Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistics
3. Results
3.1. Characteristics of Weight Loss Maintainers versus Controls
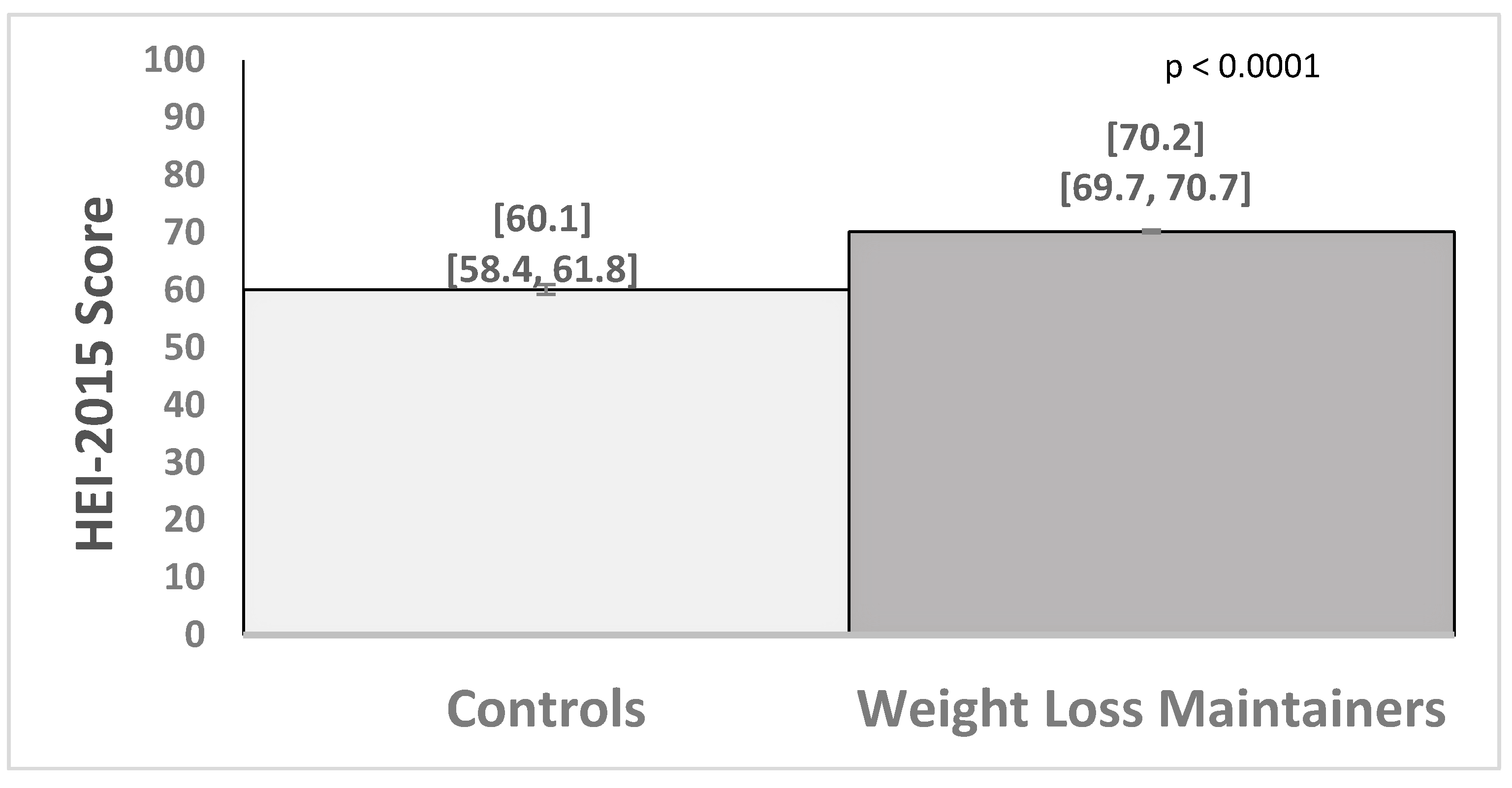
3.2. Group Differences in Healthy Eating Index and Macronutrients
3.3. Group Differences in Proportions Meeting Estimated Average Requirement for Micronutrients
3.4. Multiple Discriminant Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Astrup, A.; Bugel, S. Overfed but undernourished: Recognizing nutritional inadequacies/deficiencies in patients with overweight or obesity. Int. J. Obes. (Lond.) 2019, 43, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Reider, C.; Brooks, J.R.; Fulgoni, V.L. Comparison of prevalence of inadequate nutrient intake based on body weight status of adults in the United States: An analysis of NHANES 2001–2008. J. Am. Coll. Nutr. 2015, 34, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Via, M. The malnutrition of obesity: Micronutrient deficiencies that promote diabetes. ISRN Endocrinol. 2012, 2012, 103472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Marriott, B.P.; Olsho, L.; Hadden, L.; Connor, P. Intake of added sugars and selected nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003–2006. Crit. Rev. Food. Sci. Nutr. 2010, 50, 228–258. [Google Scholar] [CrossRef]
- Kaidar-Person, O.; Person, B.; Szomstein, S.; Rosenthal, R.J. Nutritional deficiencies in morbidly obese patients: A new form of malnutrition? Part B: Minerals. Obes. Surg. 2008, 18, 1028–1034. [Google Scholar] [CrossRef]
- García, O.P.; Long, K.Z.; Rosado, J.L. Impact of micronutrient deficiencies on obesity. Nutr. Rev. 2009, 67, 559–572. [Google Scholar] [CrossRef]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef]
- Fulgoni, V.L.; Keast, D.R.; Bailey, R.L.; Dwyer, J. Foods, fortificants, and supplements: Where do Americans get their nutrients? J. Nutr. 2011, 141, 1847–1854. [Google Scholar] [CrossRef]
- Blumberg, J.B.; Bailey, R.L.; Sesso, H.D.; Ulrich, C.M. The evolving role of multivitamin/multimineral supplement use among adults in the age of personalized nutrition. Nutrients 2018, 10, E248. [Google Scholar] [CrossRef] [Green Version]
- Webber, K.H.; Lee, E. The diet quality of adult women participating in a behavioural weight-loss programme. J. Hum. Nutr. Diet. 2011, 24, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Harrigan, M.; George, S.M.; Ferrucci, L.M.; Sanft, T.; Irwin, M.L.; Cartmel, B. Changes in diet quality in a randomized weight loss trial in breast cancer survivors: The lifestyle, exercise, and nutrition (LEAN) study. NPJ Breast Cancer 