Abstract
There are well-recognised associations between excessive gestational weight gain (GWG) and adverse pregnancy outcomes, including an increased risk of pre-eclampsia, gestational diabetes and caesarean birth. The aim of the OPTIMISE randomised trial was to evaluate the effect of dietary and exercise advice among pregnant women of normal body mass index (BMI), on pregnancy and birth outcomes. The trial was conducted in Adelaide, South Australia. Pregnant women with a body mass index in the healthy weight range (18.5–24.9 kg/m2) were enrolled in a randomised controlled trial of a dietary and lifestyle intervention versus standard antenatal care. The dietitian-led dietary and lifestyle intervention over the course of pregnancy was based on the Australian Guide to Healthy Eating. Baseline characteristics of women in the two treatment groups were similar. There was no statistically significant difference in the proportion of infants with birth weight above 4.0 kg between the Lifestyle Advice and Standard Care groups (24/316 (7.59%) Lifestyle Advice versus 26/313 (8.31%) Standard Care; adjusted risk ratio (aRR) 0.91; 95% confidence interval (CI) 0.54 to 1.55; p = 0.732). Despite improvements in maternal diet quality, no significant differences between the treatment groups were observed for total GWG, or other pregnancy and birth outcomes.
1. Introduction
Obesity represents a significant global health burden, with the World Health Organisation highlighting the importance of weight gain prevention in adults of healthy weight, particularly among women of reproductive age [1]. In any given 5-year period, 20% of women of reproductive age have sufficient weight gain to progress them into a higher body mass index (BMI) category [2,3]. Furthermore, the rate of weight gain is highest (approximately 700 g per year) among women of normal BMI [4,5]. Pregnancy often represents a significant turning point in a woman’s cardiovascular and metabolic health trajectory secondary to pregnancy-related changes, including relative insulin resistance, which promotes weight gain [6], and risk of developing obesity subsequently [7,8].
There is substantial observational literature relating to gestational weight gain (GWG), which has been summarised by the Institute of Medicine (IoM) [9,10]. These recommendations advocate a GWG of 11.5 to 16.0 kg for women of normal body mass index (BMI 18.5–24.9 kg/m2) [9,10]. However, approximately 40% of women gain in excess of this amount [10]. There are well-recognised associations between excessive GWG and adverse pregnancy outcomes for the woman, including an increased risk of pre-eclampsia, gestational diabetes and caesarean birth [11,12,13,14]. There are also longer-term health consequences for women, including post-partum weight retention (PPWR) and development of obesity [15,16,17], with over 70% of women of normal BMI retaining more than 5 kg of weight 1 year after birth [18,19]. Women with excessive GWG also have a greatly increased risk of developing both diabetes [20,21] and cardiovascular disease in later life [22,23,24,25].
Excessive GWG is a well-recognised risk factor for high infant birth weight and is independently associated with an increased risk of child obesity in the offspring [26,27,28], thereby creating a vicious cycle in which the intergenerational effects of obesity are perpetuated [29]. Specifically, the risk of early childhood obesity increases by a factor of 1.08 (95% CI 1.03–1.14) per kilogram of maternal weight gained above the IoM recommendations [30]. Furthermore, it has been suggested that high maternal weight gain may induce a persisting susceptibility of an individual to an obesogenic environment [30,31]. There is also increasing evidence for an effect of excessive maternal GWG on subsequent cardiovascular risk and hypertension in children [27,32] and adolescents [33].
Despite recognition of the associations between excessive GWG in women of normal BMI during pregnancy and beyond, there is more limited information describing effective antenatal dietary interventions to optimise weight gain and improve health. In a systematic review of the literature, 12 randomised trials involving 2713 pregnant women were identified [34]. Of these trials, 8 specifically recruited 1048 women of normal BMI, although only 5 reported clinical outcomes (714 women) [34]. Providing a combined dietary and lifestyle intervention during pregnancy was associated with a modest 1.25 kg difference in weight gain (5 studies, 714 women) [34]. However, the effect on clinical pregnancy outcomes was less clear, being reported in only 2 trials, with 243 women [34].
The aim of the OPTIMISE randomised trial was therefore to evaluate the effect of dietary and exercise advice among pregnant women of normal BMI, on pregnancy and birth outcomes.
2. Materials and Methods
2.1. Trial Design
We conducted a randomised controlled trial, in which women with a BMI of 18.5 to 24.9 kg/m2, and a singleton pregnancy between 10 + 0–20 + 0 weeks were eligible to participate [35]. Women with a multiple pregnancy, or with diabetes (type 1 or type 2) diagnosed prior to pregnancy were excluded. Ethical approval was provided by the research ethics committee of the Women’s and Children’s Hospital (Adelaide, South Australia), approval number HREC/13/WCHN/152, and the study registered with the Australian and New Zealand Clinical Trials Registry (ACTRN 12614000583640). Recruitment to the trial commenced in June 2014.
Women were screened for eligibility at the time of their first antenatal appointment. All women presenting to the Women’s and Children’s Hospital had their height and weight measured, and BMI calculated by research staff. Eligible women were provided with information about the study and were counselled by a research assistant, prior to their provision of written consent to participate.
Randomisation: We used a computer-based randomisation service in the Discipline of Obstetrics and Gynaecology, The University of Adelaide. The randomisation schedule used balanced variable blocks with stratification for parity (0 versus 1 or more) and was prepared by an investigator who was not involved with recruitment or clinical care.
