The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment

 ,
,
Abstract
:1. Introduction
2. The Assessment of Food Intake
2.1. The Food Records
2.2. The 24 h Recall
2.3. The Food Frequency Questionnaire
3. Studies Focused on Food Intake in Patients Awaiting LT
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL clinical practice guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed]
- Burra, P.; Giannini, E.G.; Caraceni, P.; Ginanni Corradini, S.; Rendina, M.; Volpes, R.; Toniutto, P. Specific issues concerning the management of patients on the waiting list and after liver transplantation. Liver Int. 2018, 38, 1338–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamboni, M.; Mazzali, G.; Fantin, F.; Rossi, A.; Di Francesco, V. Sarcopenic obesity: A new category of obesity in the elderly. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Angulo, P.; Meza-Junco, J.; Prado, C.M.; Sawyer, M.B.; Beaumont, C.; Esfandiari, N.; Ma, M.; Baracos, V.E. Sarcopenic obesity and myosteatosis are associated with higher mortality in patients with cirrhosis. J. Cachexia Sarcopenia Muscle 2016, 7, 126–135. [Google Scholar] [CrossRef]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International society for hepatic encephalopathy and nitrogen metabolism consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef]
- Norman, K.; Kirchner, H.; Lochs, H.; Pirlich, M. Malnutrition affects quality of life in gastroenterology patients. World J. Gastroenterol. 2006, 12, 3380–3385. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, Z.; Zhang, H.; Zhang, M.; Qiu, M.; Yuan, W. Italian multicentre cooperative project on nutrition in liver cirrhosis. Nutritional status in cirrhosis. J. Hepatol. 1994, 21, 317–325. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Terry, M.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef]
- Merli, M.; Giusto, M.; Gentili, F.; Novelli, G.; Ferretti, G.; Riggio, O.; Corradini, S.G.; Siciliano, M.; Farcomeni, A.; Attili, A.F.; et al. Nutritional status: Its influence on the outcome of patients undergoing liver transplantation. Liver Int. 2010, 30, 208–214. [Google Scholar] [CrossRef]
- Harrison, J.; McKiernan, J.; Neuberger, J.M. A prospective study on the effect of recipient nutritional status on outcome in liver transplantation. Transpl. Int. 1997, 10, 369–374. [Google Scholar] [CrossRef]
- McCoy, S.M.; Campbell, K.L.; Lassemillante, A.-C.M.; Wallen, M.P.; Fawcett, J.; Jarrett, M.; Macdonald, G.A.; Hickman, I.J. Changes in dietary patterns and body composition within 12 months of liver transplantation. Hepatobiliary Surg. Nutr. 2017, 6, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunati, M.E.; Grancini, V.; Agnelli, F.; Gattic, S.; Masserinia, B.; Zimbalattia, D.; Pugliesed, G.; Rossic, G.; Donatob, M.F.; Colombob, M.; et al. Metabolic syndrome after liver transplantation: Short-term prevalence and pre- and post-operative risk factors. Dig. Liver Dis. 2013, 45, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Ney, M.; Gramlich, L.; Mathiesen, V.; Bailey, R.J.; Haykowsky, M.; Ma, M.; Abraldes, J.G.; Tandon, P. Patient-perceived barriers to lifestyle interventions in cirrhosis. Saudi J. Gastroenterol. 2017, 23, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bémeur, C.; Butterworth, R.F. Reprint of: Nutrition in the management of Cirrhosis and its neurological complications. J. Clin. Exp. Hepatol. 2015, 5, S131–S140. [Google Scholar] [CrossRef]
- Borhofen, S.M.; Gerner, C.; Lehmann, J.; Fimmers, R.; Görtzen, J.; Hey, B.; Geiser, F.; Strassburg, C.P.; Trebicka, J. The royal free hospital-nutritional prioritizing tool is an independent predictor of deterioration of liver function and survival in Cirrhosis. Dig. Dis. Sci. 2016, 61, 1735–1743. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- García-Rodríguez, M.T.; López-Calviño, B.; Piñon-Villar, M.D.C.; Otero-Ferreiro, A.; Suárez-López, F.; Gómez-Gutiérrez, M.; Pértega-Díaz, S.; Seoane-Pillado, M.T.; Pita-Fernández, S. Concordance among methods of nutritional assessment in patients included on the waiting list for liver transplantation. J. Epidemiol. 2017, 27, 469–475. [Google Scholar] [CrossRef]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.M.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101, S73–S85. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.J.; Kim, M.K.; Hwang, S.H.; Ahn, Y.; Shim, J.E.; Kim, D.H. Relative validities of 3-day food records and the food frequency questionnaire. Nutr. Res. Pract. 2010, 4, 142. [Google Scholar] [CrossRef]
