Socio-Demographic Factors and Body Image Perception Are Associated with BMI-For-Age among Children Living in Welfare Homes in Selangor, Malaysia




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Respondents
2.2. Study Measurements
2.2.1. Anthropometric Measurements
2.2.2. Socio-Demographic Factors
2.2.3. Psychological Factors
Self-Esteem
Depressive Disorders
Perception of Body Shape
Perception of Body Weight Status
2.3. Statistical Analyses
3. Results
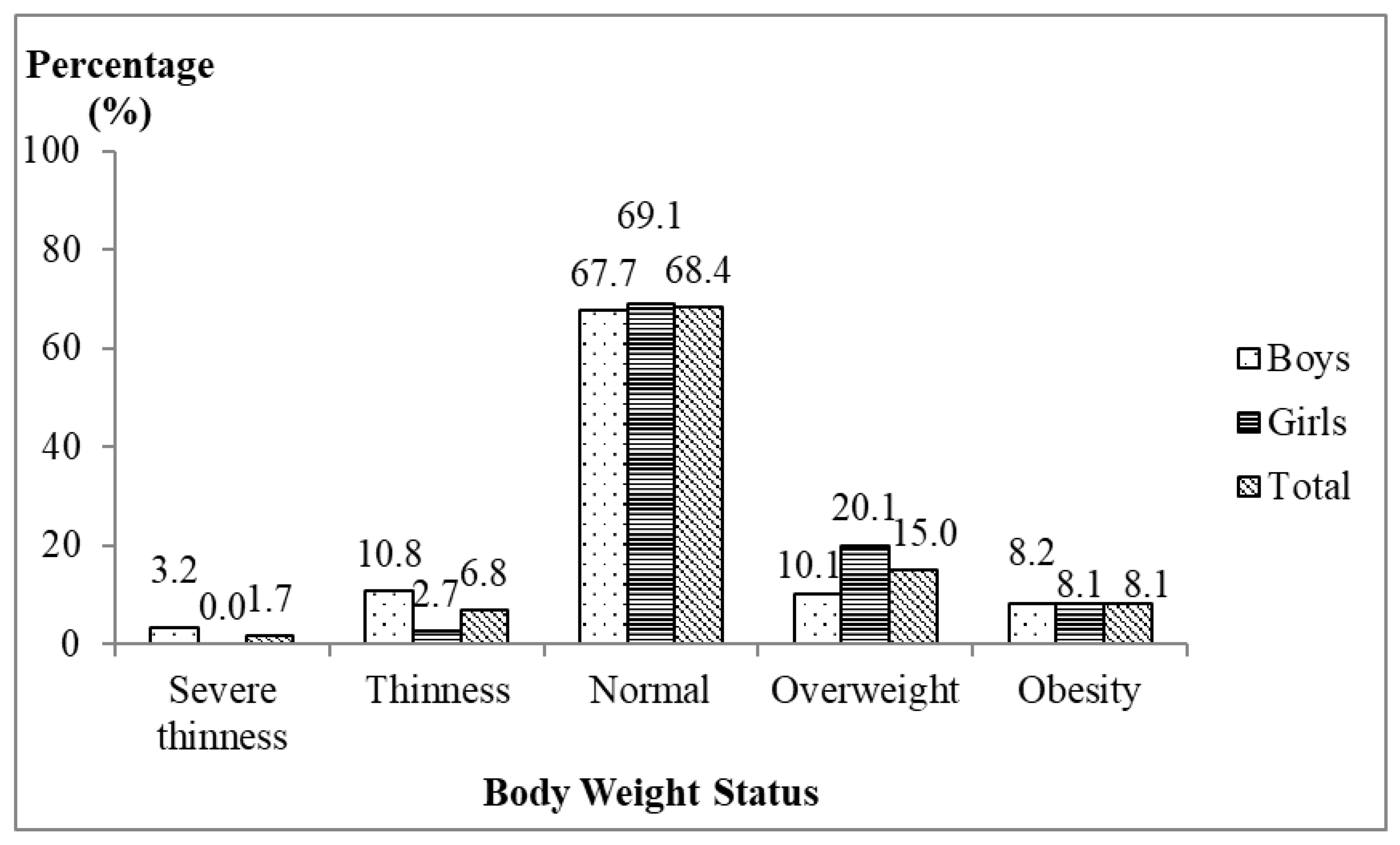
3.1. Body Weight Status of the Respondents
3.2. Socio-Demographic Factors of the Respondents
3.3. Psychological Factors of the Respondents
3.4. Associations between Socio-Demographic and Psychological Factors with BMI-for-Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Cash, T.F. Body image: Past, present, and future. Body Image 2004, 1, 1–5. [Google Scholar] [CrossRef]
- Grogan, S. Promoting positive body image in males and females: Contemporary issues and future directions. Sex Roles 2010, 63, 757–765. [Google Scholar] [CrossRef]
- Voelker, D.K.; Reel, J.J.; Greenleaf, C. Weight status and body image perceptions in adolescents: Current perspectives. Adolesc. Health Med. Ther. 2015, 6, 149–158. [Google Scholar] [PubMed]
- Harriger, J.A.; Thompson, J.K. Psychological consequences of obesity: Weight bias and body image in overweight and obese youth. Int. Rev. Psychiatry 2012, 24, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibiloni Mdel, M.; Pich, J.; Pons, A.; Tur, J.A. Body image and eating patterns among adolescents. BMC Public Health 2013, 13, 1104. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; McLean, S.A.; Marques, M.; Dunstan, C.J.; Paxton, S.J. Trajectories of body dissatisfaction and dietary restriction in early adolescent girls: A latent class growth analysis. J. Youth Adolesc. 2016, 45, 1664–1677. [Google Scholar] [CrossRef] [PubMed]
