We found that Codex guidance was perceived as likely to have a high impact on FoP nutrition labelling globally, either positive or negative depending on the nature of the guidance ultimately developed. We also identified a small and highly interconnected “regime complex” surrounding FoP nutrition labelling at the global level and found that influence on Codex discussions is being exerted differentially by actors at the national and global level, particularly by government and industry actors.
3.1. Impact of Codex
All the respondents made mention of Codex as a norm-setting institution, with a strong influence on national food regulation globally, as well as on industry standards and regional standards. Countries with limited regulatory capacity (i.e., many LMICs) were identified as likely to adopt Codex guidance without amendment, adding to the impact of Codex decisions on national regulation. Almost all respondents referred to the fact that the (voluntary) standards and guidelines of Codex are referenced by the (binding) Agreements of the WTO, and observed that without a Codex standard, national governments were likely to be vulnerable to challenges at the WTO (more detail in following section).
However, Codex processes were seen by public health actors—particularly academics—to tend towards resulting in guidance that reflected the “lowest common denominator”. Several respondents articulated a contrast with the WHO’s Framework Convention on Tobacco Control, which was seen as a reference for strengthening public health action and leadership; whereas Codex guidance was more commonly seen as a reflection or codification of existing practice. Four public health respondents also identified instances of industry actors (who were often