Women were randomised to either the ‘Lifestyle Advice Group’ or the ‘Standard Care Group’. Blinding of participants was not possible given the nature of the intervention, but where possible, antenatal care-providers, outcome assessors and data analysts were blinded to treatment allocation.
Treatment Allocation: Women randomised to the Lifestyle Advice Group received an intervention consisting of six sessions provided across the course of pregnancy. Three sessions were face-to-face, with two provided by the dietitian shortly after trial entry and again at 28 weeks’ gestation, and one provided by a research assistant at 36 weeks’ gestation. Women also received three telephone calls from the research assistant at 20, 24 and 32 weeks’ gestation. The dietary advice provided was consistent with current Australian dietary standards [36], while specifically maintaining a balance of carbohydrates, fat and protein, and encouraging women to reduce their intake of energy dense and non-core foods high in refined carbohydrates and saturated fats. Women were advised to increase their intake of fibre, and to consume two servings of fruit, five servings of vegetables and three servings of dairy each day [36,37,38].
Tailoring of the intervention was informed by stage theories of health decision making where an individual progresses through a series of cognitive phases when undertaking behavioural change [39]. The initial planning session with a research dietitian provided women with written dietary and activity information, an individual diet and physical activity plan, recipe book and example menu plans. Women were encouraged to set achievable goals for dietary and exercise change, supported to make these lifestyle changes and to self-monitor their progress, using a SMART goals approach. The SMART Goal approach includes setting goals that are specific, measurable, achievable, realistic and timely. Therefore, a SMART goal incorporates all of these criteria to increase the chances of goal achievement. These principles were reinforced at subsequent contacts with research staff [37,38].
Women who were randomised to the Standard Care Group received their antenatal care according to hospital guidelines, which did not include information relating to dietary intake, physical activity or weight gain during pregnancy.
All women were asked to complete a food frequency questionnaire, physical activity questionnaire and quality of life assessments at trial entry, 28 and 36 weeks’ gestation and six months postpartum. Each woman’s weight was recorded at trial entry and at 36 weeks’ gestation or nearest to birth, with gestational weight gain determined as the difference between weight at 36 weeks and trial entry. All women were offered a research ultrasound at 28 and 36 weeks’ gestation to assess foetal growth (results not presented in this manuscript). After birth, information relating to birth and infant outcomes was obtained from the case notes by the research assistant, who remained blinded to the woman’s allocated treatment group.
Consistent with state-wide clinical practice guidelines, all women were screened for gestational diabetes at approximately 28 weeks’ gestation [40]. During the course of the trial, diagnostic criteria for gestational diabetes changed across the state from a positive 75 g oral glucose tolerance test with fasting blood glucose > 5.5 mmol/L, or 2 h ≥ 7.8 mmol/L, to fasting blood glucose ≥ 5.1 mmol/L, 1 h ≥ 10.0 mmol/L, or 2 h ≥ 8.5 mmol/L [40]. Women diagnosed with gestational diabetes remained in the study and were offered treatment with further dietary modification and metformin or insulin added as required to maintain appropriate glycaemic control [40].
2.2. Outcome Measures
The primary trial outcome was the proportion of infants with birth weight > 4 kg. A range of secondary study outcomes were collected and listed below.
2.2.1. Secondary Infant Outcomes
Adverse outcomes for the infant: including preterm birth before 37 weeks’ gestation; perinatal mortality (either stillbirth (intrauterine foetal death after trial entry and prior to birth), or infant death (death of a live born infant prior to hospital discharge, and excluding lethal congenital anomalies)); infant birth weight; infant birth weight < 2500 g; infant birth weight > 4500 g; large for gestational age defined as infant birth weight > 90th percentile for gestational age and infant sex; small for gestational age defined as infant birth weight < 10th percentile for gestational age and infant sex; hypoglycaemia requiring intravenous treatment; admission to neonatal intensive care unit or special care baby unit; hyperbilirubinaemia requiring phototherapy; nerve palsy; fracture; birth trauma; shoulder dystocia; corticosteroid use; respiratory distress syndrome (with moderate or severe respiratory disease defined as mean airway pressure > 10 cm H2O and/or inspired oxygen fraction (FiO2) > 0.80 with ventilation) [41]; discharge home on oxygen; patent ductus arteriosus; proven systemic infection requiring treatment; retinopathy of prematurity; necrotising enterocolitis; neonatal encephalopathy [42]; seizures; length of hospital stay; and infant not exclusively breast fed at hospital discharge.
2.2.2. Maternal Antepartum, Labour and Birth Outcomes
Adverse outcomes for the woman: including maternal hypertension and pre-eclampsia (in accordance with recognised Australasian Society for the Study of Hypertension in Pregnancy criteria) [43]; maternal gestational diabetes; need for and length of antenatal hospital stay; antepartum haemorrhage requiring hospitalisation; preterm prelabour ruptured membranes; chorioamnionitis; need and reason for induction of labour; any antibiotic use during labour; caesarean section; postpartum haemorrhage (blood loss > 600 mL); perineal trauma; wound infection; endometritis; length of postnatal hospital stay; thromboembolic disease; maternal death.
2.2.3. Maternal Weight Change
Maternal weight changes: including total gestational weight gain; average weekly gestational gain; gestational weight gain below, within and above IoM recommendations [10]; and anthropometric assessment (skin-fold thickness measurement (SFTM), body circumferences and bio-impedance to assess adiposity).