- De Keyzer, W.; Huybrechts, I.; De Vriendt, V.; Vandevijvere, S.; Slimani, N.; Van Oyen, H.; De Henauw, S. Repeated 24-hour recalls versus dietary records for estimating nutrient intakes in a national food consumption survey. Food Nutr. Res. 2011, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talegawkar, S.A.; Tanaka, T.; Maras, J.E.; Ferrucci, L.; Tucker, K.L. Validation of nutrient intake estimates derived using a semi-quantitative FFQ against 3 day diet records in the Baltimore Longitudinal Study of Aging. J. Nutr. Health Aging 2015, 19, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Amorim Cruz, J.A. Selection of methodology to assess food intake. Eur. J. Clin. Nutr. 2002, 56, S25–S32. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, L.G.; Santos, L.F.; Anastácio, L.R.; Lima, A.S.; Correia, M.I.T.D. Resting energy expenditure, body composition, and dietary intake. Transplantation 2013, 96, 579–585. [Google Scholar] [CrossRef]
- Brito-Costa, A.; Pereira-Da-Silva, L.; Papoila, A.L.; Alves, M.; Mateus, É.; Nolasco, F.; Barroso, E. Factors associated with changes in body composition shortly after orthotopic liver transplantation: The potential influence of immunosuppressive agents. Transplantation 2016, 100, 1714–1722. [Google Scholar] [CrossRef]
- Merli, M.; Giusto, M.; Riggio, O.; Gentili, F.; Molinaro, A.; Francesco Attili, A.; Ginanni Corradini, S.; Rossi, M. Improvement of nutritional status in malnourished cirrhotic patients one year after liver transplantation. e-SPEN 2011, 6, e142–e147. [Google Scholar] [CrossRef] [Green Version]
- Marr, K.J.; Shaheen, A.A.; Lam, L.; Stapleton, M.; Burak, K.; Raman, M. Nutritional status and the performance of multiple bedside tools for nutrition assessment among patients waiting for liver transplantation: A Canadian experience. Clin. Nutr. ESPEN 2017, 17, 68–74. [Google Scholar] [CrossRef]
- Andrade, C.P.R.; Portugal, M.L.T.; de Sousa Paz, E.; Freitas, P.A.; Daltro, A.F.C.S.; Almondes, K.G.S.; Maia, C.S.C.; Oliveira, A.C. Influence of liver transplantation in the nutritional profile of severe cirrhotic patients. Nutr. Hosp. 2018, 35, 104–109. [Google Scholar] [CrossRef]
- Ferreira, L.G.; Ferreira Martins, A.I.; Cunha, C.E.; Anastácio, L.R.; Lima, A.S.; Correia, M.I.T.D. Negative energy balance secondary to inadequate dietary intake of patients on the waiting list for liver transplantation. Nutrition 2013, 29, 1252–1258. [Google Scholar] [CrossRef]
- Ferreira, L.G.; Santos, L.F.; Silva, T.R.; Anastácio, L.R.; Lima, A.S.; Correia, M.I.T.D. Hyper- and hypometabolism are not related to nutritional status of patients on the waiting list for liver transplantation. Clin. Nutr. 2014, 33, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Richardson, R.A.; Garden, O.J.; Davidson, H.I. Reduction in energy expenditure after liver transplantation. Nutrition 2001, 17, 585–589. [Google Scholar] [CrossRef]
- Ferreira, L.G.; Anastácio, L.R.; Lima, A.S.; Correia, M.I.T.D. Malnutrition and inadequate food intake of patients in the waiting list for liver transplant. Rev. Assoc. Med. Bras. 2009, 55, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Palmese, F.; Giannone, F.A.; Bolondi, I.; Baldassarre, M.; Zaccherini, G.; Tufoni, M.; Boffelli, S.; Berardi, S.; Trevisani, F.; Caraceni, P. Low adherence to nutritional recommendations in patients with Cirrhosis : A prospective observational study. J. Gastroenterol. Hepatol. Res. 2019, 8, 2896–2902. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Salvini, S.; Parpinel, M. Food Composition Database for Epidemiological Studies in Italy. Available online: http://www.bda-ieo.it/ (accessed on 15 May 2019).