more knowledgeable about detail and implications of Codex guidance than public officials) effectively using Codex strategically: alleging to government actors that certain public health measures were non-compliant with Codex, even when the legal implications of Codex guidance at the national level were unclear.
There was consistent articulation by respondents of the need for Codex guidance to support effective and contextually appropriate approaches to FoP nutrition labelling. All respondents identified the objective of preventing diet-related NCDs as important, and all but a few perceived FoP nutrition labelling as an effective measure to achieve this aim. Almost all respondents indicated Codex guidance done “well” would strengthen and expand FoP nutrition labelling action, because of its role in providing a reference to countries and protection from trade challenges, but there was a preference by many respondents for a “non-prescriptive” guideline. Three respondents from multilateral institutions specifically highlighted the value of broad guidance that identified core principles as a common starting point for developing regulation. However, there was some disagreement about whether it would be appropriate for Codex guidance to stipulate process requirements, with three respondents referring to the EU’s process-oriented guidance on FoP nutrition labelling as a potential model, and others raising concerns that this would place onerous requirements on countries with low resources.
All but a few respondents highlighted the divergence between industry-preferred and public health-preferred approaches to labelling, with public health respondents often characterizing industry-preferred approaches as “complex” or “weak”. All the public health respondents identified a risk that “poor” Codex guidance could limit or constrain policy space for countries desiring to implement innovative, mandatory, and/or strongly interpretive (rather than descriptive) forms of labelling.