2.2.4. Maternal Diet and Physical Activity
Maternal changes in diet and physical activity as measured by questionnaires completed by the woman at trial entry, 28 and 36 weeks’ gestation (Harvard Semi-quantitative Food Frequency Questionnaire [44,45], and the Short Questionnaire to Assess Health-enhancing physical activity (SQUASH) [46]).
2.2.5. Maternal Quality of Life
Maternal quality of life and emotional wellbeing as measured by questionnaires completed by the woman at trial entry, 28 weeks and 36 weeks’ gestation relating to quality of life (as measured using the SF12 Health Survey Questionnaire) [47]; preferences for treatment, satisfaction with care; anxiety (as measured by the Short Form Spielberger State Trait Inventory [48]) and depression (as measured by the Edinburgh Postnatal Depression Scale [49]).
2.3. Sample Size Estimate
The primary clinical endpoint was the incidence of infants born with birth weight > 4 kg, with an estimated incidence in women eligible for this trial of 8.72% [50]. To detect a difference from 8.72% to 3.89% (alpha 0.05; power 70%), we required 624 women.
2.4. Analysis and Reporting of Results
All analyses followed a pre-specified statistical analysis plan, as shown in Supplementary File 1. Baseline characteristics of all randomised women were examined descriptively as an indication of comparable treatment groups, and included maternal age, parity, race, height, weight, smoking status, past obstetric history and a diagnosis of previous gestational diabetes. Primary and secondary outcomes were analysed on an “intention to treat” basis, according to the treatment allocated (Lifestyle Advice or Standard Care) at the time of randomisation. Continuous outcomes were analysed using linear regression, and binary outcomes were analysed using log binomial regression. Outcomes measured at multiple time points included a time-by-treatment interaction term, with generalised estimating equations used to account for correlation between repeated measures.
As specified in the Statistical Analysis Plan, the primary analyses were adjusted analyses based on imputed data. Unadjusted analyses, and analyses on unimputed data (not presented), were also performed as secondary sensitivity analyses. Adjusted models included the stratification variable (parity) as well as BMI (continuous variable), smoking, socio-economic status (as indicated by the Australian Bureau of Statistics’ 2011 Socio-economic Index for Areas—Index of Relative Socio-economic Disadvantage (SEIFA IRSD) quintile) and maternal age at trial entry as covariates.
There was one missing value for the primary outcome and other infant birth weight outcomes; many other outcomes (including infant anthropometry, infant and maternal delivery data) had less than 1% missing data, while infant SFTM and other maternal antenatal measures had between 20–40% missing data. Multiple imputation by the fully conditional specification (chained equations) method was used to create 100 complete datasets for analysis [51]. The imputation model included all outcomes, all stratification variables, maternal baseline height, weight and gestational age, and maternal weight at 36 weeks’ gestation. Estimates were derived in the standard manner by combining the estimates from each imputation using Rubin’s rules [51]. As there was only one missing value for the primary outcome, no missing not at random (MNAR) sensitivity analyses were performed. Analyses were performed using Stata version 15 (StataCorp, 77845 Texas, USA).
Data cannot be made publicly available because of ethics and Institutional Review Board restrictions. However, researchers can apply for data access to the corresponding author.
3. Results
3.1. Participant Characteristics
Between June 2014 and April 2017, 2602 eligible women were approached to participate, with 645 randomised, 323 (50.1%) to Lifestyle Advice and 322 (49.9%) to Standard Care, as shown in Figure 1. Four women were randomised in error prior to the start of the trial (all four from the Lifestyle Advice Group) and were not included in analyses, leaving a total of 641 women (319 Lifestyle Advice Group and 322 Standard Care). A further four women (two in each group) terminated pregnancies for foetal anomalies; four women suffered a stillbirth (all in the Standard Care Group); and two liveborn infants died after birth (both in the Lifestyle Advice Group). Two stillbirths occurred in the setting of chorioamnionitis prior to 24 weeks’ gestation; one occurred at 40 weeks secondary to Escherichia coli sepsis; and one unexplained stillbirth occurred at 39 weeks. One liveborn infant died secondary to extreme prematurity following spontaneous birth at 23 weeks, and the second infant, born at 36 weeks, died at a few hours of age from pulmonary hypoplasia secondary to multicystic dysplastic kidney disease. Overall, 633 women and 629 liveborn infants were included in the analyses, with adequate data available for 628 (99.8%) for the primary outcome of birth weight above 4.0 kg. There were no maternal deaths.
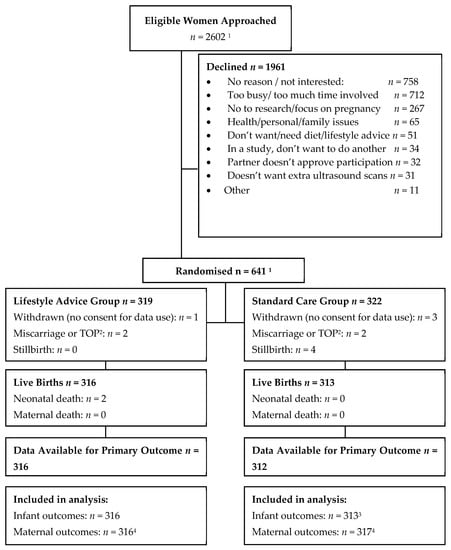
Figure 1.
