Enteral Nutrition in Patients with Inflammatory Bowel Disease. Systematic Review, Meta-Analysis, and Meta-Regression

 ,
,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Review
2.1.1. Inclusion and Exclusion Criteria
2.1.2. Search Equation
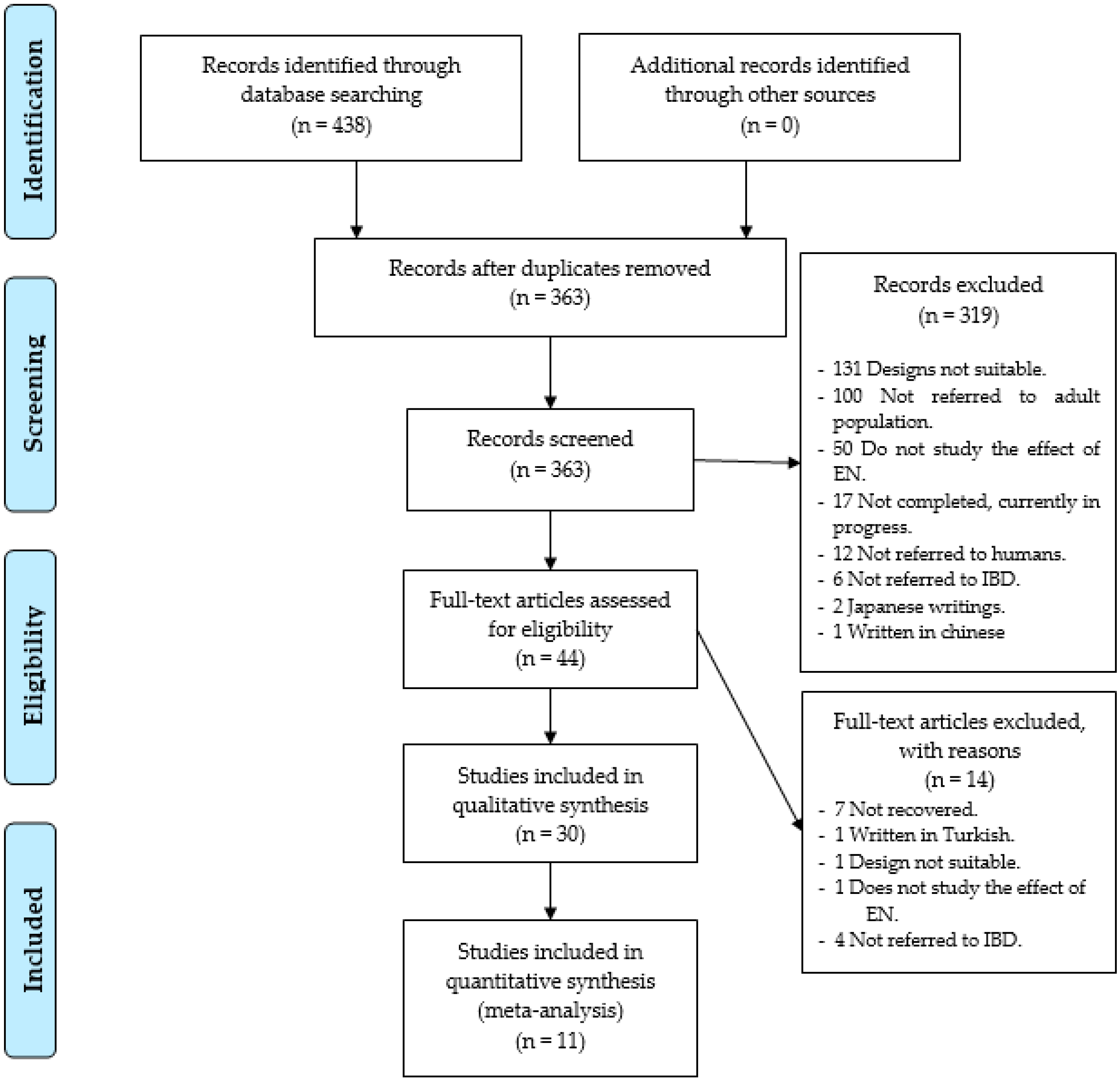
2.1.3. Selection Process
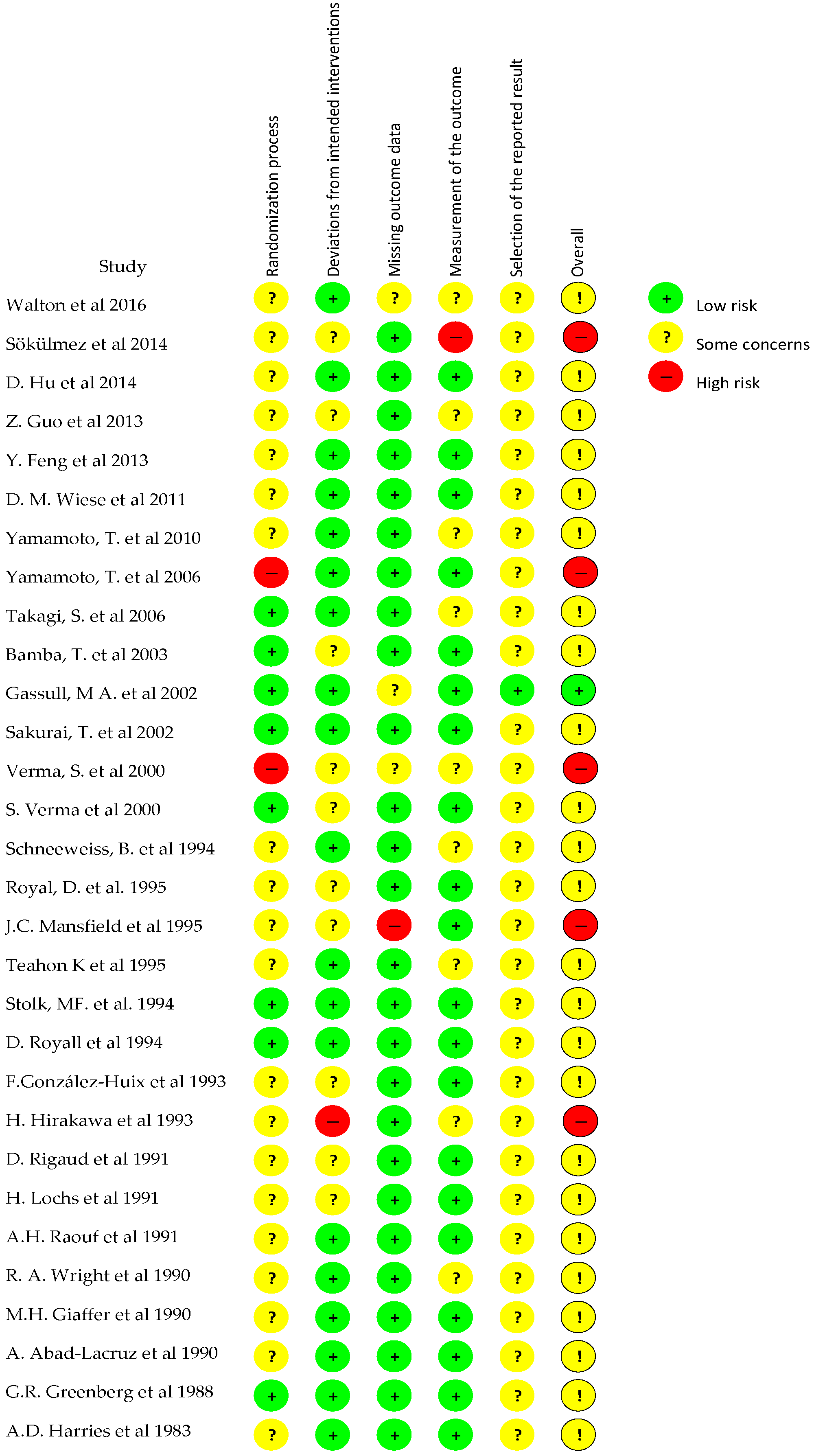
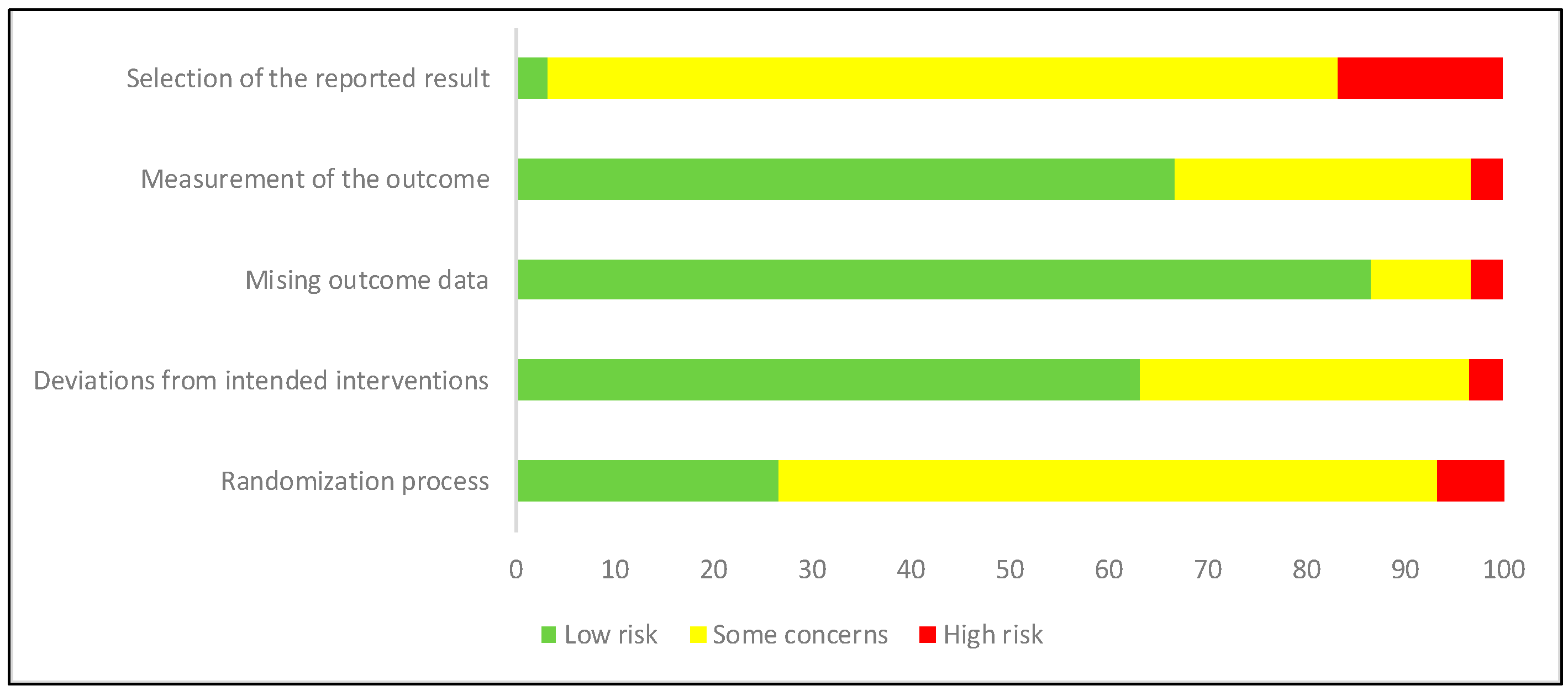
2.1.4. Evaluation of the Quality of the Studies
2.2. Meta-Analysis and Meta-Regression
3. Results
3.1. Systematic Review
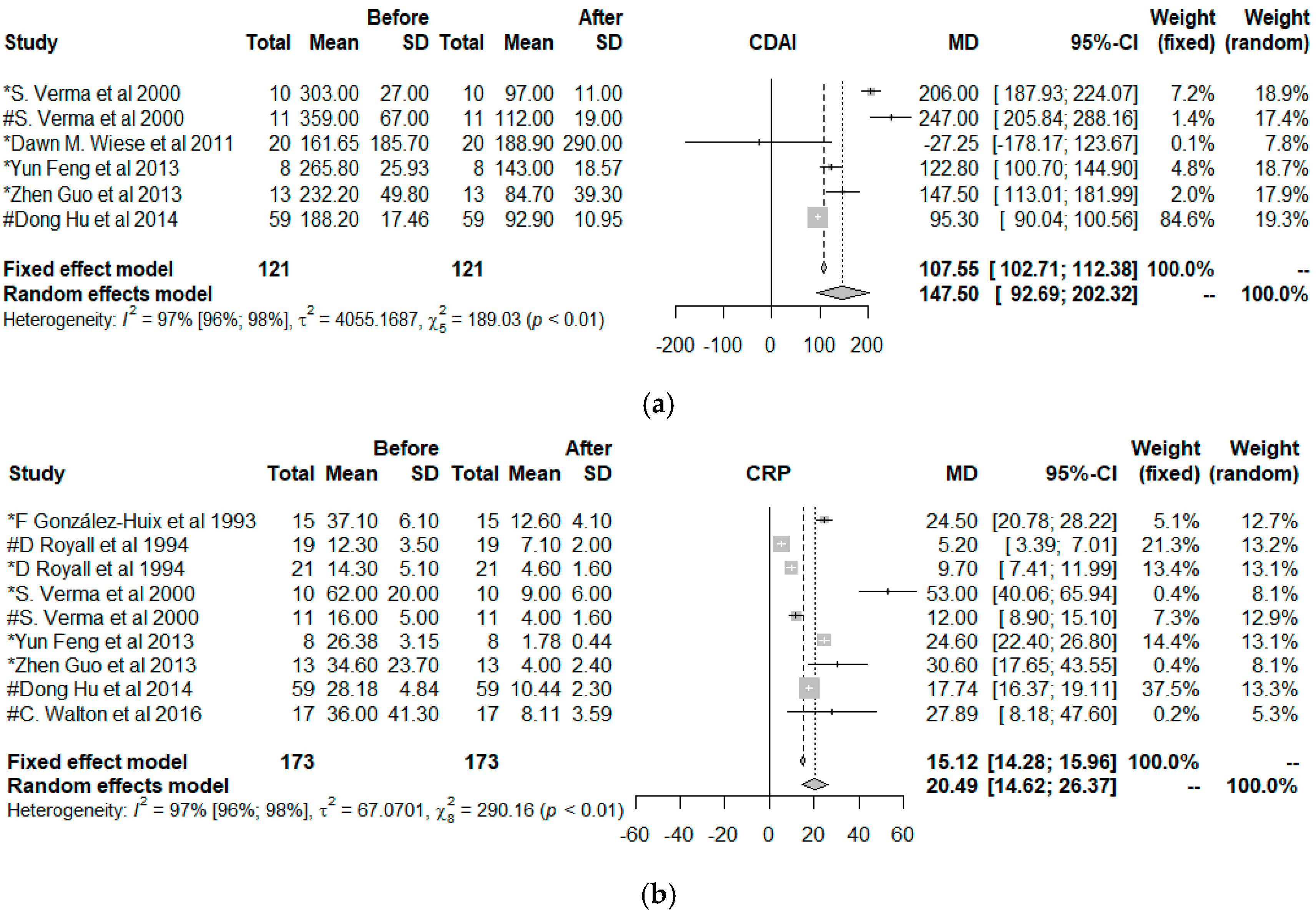
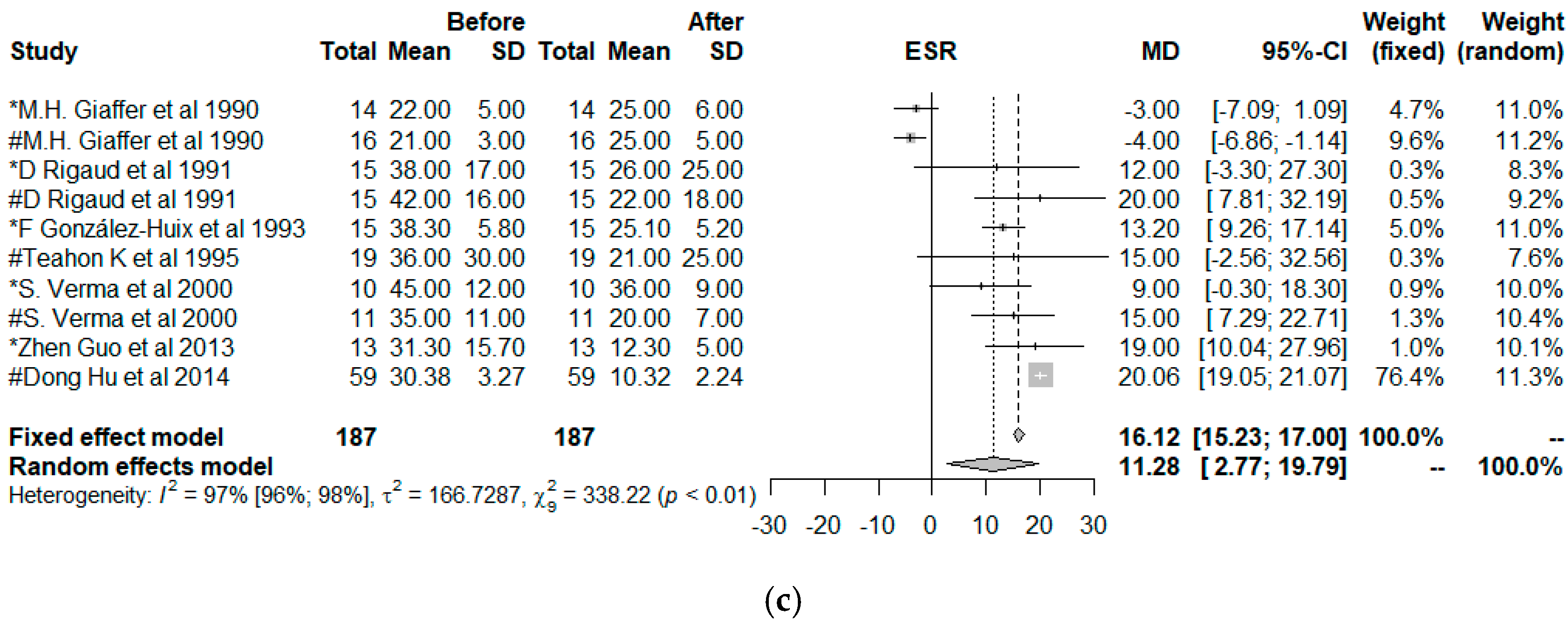
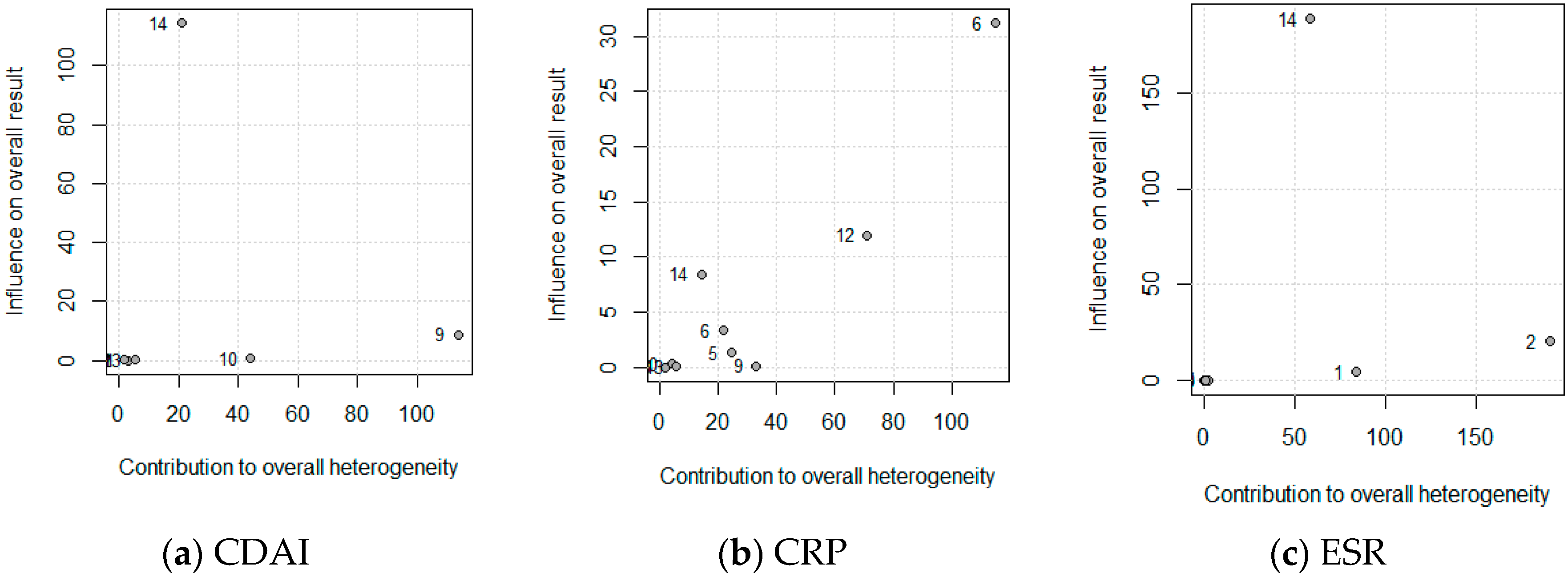
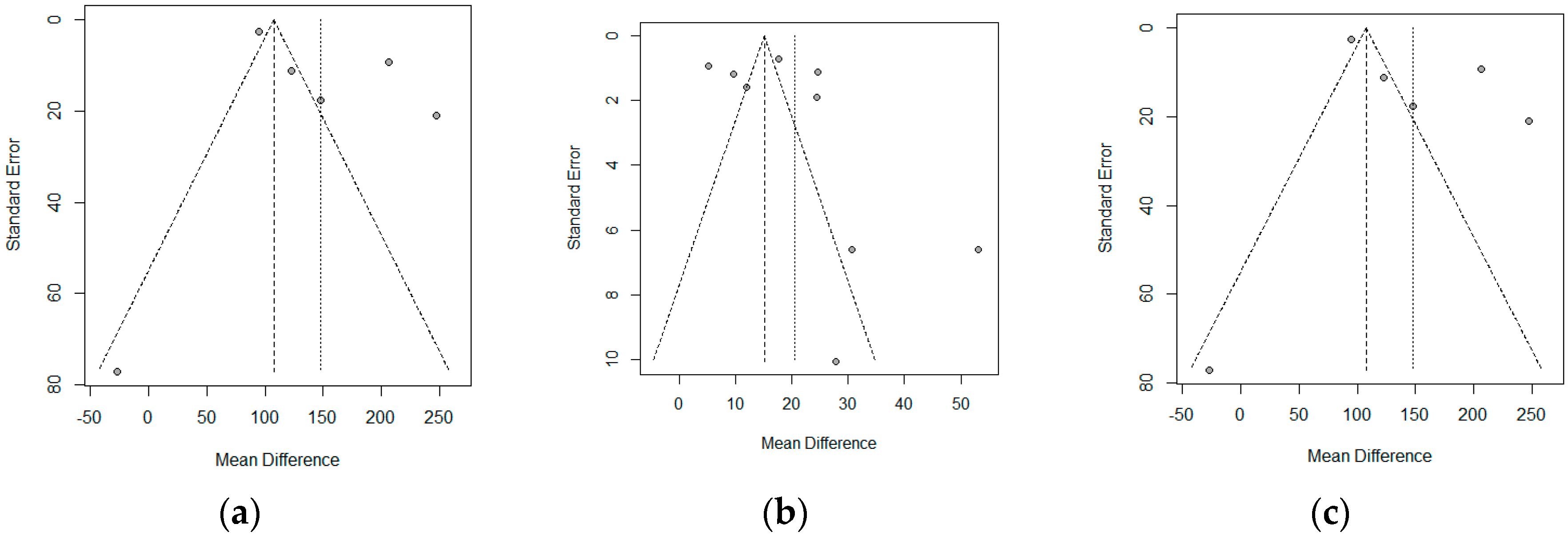
3.2. Meta-Analysis and Meta-Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Celiberto, L.S.; Graef, F.A.; Healey, G.R.; Bosman, E.S.; Jacobson, K.; Sly, L.M.; Vallance, B.A. Inflammatory bowel disease and immunonutrition: Novel therapeutic approaches through modulation of diet and the gut microbiome. Immunology 2018, 155, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.J.; Cho, J.H.; Gevers, D.; Chu, H. Genetic Factors and the Intestinal Microbiome Guide Development of Microbe-Based Therapies for Inflammatory Bowel Diseases. Gastroenterology 2019, 156, 2174–2189. [Google Scholar] [CrossRef] [PubMed]