- Malete, L.; Motlhoiwa, K.; Shaibu, S.; Wrotniak, B.H.; Maruapula, S.D.; Jackson, J.; Compher, C.W. Body image dissatisfaction is increased in male and overweight/obese adolescents in Botswana. J. Obes. 2013, 2013, 763624. [Google Scholar] [CrossRef]
- Alipour, B.; Abbasalizad Farhangi, M.; Dehghan, P.; Alipour, M. Body image perception and its association with body mass index and nutrient intakes among female college students aged 18–35 years from Tabriz, Iran. Eat. Weight Disord. 2015, 20, 465–471. [Google Scholar] [CrossRef]
- Kopcakova, J.; Veselska, Z.D.; Geckova, A.M.; van Dijk, J.P.; Reijneveld, S.A. Is being a boy and feeling fat a barrier for physical activity? The association between body image, gender and physical activity among adolescents. Int. J. Environ. Res. Public Health 2014, 11, 11167–11176. [Google Scholar] [CrossRef]
- Slater, A.; Tiggemann, M. Gender differences in adolescent sport participation, teasing, self-objectification and body image concerns. J. Adolesc. 2011, 34, 455–463. [Google Scholar] [CrossRef]
- Khor, G.L.; Zalilah, M.S.; Phan, Y.Y.; Maznah, B.; Norimah, A.K. Perception of body image among Malaysian male and female adolescents. Singap. Med. J. 2009, 50, 303–311. [Google Scholar]
- Zainuddin, A.A.; Manickam, M.A.; Baharudin, A.; Omar, A.; Cheong, S.M.; Ambak, R.; Ahmad, M.H.; Ghaffar, S.A. Self-Perception of Body Weight Status and Weight Control Practices among Adolescents in Malaysia. Asia Pac. J. Public Health 2014, 26, 18S–26S. [Google Scholar] [CrossRef] [PubMed]
- Institute for Public Health (IPH). National Health and Morbidity Survey 2015 (NHMS 2015). Volume II: Non-Communicable Diseases, Risk Factors & Other Health Problems. 2015. Available online: http://iku.moh.gov.my/images/IKU/Document/REPORT/nhmsreport2015vol2.pdf (accessed on 26 July 2015).