Flow of participants in the trial. Notes: 1 This number excludes four women who were randomised in error prior to trial registration. 2 Termination of pregnancy (TOP) 3 Three hundred and twelve infants with non-missing data included in raw data analysis, one infant with missing data had outcomes imputed and was therefore included in the imputed analysis. 4 Stillbirths excluded from infant outcomes analysis but included for analysis of maternal antenatal outcomes only.
The baseline characteristics of women in the two treatment groups were similar at trial entry, as shown in Table 1. The median BMI of the cohort was 22.20 kg/m2 (inter-quartile range (IQR) 20.87 to 23.60 kg/m2). The mean maternal age of participants was 31.5 years, with 59% of women in their first ongoing pregnancy. The median gestational age at trial entry was approximately 16.3 weeks (IQR 14.57 to 18.14 weeks), 4.4% of women were smokers, and 30.5% of women were from the highest two quintiles of social disadvantage.

Table 1.
Baseline characteristics.
3.2. Pre-Specified Infant Outcomes
There was no statistically significant difference in the proportion of infants with birth weight above 4.0 kg between the Lifestyle Advice and Standard Care groups (24/316 (7.59%) Lifestyle Advice versus 26/313 (8.31%) Standard Care; adjusted risk ratio (aRR) 0.91; 95% confidence interval (CI) 0.54 to 1.55; p = 0.732), as shown in Table 2.
Table 2.
Pre-specified infant outcomes by treatment group.
3.3. Maternal Diet Quality
When compared with women who received standard care, women who received lifestyle advice demonstrated improvements in their reported dietary quality as measured by the healthy eating index (HEI) at both 28 (74.35 ± 7.65 Lifestyle Advice Group vs. 72.11 ± 8.21 Standard Care Group; adjusted mean difference 2.21; 95% CI 0.98 to 3.45; p < 0.001) and 36 weeks’ gestation (74.10 ± 8.77 Lifestyle Advice Group vs. 72.50 ± 8.43 Standard Care Group; adjusted mean difference 1.57; 95% CI 0.22 to 2.91; p = 0.023), as shown in Table 3. There were no observed differences in reported physical activity, as shown in Table 3.
Table 3.
Pre-specified maternal antepartum diet quality and physical activity outcomes by treatment group.
3.4. Pre-Specified Maternal Antepartum Outcomes
Despite improvements in maternal diet quality, there were no differences between the treatment groups observed for total GWG (11.32 ± 3.96 kg Lifestyle Advice versus 11.70 ± 3.78 kg Standard Care; adjusted mean difference (aMD)—0.37; 95% CI—0.97 to 0.23; p = 0·227), as shown in Table 4. Similarly, there were no observed differences in the proportion of women who gained weight above (28 (8.72%) Lifestyle Advice versus 41 (13.16%) Standard Care; aRR 0.58; 95% CI 0.32 to 1.04; p = 0.066) or below (160 (50.71%) Lifestyle Advice versus 162 (51.68%) Standard Care; aRR 0.85; 95% CI 0.60 to 1.21; p = 0.366) the IOM recommendations, as shown in Table 4.
Table 4.
Pre-specified maternal antepartum outcomes by treatment group.
There were no significant differences observed between the two treatment groups with regards to the occurrence of pregnancy-related complications, including hypertension, pre-eclampsia or eclampsia, gestational diabetes, antepartum haemorrhage or preterm prelabour ruptured membranes, as shown in Table 4. There were no significant differences in the number of antenatal hospital admissions between the two groups, however, there was a borderline statistically significant difference in the mean number of antenatal days in hospital (0.83 (4.18) Lifestyle Advice Group versus 0.42 (1.49) in the Standard Care Group; aRR 1.99; 95% CI 1.03 to 3.85; p = 0.042). This difference can be explained by the extremely long antenatal hospital admissions for three women in the Lifestyle Advice Group, as shown in Table 4. Self-reported maternal quality of life was similar between groups, as shown in Table S1.
3.5. Pre-Specified Maternal Labour and Birth Outcomes
While there was a reduction in the risk of requiring induction of labour among women in the Lifestyle Advice group (74 (23.42%) Lifestyle Advice versus 109 (34.96%) Standard Care; aRR 0.66; 95% CI 0.52 to 0.85; p = 0·001), this likely reflected chance differences in the need for induction of labour for post-dates pregnancy (21 (28.38%) Lifestyle Advice versus 43 (39.45%) Standard Care), as shown in Table 5. There were no significant differences observed between the two groups with regards to risk of caesarean birth (73 (23.17%) Lifestyle Advice versus 74 (23.79%) Standard Care; aRR 0.95; 95% CI 0.72 to 1.26; p = 0.713).
Table 5.
Pre-specified maternal labour and birth outcomes by treatment group.
The mean gestational age at birth was lower in the Lifestyle Advice Group (39.12 ± 2.38 weeks Lifestyle Advice versus 39.46 ± 1.63 weeks Standard Care; aMD—0.34; 95% CI—0.66 to −0.02; p = 0·039), as shown in Table 2. While this difference is statistically significant, the difference is considered clinically small, and reflective of the differences in induction of labour for post-dates pregnancy. The non-statistically significant difference observed in mean infant birth weight (3291.97 ± 586.20 g Lifestyle Advice versus 3370.92 ± 511.24 g Standard Care; aMD—78.39; 95% CI—164.00 to 7.22; p = 0.073) is also reflective of the observed difference in mean gestational age at birth; the mean difference in birthweight z-score was not near statistical significance (aMD—0.04; 95% CI—0.18, 0.09, p = 0.532). There were no statistically significant differences between the two groups with regards to other infant outcomes, as shown in Table 2, or newborn anthropometric measures, as shown in Table S2.