- Coward, S.; Clement, F.; Benchimol, E.I.; Bernstein, C.N.; Avina-Zubieta, J.A.; Bitton, A.; Carroll, M.W.; Hazlewood, G.; Jacobson, K.; Jelinski, S.; et al. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology 2019, 156, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Reddavide, R.; Rotolo, O.; Caruso, M.G.; Stasi, E.; Notarnicola, M.; Miraglia, C.; Nouvenne, A.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F.; et al. The role of diet in the prevention and treatment of inflammatory bowel diseases. Acta Biomed. 2018, 89, 60–75. [Google Scholar]
- Eom, T.; Kim, Y.S.; Choi, C.H.; Sadowsky, M.J.; Unno, T. Current understanding of microbiota- and dietary-therapies for treating inflammatory bowel disease. J. Microbiol. 2018, 56, 189–198. [Google Scholar] [CrossRef]
- Abegunde, A.T.; Muhammad, B.H.; Bhatti, O.; Ali, T. Environmental risk factors for inflammatory bowel diseases: Evidence based literature review. World J. Gastroenterol. 2016, 22, 6296–6317. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Romero-Mosquera, B.; Hernandez, V. Diet, Gut Microbiome and Epigenetics: Emerging Links with Inflammatory Bowel Diseases and Prospects for Management and Prevention. Nutrients 2017, 9, 962. [Google Scholar] [CrossRef]
- Ruemmele, F.M. Role of Diet in Inflammatory Bowel Disease. Ann. Nutr. Metab. 2016, 68, 33–41. [Google Scholar] [CrossRef]
- Walton, C.; Montoya, M.P.; Fowler, D.P.; Turner, C.; Jia, W.; Whitehead, R.N.; Griffiths, L.; Waring, R.H.; Ramsden, D.B.; Cole, J.A.; et al. Enteral feeding reduces metabolic activity of the intestinal microbiome in Crohn’s disease: An observational study. Eur. J. Clin. Nutr. 2016, 70, 1052–1056. [Google Scholar] [CrossRef]