- Chee, Y.F.; Roseline Yap, W.K.; Siti, S.B. Weight Status and Dietary Intake among Female Children and Adolescents Aged 6–17 Years in a Welfare Home, Kuala Lumpur. Malays. J. Nutr. 2008, 14, 79–89. [Google Scholar] [PubMed]
- Mohd Dzulkhairi, M.R.; Syimir, S.; Zairina, A.R.; Wan Noraini, W.S.; Khairun Nain, N.; Nazefah, A.H. Nutritional status, knowledge, attitude, and practice among orphans living in institutions in Selangor and Melaka. Med. J. Malays. 2015, 70, 1. [Google Scholar]
- Côté, S.M.; Orri, M.; Marttila, M.; Ristikari, T. Out-of-home placement in early childhood and psychiatric diagnoses and criminal convictions in young adulthood: A population-based propensity score-matched study. Lancet Child Adolesc. Health 2018, 2, 647–653. [Google Scholar] [CrossRef]
- Brännström, L.; Vinnerljung, B.; Forsman, H.; Almquist, Y.B. Children Placed in Out-of-Home Care as Midlife Adults: Are They Still Disadvantaged or Have They Caught up with Their Peers? Child Maltreat. 2017, 22, 205–214. [Google Scholar] [CrossRef]
- Forsman, H.; Brännström, L.; Vinnerljung, B.; Hjern, A. Does poor school performance cause later psychosocial problems among children in foster care? Evidence from national longitudinal registry data. Child Abuse Negl. 2016, 57, 61–71. [Google Scholar] [CrossRef]
- Fallesen, P. Identifying divergent foster care careers for Danish children. Child Abuse Negl. 2014, 38, 1860–1871. [Google Scholar] [CrossRef] [Green Version]
- Stein, R.E.K.; Hurlburt, M.S.; Heneghan, A. Chronic conditions among children investigated by child welfare. Pediatrics 2013, 131, 455–462. [Google Scholar] [CrossRef]
- Turney, K.; Wildeman, C. Mental and Physical Health of Children in Foster Care. Pediatrics 2016, 138, e20161118. [Google Scholar] [CrossRef]
- Horwitz, S.M.; Hurlburt, M.S.; Cohen, S.D.; Zhang, J.; Landsverk, J. Predictors of placement for children who initially remained in their homes after an investigation for abuse and neglect. Child Abuse Negl. 2011, 35, 188–198. [Google Scholar] [CrossRef]
- Thompson, A.H. Childhood depression revisited: Indicators, normative tests and clinical course. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 5–8. [Google Scholar]
- Gürsoy, F.; Biçakçi, M.Y.; Orhan, E.; Bakırcı, S.; Çatak, S.; Yerebakan, Ö. Study on Self-Concept Levels of Adolescents in the Age Group of 13–18 who Live in Orphanage and those who do not Live in Orphanage. Int. J. Soc. Sci. Educ. 2012, 2, 56–66. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- WHO AnthroPlus for Personal Computers Manual. Software for Assessing the Growth of the World’s Children and Adolescents. Geneva: World Health Organization. 2009. Available online: http://www.who.int/growthref/tools/en/ (accessed on 10 March 2014).
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Fawzy, N.; Fouad, A. Psychosocial and Developmental Status of Orphanage Children: Epidemiological Study. Curr. Psychiatry 2010, 17, 41–48. [Google Scholar]
- Kovacs, M. The Children’s Depression Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Kovacs, M. The Children’s Depression Inventory (CDI) Manual; Multi-Health Systems: Toronto, ON, USA, 1992; pp. 15–25. [Google Scholar]
- Collins, M.E. Body figure perceptions and preferences among preadolescent children. Int. J. Eat. Disord. 1991, 10, 199–208. [Google Scholar] [CrossRef]
- Thompson, M.A.; Gray, J.J. Development and validation of a new body image assessment tool. J. Pers. Assess. 1995, 64, 258–269. [Google Scholar] [CrossRef]
- Simko, M.D.; Cowell, C.; Hreha, M. Practical Nutrition: A Quick Reference for the Health Care Practitioner; Aspen Publishers: Rockville, MD, USA, 1989; pp. 282–286. [Google Scholar]
- Reimann, C.; Filzmoser, P.; Garret, R.G.; Dutter, R. Statistical Data Analysis Explained: Applied Environmental Statistics with R; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Institute for Public Health (IPH) 2017. National Health and Morbidity Survey (NHMS) 2017: Adolescent Nutrition Survey 2017, Malaysia. Available online: http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2017/NutritionSurveyNHMS2017.pdf (accessed on 18 August 2018).
- Obidual Hug, A.K.; Chowdhury, T.; Roy, P.; Formuzul Haque, K.M.; Bellal Hossain, M. Healthcare facilities and nutritional status of orphans residing in selected orphanage in capital city of Bangladesh. Int. J. Curr. Microbiol. Appl. Sci. 2013, 2, 118–125. [Google Scholar]
- Nwaeri, D.U.; Omuemu, V.O. Intestinal helminthiasis and nutritional status of children living in orphanages in Benin–City, Nigeria. Int. J. Clin. Pract. 2013, 16, 243–248. [Google Scholar]
- Sadik, A. Orphanage children in Ghana: Are their dietary needs met? Pak. J. Nutr. 2010, 9, 844–852. [Google Scholar] [CrossRef]
- Jayasekera, C.R. Nutritional status of children under five in three State foster care institutions in Sri Lanka. Ceylon Med. J. 2006, 51, 63–65. [Google Scholar] [CrossRef]
- Bismarck, E.C.; Onyeka, E.B.; Mildred, U.O.; Nnaemeka, I.A. Nutritional status of children living in motherless babies’ homes in Enugu State Southeast Nigeria. Indian J. Appl. Res. 2014, 4, 478–482. [Google Scholar] [CrossRef]
- CDC. About Child & Teen BMI: Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html (accessed on 20 September 2015).