2016, 2, 16026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ptomey, L.T.; Willis, E.A.; Goetz, J.R.; Lee, J.; Szabo-Reed, A.N.; Sullivan, D.K.; Donnelly, J.E. Portion-controlled meals provide increases in diet quality during weight loss and maintenance. J. Hum. Nutr. Diet. 2016, 29, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, G.D.; Beavers, D.P.; Hamm, D.; Mihalko, S.L.; Messier, S.P. Nutrient intake during diet-induced weight loss and exercise interventions in a randomized trial in older overweight and obese adults. J. Nutr. Health Aging 2017, 21, 1216–1224. [Google Scholar] [CrossRef]
- Mueller-Cunningham, W.M.; Quintana, R.; Kasim-Karakas, S.E. An ad libitum, very low-fat diet results in weight loss and changes in nutrient intakes in postmenopausal women. J. Am. Diet. Assoc. 2003, 103, 1600–1606. [Google Scholar] [CrossRef]
- Ma, Y.; Pagoto, S.L.; Griffith, J.A.; Merriam, P.A.; Ockene, I.S.; Hafner, A.R.; Olendzki, B.C. dietary quality comparison of popular weight-loss plans. J. Am. Diet. Assoc. 2007, 107, 1786–1791. [Google Scholar] [CrossRef] [Green Version]
- Truby, H.; Hiscutt, R.; Herriot, A.M.; Stanley, M.; Delooy, A.; Fox, K.R.; Baic, S.; Robson, P.J.; Macdonald, I.; Taylor, M.A.; et al. Commercial weight loss diets meet nutrient requirements in free living adults over 8 weeks: A randomised controlled weight loss trial. Nutr. J. 2008, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Eberhard, M.I.; Olson, A.D.; Ambrosini, G.L.; Ahern, A.L.; Caterson, I.; Hauner, H.; Jebb, S.A. Greater improvements in diet quality in participants randomised to a commercial weight loss programme compared with standard care delivered in GP practices. Proc. Nutr. Soc. 2011, 70, E252. [Google Scholar] [CrossRef] [Green Version]
- Shick, S.M.; Wing, R.R.; Klem, M.L.; McGuire, M.T.; Hill, J.O.; Seagle, H. Persons successful at long-term weight loss and maintenance continue to consume a low-energy, low-fat diet. J. Am. Diet. Assoc. 1998, 98, 408–413. [Google Scholar] [CrossRef]
- Jolly, K.; Lewis, A.; Beach, J.; Denley, J.; Adab, P.; Deeks, J.J.; Daley, A.; Aveyard, P. Comparison of range of commercial or primary care led weight reduction programmes with minimal intervention control for weight loss in obesity: Lighten Up randomised controlled trial. BMJ 2011, 343, d6500. [Google Scholar] [CrossRef] [Green Version]