- Kakodkar, S.; Mutlu, E.A. Diet as a Therapeutic Option for Adult Inflammatory Bowel Disease. Gastroenterol. Clin. N. Am. 2017, 46, 745–767. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.; Duerksen, D.R. Enteral nutrition in the management of pediatric and adult crohn’s disease. Nutrients 2018, 10, 537. [Google Scholar] [CrossRef] [PubMed]
- Guagnozzi, D.; González-Castillo, S.; Olveira, A.; Lucendo, A.J. Nutritional treatment in inflammatory bowel disease. An update. Rev. Esp. Enferm. Dig. 2012, 104, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Baujat, B.; Mahé, C.; Pignon, J.P.; Hill, C. A graphical method for exploring heterogeneity in meta-analyses: Application to a meta-analysis of 65 trials. Stat. Med. 2002, 21, 2641–2652. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A Nonparametric “Trim and Fill” Method of Accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar]
- Copas, J.B.; Shi, J.Q. A sensitivity analysis for publication bias in systematic reviews. Stat. Methods Med. Res. 2001, 10, 251–265. [Google Scholar] [CrossRef]
- Schwarzer, G. meta: An R package for meta-analysis. R News 2007, 7, 40–45. [Google Scholar]
- Schwarzer, G.; Carpenter, J.R.; Rüker, G. Metasens: Advanced Statistical Methods to Model and Adjust for Bias in Meta-Analysis. R package version 0.4-0. 2019. Available online: https://CRAN.R-project.org/package=metasens (accessed on 29 October 2019).