- Tsiaousi, E.T.; Hatzitolios, A.I.; Trygonis, S.K.; Savopoulos, C.G. Malnutrition in end stage liver disease: Recommendations and nutritional support. J. Gastroenterol. Hepatol. 2008, 23, 527–533. [Google Scholar] [CrossRef]

{kind=link}
| Nutritional Recommendations | |
|---|---|
| Energy | 35 kcal/kg body weight 1 |
| Protein | 1.2–1.5 g/kg body weight 2 |
| Total Carbohydrates | 45–75% of caloric intake |
| Simple Carbohydrates | 10–15% of caloric intake |
| Fibers | 25–45 g/daily |
| Lipids | 20–30% of caloric intake |
| Special Considerations | |
| Hepatic Encephalopathy | Increase BCAAs and decrease ammonia intake |
| Ascites | Fluid restriction and low-sodium intake (<2 g/day) |
| Advantages | Disadvantages | |
|---|---|---|
| Food Records |
|
|
| 24 h Recall |
|
|
| FFQ |
|
|
| Authors | n | Tool | Total Energy Intake (kcal/Day) | Carbohydrates (g) | Protein (g) | Lipids (g) |
|---|---|---|---|---|---|---|
| Ferreira et al. [25] | 17 | 3d-FR | 1670.5 ± 489.8 * | 236.5 | 72.9 | 48.2 |
| Lunati et al. [12] | 84 | 3d-FR | 2006 ± 624 * | 285.9 | 75.2 | 62.4 |
| Brito-Costa et al. [26] | 56 | 24 hR | 2062.8 ± 797.8 * | 259.4 | 94.9 | 71.5 |
| Mc Coy et al. [11] | 17 | 7d-FR | 2257.2 ± 605.9 * | 281 | 132.6 | 73 |
| Merli et al. [27] | 25 | ‡ | 2030 (1610–2870) † | − | 63 | − |
| Marr et al. [28] | 70 | 3d-FR | 1766.4 * | − | − | − |
| Andrade et al. [29] | 23 | 24 hR | 1774.3 ± 537.9 * | 234.5 | 93.6 | 53.9 |
| Ney et al. [13] | 630 | 2d-FR + FFQ | − | − | 68.8 | − |
| Ferreira et al. [30] | 73 | 3d-FR | 1485.1 (559.3–3432) † | 218.1 | 60.5 | 42.8 |
| Merli et al. [9] | 38 | ‡ | 2006 ± 423 * | − | − | − |