- Heshka, S.; Anderson, J.W.; Atkinson, R.L.; Greenway, F.L.; Hill, J.O.; Phinney, S.D.; Kolotkin, R.L.; Miller-Kovach, K.; Pi-Sunyer, F.X. Weight loss with self-help compared with a structured commercial program: A randomized trial. JAMA 2003, 289, 1792–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudzune, K.A.; Doshi, R.S.; Mehta, A.K.; Chaudhry, Z.W.; Jacobs, D.K.; Vakil, R.M.; Lee, C.J.; Bleich, S.N.; Clark, J.M. Efficacy of commercial weight-loss programs: An updated systematic review. Ann. Intern. Med. 2015, 162, 501–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahern, A.L.; Wheeler, G.M.; Aveyard, P.; Boyland, E.J.; Halford, J.C.G.; Mander, A.P.; Woolston, J.; Thomson, A.M.; Tsiountsioura, M.; Cole, D.; et al. Extended and standard duration weight-loss programme referrals for adults in primary care (WRAP): A randomised controlled trial. Lancet 2017, 389, 2214–2225. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63 Pt B, 2985–3023. [Google Scholar] [CrossRef] [Green Version]
- Look AHEAD Research Group; Pi-Sunyer, X.; Blackburn, G.; Brancati, F.L.; Bray, G.A.; Bright, R.; Clark, J.M.; Curtis, J.M.; Espeland, M.A.; Foreyt, J.P.; et al. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: One-year results of the look AHEAD trial. Diabetes Care 2007, 30, 1374–1383. [Google Scholar]
- McGuire, M.T.; Wing, R.R.; Klem, M.L.; Hill, J.O. Behavioral strategies of individuals who have maintained long-term weight losses. Obes. Res. 1999, 7, 334–341. [Google Scholar] [CrossRef]
- Klem, M.L.; Wing, R.R.; McGuire, M.T.; Seagle, H.M.; Hill, J.O. A descriptive study of individuals successful at long-term maintenance of substantial weight loss. Am. J. Clin. Nutr. 1997, 66, 239–246. [Google Scholar] [CrossRef] [Green Version]
- McGuire, M.T.; Wing, R.R.; Klem, M.L.; Lang, W.; Hill, J.O. What predicts weight regain in a group of successful weight losers? J. Consult. Clin. Psychol. 1999, 67, 177–185. [Google Scholar] [CrossRef]
- National Institutes of Health, Epidemiology and Genomics Research Program. Diet History Questionnaire, Version 3.0; National Cancer Institute: Bethesda, MD, USA, 2015. [Google Scholar]
- Subar, A.F.; Thompson, F.E.; Kipnis, V.; Midthune, D.; Hurwitz, P.; McNutt, S.; McIntosh, A.; Rosenfeld, S. Comparative validation of the Block, Willett, and National Cancer Institute food frequency questionnaires: The Eating at America’s Table Study. Am. J. Epidemiol. 2001, 154, 1089–1099. [Google Scholar] [CrossRef]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.P.; Poos, M.I. Dietary Reference Intakes: Summary of applications in dietary assessment. Public Health Nutr. 2002, 5, 843–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christifano, D.N.; Fazzino, T.L.; Sullivan, D.K.; Befort, C. Diet Quality of Breast Cancer Survivors after a Six-Month Weight Management Intervention: Improvements and Association with Weight Loss. Nutr. Cancer 2016, 68, 1301–1308. [Google Scholar]