- Sokulmez, P.; Demirbag, A.E.; Arslan, P.; Disibeyaz, S. Effects of enteral nutritional support on malnourished patients with inflammatory bowel disease by subjective global assessment. Turk. J. Gastroenterol. 2014, 25, 493–507. [Google Scholar] [CrossRef]
- Hu, D.; Ren, J.; Wang, G.; Li, G.; Liu, S.; Yan, D.; Gu, G.; Zhou, B.; Wu, X.; Chen, J.; et al. Exclusive enteral nutritional therapy can relieve inflammatory bowel stricture in Crohn’s disease. J. Clin. Gastroenterol. 2014, 48, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Wu, R.; Zhu, W.; Gong, J.; Zhang, W.; Li, Y.; Gu, L.; Li, N.; Li, J. Effect of exclusive enteral nutrition on health-related quality of life for adults with active Crohn’s disease. Nutr. Clin. Pract. 2014, 28, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Li, Y.; Mei, S.; Zhang, L.; Gong, J.; Gu, L.; Zhang, W.; Zhu, W.; Li, N.; Li, J. Exclusive enteral nutrition ameliorates mesenteric adipose tissue alterations in patients with active Crohn’ s disease. Clin. Nutr. 2013, 33, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Wiese, D.M.; Lashner, B.A.; Lerner, E.; Demichele, S.J.; Seidner, D.L. The effects of an oral supplement enriched with fish oil, prebiotics, and antioxidants on nutrition status in Crohn’s disease patients. Nutr. Clin. Pract. 2011, 26, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Matsumoto, K. Prospective clinical trial: Enteral nutrition during maintenance infliximab in Crohn’s disease. J. Gastroenterol. 2010, 45, 24–29. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Kitagawa, T.; Matsumoto, K. Impact of long-term enteral nutrition on clinical and endoscopic recurrence after resection for Crohn’s disease: A prospective, non-randomized, parallel, controlled study. Aliment. Pharmacol. Ther. 2007, 25, 67–72. [Google Scholar] [CrossRef]
- Takagi, S.; Utsunomiya, K.; Kuriyama, S.; Yokoyama, H.; Takahashi, S.; Iwabuchi, M.; Takahashi, H.; Takahashi, S.; Kinouchi, Y.; Hiwatashi, N.; et al. Effectiveness of an “half elemental diet” as maintenance therapy for Crohn’s disease: A randomized-controlled trial. Aliment. Pharmacol. Ther. 2006, 24, 1333–1340. [Google Scholar] [CrossRef]
- Bamba, T.; Shimoyama, T.; Sasaki, M.; Tsujikawa, T.; Fukuda, Y.; Koganei, K.; Hibi, T.; Iwao, Y.; Munakata, A.; Fukuda, S.; et al. Dietary fat attenuates the benefits of an elemental diet in active Crohn’s disease: A randomized, controlled trial. Eur. J. Gastroenterol. Hepatol. 2003, 15, 151–157. [Google Scholar] [CrossRef]
- Gassull, M.A.; Fernández-Bañares, F.; Cabré, E.; Papo, M.; Giaffer, M.H.; Sánchez-Lombraña, J.L.; Richart, C.; Malchow, H.; González-Huix, F.; Esteve, M. Fat composition may be a clue to explain the primary therapeutic effect of enteral nutrition in Crohn’s disease: Results of a double blind randomised multicentre European trial. Gut 2002, 51, 164–168. [Google Scholar] [CrossRef]
- Sakurai, T.; Matsui, T.; Yao, T.; Takagi, Y.; Hirai, F.; Aoyagi, K.; Okada, M. Short-term efficacy of enteral nutrition in the treatment of active Crohn’s disease: A randomized, controlled trial comparing nutrient formulas. JPEN J. Parenter. Enteral Nutr. 2002, 26, 98–103. [Google Scholar] [CrossRef]
- Verma, S.; Kirkwood, B.; Brown, S.; Giaffer, M.H. Oral nutritional supplementation is effective in the maintenance of remission in Crohn’s disease. Dig. Liver Dis. 2000, 32, 769–774. [Google Scholar] [CrossRef]
- Verma, S.; Brown, S.; Kirkwood, B.; Giaffer, M.H.H. Polymeric versus elemental diet as primary treatment in active Crohn’s disease: A randomized, double-blind trial. Am. J. Gastroenterol. 2000, 95, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, B.; Lochs, H.; Zauner, C.; Fischer, M.; Wyatt, J.; Maier-Dobersberger, T.; Schneider, B. Energy and substrate metabolism in patients with active Crohn’s disease. J. Nutr. 1999, 129, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Royall, D.; Greenberg, G.R.; Allard, J.P.; Baker, J.P.; Jeejeebhoy, K.N. Total enteral nutrition support improves body composition of patients with active Crohn’s disease. JPEN J. Parenter. Enteral Nutr. 1995, 19, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, J.C.; Giaffer, M.H.; Holdsworth, C.D. Controlled trial of oligopeptide versus amino acid diet in treatment of active Crohn’s disease. Gut 1995, 36, 60–66. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Teahon, K.; Pearson, M.; Smith, T.; Bjarnason, I. Alterations in nutritional status and disease activity during treatment of crohn’s disease with elemental diet. Scand. J. Gastroenterol. 1995, 30, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Stolk, M.F.; Van Erpecum, K.J.; Hiemstra, G.; Jansen, J.B.; Van Berge-Henegouwen, G.P. Gallbladder motility and cholecystokinin release during long-term enteral nutrition in patients with Crohn’s disease. Scand. J. Gastroenterol. 1994, 29, 934–939. [Google Scholar] [CrossRef]
- Royall, D.; Jeejeebhoy, K.N.; Baker, J.P.; Allard, J.P.; Habal, F.M.; Cunnane, S.C.; Greenberg, G.R. Comparison of amino acid v peptide based enteral diets in active Crohn’s disease: Clinical and nutritional outcome. Gut 1994, 35, 783–787. [Google Scholar] [CrossRef]
- Gonzalez-Huix, F.; de Leon, R.; Fernandez-Banares, F.; Esteve, M.; Cabre, E.; Acero, D.; Abad-Lacruz, A.; Figa, M.; Guilera, M.; Planas, R.; et al. Polymeric enteral diets as primary treatment of active Crohn’s disease: A prospective steroid controlled trial. Gut 1993, 34, 778–782. [Google Scholar] [CrossRef]
- Hirakawa, H.; Fukuda, Y.; Tanida, N.; Hosomi, M.; Shimoyama, T. Home elemental enteral hyperalimentation (HEEH) for the maintenance of remission in patients with Crohn’s disease. Gastroenterol. JPN 1993, 28, 379–384. [Google Scholar] [CrossRef]
- Rigaud, D.; Cosnes, J.; Le Quintrec, Y.; René, E.; Gendre, J.P.; Mignon, M. Controlled trial comparing two types of enteral nutrition in treatment of active Crohn’s disease: Elemental versus polymeric diet. Gut 1991, 32, 1492–1497. [Google Scholar] [CrossRef] [PubMed]
- Lochs, H.; Steinhardt, H.J.R.G.; Klaus-wentz, B.; Zeitz, M.; Vogelsang, H.; Sommer, H.; Fleig, W.E.; Bauer, P.; Schirrmeister, J.R.G.; Malchow, H. Comparison of Enteral Nutrition and Drug Treatment in Active Crohn’ s Disease Cooperative. Gastroenterology 1991, 101, 881–888. [Google Scholar] [CrossRef]
- Raouf, A.H.; Hildrey, V.; Daniel, J.; Walker, R.J.; Krasner, N.; Elias, E.; Rhodes, J.M. Enteral feeding as sole treatment for Crohn’s disease: Controlled trial of whole protein v amino acid based feed and a case study of dietary challenge. Gut 1991, 32, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.A.; Adler, E.C. Peripheral parenteral nutrition is no better than enteral nutrition in acute exacerbation of Crohn’s disease: A prospective trial. J. Clin. Gastroenterol. 1990, 12, 396–399. [Google Scholar] [CrossRef]
- Giaffer, M.H.; North, G.; Holdsworth, C.D. Controlled trial of polymeric versus elemental diet in treatment of active Crohn’s disease. Lancet 1990, 335, 816–819. [Google Scholar] [CrossRef]
- Abad-Lacruz, A.; González-Huix, F.; Esteve, M.; Fernández-Bañares, F.; Cabré, E.; Boix, J.; Acero, D.; Humbert, P.; Gassull, M.A. Liver function tests abnormalities in patients with inflammatory bowel disease receiving artificial nutrition: A prospective randomized study of total enteral nutrition vs total parenteral nutrition. JPEN J. Parenter. Enteral Nutr. 1990, 14, 618–621. [Google Scholar] [CrossRef]
- Greenberg, G.R.; Fleming, C.R.; Jeejeebhoy, K.N.; Rosenberg, I.H.; Sales, D.; Tremaine, W.J. Controlled trial of bowel rest and nutritional support in the management of Crohn’s disease. Gut 1988, 29, 1309–1315. [Google Scholar] [CrossRef]
- Harries, A.D.; Jones, L.A.; Danis, V.; Fifield, R.; Heatley, R.V.; Newcombe, R.G.; Rhodes, J. Controlled trial of supplemented oral nutrition in Crohn’s disease. Lancet 1983, 1, 887–890. [Google Scholar] [CrossRef]