3.6. Effect Modification by Maternal Pre-Pregnancy BMI
Pre-specified secondary analyses identified some evidence of effect modification by maternal pre-pregnancy BMI, suggesting that the intervention may have been more effective in women with higher maternal BMI in reducing infant birth weight and head, abdominal and chest circumferences, as shown in Table S3. There was also some weak evidence suggesting a differential effect of the intervention by parity on infant birth weight, chest and arm circumference and thigh skinfold measurement, with lifestyle advice being more effective in reducing these measures among women in their second and subsequent pregnancy.
4. Discussion
Our findings indicate that providing lifestyle advice during pregnancy to women with BMI within the normal range was associated with improvements in maternal diet quality over the course of pregnancy. However, despite improvements in maternal diet, lifestyle advice was not associated with any differences in total gestational weight gain or risk of weight gain below or above the IOM recommendations. There were no significant differences in clinical outcomes for either women or their infants, including risk of infant birth weight above 4 kg.
There were a number of strengths to our randomised trial. To our knowledge, it was the largest of its kind recruiting women with healthy BMI during pregnancy, with comprehensive reporting of relevant maternal and infant clinical outcomes, high rates of participant follow-up and broad inclusion criteria. Our methodology was robust, with all participating women prospectively having their height, weight and BMI measured, use of a central randomisation service and outcome assessors who were blinded to the woman’s allocated treatment group. Furthermore, both the content and intensity of the intervention reflect one that could be realistically achieved within current public antenatal care services.
Participants in our trial were predominantly white Caucasian, with less than half of women from areas of high social disadvantage. Furthermore, 75% of eligible women declined participation due to time constraints, lack of interest or lack of perceived need. These factors may limit our external validity and generalisability of our findings to other patient populations.
Our systematic review evaluating dietary and lifestyle interventions in pregnant women with healthy BMI, providing a combined intervention was associated with a modest 1.25 kg difference in weight gain (5 studies, 714 women) [34]. Overall, the methodological quality of the studies included were of medium to high quality, and low to medium risk of bias [34]. The intensity and nature of the intervention overall was poorly described, with nine interventions consisting of face-to-face sessions with a trained professional [52,53,54,55,56,57,58,59,60]. The intensity ranged from three dietetic sessions over pregnancy [58,59], up to one at each antenatal visit [61]. Three studies [52,54,58] provided an additional session post-partum.
The findings of our current study are in contrast to this review [34], finding no clinically or statistically significant difference in total gestational weight gain, or risk of weight gain below or above the IOM recommendations. However, provision of dietary and lifestyle advice during pregnancy was associated with improvements in maternal self-reported diet quality as measured by the HEI. These findings are consistent with those we have reported previously from both the LIMIT [37,38] and GROW [61] randomised trials, highlighting the reproducibility of the intervention among pregnant women across the BMI spectrum in effecting dietary change.
Overall, however, our findings are consistent with the broader literature describing antenatal dietary and lifestyle interventions in pregnant women across all BMI categories [62]. In a comprehensive individual participant data meta-analysis utilising data from 36 randomised trials, and more than 12,500 pregnant women, a modest effect on GWG was identified following dietary and physical activity advice (mean difference −0.7 kg), although there was very little effect on clinical pregnancy and neonatal outcomes [62]. When considered in their totality, the available literature challenges the current underlying rationale of providing an antenatal dietary and lifestyle intervention with the intention of limiting weight gain as a means to improving pregnancy outcomes. GWG reflects a combination of maternal fat deposition, pregnancy related plasma volume expansion, breast and uterine tissue hypertrophy, extracellular fluid, placental mass, foetal mass and amniotic fluid volume [63], and while it has been considered a surrogate for adiposity gain in pregnancy, the evidence to date suggests that it may not be readily modified simply through changes in maternal dietary intake and physical activity.
5. Conclusions
Our findings indicate that while providing lifestyle advice during pregnancy to women with BMI within the normal range was associated with improvements in maternal diet quality, there were no clinically or statistically significant differences in total gestational weight gain or in clinical outcomes for either women or their infants. Providing such an intervention in pregnancy is not advocated.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6643/11/12/2911/s1, Table S1: Maternal Quality of Life, Table S2: Infant anthropometry, and Table S3: Pre-specified analysis of effect modification by maternal pre-pregnancy BMI.
Author Contributions
J.M.D. was responsible for conceptualisation, funding acquisition, methodology, project administration, supervision of the trial, data curation, data interpretation, original draft preparation, writing and review and editing. A.R.D. was responsible for trial management and administration, data curation, writing, review and editing. J.L. was responsible for trial administration, data curation, formal data analysis and interpretation, writing, review and editing.
Funding
This project was funded by intramural funding from The University of Adelaide. The trial has received competitive funding (Lloyd Cox Strategic Research Excellence Award), and ethical approval from the Women’s and Children’s Hospital research and ethics committee. J.M.D. is supported through a NHMRC Practitioner Fellowship (ID 1078980).