- Kimmons, J.E.; Blanck, H.M.; Tohill, B.C.; Zhang, J.; Khan, L.K. Associations between body mass index and the prevalence of low micronutrient levels among US adults. MedGenMed 2006, 8, 59. [Google Scholar] [PubMed]
- McNulty, H.; Ward, M.; Hoey, L.; Hughes, C.F.; Pentieva, K. Addressing optimal folate and related B-vitamin status through the lifecycle: Health impacts and challenges. Proc. Nutr. Soc. 2019, 78, 449–462. [Google Scholar] [CrossRef]
- Yang, Q.; Liu, T.; Kuklina, E.V.; Hong, Y.; Gillespie, C.; Chang, M.H.; Gwinn, M.; Dowling, N.; Khoury, M.J.; Hu, F.B. Sodium and potassium intake and mortality among US adults: Prospective data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2011, 171, 1183–1191. [Google Scholar] [CrossRef] [Green Version]
- Gahche, J.J.; Bailey, R.L.; Potischman, N.; Ershow, A.G.; Herrick, K.A.; Ahluwalia, N.; Dwyer, J.T. Federal Monitoring of Dietary Supplement Use in the Resident, Civilian, Noninstitutionalized US Population, National Health and Nutrition Examination Survey. J. Nutr. 2018, 148 (Suppl 2), 1436S–1444S. [Google Scholar] [CrossRef] [Green Version]
- DeSalvo, K.B.; Olson, R.; Casavale, K.O. Dietary Guidelines for Americans. JAMA 2016, 315, 457–458. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services and the U.S. Department of Agriculture. Dietary Guidelines for Americans 2015–2020. 2014. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 12 March 2019).
- Varkevisser, R.D.M.; van Stralen, M.M.; Kroeze, W.; Ket, J.C.F.; Steenhuis, I.H.M. Determinants of weight loss maintenance: A systematic review. Obes. Rev. 2019, 20, 171–211. [Google Scholar] [CrossRef] [Green Version]
- Phelan, S.; Wyatt, H.R.; Hill, J.O.; Wing, R.R. Are the eating and exercise habits of successful weight losers changing? Obesity (Silver Spring) 2006, 14, 710–716. [Google Scholar] [CrossRef]
- Kipnis, V.; Subar, A.F.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Bingham, S.; Schoeller, D.A.; Schatzkin, A.; Carroll, R.J. Structure of dietary measurement error: Results of the OPEN biomarker study. Am. J. Epidemiol. 2003, 158, 14–21; discussion 22–26. [Google Scholar] [CrossRef] [Green Version]
- Subar, A.F.; Kipnis, V.; Troiano, R.P.; Midthune, D.; Schoeller, D.A.; Bingham, S.; Sharbaugh, C.O.; Trabulsi, J.; Runswick, S.; Ballard-Barbash, R. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN study. Am. J. Epidemiol. 2003, 158, 1–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Controls | WLM | p Value | |