- Cuív, P.Ó.; Begun, J.; Keely, S.; Lewindon, P.J.; Morrison, M. Towards an integrated understanding of the therapeutic utility of exclusive enteral nutrition in the treatment of Crohn’s disease. Food Funct. 2016, 7, 1741–1751. [Google Scholar] [CrossRef]
- Dupont, B.; Dupont, C.; Justum, A.-M.; Piquet, M.-A.; Reimund, J.-M. Enteral nutrition in adult Crohn’s disease: Present status and perspectives. Mol. Nutr. Food Res. 2008, 52, 875–884. [Google Scholar] [CrossRef]
- Halmos, E.P.; Gibson, P.R. Dietary management of IBD—insights and advice. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Ruemmele, F.M.; Pigneur, B.; Garnier-Lengliné, H. Enteral Nutrition as Treatment Option for Crohn’s Disease: In Kids Only? Nestle Nutr. Inst. Workshop Ser. 2014, 79, 115–123. [Google Scholar] [PubMed]
- Rubio, A.; Pigneur, B.; Garnier-Lengliné, H.; Talbotec, C.; Schmitz, J.; Canioni, D.; Goulet, O.; Ruemmele, F.M. The efficacy of exclusive nutritional therapy in paediatric Crohn’s disease, comparing fractionated oral vs. continuous enteral feeding. Aliment. Pharmacol. Ther. 2011, 33, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Mohri, T.; Matsuda, H.; Kubo, N.; Inadome, N.; Nakamori, Y.; Fujimi, S.; Yoshioka, T. The effect on glycemic control of a low-carbohydrate, high-fat enteral formula in critically ill patients admitted to a trauma and critical care center. Nihon Kyukyu Igakukai Zasshi 2011, 22, 871–877. [Google Scholar] [CrossRef][Green Version]
- Wewalka, M.; Drolz, A.; Zauner, C. Influence of fat-based versus glucose-based enteral nutrition formulas on glucose homeostasis. Crit. Care 2013, 17, P250. [Google Scholar]
- Lubbers, T.; Luyer, M.D.P.; de Haan, J.-J.; Hadfoune, M.; Buurman, W.A.; Greve, J.W.M. Lipid-Rich Enteral Nutrition Reduces Postoperative Ileus in Rats via Activation of Cholecystokinin-Receptors. Ann. Surg. 2009, 249, 481–487. [Google Scholar] [CrossRef]
- Tan, S.-J.; Yu, C.; Yu, Z.; Lin, Z.-L.; Wu, G.-H.; Yu, W.-K.; Li, J.-S.; Li, N. High-fat enteral nutrition reduces intestinal mucosal barrier damage after peritoneal air exposure. J. Surg. Res. 2016, 202, 77–86. [Google Scholar] [CrossRef]
- Xie, C.; Lin, J.; Su, J.; Ren, J. Synergistic effect of enteral nutrition on remission induction in a patient with penetrating Crohn disease. Medicine 2019, 98, e16750. [Google Scholar] [CrossRef]
- Lochs, H.; Steinhardt, H.J.; Klaus-Wentz, B.; Zeitz, M.; Vogelsang, H.; Sommer, H.; Fleig, W.E.; Bauer, P.; Schirrmeister, J.; Malchow, H. Comparison of enteral nutrition and drug treatment in active Crohn’s disease. Results of the European Cooperative Crohn’s Disease Study. IV. Gastroenterology 1991, 101, 881–888. [Google Scholar] [CrossRef]
- Papi, C.; Fascì-Spurio, F.; Rogai, F.; Settesoldi, A.; Margagnoni, G.; Annese, V. Mucosal healing in inflammatory bowel disease: Treatment efficacy and predictive factors. Dig. Liver Dis. 2013, 45, 978–985. [Google Scholar] [CrossRef]
- Armuzzi, A.; Van Assche, G.; Reinisch, W.; de Chambrun, G.P.; Griffiths, A.; Sladek, M.; Preiss, J.C.; Lukas, M.; D’Haens, G. Results of the 2nd scientific workshop of the ECCO (IV): Therapeutic strategies to enhance intestinal healing in inflammatory bowel disease. J. Crohn’s Colitis 2012, 6, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Nahidi, L.; Day, A.S.; Lemberg, D.A.; Leach, S.T. Differential effects of nutritional and non-nutritional therapies on intestinal barrier function in an in vitro model. J. Gastroenterol. 2012, 47, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Teahon, K.; Smethurst, P.; Pearson, M.; Levi, A.J.; Bjarnason, I. The effect of elemental diet on intestinal permeability and inflammation in Crohn’s disease. Gastroenterology 1991, 101, 84–89. [Google Scholar] [CrossRef]
- Ahmad, S.J.; Khan, A.; Madhotra, R.; Exadaktylos, A.K.; Milioto, M.E.; Macfaul, G.; Rostami, K. Semi-elemental diet is effective in managing high output ileostomy; a case report. Gastroenterol. Hepatol. Bed Bench 2019, 12, 169–173. [Google Scholar] [PubMed]
- Rostami, K.; Al Dulaimi, D. Elemental diets role in treatment of high ileostomy output and other gastrointestinal disorders. Gastroenterol. Hepatol. Bed Bench 2015, 8, 71–76. [Google Scholar]
- Damas, O.M.; Garces, L.; Abreu, M.T. Diet as Adjunctive Treatment for Inflammatory Bowel Disease: Review and Update of the Latest Literature. Curr. Treat. Options Gastroenterol. 2019, 17, 313–325. [Google Scholar] [CrossRef]
- Voitk, A.J.; Echave, V.; Feller, J.H.; Brown, R.A.; Gurd, F.N. Experience with elemental diet in the treatment of inflammatory bowel disease. Is this primary therapy? Arch. Surg. 1973, 107, 329. [Google Scholar] [CrossRef]
- Ruemmele, F.M.; Roy, C.C.; Levy, E.; Seidman, E.G. Nutrition as primary therapy in pediatric Crohn’s disease: Fact or fantasy? J. Pediatr. 2000, 136, 285–291. [Google Scholar] [CrossRef]
- Johnson, T.; Macdonald, S.; Hill, S.M.; Thomas, A.; Murphy, M.S. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: A randomised controlled trial. Gut 2006, 55, 356–361. [Google Scholar] [CrossRef]
- Fell, J.M.; Paintin, M.; Arnaud-Battandier, F.; Beattie, R.M.; Hollis, A.; Kitching, P.; Donnet-Hughes, A.; MacDonald, T.T.; Walker-Smith, J.A. Mucosal healing and a fall in mucosal pro-inflammatory cytokine mRNA induced by a specific oral polymeric diet in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2000, 14, 281–289. [Google Scholar] [CrossRef]
- Wedlake, L.; Slack, N.; Andreyev, H.J.N.; Whelan, K. Fiber in the treatment and maintenance of inflammatory bowel disease: A systematic review of randomized controlled trials. Inflamm. Bowel Dis. 2014, 20, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Scolapio, J.S. The Role of Total Parenteral Nutrition in the Management of Patients with Acute Attacks of Inflammatory Bowel Disease. J. Clin. Gastroenterol. 1999, 29, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Storck, L.J.; Imoberdorf, R.; Ballmer, P.E. Nutrition in Gastrointestinal Disease: Liver, Pancreatic, and Inflammatory Bowel Disease. J. Clin. Med. 2019, 8, 1098. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, A.M. Enteral Nutrition in the Management of Crohn’s Disease. J. Parenter. Enter. Nutr. 2005, 29, S108–S117. [Google Scholar] [CrossRef]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN guideline: Clinical nutrition in inflammatory bowel disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study | n/age | Disease | P/d | CC | Treatment | Variables | Main Results |
|---|---|---|---|---|---|---|---|---|
| Walton et al. 2016 [10] | UNRCT | 17/- | ACT CD | 14 | GB | Enteral feeding E028 extra (Elementary diet) | CRP, HBI and automated spectral identification in feces | The HBI decreased from 6.88 ± 2.93 to 4 ± 5.50, (p < 0.05), the CRP from 36.0 ± 41.3 mg/L to 8.11 ± 3.59 (p < 0.05), the concentration of 1-propanol and 1-butanol decreased too. No modifications in phenol and indole. The SCFA esters disappeared. |
| Pinar Sökülmez et al. 2014 [21] | RCCT | 38/37 M 28 F 10 | ACT IBD EG/CG: 15/23 CD EG/CG: 6/7 UC EG/CG: 9/16 | 21 | TR | EG/CG Diet and EN Novasource®/Unrestricted Diet | SGA, BMI, nausea, vomiting, bowel movements, change in malnutrition state, general status, and disease severity. | Although at the beginning of the study the proportion of patients with a severe UC in the EG was higher than in the CG (8/9, and 7/16 respectively), there were no significant differences at the end of the study (p > 0.05). In both groups the improvements in disease activity of patients with UC were significant, but non-significant positive changes were observed in the clinical findings during the hospitalization period. Significant improvements of the SGA in both groups. |