Acknowledgments
We are indebted to the 641 women who participated in this randomised trial. The following persons and institutions (except where indicated, in Adelaide, South Australia) participated in the OPTIMISE Trial: Co-ordinating Team—Jodie M. Dodd, Andrea R. Deussen, Jennie Louise, A. Newman, L. Greenham, A. Jacobssen, C. Sheppard, F. Spronk, Z. Sui, L. Williams, E. Lyrtzis, C. Cramp, S. Han, M. Kelsey. Statistical Analyses—Jennie Louise. Adverse Events Committee—J. Svigos, V. Bhatia, N. Manton. Writing Group—Jodie M. Dodd, Andrea R. Deussen, Jennie Louise. Women’s and Children’s Hospital (South Australia): Jodie M. Dodd, Andrea R. Deussen, H. Purcell, Midwifery Staff of the Antenatal Clinic.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- World Health Organisation. 2008–2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases: Prevent and Control Cardiovascular Diseases, Cancers, Chronic Respiratory Diseases and Diabetes; World Health Organisation WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Walls, H.L.; Magliano, D.J.; Stevenson, C.E.; Backholer, K.; Mannan, H.R.; Shaw, J.E.; Peeters, A. Projected progression of the prevalence of obesity in australia. Obesity (Silver Spring) 2012, 20, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Crawford, D.; Ireland, P.; Hodge, A. Patterns and demographic predictors of 5-year weight change in a multi-ethnic cohort of men and women in Australia. Public Health Nutr. 2003, 6, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Adamson, L.; Brown, W.; Byles, J.; Chojenta, C.; Dobson, A.; Fitzgerald, D.; Hockey, R.; Loxton, D.; Powers, J.; Spallek, M.; et al. Women’s Weight: Findings from the Australian Longitudinal Study on Women’s Health, Report prepared for the Australian Government Department of Health. Available online: https://www.alswh.org.au/images/content/pdf/major_reports/ALSWH%202018%20Major%20Report_Caring%20final.pdf (accessed on 30 June 2013).
- Cameron, A.J.; Welborn, T.A.; Zimmet, P.Z.; Dunstan, D.W.; Owen, N.; Salmon, J.; Dalton, M.; Jolley, D.; Shaw, J.E. Overweight and obesity in Australia: The 1999–2000 Australian diabetes, obesity and lifestyle study (ausdiab). Med. J. Aust. 2003, 178, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Mannan, M.; Doi, S.A.R.; Mamun, A.A. Association between weight gain during pregnancy and postpartum weight retention and obesity: A bias-adjusted meta-analysis. Nutr. Rev. 2013, 71, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, E.P.; Abrams, B. Epidemiology of gestational weight gain and body weight changes after pregnancy. Epidemiol. Rev. 2000, 22, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, N.M.; Nicholson, W.K.; Schmitt, J. The association of pregnancy and the development of obesity—Results of a systematic review and meta-analysis on the natural history of postpartum weight retention. Int. J. Obes. (Lond.) 2007, 31, 1642–1651. [Google Scholar] [CrossRef]
- Institute of Medicine. Subcommittee on Nutritional Status and Weight Gain in Pregnancy. In Nutrition during Pregnancy; National Academy Press: Washington, DC, USA, 1990. [Google Scholar]
- Institute of Medicine. Subcommittee on Nutritional Status and Weight Gain in Pregnancy. In Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Dodd, J.M.; Grivell, R.M.; Nguyen, A.M.; Chan, A.; Robinson, J.S. Maternal and perinatal health outcomes by body mass index category. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 136–140. [Google Scholar] [CrossRef]
- Callaway, L.K.; Prins, J.B.; Chang, A.M.; McIntyre, H.D. The prevalence and impact of overweight and obesity in an australian obstetric population. Med. J. Aust. 2006, 184, 56–59. [Google Scholar] [CrossRef]
- Cedergren, M. Effects of gestational weight gain and body mass index on obstetric outcome in sweden. Int. J. Gynecol. Obstet. 2006, 93, 269–274. [Google Scholar] [CrossRef]
- Cedergren, M.I. Optimal gestational weight gain for body mass index categories. Obstet. Gynecol. 2007, 110, 759–764. [Google Scholar] [CrossRef]
- Rooney, B.L.; Schauberger, C.W. Excess pregnancy weight gain and long-term obesity: One decade later. Obstet. Gynecol. 2002, 100, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.L.; Schauberger, C.W.; Mathiason, M.A. Impact of perinatal weight change on long-term obesity and obesity-related illnesses. Obstet. Gynecol. 2005, 106, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Amorim, A.R.; Rössner, S.; Neovius, M.; Lourenço, P.M.; Linné, Y. Does excess pregnancy weight gain constitute a major risk for increasing long-term bmi? Obesity (Silver Spring) 2007, 15, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Szeto, I.M.; Yu, K.; Ning, Y.; Li, W.; Wang, J.; Zheng, Y.; Zhang, Y.; Wang, P. Association between gestational weight gain according to prepregnancy body mass index and short postpartum weight retention in postpartum women. Clin. Nutr. 2015, 34, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Schmoll, S.; Beyerlein, A.; Hauner, H.; von Kries, R. Gestational weight gain and long-term postpartum weight retention: A meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Qi, Y.; Sermer, M.; Connelly, P.W.; Hanley, A.J.; Zinman, B. Glucose intolerance in pregnancy and future risk of pre-diabetes or diabetes. Diabetes Care 2008, 31, 2026–2031. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational weight gain and risk of gestational diabetes mellitus. Obstet. Gynecol. 2010, 115, 597–604. [Google Scholar] [CrossRef]
