident frailty in the women’s health initiative observational study. J. Am. Geriatr. Soc. 2010, 58, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Insausti, H.; Perez-Tasigchana, R.F.; Lopez-Garcia, E.; Garcia-Esquinas, E.; Rodriguez-Artalejo, F.; Guallar-Castillon, P. Macronutrients Intake and Incident Frailty in Older Adults: A Prospective Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Berrut, G.; Lesourd, B.; Ferry, M.; Gilbert, T.; Guerin, O.; Hanon, C.; Jeandel, C.; Paillaud, E.; Raynaud-Simon, A.; et al. Frailty and nutrition: Searching for evidence. J. Nutr. Health Aging 2015, 19, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Lopez, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodriguez-Villamil, J.L.; Millan-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T. Overlaps between Frailty and Sarcopenia Definitions. In Nestle Nutrition Institute Workshop Series; Karger Publishers: Basel, Switzerland, 2015; Volume 83, pp. 65–70. [Google Scholar]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the Biological Substrate of Physical Frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Cesari, M.; Tosato, M.; Cherubini, A.; Di Bari, M.; Pahor, M.; Savera, G.; Collamati, A.; D’Angelo, E.; et al. Operationalization of the physical frailty & sarcopenia syndrome: Rationale and clinical implementation. Transl. Med. UniSa. 2015, 13, 29. [Google Scholar] [PubMed]
- Ziaaldini, M.M.; Marzetti, E.; Picca, A.; Murlasits, Z. Biochemical Pathways of Sarcopenia and Their Modulation by Physical Exercise: A Narrative Review. Front. Med. 2017, 4, 167. [Google Scholar] [CrossRef] [PubMed]
- Frisoli, A.; Chaves, P.H.; Ingham, S.J.M.; Fried, L.P. Severe osteopenia and osteoporosis, sarcopenia, and frailty status in community-dwelling older women: Results from the Women’s Health and Aging Study (WHAS) II. Bone 2011, 48, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M.; Schols, J.M.G.A.; Meijers, J.M.M.; Tan, F.E.S.; Verlaan, S.; Luiking, Y.C.; Morley, J.E.; Halfens, R.J.G. Instruments to assess sarcopenia and physical frailty in older people living in a community (care) setting: Similarities and discrepancies. J. Am. Med. Dir. Assoc. 2015, 16, 301–308. [Google Scholar] [CrossRef] [PubMed]
- McGlory, C.; Devries, M.C.; Phillips, S.M. Skeletal muscle and resistance exercise training; the role of protein synthesis in recovery and remodeling. J. Appl. Physiol. 2016, 122, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-O.; Lee, K.-R. Preventive effect of protein-energy supplementation on the functional decline of frail older adults with low socioeconomic status: A community-based randomized controlled study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.C.; de Groot, L.C. Protein Supplementation Improves Physical Performance in Frail Elderly People: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Barbagallo, M. Perspective: Protein supplementation in frail older persons: Often necessary but not always sufficient. J. Am. Med. Dir. Assoc. 2013, 14, 72–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeymans, N.; Feskens, E.J.; van den Bos, G.A.; Kromhout, D. Measuring functional status: Cross-sectional and longitudinal associations between performance and self-report (Zutphen Elderly Study 1990–1993). J. Clin. Epidemiol. 1996, 49, 1103–1110. [Google Scholar] [CrossRef]
- Cress, M.E.; Buchner, D.M.; Questad, K.A.; Esselman, P.C.; deLateur, B.J.; Schwartz, R.S. Exercise: Effects on physical functional performance in independent older adults. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M242–M248. [Google Scholar] [CrossRef] [PubMed]