| Dong Hu et al. 2014 [22] | UNRCT | 59/32 M 42 F 17 | ACT CD | 84 | CN | Elemental formula Peptide (Nutricia) through nasogastric or nasointestinal tube, plus water and weak tea. | Symptoms, CDAI, peripheral blood samples. Laboratory tests, including nutritional parameters and inflammatory parameters and CT. | 50 patients achieved a partial remission, 30 a complete remission. 48 symptomatic remission, 35 radiological remission and 42 clinical remission. The CDAI decreased from 188.2 to 132.4 in 21 days (p < 0.05), and to 92.9 after 81 days (p < 0.05). Significant decrease in the thickness of the intestinal wall and an increase in the area of the luminal cross section. CRP and ESR decreased significantly (p < 0.05), the BMI, albumin, prealbumin and transferrin, HB, platelets, red blood cells, globulin and total protein increased significantly (p < 0.05). |
| Zhen Guo et al. 2013 [23] | UNRCT | 13/26 M = 9 F = 4 | ACT CD | 28 | CN | Exclusive EN through polymer formula Administration: Nasogastric tube at night and orally by day. They allowed water consumption. | IBDQ, CDAI, BMI, CRP, ESR, WBC count, HB and serum albumin level in peripheral venous blood. | 11 patients achieved clinical remission and 2 did not. CDAI and CRP decreased from 232.2 and 34.6 to 84.7 and 4.0 (p ≤ 0.001). Significantly decreased the number of liquid or soft stools, abdominal pain, general well-being and percentage deviation of the standard weight (p < 0.05), no differences were found in the presence of complications, taking atropine/diphenoxylate or opiates, presence of a mass abdominal and hematocrit. There were significant improvements in the IBDQ, from 128.3 to 182.9 (p < 0.001). Significant improvement in all categories: intestinal symptoms (from 41.5 to 62.0, p < 0.001), systemic symptoms (16.5 to 27.5, p < 0.001), social function (20.5 to 26.5, p = 0.03) and emotional state (49.8 to 66.9, p < 0.001). Correlation between IBDQ and CDAI after treatment (r = −0.57; p = 0.042). |
| Feng Y et al. 2013 [24] | NRCCT | 24/33 M 17 F 7 | ACT CD ENG/NoEN/CG 8/8/8 | 28 | CN | ENG: Enteral formula “Peptisorb” by nasogastric tube, plus water. NoENG: EC patients without EN. CG: Patients with colon carcinoma. | Adipocyte size, adipokine production and level of CRP were evaluated. Leptin, resistin, TNF, and IL-6 and IL-10 levels were determined. BMI, CDAI, etc. were calculated. | ENG patients had a higher BMI level and lower levels of CRP and CDAI (p < 0.001) and achieved clinical remission (CDAI < 150). In addition, protein levels of proinflammatory adipokines (TNF-alpha and leptin) were lower, leptin was negatively regulated, and adipokine expression (mRNA level) was positively regulated. In the NoEN group the level of adiponectin protein was higher |
| Dawn M. Wiese et al. 2011 [25] | NRCCT | 20/46 M 4 F 16 | ACT CD EPA>2%/EPA<2% 10/10 | 120 | US | Two 8-oz each day of NE EPA>2% or EPA<2% respectively. | CDAI, IBDQ, nutritional status, micronutrient levels, CRP and body composition among others were measured. | EPA > 2% group increased the BMI, fat mass, fat-free mass, IBDQ (+41.4 [23.1, 47.0]; p = 0.002) and the CDAI decreased (−47.8 [−65, −37.8]; p = 0.05). There were no differences between groups for the rest of the variables studied. |
| Takayuki Yamamoto et al. 2010 [26] | NRCCT | 56/32 M 36 F 20 | REM CD EG/CG 32/24 | 392 | JP | EG. Elemental formula “Elental” by nasogastric tube at night and low-fat foods during the day. CG. Unrestricted Diet | WBC, HB, hematocrit, platelet count, ESR, CRP and albumin. CDAI. Symptoms, adverse effects, stool parameters. | The CDAI did not decrease significantly. No differences were observed between the groups. (p = 0.51). The cumulative proportion of patients in clinical remission was not significantly different between the groups. |
| Takayuki Yamamoto et al. 2006 [27] | NRCCT | 40/32 M 26 F 14 | ACT CD EG/CG 20/20 | +365 | JP | EG: Elemental formula “Elental” by nasogastric tube at night and low-fat foods during the day. CG. Unrestricted Diet | WBC, HB, platelet count, ESR, CRP and albumin. CDAI and parameters by ileocolonoscopy. | During the year of follow-up, 1 patient of the EG and 7 in the CG developed clinical recurrence (p = 0.048). At 6 months, 5 patients of the EG and 8 of the CG developed endoscopic recurrence (odds ratio, 2.0; p = 0.50). At 12 months, 6 patients from the EG and 14 from the CG showed endoscopic recurrence (odds ratio, 5.4; p = 0.027) |
| S. Takagi et al. 2006 [28] | RCCT | 51/30 M 37 F 14 | REM CD EG/CG 26/25 | 730 | JP | EG: Half of calories, elementary diet through a enteral or oral intake and the remaining half by regular meals. CG: Unrestricted Diet | CDAI. Parameters of: feces, symptoms and laboratory tests. | After an average follow-up of 11.9 months, the relapse rate in the EG was significantly lower than in the CG [34.6% vs. 64.0%; Multivariate risk ratio 0.40 (95% CI: 0.16–0.98)]. No significant changes on the rest of the variables |
| Tadao Bamba et al. 2003 [29] | RCCT | 28/28 M 17 F 11 | ACT CD Low/ Medium/ High Fat EN 10/10/8 | 28 | JP | LOWG: 6 packages of elemental diet “Elental” and 6 packages of dextrin MEDG: 6 packages of elemental diet “Elemental”, 3 packages of dextrin and 3 packages of dextrin C-1 (dextrin + soybean oil). HIGHG: 6 packages of elemental diet "Elemental" and 6 packages of dextrin C-1. Administration: Nasogastric tube. | IOIBD, inflammatory markers (CRP, ESR) and body weight were recorded at each follow-up. | No differences in body weight gains. The LOWG’s IOIBD was significantly higher than in the MEDG and HIGHG groups (p = 0.048) and the CRP lower after the first week. In the MEDG and HIGHG groups the CRP fluctuated during the study. In the LOWG group the ESR decreased, but for the other groups they remained high or increased during the study. Clinical remission was achieved in 8, 4 and 2 patients in the LOWG, MEDG and HIGHG groups respectively. This remission rate is significant if grouped in LOWG vs. MEDG & HIGHG (p = 0.046). |
| M A Gassull et al. 2002 [30] | RCCT | 62/29 M 24 F 29 | ACT CD PEN1/PEN2/ESTG 20/23/19 | 28 | ES GB DE | PEN 1: Polymeric EN, rich in n9 monounsaturated fatty acids (MUFA) (oleic acid). PEN 2: Polymeric EN rich in n6 polyunsaturated fatty acids (PUFA) (linoleic acid) ESTG (Steroid group): Prednisone. | ESR, CRP, serum fibrinogen, VHAI, CDAI, NRI, serum albumin and grip strength | The intention-to-treat analysis showed that the remission rates were 20%, 52% and 79% for PEN1, PEN2 and ESTG (p = 0.001). Withdrawal from treatment, remission rates were 27%, 63% and 79%, respectively (p = 0.008). No differences in remission time and changes in activity rates, inflammatory biological parameters, NRIs and nutritional variables. |
| Toshihiro Sakurai et al. 2002 [31] | RCCT | 36/26 M 30 F 6 | ACT CD = 36 EDG/TLG 18/18 | 42 | JP | EDG: “Elental” Formula (Ajinomoto Pharma) low in fat. TLG: Twinline Formula (Otsuka Pharma) large amount of medium chain triglycerides Administration: Tube in the duodenum. | CDAI, VHAI, CRP, ESR, levels of: serum albumin, plasma prealbumin, plasma transferrin and retinol binding protein in plasma and triene/tetraeno ratio. | After 2 weeks, serum levels of linoleic acid, an omega 6 fatty acid, decreased significantly in the EDG group. Without significant differences was observed: a short-term remission in 67% in the EDG and 72% in the TLG, a reduction in the CDAI and the VHAI, a normalization of the CRP and an improvement in the ESR and levels serum; albumin, plasma prealbumin, plasma transferrin and plasma retinol binding protein, the linolenic acid levels decreased in both groups. |
| S. Verma et al. 2000 [32] | NRCCT | 39/40 M 12 F 27 | REM CD EG/CG 21/28 | 365 | GB | EG: Oral nutritional supplementation with elemental diet “EO28 Extra”, plus normal diet. CG: Unrestricted Diet. | CDAI, inflammatory markers such as CRP, ESR, albumin, HB and platelet count. | The intention-to-treat analysis showed that the remission rates were 48% and 22% for EG AND CG (p = 0.0003). Withdrawal from treatment, remission rates were 60%, and 22%, respectively (p < 0.00001). Without showing significant differences were observed: a stability of the levels of CDAI and albumin and an increase in BMI. A significant decrease in ESR was observed |