| Ferreira et al. [31] | 16 | 3d-FR | 1520 (576–2713.6) † | − | − | − |
| Richardson et al. [32] | 23 | 3d-FR | 1542 ± 124 * | 199 | 60.3 | 62.3 |
| Ferreira et al. [33] | 159 | 24 hR | 1490.9 ± 580.7 * | 225.7 | 56 | 36.7 |
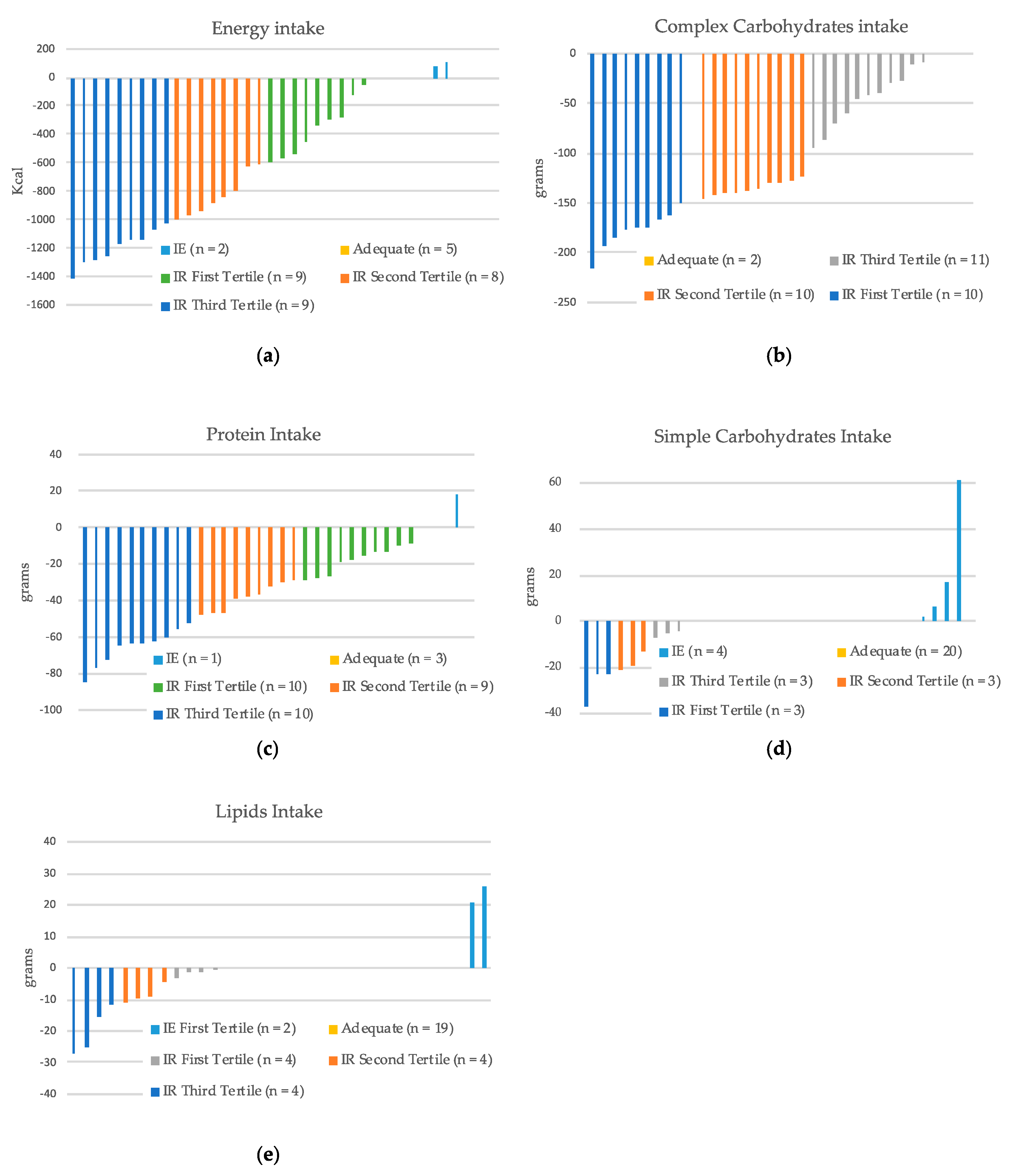
| Energy and Macronutrients Intake | Adequate | Inadequate Reduced | Inadequate Excessive |
|---|---|---|---|
| Total energy intake | 5 (15%) | 26 (79%) | 2 (6%) |
| Protein intake | 3 (9%) | 29 (88%) | 1 (3%) |
| Complex carbohydrates intake | 2 (6%) | 31 (94%) | 0 (0%) |
| Lipids intake | 19 (58%) | 12 (36%) | 2 (6%) |
| Simple carbohydrate intake | 20 (61%) | 9 (27%) | 4 (12%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmese, F.; Bolondi, I.; Giannone, F.A.; Zaccherini, G.; Tufoni, M.; Baldassarre, M.; Caraceni, P. The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment. Nutrients 2019, 11, 2462. https://doi.org/10.3390/nu11102462
Palmese F, Bolondi I, Giannone FA, Zaccherini G, Tufoni M, Baldassarre M, Caraceni P. The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment. Nutrients. 2019; 11(10):2462. https://doi.org/10.3390/nu11102462
Chicago/Turabian StylePalmese, Francesco, Ilaria Bolondi, Ferdinando Antonino Giannone, Giacomo Zaccherini, Manuel Tufoni, Maurizio Baldassarre, and Paolo Caraceni. 2019. "The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment" Nutrients 11, no. 10: 2462. https://doi.org/10.3390/nu11102462
APA StylePalmese, F., Bolondi, I., Giannone, F. A., Zaccherini, G., Tufoni, M., Baldassarre, M., & Caraceni, P. (2019). The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment. Nutrients, 11(10), 2462. https://doi.org/10.3390/nu11102462