- Shah, B.R.; Retnakaran, R.; Booth, G.L. Increased risk of cardiovascular disease in young women following gestational diabetes mellitus. Diabetes Care 2008, 31, 1668–1669. [Google Scholar] [CrossRef]
- Jonsdottir, L.S.; Arngrimsson, R.; Geirsson, R.T.; Sigvaldason, H.; Sigfusson, N. Death rates from ischemic heart disease in women with a history of hypertension in pregnancy. Acta. Obstet. Gynecol. Scand. 1995, 74, 772–776. [Google Scholar] [CrossRef]
- Fraser, A.; Tilling, K.; Macdonald-Wallis, C.; Hughes, R.; Sattar, N.; Nelson, S.M.; Lawlor, D.A. Associations of gestational weight gain with maternal body mass index, waist circumference, and blood pressure measured 16 y after pregnancy: The avon longitudinal study of parents and children (alspac). Am. J. Clin. Nutr. 2011, 93, 1285–1292. [Google Scholar] [CrossRef]
- Mamun, A.A.; Kinarivala, M.; O’Callaghan, M.J.; Williams, G.M.; Najman, J.M.; Callaway, L.K. Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21y postpartum follow-up. Am. J. Clin. Nutr. 2010, 91, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.L.; Mathiason, M.A.; Schauberger, C.W. Predictors of obesity in childhood, adolescence, and adulthood in a birth cohort. Matern. Child Health J. 2011, 15, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Oken, E.; Taveras, E.M.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Gestational weight gain and child adiposity at age 3 years. Am. J. Obstet. Gynecol. 2007, 196, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Wrotniak, B.H.; Shults, J.; Butts, S.; Stettler, N. Gestational weight gain and risk of overweight in the offspring at age 7 y in a multicenter, multiethnic cohort study. Am. J. Clin. Nutr. 2008, 87, 1818–1824. [Google Scholar] [CrossRef] [PubMed]
- Cnattingius, S.; Villamor, E.; Lagerros, Y.T.; Wikstrom, A.K.; Granath, F. High birth weight and obesity—A vicious circle across generations. Int. J. Obes. (Lond.) 2012, 36, 1320–1324. [Google Scholar] [CrossRef] [PubMed]
- Schack-Nielsen, L.; Michaelsen, K.F.; Gamborg, M.; Mortensen, E.L.; Sorensen, T.I.A. Gestational weight gain in relation to offspring body mass index and obesity from infancy through adulthood. Int. J. Obesity 2010, 34, 67–74. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Lichtenstein, P.; Fraser, A.; Långström, N. Does maternal weight gain in pregnancy have long-term effects on offspring adiposity? A sibling study in a prospective cohort of 146,894 men from 136,050 families. Am. J. Clin. Nutr. 2011, 94, 142–148. [Google Scholar] [CrossRef]
- Fraser, A.; Tilling, K.; Macdonald-Wallis, C.; Sattar, N.; Brion, M.J.; Benfield, L.; Ness, A.; Deanfield, J.; Hingorani, A.; Nelson, S.M.; et al. Association of maternal weight gain in pregnancy with offspring obesity and metabolic and vascular traits in childhood. Circulation 2010, 121, 2557–2564. [Google Scholar] [CrossRef]
- Gaillard, R.; Welten, M.; Oddy, W.H.; Beilin, L.J.; Mori, T.A.; Jaddoe, V.W.V.; Huang, R.-C. Associations of maternal prepregnancy body mass index and gestational weight gain with cardio-metabolic risk factors in adolescent offspring: A prospective cohort study. BJOG 2016, 123, 207–216. [Google Scholar] [CrossRef]
- O’Brien, C.M.; Grivell, R.M.; Dodd, J.M. Systematic review of antenatal dietary and lifestyle interventions in women with a normal body mass index. Acta. Obstet. Gynecol. Scand. 2016, 95, 259–269. [Google Scholar] [CrossRef]
- Dodd, J.M.; Deussen, A.R.; Louise, J. Optimising gestational weight gain and improving maternal and infant health outcomes through antenatal dietary, lifestyle and physical activity advice: The optimise randomised controlled trial protocol. BMJ Open 2018, 8, e019583. [Google Scholar] [CrossRef] [PubMed]
- Australian Guide to Healthy Eating. Australian Guide to Healthy Eating. Available online: https://www.eatforhealth.gov.au/guidelines/australian-guide-healthy-eating (accessed on 1 January 2014).
- Dodd, J.M.; Cramp, C.; Sui, Z.; Yelland, L.N.; Deussen, A.R.; Grivell, R.M.; Moran, L.J.; Crowther, C.A.; Turnbull, D.; McPhee, A.J.; et al. The effects of antenatal dietary and lifestyle advice for women who are overweight or obese on maternal diet and physical activity: The limit randomised trial. BMC Med. 2014, 12, 161. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.M.; Turnbull, D.A.; McPhee, A.J.; Deussen, A.R.; Grivell, R.M.; Yelland, L.N.; Crowther, C.A.; Wittert, G.; Owens, J.A.; Robinson, J.S. Antenatal lifestyle advice for women who are overweight or obese: The limit randomised trial. BMJ 2014, 348, g1285. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.; Murphy, S. Psychology and Health Promotion; Open University Press: Buckingham, UK, 1997. [Google Scholar]
- SA Perinatal Practice Guidelines. Diabetes Mellitus and Gestational Diabetes. Available online: https://www.sahealth.sa.gov.au/wps/wcm/connect/146238004ee2144cb404bdd150ce4f37/Diabetes+Mellitus+and+GDM_+PPG_v5_0+%281%292.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-146238004ee2144cb404bdd150ce4f37-mSkq58x (accessed on 10 October 2013).