| Verma S et al. 2000 [33] | RCCT | 21/35 M 8 F 13 | ACT CD GA/GP 11/10 | 28 | UK | GA: Free amino acids diet. GP: Polymeric diet. Administration: nasogastric tube. Water was allowed. | CDAI, inflammatory markers (CRP, etc.), BMI and body weight. | Clinical remission was achieved in 8 (80%) and 6 (55%) patients in the GA and GP groups, respectively (without significant differences, p = 0.1). In both groups CDAI (GA, 359 ± 67 to 112 ± 19, p ≤ 0.0002; GP, 303 ± 27 to 97 ± 11, p ≤ 0.0005) and CRP (GA, 16 ± 5 to 4 ± 1.6, p < 0.1; GP, 62 ± 20 to 9 ± 6, p < 0.04) decreased. Remission was achieved earlier in GA (7 ± 2 days) than in GP (14 ± 2 days) (without significant differences). Overall, enteral feeding was successful in 14 patients (63%). |
| Bruno Schneeweiss et al. 1999 [34] | NRCCT | 26/28 M 9 F 17 | ACT CD EG/CG 7/19 | 15 | AT | EG: 7 patients received enteral nutrition by nasogastric tube | Energy expenditure, UNP, changes in the body’s urea nitrogen set and body composition. | The REE did not change. From day 7 the UNP, RQ and RQ without proteins increased significantly. These changes (except carbohydrate oxidation rates) were reversed when the EN was interrupted. |
| Dawna Royall et al. 1995 [35] | NRCCT | 60/30 M 32 F 28 | ACT CD EG/CG 30/30 | 21 | CA | EG: one of two elementary diets, Peptamen or Vivonex-TEN, administered by nasoduodenal tube. | Total body protein, fat, water and body potassium. | Compared to the CG, the EG lost 11.3 kg (p < 0.0005), (5.1 kg fat (p < 0.0005), 2.2 kg protein (p < 0.025), 3.7 kg water, 24.9 g body potassium (p < 0.01)). After EN, body weight (1.9 ± 0.3 kg; p < 0.0005), body protein (0.3 ± 0.1 kg; p < 0.025), fat (0.3 ± 0.1 kg; p < 0.025) and water (1.1 ± more; 0.4 kg; p < 0.025) was significantly increased. Body potassium increased but not significantly. |
| Mansfield JC et al. 1995 [36] | RCCT | 44/- M 16 F 28 | ACT CD GA/GP 22/22 | 28 | GB | GA: Enteral formula based on amino acids “Elemental 028”. GP: Enteral formula based on oligopeptide-based diet “Pepti-2000 LF liquid”. Water was allowed. | CDAI, laboratory activity measures (HB, platelet count, ESR, serum albumin concentration, AAGP and CRP) and body weight. | 16 patients (36.4%) achieved clinical remission and decreased CRP (p = 0.05). Both groups had identical rates of remission, failure, early withdrawal and nasogastric feeding intolerance. There was an increase in serum albumin in patients who started the study at a low level. |
| Teahon K et al. 1995 [37] | UNRCT | 19/37 M 10 F 9 | ACT CD | 35 | GB | Elemental diet “Vivonex” was using in one group (n = 8) and “Elemental 028” in the other (n = 11), by oral route. | CDAS, biochemical parameters (HB, platelet count, leukocytes, ESR, iron, magnesium, copper, zinc…), fecal parameters, BMI and body composition. | Changes were similar in both groups. Clinical disease activity and fecal excretion of leukocytes were significantly reduced after 2 weeks of treatment. Transferrin, prealbumin, albumin and serum iron were significantly increased at 4 weeks. Serum copper decreased during the study period. Changes in nutrition measures did not correlate significantly with changes in disease activity. |
| M.F.J. Stolk et al. 1994 [38] | UNRCT | 6/27 M 3 F 3 | CD | 42 | NL | By using a pump, the formula “Peptison” (Nutricia) was supplied. | Volume, motility, emptying and filling variables of the gallbladder were calculated, and concentration of CCK in the plasma | At the start of treatment, the fasting gallbladder volume decreased from 19.3 +/− 4.5 to 4.9 +/− 3.6 mL. The CCK increased from 1.5 +/− 0.3 to 3.9 +/− 1.1 pmol/L. After 8 days, the gallbladder contracted almost completely, the CCK increased to 7.5 +/− 2.7, and at 36 days, CCK increased to 8.3 +/− 2.6 pmol/L. After 22 days 22 the volume of the gallbladder increased, and after 46 the CCK decreased. This change was significantly greater than the CCK change on day 1 (p < 0.05) |
| D Royall et al. 1994 [39] | RCCT | 40/31 M 23 F 17 | ACT CD AG/PG 19/21 | 21 | CA | AG: Enteral formula based on amino acids “Vivonex-TEN”. PG: Enteral formula based on peptides “Peptamen”. Administered by nasogastric tube. Water was allowed. | CDAI, CRP, AAGP, phospholipids, albumin and transferrin. Body weight and total body nitrogen was evaluated. | After 21 days, remission rates were equivalent between the two groups: 84% for the AG and 75% for the PG (p = 0.38). At 12 months, it remained at 31% and 40% respectively (p = 0.39). Also, the reductions of CDAI, AAGP and CRP were significant. Linoleic acid decreased and total body nitrogen increased significantly in AG but not in PG (p < 0.025). The concentration of phospholipids in plasma increased significantly in the PG |
| F González-Huix et al. 1993 [40] | RCCT | 32/31 M 17 F15 | ACT CD PENG/ESTG 15/17 | 28 | ES | PENG: The polymeric EN administered by nasogastric tube. ESTG: Prednisone administration. And diet lactose-free while they were in the hospital. | VHAI, CRP. Evaluation of body weight, % IBW, MAMC, TSF, serum albumin concentration. Complete hematological and biochemical analysis. | There were no significant differences in the mean time (p = 0.47) and the number of patients who obtained clinical remission (p = 0.43). The VHAI decreased in both groups; PENG from 172.5 to 113.8, (p = 0.0001), ESTG from 184.3 to 118.1, (p = 0.0003). In both groups the CRP decreased and the serum albumin concentration increased significantly. After one year, 10 patients (66.6%) in the ESTG and 5 (41.6%) in the PENG relapsed. No differences in the cumulative probability of relapse. |
| Hiroyuki Hirakawa et al. 1993 [41] | NRCCT | 61/25 M 39 F 22 | REM CD ENG/ENG+D/DG/CG 25/22/8/6 | 60 | JP | ENG: Elemental EN (“Elental”) through nasoenteral tube. ENG+D: ½ ENG + ½ Low-fat diet and prednisolone DG: Low-fat diet and prednisolone CG: Unrestricted Diet | IOIBD, ESR and CRP | The cumulative rates of continuous remission after 1, 2 and 4 years were in the ENG 94%, 63% and 63%; in the ENG + D 75%, 66% and 66% in the DG 63%; 42% and 0%, and in the CG 50%, 33%. and 0%. The ENG had a higher rate than DG (p < 0.05) and CG (p < 0.01). The ENG + D had a higher rate than the CG (p < 0.05). Patients who received more than 30 kcal of EN showed a higher continuous remission rate (p < 0.001). |
| D Rigaud et al. 1991 [42] | RCCT | 30/35 M 18 F 12 | ACT CD EENG/PENG 15/15 | 28 | FR | EENG: Elementary enteral formula “Vivonex HN” PENG: “Realmentyl” polymeric formula | CDAI, fecal production, colonoscopies. Body weight; TSF, MAMC, daily urinary, creatinine-height ratio; blood levels of HB, albumin and transferrin. ESR, α2 globulin level and WBC counts. | The clinical remission was in the EENG of 66% and in the PENG of 73%. The CDAI and ESR levels were significantly reduced in both groups. There were no differences between groups for inflammatory markers, colonoscopic lesions, fecal production, body weight and creatinine index. |
| Herbert Lochs et al. 1991 [43] | RCCT | 107/29 M 37 F 70 | ACT CD OENG/CSG 55/52 | 42 | DE | OENG: Enteral nutrition by oligopetidic formula “Peptisorb” through nasogastric or nasoduodenal tube. More tea or water. CSG: Combination of corticosteroids and sulfasalazine. | CDAI and laboratory tests. | After 6 weeks, 29 patients achieved remission in the OENG and 41 patients in the CSG (p < 0.01). The remission time was significantly different (p < 0.01). A CDAI below 150 was achieved in the OENG in 24 patients and in the CSG in 35. The CDAI and severe malnutrition parameters showed no significant differences in patients in remission. |