|---|---|---|---|
| N = 102 | N = 1207 | ||
| Age, years, mean (SD) | 48.6 (13.2) | 55.6 (12.3) | 0.0001 |
| Female, % | 82.4 | 91.4 | 0.003 |
| Currently in WW, % | 5.4 | 92.2 | 0.0001 |
| Lifetime maximum weight, kg | 124.5 (29.7) | 105.0 (22.1) | 0.0001 |
| Weight at start of WW, kg | — | 100.9 (20.9) | |
| BMI at start of WW, kg/m2 | — | 36.5 (7.0) | |
| Current weight, kg | 113.2 (24.3) | 75.2 (15.2) | 0.0001 |
| Weight loss since WW start, kg | — | 25.7 (13.2) | |
| Duration of 9.1 kg loss from WW start, years | — | 3.4 (3.0) | |
| Weight lost from maximum weight, kg | 11.3 (13.2) | 29.7 (15.0) | 0.0001 |
| Current BMI, kg/m2 | 41.1 (8.8) | 27.2 (5.1) | 0.0001 |
| BMI Categories | 0.0001 | ||
| Obese, % | 100 | 19.4 | |
| Overweight, % | 0 | 45.4 | |
| Normal weight, % | 0 | 35.2 | |
| Underweight, % | 0 | 0 | |
| Income (total in family per year) | 0.0001 | ||
| <$25,000 | 16.8 | 4.3 | |
| $25,001–75,000 | 52.5 | 31.6 | |
| >$75,000 | 30.7 | 64.0 | |
| Race/ethnicity | |||
| White, % | 84.3 | 94.9 | 0.0001 |
| Black, % | 13.7 | 2.2 | 0.0001 |
| Hispanic, % | 3.9 | 3.4 | 0.773 |
| Employed, % | 72.5 | 62.5 | 0.043 |
| College education or more, % | 88.2 | 90.1 | 0.794 |
| Married, % | 55.0 | 74.2 | 0.0001 |
| Supplement use a, % | 68.6 | 76.6 | 0.069 |
| Controls | WLM | Chi-Square a | Odds Ratio b | ||
|---|---|---|---|---|---|
| (N = 102) | (N = 1207) | p-Value | 95% CI | ||
| Calcium | Diet | 42.2% | 32.1% | 0.037 * | 0.92 (0.58–1.47); p = 0.726 |
| Diet + Suppl | 56.9% | 54.4% | 0.636 | 1.05 (0.67–1.65); p = 0.823 | |
| Copper | Diet | 81.4% | 96.2% | 0.0001 * | 7.56 (3.74–15.32); p = 0.0001 * |
| Diet + Suppl | 87.3% | 97.2% | 0.0001 * | 5.84 (2.60–13.11); p = 0.0001 * | |
| Iron | Diet | 75.5% | 78.1% | 0.537 | 1.47 (0.86–2.51); p = 0.159 |
| Diet + Suppl | 91.2% | 96.3% | 0.013 * | 1.91 (0.79–4.62); p = 0.151 | |
| Magnesium | Diet | 49.0% | 62.1% | 0.010 * | 1.73 (1.10–2.72); p = 0.017 |
| Diet + Suppl | 61.8% | 81.4% | 0.0001 * | 2.87 (1.77–4.65); p = 0.0001 * | |
| Phosphorus | Diet | 89.2% | 93.5% | 0.096 | 1.54 (0.72–3.32); p = 0.269 |
| Diet + Suppl | 90.2% | 95.6% | 0.014 * | 1.97 (0.88–4.45); p = 0.101 | |
| Potassium c | Diet | 2.0% | 9.6% | 0.010 * | 6.83 (1.53–30.48); p = 0.012 |
| Diet + Suppl | 2.9% | 10.1% | 0.018 * | 4.72 (1.35–16.47); p = 0.015 | |
| Selenium | Diet | 90.2% | 91.6% | 0.617 | 1.14 (0.53–2.48); p = 0.739 |
| Diet + Suppl | 92.2% | 95.6% | 0.112 | 1.56 (0.64–3.81); p = 0.332 | |
| Zinc | Diet | 70.6% | 72.9% | 0.613 | 1.21 (0.74–2.00); p = 0.447 |
| Diet + Suppl | 81.4% | 87.3% | 0.088 | 1.66 (0.92–3.01); p = 0.095 |