- Australian and New Zealand Neonatal Network (ANZNN). Available online: https://anznn.net/dataresources/datadictionaries (accessed on 10 October 2013).
- Sarnat, H.B.; Sarnat, M.S. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch. Neurol. 1976, 33, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Hague, W.M.; Higgins, J.; Lowe, S.; McCowan, L.; Oats, J.; Peek, M.J.; Rowan, J.A.; Walters, B.N.; Austalasian Society of the Study of Hypertension in Pregnancy. The detection, investigation and management of hypertension in pregnancy: Full consensus statement. Aust. N. Z. J. Obstet. Gynaecol. 2000, 40, 139–155. [Google Scholar] [CrossRef]
- Willett, W.C.; Reynolds, R.D.; Cottrell-Hoehner, S.; Sampson, L.; Browne, M.L. Validation of a semi-quantitative food frequency questionnaire: Comparison with a 1-year diet record. J. Am. Diet. Assoc. 1987, 87, 43–47. [Google Scholar]
- Ibiebele, T.I.; Parekh, S.; Mallitt, K.A.; Hughes, M.C.; O’Rourke, P.K.; Webb, P.M.; Grp, A.O.C.S.; Study, A.C. Reproducibility of food and nutrient intake estimates using a semi-quantitative ffq in Australian adults. Public Health Nutr. 2009, 12, 2359–2365. [Google Scholar] [CrossRef]
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The mos 36 item short form health survey (sf36) conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the spielberger state-trait anxiety inventory (stai). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10 item edinburgh postnatal depression scale (edps). Brit. J. Psych. 1987, 154, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Scheil, W.; Scott, J.; Catcheside, B.; Sage, L.; Kennare, R. Pregnancy Outcome in South Australia 2014; Pregnancy Outcome Unit, SA Health, Ed.; Government of South Australia: Adelaide, Australia, 2016.
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Althuizen, E.; van der Wijden, C.L.; van Mechelen, W.; Seidell, J.C.; van Poppel, M.N. The effect of a counselling intervention on weight changes during and after pregnancy: A randomised trial. BJOG 2013, 120, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Asbee, S.M.; Jenkins, T.R.; Butler, J.R.; White, J.; Elliot, M.; Rutledge, A. Preventing excessive weight gain during pregnancy through dietary and lifestyle counseling a randomized controlled trial. Obstet. Gynecol. 2009, 113, 305–311. [Google Scholar] [CrossRef]
- Huang, T.T.; Yeh, C.Y.; Tsai, Y.C. A diet and physical activity intervention for preventing weight retention among taiwanese childbearing women: A randomised controlled trial. Midwifery 2011, 27, 257–264. [Google Scholar] [CrossRef]
- Hui, A.; Back, L.; Ludwig, S.; Gardiner, P.; Sevenhuysen, G.; Dean, H.; Sellers, E.; McGavock, J.; Morris, M.; Bruce, S.; et al. Lifestyle intervention on diet and exercise reduced excessive gestational weight gain in pregnant women under a randomised controlled trial. BJOG 2012, 119, 70–77. [Google Scholar] [CrossRef]
- Hui, A.L.; Back, L.; Ludwig, S.; Gardiner, P.; Sevenhuysen, G.; Dean, H.J.; Sellers, E.; McGavock, J.; Morris, M.; Jiang, D.; et al. Effects of lifestyle intervention on dietary intake, physical activity level, and gestational weight gain in pregnant women with different pre-pregnancy body mass index in a randomized control trial. BMC Pregnancy Childbirth 2014, 14, 331. [Google Scholar] [CrossRef]
- Hui, A.L.; Ludwig, S.M.; Gardiner, P.; Sevenhuysen, G.; Murray, R.; Morris, M.; Shen, G.X. Community-based exercise and dietary intervention during pregnancy: A pilot study. Can. J. Diabetes 2006, 30, 169–175. [Google Scholar] [CrossRef]
- Laitinen, K.; Poussa, T.; Isolauri, E.; Nutrition, Allergy, Mucosal Immunology and Intestinal Microbiota Group. Probiotics and dietary counselling contribute to glucose regulation during and after pregnancy: A randomised controlled trial. Br. J. Nutr. 2009, 101, 1679–1687. [Google Scholar] [CrossRef]
- Phelan, S.; Phipps, M.G.; Abrams, B.; Darroch, F.; Schaffner, A.; Wing, R.R. Randomized trial of a behavioral intervention to prevent excessive gestational weight gain: The fit for delivery study. Am. J. Clin. Nutr. 2011, 93, 772–779. [Google Scholar] [CrossRef]
- Polley, B.A.; Wing, R.R.; Sims, C.J. Randomized controlled trial to prevent excessive weight gain in pregnant women. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.M.; Louise, J.; Deussen, A.R.; Grivell, R.M.; Dekker, G.; McPhee, A.J.; Hague, W. Effect of metformin in addition to dietary and lifestyle advice for pregnant women who are overweight or obese: The grow randomised, double-blind, placebo-controlled trial. Lancet. Diabetes Endocrinol. 2019, 7, 15–24. [Google Scholar] [CrossRef]
- International Weight Management in Pregnancy Collaborative Group. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. BMJ 2017, 358, j3119. [Google Scholar]
- Dodd, J.M. Pregnancy: Managing obesity during pregnancy-what are the options? Nat. Rev. Endocrinol. 2015, 11, 691–692. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).