- Gregorio, L.; Brindisi, J.; Kleppinger, A.; Sullivan, R.; Mangano, K.M.; Bihuniak, J.D.; Kenny, A.M.; Kerstetter, J.E.; Insogna, K.L. Adequate dietary protein is associated with better physical performance among post-menopausal women 60–90 years. J. Nutr. Health Aging 2014, 18, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.S.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2017, 36, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kröger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkilä, A.T. Dietary protein intake is associated with better physical function and muscle strength among elderly women. Br. J. Nutr. 2016, 115, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Ten Haaf, D.; van Dongen, E.; Nuijten, M.; Eijsvogels, T.; de Groot, L.; Hopman, M. Protein Intake and Distribution in Relation to Physical Functioning and Quality of Life in Community-Dwelling Elderly People: Acknowledging the Role of Physical Activity. Nutrients 2018, 10, 506. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Loprinzi, P.D.; Murphy, C.H.; Phillips, S.M. Per meal dose and frequency of protein consumption is associated with lean mass and muscle performance. Clin. Nutr. 2016, 35, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Imai, E.; Tsubota-Utsugi, M.; Kikuya, M.; Satoh, M.; Inoue, R.; Hosaka, M.; Metoki, H.; Fukushima, N.; Kurimoto, A.; Hirose, T.; et al. Animal Protein Intake Is Associated with Higher-Level Functional Capacity in Elderly Adults: The Ohasama Study. J. Am. Geriatr. Soc. 2014, 62, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Borgonjen-Van den Berg, K.; Van Loon, L.; de Groot, L. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697–9706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Costa, B.R.; Cevallos, M.; Altman, D.G.; Rutjes, A.W.S.; Egger, M. Uses and misuses of the STROBE statement: Bibliographic study. BMJ Open 2011, 1, e000048. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Year | Authors | Country | Study Design | Setting | n | Mean Age (age range; min–max) | Sex Ratio of Participants (female/male) by frail vs. non-frail | Frailty Assessment Method | Dietary Intake Assessment Method | Protein Intake (g/day) | Protein Intake Level Definition | Outcomes | Covariates Included in Models | Quality Analysis Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cross-sectional | ||||||||||||||
| 2006 | Bartali et al. [23] | Italy | Cross-sectional | Community-dwelling | 802 | 74.1 | 1.2 | CHS frailty index (a) | Food-frequency questionnaire | - | Dichotomous | Low protein intake is associated with frailty | Results were adjusted for age, sex, education, economic status, household composition, smoking status, number of diseases, cognitive function, body mass index, and “happiness.” | 22 |
| 2013 | Kobayashi et al. [24] | Japan | Cross-sectional | Community-dwelling | 2108 | 74.7 | - | CHS frailty index (b) | Self-administered diet history questionnaire | 74.0 | Quintile (≤62.9 g/day, 6369.8 g/day, 69.8–76.1 g/day, 76.1–84.3 g/day, ≥84.3 g/day) | Protein intake was inversely associated with frailty | Results were energy-adjusted and for age, BMI, residential block, size of residential area, living alone, current smoking, alcohol drinking, dietary supplement use, history of chronic disease, depression symptoms, and energy intake. | 20 |
| 2013 | Bollwein et al. [26] | Germany | Cross-sectional | Community-dwelling | 194 | 83.0 (75–96) | 6.5 vs. 1.3 | CHS frailty index | Food-frequency questionnaire | 76.6 | Quartiles (≤0.90, 0.91–1.07, 1.08, ≥1.27) | Protein intake was not associated with frailty | Results were adjusted for age and sex, instrumental activities of the daily living score, number of medications, and chewing difficulties | 19 |
| 2014 | Shikany et al. [27] | United States of America | Cross-sectional | Commnity-dwelling | 5925 | 75.0 | - | CHS frailty index (c) | Food-frequency questionnaire | - | Quintile (≤6.0–13.7%, 13.8–15.2%, 15.3–16.5%, 16.6%–18.3%, 18.4–29.3%) | Protein intake was not associated with frailty | Results were adjusted for age, race, center, education, marital status, smoking, health status, medical conditions, body mass index, and energy intake | 20 |