| Control (N = 102) | WLM (N = 1207) | Chi-sq p-Value a | Odds Ratio (95% CI) b | ||
|---|---|---|---|---|---|
| Vitamin A | Diet | 48.0% | 71.4% | 0.0001 * | 2.28 (1.42–3.66); p = 0.001 * |
| Diet + Suppl | 69.6% | 85.9% | 0.0001 * | 2.82 (1.68–4.75); p = 0.0001 * | |
| Thiamin (B1) | Diet | 64.7% | 73.9% | 0.044 * | 1.72 (1.07–2.78); p = 0.026 |
| Diet + Suppl | 77.5% | 88.1% | 0.002 * | 2.33 (1.33– 4.09); p = 0.003 | |
| Riboflavin (B2) | Diet | 89.2% | 98.0% | 0.0001 * | 5.33 (2.11–13.5); p = 0.0001 * |
| Diet + Suppl | 92.2% | 99.0% | 0.0001 * | 6.54 (2.21–19.34); p = 0.001 * | |
| Niacin (B3) | Diet | 82.4% | 87.4% | 0.145 | 1.64 (0.90–2.98); p = 0.110 |
| Diet + Suppl | 90.2% | 94.7% | 0.059 | 1.85 (0.82–4.14); p = 0.136 | |
| Vitamin B6 | Diet | 65.7% | 76.6% | 0.014 * | 2.29 (1.41–3.73); p = 0.001 * |
| Diet + Suppl | 79.4% | 88.9% | 0.004 * | 2.91 (1.61–5.24); p = 0.0001 * | |
| Vitamin B12 | Diet | 85.3% | 86.6% | 0.716 | 1.12 (0.58–2.13); p = 0.741 |
| Diet + Suppl | 92.2% | 93.5% | 0.613 | 1.23 (0.53–2.84); p = 0.625 | |
| Vitamin C | Diet | 56.9% | 85.3% | 0.0001 * | 4.29 (2.63–7.00); p = 0.0001 * |
| Diet + Suppl | 71.6% | 92.7% | 0.0001 * | 4.97 (2.80–8.80); p = 0.0001 * | |
| Vitamin D | Diet | 4.9% | 5.3% | 0.862 | 1.22 (0.44–3.44); p = 0.704 |
| Diet + Suppl | 42.2% | 54.0% | 0.021 * | 1.49 (0.94–2.35); p = 0.090 | |
| Vitamin E | Diet | 11.8% | 11.1% | 0.838 | 0.87 (0.44–1.72); p = 0.680 |
| Diet + Suppl | 46.1% | 61.2% | 0.003 * | 1.76 (1.12–2.77); p = 0.014 | |
| Folate | Diet | 53.9% | 63.6% | 0.051 | 1.72 (1.09–2.72); p = 0.020 |
| Diet + Suppl | 70.6% | 83.1% | 0.002 * | 2.20 (1.32–3.68); p = 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascual, R.W.; Phelan, S.; La Frano, M.R.; Pilolla, K.D.; Griffiths, Z.; Foster, G.D. Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers. Nutrients 2019, 11, 3046. https://doi.org/10.3390/nu11123046
Pascual RW, Phelan S, La Frano MR, Pilolla KD, Griffiths Z, Foster GD. Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers. Nutrients. 2019; 11(12):3046. https://doi.org/10.3390/nu11123046
Chicago/Turabian StylePascual, Rebecca W., Suzanne Phelan, Michael R. La Frano, Kari D. Pilolla, Zoe Griffiths, and Gary D. Foster. 2019. "Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers" Nutrients 11, no. 12: 3046. https://doi.org/10.3390/nu11123046
APA StylePascual, R. W., Phelan, S., La Frano, M. R., Pilolla, K. D., Griffiths, Z., & Foster, G. D. (2019). Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers. Nutrients, 11(12), 3046. https://doi.org/10.3390/nu11123046