3.2. The Global Regime Complex for FoP Nutrition Labelling
A regime complex is characterized by partially overlapping and nonhierarchical institutions, including more than one international agreement or authority [
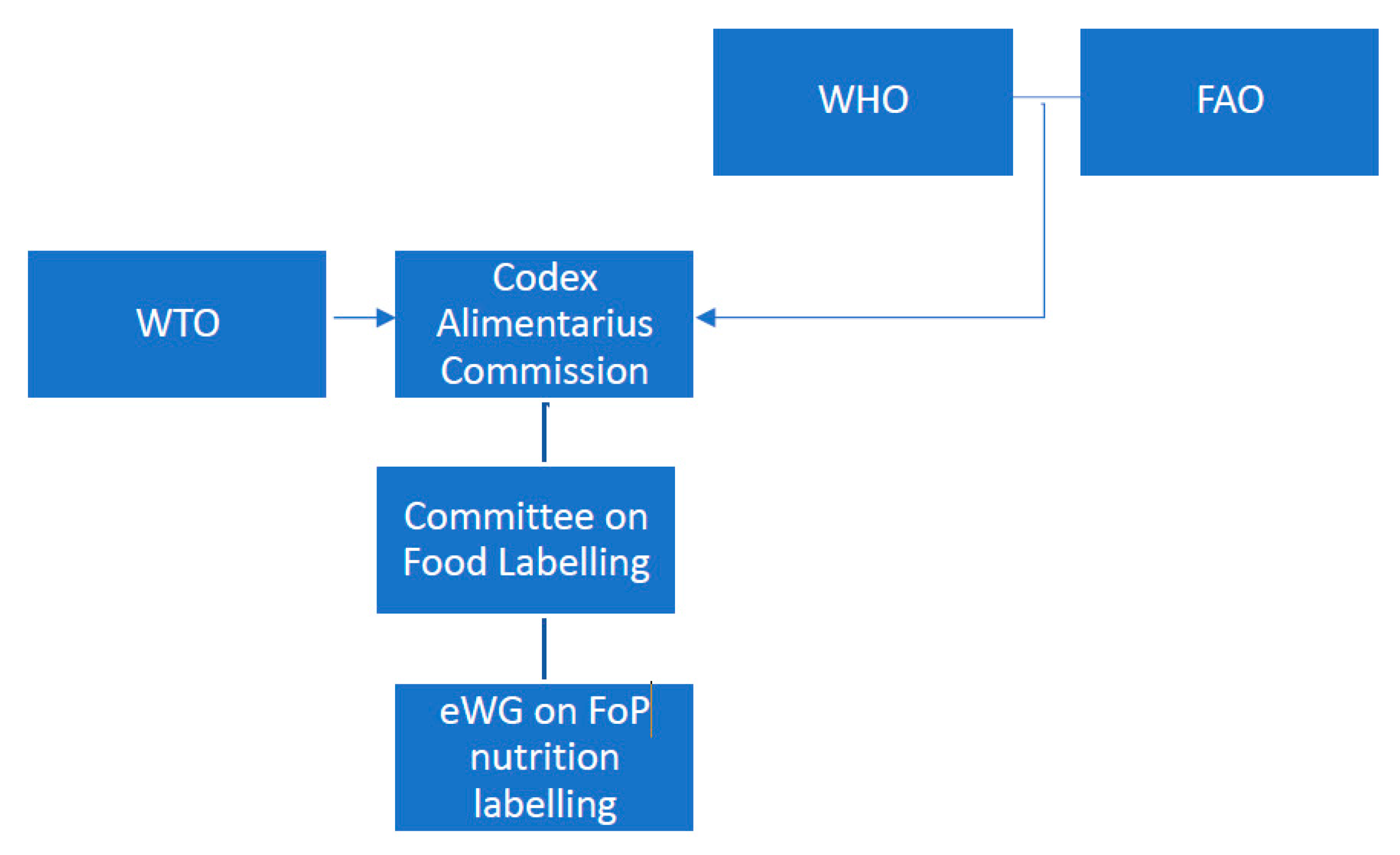
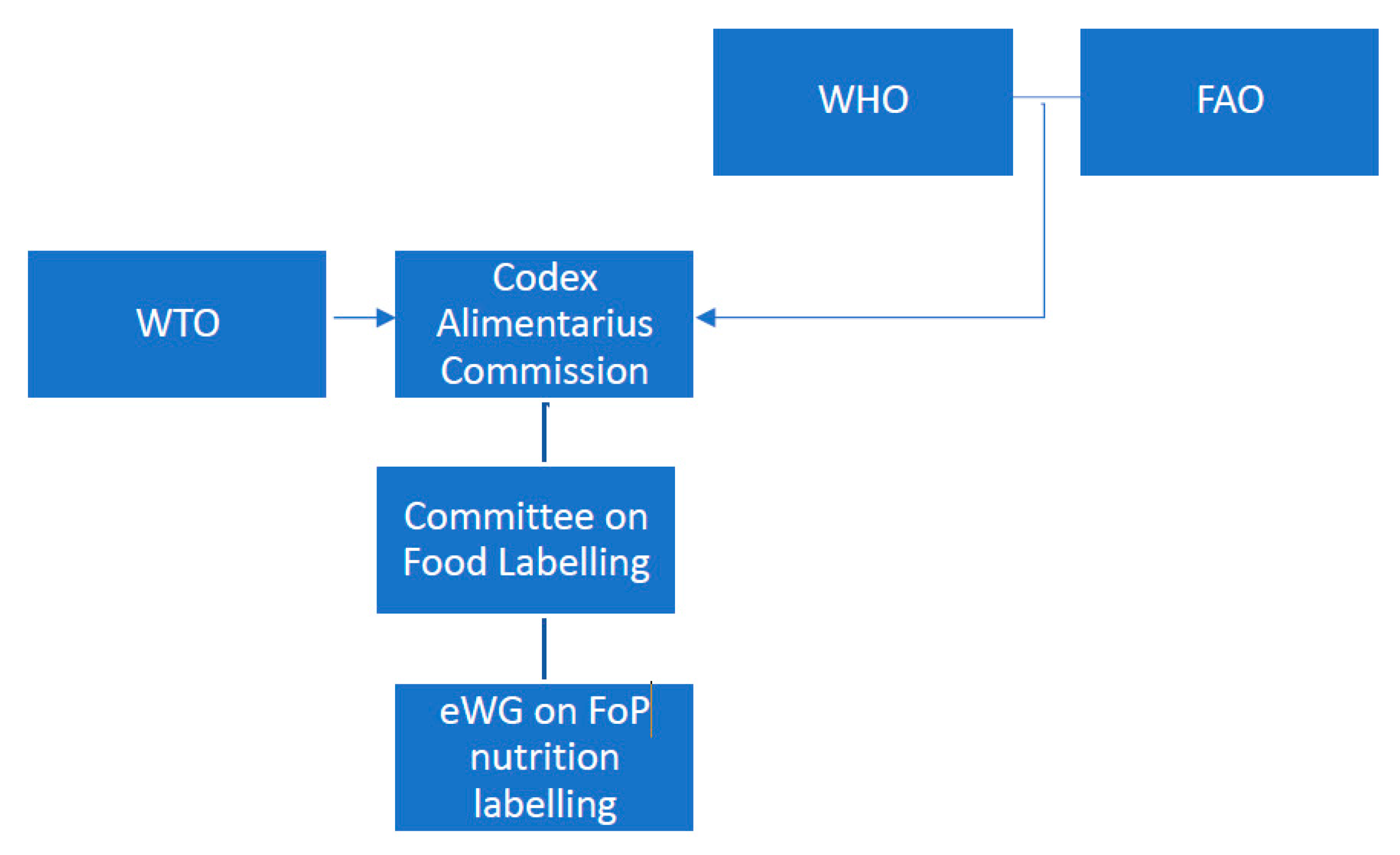
27]. The four institutions identified by respondents as core to the global governance of FoP nutrition labelling were Codex, the WTO, the WHO, and the FAO.
Codex was consistently identified as an appropriate forum for international discussions and guidance on FoP nutrition labelling due to its historical responsibilities for standards and guidance on food labelling, and its status as a standards-setting body according to the Agreements of the WTO. However, public health respondents (from NGOs, academia and WHO) raised concerns about the structure of Codex and its appropriateness as a forum for making decisions on NCD prevention policy. Codex was repeatedly described as at the interface between science and politics and/or trade and health. This reflected the tensions between Codex’s status as both an intergovernmental (UN) body, and a science-based standards-setting body, and its dual mandate of promoting trade and protecting consumer health. These were described by many respondents as necessary tensions—reflecting similar tensions faced by national governments in achieving both trade and health objectives—but also as limiting the ability of Codex to fully champion effective public health measures.