- Goldfield, G.S.; Moore, C.; Henderson, K.; Buchholz, A.; Obeid, N.; Flament, M.F. Body dissatisfaction, dietary restraint, depression, and weight status in adolescents. J. Sch. Health 2010, 80, 186–192. [Google Scholar] [CrossRef]
- Yen, C.F.; Hsiao, R.C.; Ko, C.H.; Yen, J.Y. The relationship between overweight/obesity and self-esteem in adolescents: The moderating effects of socio-demographic characteristics, family support, academic achievement and peer interaction. Taiwan J. Psychiatry 2010, 24, 210–221. [Google Scholar]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Wardle, J.; Williamson, S.; Johnson, F.; Edwards, C. Depression in adolescent obesity: Cultural moderators of the association between obesity and depressive symptoms. Int. J. Obes. 2006, 30, 634–643. [Google Scholar] [CrossRef]
- Faith, M.S.; Matz, P.E.; Jorge, M.A. Obesity-depression associations in the population. J. Psychosom. Res. 2002, 53, 935–942. [Google Scholar] [CrossRef]
- Fara Wahida, R.; Chin, Y.S.; Barakatun Nisak, M.Y. Obesity-related behaviors of Malaysian adolescents: A sample from Kajang district of Selangor state. Nutr. Res. Pract. 2012, 6, 458–465. [Google Scholar]
- Woon, F.C.; Chin, Y.S.; Mohd Nasir, M.T. Association between behavioural factors and BMI-for-age among early adolescents in Hulu Langat district, Selangor, Malaysia. Obes. Res. Clin. Pract. 2015, 9, 346–356. [Google Scholar] [CrossRef]
- Anuar Zaini, M.Z.; Lim, C.T.; Low, W.Y.; Harun, F. Factors affecting nutritional status of Malaysian primary school children. Asia Pac. J. Public Health 2005, 17, 71–80. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, S. Prevalent change in overweight and obesity in children and adolescents from 1995 to 2005 in Shandong, China. Asia Pac. J. Public Health 2005, 23, 904–916. [Google Scholar] [CrossRef]
- Nazrat, M.M.; Dawnavan Davis, M.S.; Yanovski, J.A. Body dissatisfaction, self-esteem, and overweight among innercity Hispanic children and adolescents. J. Adolesc. Health 2005, 36, 267.e16-20. [Google Scholar]
- Ozmen, D.; Ozmen, E.; Ergin, D.; Cetinkaya, A.C.; Sen, N.; Dundar, P.E.; Taskin, E.O. The association of self-esteem, depression and body satisfaction with obesity among Turkish adolescents. BMC Public Health 2007, 7, 80. [Google Scholar] [CrossRef]
- Chin, Y.S.; Taib, M.N.; Shariff, Z.M.; Khor, G.L. Development of Multidimensional Body Image Scale for Malaysian female adolescents. Nutr. Res. Pract. 2008, 2, 85–92. [Google Scholar] [CrossRef]
- Nur Syuhada Zofiran, M.J.; Kartini, I.; Siti Sabariah, B.; Ajau, D. The relationship between eating behaviours, body image, and BMI status among adolescents age 13 to 17 years in Meru, Klang, Malaysia. Am. J. Food Nutr. 2011, 1, 185–192. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and unhealthy weight control behaviors during adolescence: Associations with 10-year changes in body mass index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef]


{kind=link}
| Psychological Factors | Boys (n = 158) | Girl (n = 149) | Total (N = 307) | t/χ2 | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | n (%) | Mean ± SD | n (%) | Mean ± SD | n (%) | |||
| Self-esteem | 18.7 ± 3.9 | 17.6 ± 3.4 | 18.2 ± 3.7 | 2.565 a | 0.011 * | |||
| Low | 25 (15.8) | 25 (16.8) | 50 (16.3) | |||||
| Normal | 133 (84.2) | 124 (83.2) | 257 (83.7) | |||||