| A.H. Raouf et al. 1991 [44] | RCCT | 24/- | ACT CD EENG/PENG 13/11 | 21 | GB | EENG: Enteral amino acid-based food “EO28” PENG: Whole protein-based whole food “Triosrbon”. Administration: Oral, flavored with Nesquick. | ESR, erythrocytes, VHAI, Bristol simple activity index and the CRP. | After 3 weeks, they reached remission in the EENG 9 patients and in the PENG 8 patients (p < 0.01). The Bristol simple activity index improved in the two groups (EENG; 91.7%, PENG; 86.7% (p = 0.35)), Similarly; VHAI (EENG; 18.5%, PENG; 30.0%, (p = 0.23)), and CRP (EENG; 58.3%, PENG; 57.1%, (p = 0.49)). |
| Richard A. Wright et al. 1990 [45] | RCCT | 11/- M 7 F 4 | ACT CD EENG/PNG 6/5 | 14 | US | EENG: Elemental enteral feeding “Vital” PNG: Determined peripheral parenteral nutrition. | CDAI, standard anthropometric parameters, nitrogen balance studies and chemical profiles. | CDAI improved significantly in both groups. Plasma transferrin levels and total lymphocyte count improved in the EENG group (p < 0.05). No significant differences in weight gain. |
| Giaffer MH et al. 1990 [46] | RCCT | 30/38 M 8 F 22 | ACT CD AG/PG 16/14 | 28 | UK | AG: Amino acid diet “Vivonex”. PG: Polymeric diet “Fortison”. Administration: nasogastric tube. Water was allowed. | CDAI, total body weight, MAMC, TSF and biochemical measurements such as serum albumin. | 12 (75%) AG patients achieved remission at 10 days, compared with 5 (35.8%) in the PG group (p = 0.03). CDAI decreased significantly in the AG group, not the PG group. The mean weight gain in both groups was similar. Mean serum albumin increased from 26 g/L to 33 g/L (p < 0.001). Also, there were significant changes in ESR and AAGP in both groups. |
| Abad-Lacruz A et al. 1990 [47] | RCCT | 22/32 M 15 F 14 | ACT IBD PG/TPNG 16/13 | NI | ES | PG: Polymeric diet high in nitrogen “UNIASA” by nasogastric tube. TPNG: Specific total parenteral nutrition by a central vein. | Biochemical measurements (total serum bilirubin, alkaline phosphatase, GGT, ALT, and AST) and VHAI and the Truelove and Witts index were measured. | PG had a significant increase in serum albumin concentration (32 ± 1 to 38.2 ± 1.6 g/L; p < 0.01). There was lower disease activity in both groups (3.31 ± 0.15 to 2.31 ± 0.24, p < 0.05 in GP; and 3.38 ± 0.21 to 2.61 ± 0.27, p < 0.05 in TPNG). 8 (5 CD and 3 UC) of 13 patients (61.5%) in the TPNG group developed abnormalities in LFT, while in the PG group only occurred in 1 of 16 patients (6.2%) (p = 0.002). |
| Greenberg GR et al. 1988 [48] | RCCT | 51/30 M 25 F 26 | ACT CD TPNG/ENG/PPNG 17/19/15 | 21 | CA | TPNG: Total parenteral nutrition, more water, plus daily one ampoule of vitamins. ENG: formula diet “Precision-Isotonic”. PPNG: Unrestricted diet and a partial protein/calorie parenteral nutrition. | CDAI, nutritional assessment and biochemical measurements (hematocrit, blood glucose, serum electrolytes, creatinine, magnesium and albumin). | The average CDAI decreased (p < 0.01) with no significant differences between groups. Remission rates to discharge were equivalent among the three groups: 12 patients in TPNG, 11 patients in ENG and 9 patients in PPNG and oral diet (X2 1.42 and 1.15; p = n/s). Remission rates of 42% in TPNG, 55% in EN and 56% in PPNG at 12 months were equivalent and not influenced by the type of nutritional support initially administered. At 12 months, 18 patients (35%) required surgery, 17 (34%) were medically treated for relapse, and 16 (31%) had sustained remission. |
| Harries AD et al. 1983 [49] | RCCT | 28/37 M 17 F 11 | ACT CD G1/G2 14/14 | 120 | GB | G1: 2 months ordinary diet followed by 2 months supplementation with the non-elementary low-waste formula “Guarantee Plus”. G2: same intervention than G1 with invested order. | Nutritional measurements (height, weight, MAMC and thickness of the skin fold), biochemical measurements (serum prealbumin, serum, red cell folate, creatinine height index, platelets, T lymphocytes, etc.) and urine tests parameters. | The general effect of EN during the 2 months was to increase serum albumin, serum protein and prealbumin levels, creatinine height index and T-lymphocyte count. With EN decreased levels of orosomucoids and serum alkaline phosphatase and its activity (p < 0.05) Patients felt better when they received EN, although their monthly symptom scores showed no significant benefit. |
| Meta-Analysis for: Effect Size (%Heterogeneity) | ||||||
|---|---|---|---|---|---|---|
| ID | Omitting | KN | n | CDAI | CRP | ESR |
| 1 | M.H. Giaffer et al. 1990 | Pol | 14 | 13.0 (96.8%) | ||
| 2 | M.H. Giaffer et al. 1990 | Elm | 16 | 13.1 (93.7%) | ||
| 3 | D. Rigaud et al. 1991 | Pol | 15 | 11.2 (97.6%) | ||
| 4 | D. Rigaud et al. 1991 | Elm | 15 | 10.4 (97.6%) | ||
| 5 | F. Glez.-Huix et al. 1993 | Pol | 15 | 20.0 (97.4%) | 11.1 (97.6%) | |
| 6 | D. Royall et al. 1994 | Elm | 19 | 22.2 (95.1%) | ||
| 7 | D. Royall et al. 1994 | Pol | 21 | 22.3 (97.4%) | ||
| 8 | Teahon K et al. 1995 | Elm | 19 | 11.0 (97.6%) | ||
| 9 | S. Verma et al. 2000 | Pol | 10 | 136.9 (94.0%) | 17.5 (97.3%) | 11.5 (97.6%) |
| 10 | S. Verma et al. 2000 | Elm | 11 | 128.0 (97.2%) | 21.9 (97.6%) | 10.9 (97.6%) |
| 11 | D. M. Wiese et al. 2011 | Pol | 20 | 162.3 (97.8%) | ||
| 12 | Yun Feng et al. 2013 | Pol | 8 | 150.3 (97.9%) | 19.7 (96.6%) | |
| 13 | Zhen Guo et al. 2013 | Pol | 13 | 146.7 (97.8%) | 19.6 (97.5%) | 10.4 (97.6%) |
| 14 | Dong Hu et al. 2014 | Elm | 59 | 162.7 (92.6%) | 21.5 (97.4%) | 9.8 (91.2%) |
| 15 | C. Walton et al. 2016 | Elm | 17 | 20.1 (97.6%) | ||
| Pooled estimate | 145.7 (97.4%) | 20.5 (97.2%) | 11.3 (97.4%) | |||
| Trim-and-Fill Method | Copas Method | |||||
|---|---|---|---|---|---|---|
| Fix Model | Random Model | Random Model | ||||
| Nº Studies | Effect Size Estimated 95%CI | Nº Studies | Effect Size Estimated 95%CI | Nº Studies | Effect Size Estimated 95%CI | |
| CDAI | 2 | 98.9 [43.9;153.8] | 0 | No Changes | 0 | No Changes |
| CRP | 3 | 15.3 [9.7;20.9] | 0 | No Changes | 4 | 18.0 [12.1;23.9] |
| ESR | 5 | 19.3 [11.2;27.4] | 0 | No Changes | 0 | No Changes |
| Result | Co-Variable | Test of Moderators | ||
|---|---|---|---|---|
| Intercep | KN * | QM | p-Value | |
| CDAI | 167.9 | −33.8 | 0.289 | 0.591 |
| CRP | 13.7 | 12.6 | 3.977 | <0.001 |
| ESR | 12.9 | −3.0 | 0.106 | 0.745 |
| Intercep | Age | QM | p-Value | |
| CDAI | 225.5 | −2.38 | 0.203 | 0.652 |
| CRP | 52.9 | −1.0 | 0.985 | 0.321 |
| ESR | 48.3 | −1.1 | 1.555 | 0.212 |
| Intercep | Period | QM | p-Value | |
| CDAI | 235.5 | −1.9 | 5.662 | 0.017 |
| CRP | 21.4 | −0.0 | 0.006 | 0.941 |
| ESR | 2.5 | 0.2 | 1.551 | 0.213 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comeche, J.M.; Caballero, P.; Gutierrez-Hervas, A.; García-Sanjuan, S.; Comino, I.; Altavilla, C.; Tuells, J. Enteral Nutrition in Patients with Inflammatory Bowel Disease. Systematic Review, Meta-Analysis, and Meta-Regression. Nutrients 2019, 11, 2657. https://doi.org/10.3390/nu11112657
Comeche JM, Caballero P, Gutierrez-Hervas A, García-Sanjuan S, Comino I, Altavilla C, Tuells J. Enteral Nutrition in Patients with Inflammatory Bowel Disease. Systematic Review, Meta-Analysis, and Meta-Regression. Nutrients. 2019; 11(11):2657. https://doi.org/10.3390/nu11112657
Chicago/Turabian StyleComeche, Jose M., Pablo Caballero, Ana Gutierrez-Hervas, Sofia García-Sanjuan, Iris Comino, Cesare Altavilla, and Jose Tuells. 2019. "Enteral Nutrition in Patients with Inflammatory Bowel Disease. Systematic Review, Meta-Analysis, and Meta-Regression" Nutrients 11, no. 11: 2657. https://doi.org/10.3390/nu11112657
APA StyleComeche, J. M., Caballero, P., Gutierrez-Hervas, A., García-Sanjuan, S., Comino, I., Altavilla, C., & Tuells, J. (2019). Enteral Nutrition in Patients with Inflammatory Bowel Disease. Systematic Review, Meta-Analysis, and Meta-Regression. Nutrients, 11(11), 2657. https://doi.org/10.3390/nu11112657