Public health respondents indicated that these tensions were compounded by the presence of (food) industry actors as formal participants in Codex decision-making processes, both as observers and as members of country delegations. Almost all public health respondents and those from consumer-oriented NGOs raised concerns regarding conflicts of interest arising from industry participation in Codex decision-making. Almost all public health respondents drew attention to the imbalance of representation between public health actors and food industry actors at Codex, including in the eWG on FoP nutrition labelling, as likely to favor industry preferences in resultant guidance. Several respondents, particularly from multilateral institutions, highlighted that there was also often limited participation by LMIC governments. One respondent suggested that this may result in inappropriate standards for these countries.
There was an interesting juxtaposition, noted above, of Codex as influential but lacking leadership. This was identified as a limitation in responding to the “new” challenge of diet-related NCDs in a forum with an historical responsibility for food safety. Several respondents also pointed out that the nature of risk as historically assessed by Codex processes related to acute and direct risks associated with food safety, and that this was inappropriate in the context of NCDs, where risk is long term and multi-factorial. In line with this, five Codex-affiliated respondents (from national Codex Contact Points and Codex secretariat) indicated that they were doubtful of the effectiveness of FoP nutrition labelling in addressing obesity and NCDs.
All respondents identified the epidemiological and nutrition transition—characterized by an increased prevalence of diet-related NCDs globally—as a key contextual factor leading to a (for some respondents “urgent”) need for nutrition policy action. Two respondents identified the current back of pack nutrient information panels used in most countries, which are already subject to Codex guidance, as inadequate and/or ineffective in promoting healthier diets. One public health respondent specifically drew attention to the difference between a consumer-rights approach to labelling, focused on providing understandable information to consumers (this echoed comments by the 2 consumer NGOs), and a public health approach, which goes beyond this to actively promote healthier choices.
However, almost all respondents intimated that the primary reason that FoP nutrition labelling was on the Codex agenda was concerns about trade and harmonization. These consisted of industry concerns relating to the consistency of requirements in export markets and the concerns raised by government representatives in the WTO, in which the current guidance on supplementary nutrition labelling was implicitly identified as insufficient.
The primacy of concerns about trade and industry related issues was also evident in framing by some respondents (non-public health)—and frames used by industry actors that had been observed by public health respondents—of FoP nutrition labelling as a “restrictive regulatory measure” that was being implemented in unnecessarily diverse approaches that had associated risks of limiting trade. These actors also emphasized the importance of harmonization to reduce barriers to trade. Three respondents (non-public health) emphasized that labelling is only one intervention and by itself would not “solve obesity”.
A significant part of the influence of Codex on national policy was attributed to its reference by the Agreements of the WTO; this relationship was mentioned by all except one respondent. Codex is not the only standards-setting body referenced by the TBT—the Agreement under which specific trade concerns relating to FoP labelling have been raised—but it is the only food standards body that meets requirements. These include being an “open” organization, which involves all relevant stakeholders (in particular, government, industry, and civil society), which was identified by a few non-public health respondents as a specific strength of Codex.
The relationship between the WHO and Codex—and the WHO’s interest in FoP nutrition labelling—was mentioned by all respondents. Eight of the public health respondents mentioned the WHO’s work on nutrient profiling and FoP nutrition labelling as relevant, and indicated that the WHO guideline development related to FoP nutrition labelling should be referenced in the Codex guidance. The WHO was described as a significant point of reference or source of normative guidance on technical issues, with some respondents indicating a role for the WHO in sharing best practice and lessons for health policy development. The WHO was cited by several respondents as having a sole mandate for public health, in contrast to Codex’s dual mandate. However, WHO respondents highlighted that, in contrast to Codex, the WHO does not provide a legal framework. This statement likely refers to the requirement by the Agreements of the WTO that recognized international standards-setting bodies have “open” membership enabling input from all relevant stakeholders (i.e., from all WTO members) [
28].
Nine respondents mentioned FAO, and six of these respondents described it as a relative newcomer to issues of nutrition relevant to diet-related NCDs. It was also identified by a few respondents as having more of a trade and industry mandate than a health focus.