| Depressive disorders | 16.0 ± 7.7 | 16.9 ± 7.7 | 16.5 ± 7.7 | −1.045 a | 0.297 | |||
| No likelihood of a depressive disorder | 105 (66.5) | 84 (56.4) | 189 (61.6) | |||||
| High likelihood of a depressive disorder | 53 (33.5) | 65 (43.6) | 118 (38.4) | |||||
| Perception of body shape | −0.5 ± 1.5 | 0.8 ± 1.7 | 0.1 ± 1.7 | −7.185 a | 0.0001 * | |||
| Satisfied | 50 (31.6) | 33 (22.1) | 83 (27.0) | |||||
| Dissatisfied | 108 (68.4) | 116 (77.9) | 224 (73.0) | |||||
| Perception of body weight status | 2.242 b | 0.326 | ||||||
| Correct-estimator | 79 (50.0) | 86 (57.7) | 165 (53.7) | |||||
| Over-estimator | 13 (8.2) | 13 (8.7) | 26 (8.5) | |||||
| Under-estimator | 66 (41.8) | 50 (33.6) | 116 (37.8) | |||||
| Socio-Demographic Factors | BMI-for-Age (z-Score) | r/t/F-Value | p-Value |
|---|---|---|---|
| Mean ± SD | |||
| Age of respondents | 0.169 b | 0.003 * | |
| Sex | −2.833 c | 0.0001 * | |
| Boys | −0.36 ± 1.54 | ||
| Girls | 0.26 ± 1.23 | ||
| Ethnicity | 5.358 d | 0.001 * | |
| Malay | 0.01 ± 1.37 | ||
| Chinese | 0.60 ± 1.26 | ||
| Indian | −0.43 ± 1.47 | ||
| Others a | −0.19 ± 1.61 | ||
| Enrollment status | 5.926 d | 0.003 * | |
| Orphan | −0.12 ± 1.51 | ||
| Abandoned | 0.39 ± 1.25 | ||
| Problematic family | −0.41 ± 1.30 | ||
| Psychological Factors | BMI-for-Age (z-Score) | r/F-Value | p-Value |
|---|---|---|---|
| Mean ± SD | |||
| Self-esteem | −0.112 a | 0.003 * | |
| Likelihood of depressive disorders | 0.092 a | 0.109 | |
| Body shape dissatisfaction | 0.551 a | 0.0001 * | |
| Perception of body weight status | 6.523 b | 0.002 * | |
| Under-estimator | 0.25 ± 1.60 | ||
| Correct-estimator | −0.16 ± 1.22 | ||
| Over-estimator | −0.77 ± 1.56 | ||
| Variables | Unstandardized Coefficients | Standardized Coefficients | t | ∆R2 | p-Value | |
|---|---|---|---|---|---|---|
| β | Standard Error | Beta | ||||
| (Constant) | −0.796 | 0.131 | −6.063 | 0.0001 * | ||
| Body shape dissatisfaction | 0.457 | 0.038 | 0.549 | 12.126 | 0.304 | 0.0001 * |
| Underestimation of body weight status | 0.628 | 0.134 | 0.213 | 4.691 | 0.048 | 0.0001 * |
| Malay | 0.492 | 0.145 | 0.172 | 3.396 | 0.017 | 0.001 * |
| Chinese | 0.678 | 0.214 | 0.158 | 3.162 | 0.016 | 0.002 * |
| Abandoned status | 0.409 | 0.164 | 0.122 | 2.489 | 0.012 | 0.013 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
A Rahim, N.N.; Chin, Y.S.; Sulaiman, N. Socio-Demographic Factors and Body Image Perception Are Associated with BMI-For-Age among Children Living in Welfare Homes in Selangor, Malaysia. Nutrients 2019, 11, 142. https://doi.org/10.3390/nu11010142
A Rahim NN, Chin YS, Sulaiman N. Socio-Demographic Factors and Body Image Perception Are Associated with BMI-For-Age among Children Living in Welfare Homes in Selangor, Malaysia. Nutrients. 2019; 11(1):142. https://doi.org/10.3390/nu11010142
Chicago/Turabian StyleA Rahim, Nur Nabilla, Yit Siew Chin, and Norhasmah Sulaiman. 2019. "Socio-Demographic Factors and Body Image Perception Are Associated with BMI-For-Age among Children Living in Welfare Homes in Selangor, Malaysia" Nutrients 11, no. 1: 142. https://doi.org/10.3390/nu11010142
APA StyleA Rahim, N. N., Chin, Y. S., & Sulaiman, N. (2019). Socio-Demographic Factors and Body Image Perception Are Associated with BMI-For-Age among Children Living in Welfare Homes in Selangor, Malaysia. Nutrients, 11(1), 142. https://doi.org/10.3390/nu11010142