| 2016 | Rahi et al. [28] | France | Cross-sectional | Community-dwelling | 1345 | 75.6 | 4.0 vs. 1.46 | CHS frailty index (d) | 24 h dietary recall | 70.4 | Dicothomous <1g/kg body weight/day and ≥1g/kg body weight | Protein intake was associated with frailty | The model 1 was adjusted for age, sex, and educational level; and the model 2 was additionally adjusted for BMI, diabetes, cardiovascular history, depression, cognitive performance, number of drugs, and total energy intake. | 20 |
| 2017 | Kobayashi et al. [25] | Japan | Cross-sectional | Community-dwelling | 2108 | 74.0 | - | CHS frailty index (b) | Self-administered diet history questionnaire | 73.1 | Tertile (≤67.6 g/day, 67.6–78.3 g/day, ≥78.3 g/day) | Protein intake was inversely associated with frailty | Dietary total antioxidant capacity | 20 |
| 2018 | Nanri et al. [29] | Japan | Cross-sectional | Community-dwelling | 5638 | 73.2 | 0.88 vs. 1.05 * | KCL | Food-frequency questionnaire | - | Men = quartiles (≤48.8 g/day, 48.8–56.1 g/day, 56.1–65.4 g/day, >65.4 g/day); Women = quartiles (<43.8 g/day, 43.8–51.1 g/day, 51.1–59.5 g/day, >59.5 g/day) | Protein intake was inversely associated with frailty | For men, the model 1 was adjusted forage, body mass index, total energy intake, alcohol status, smoking status and history of disease and the model 2 was adjusted for family structure, educational attainment, population density, and self-related health. | 20 |
| Longitudinal | ||||||||||||||
| 2010 | Beasley et al. [30] | United States of America | Longitudinal (3.0 years follow-up) | Community-dwelling | 24,417 | 65–79 | - | CHS frailty index (e) | Food-frequency questionnaire | 72.8 | Quintiles of protein intake (% kilocalories) | Protein intake was significantly associated with the odds of becoming frail | Results were adjusted for age, ethnicity, BMI, income, education, having a current health care provider, smoking, alcohol, general health status, history of comorbid conditions, history of hormone therapy use, number of falls, whether participant lives alone, disabled defined by at least 1 activity of daily living affected, depressive symptoms, log-transformed calibrated energy intake | 20 |
| 2014 | Shikany et al. [27] | United States of America | Longitudinal (4.6 years follow-up) | Community-dwelling | 5925 | 75.0 | - | CHS frailty index (c) | Food-frequency questionnaire | - | Quintile (≤6.0–13.7%, 13.8–15.2%, 15.3–16.5%, 16.6%–18.3%, 18.4–29.3%) | Protein intake was not associated with the odds of becoming frail | Results were adjusted for age, race, center, education, marital status, smoking, health status, medical conditions, body mass index, and energy intake | 20 |
| 2016 | Sandoval-Insausti et al. [31] | Spain | Longitudinal (3.5 years follow-up) | Community-dwelling | 1822 | 68.7 | 0.9 vs. 2.4 | CHS frailty index | Computerized face-to-face diet history | 76.6 | Quartiles of protein intake | Protein intake was associated with the odds of becoming frail | Results were adjusted for age, energy intake, ethanol, lipids, animal or vegetal protein, level of education, marital status, tobacco consumption, BMI, abdominal obesity, and dietary fiber, diseases. | 20 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho-Júnior, H.J.; Rodrigues, B.; Uchida, M.; Marzetti, E. Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2018, 10, 1334. https://doi.org/10.3390/nu10091334
Coelho-Júnior HJ, Rodrigues B, Uchida M, Marzetti E. Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients. 2018; 10(9):1334. https://doi.org/10.3390/nu10091334
Chicago/Turabian StyleCoelho-Júnior, Hélio José, Bruno Rodrigues, Marco Uchida, and Emanuele Marzetti. 2018. "Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies" Nutrients 10, no. 9: 1334. https://doi.org/10.3390/nu10091334
APA StyleCoelho-Júnior, H. J., Rodrigues, B., Uchida, M., & Marzetti, E. (2018). Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients, 10(9), 1334. https://doi.org/10.3390/nu10091334