All respondents also noted that different Ministries and Departments are sent to represent national governments in these global decision-making bodies, specifically: Agriculture at FAO, Health at the WHO, Trade at the WTO, and a mix at Codex. One respondent highlighted that as a result, countries can end up taking different stances in different forums. For example, at the one might see unanimous support for FoP nutrition labelling from member states and the World Health Assembly, while at the same time, the same countries raise concerns over FoP standards in trade forums. This is exacerbated when national delegations to Codex include industry or food sector representatives. Countries that had existing FoP nutrition labelling schemes in place were identified by several respondents as more likely to be highly engaged in Codex processes.
3.3. Power and Influence at Codex
Country delegations were identified consistently as the actual decision makers at Codex (i.e., with voting rights). However, all public health respondents identified industry as strongly influential in Codex decision-making processes. Avenues for influence spanned national and global forums, and sources of influence identified included relational, knowledge-based, and financial resources that enabled participation in decision-making, all of which were seen as imbalanced between public health and industry actors.
3.3.1. Avenues for Influence
Most respondents identified country delegations as most influential at Codex, as they are the actual decision makers. However, respondents also identified avenues for influence by non-government actors, including lobbying and participation in formal decision-making forums, at the national government level as well as directly in Codex (both as part of member state delegations and as official observers).
Many of the LMIC respondents identified strong industry lobbying at the national level as a strategy to influence decisions relating to FoP labelling. Two respondents from Latin American countries described specific instances of “corrupt approaches” to incentivize officials to prevent adoption of policies that would reduce consumption of foods associated with diet-related NCDs, including FoP nutrition labelling and marketing restrictions.
Several public health respondents also observed differences in the targets of industry and public health lobbying at the national level, with industry having access to economic policy actors who were perceived to be more influential than health actors in setting government decision-making. One respondent mentioned that in advocating for FoP nutrition labelling at the regional level she was told to speak to health officials, whereas industry actors lobbying against public health proposals for FoP nutrition labelling spoke to trade and industry officials. One public health respondent had also observed bilateral and “backroom” industry/government negotiations that were not always visible.
This “selection” of targets for lobbying was also identified as one potential driver for locating the mandate for setting FoP standards with Codex, rather than a public health agency such as the WHO. It was noted that national Codex Contact Points and negotiators were often situated in Ministries of Industry/Commerce or Agriculture, and only rarely in Ministries of Health. This was described as often leading to a focus in discussions at Codex on trade and industry aspects of standard and guideline development, rather than health implications. National Standards Committees also often include industry representation. One public health respondent specifically attributed the selection of Codex as the forum for discussion to industry being “afraid” of warning label approaches that could prove to be effective public health measures and therefore likely to reduce profits.
Observers at Codex were identified by 11 of the public health respondents to be heavily weighted towards food industry participation, and one noted that only two of the 15 observers to the initial eWG were non-industry. In addition, the inclusion of industry representatives—and more rarely, non-industry actors—in national Codex delegations was identified by public health respondents as a highly influential avenue, although, the Codex Contact Point representatives interviewed stated that industry representatives did not influence decisions.
Two public health interviewees, however, noted that Codex committees seemed cognizant of the imbalance between industry and public health voices, and had observed committees actively pursuing and attempting to give greater attention to comments by NGO observers at Codex discussions in general.
3.3.2. Sources of Influence
In addition to the relational and access-based sources of influence identified in the previous section, the two main sources of influence described by respondents related to knowledge and financial resources.
Large, high-income countries with their own labelling in place were identified as exercising influence based on their expertise, particularly technical expertise housed in regulatory agencies, and their experience with FoP nutrition labelling development and implementation. However, four public health respondents suggested that Codex member states—particularly LMICs—were not always knowledgeable about the implications of Codex guidance, and industry is often more aware of potential implications and better able to identify and lobby for outcomes that protect their interests. Respondents observed that industry actors were often positioned as technical experts, and used this positioning to engage with decision makers. A few public health respondents noted that in economic and trade-oriented forums (the orientation of many of the relevant Codex decision makers) industry arguments relating to economic impacts were considered more favorably than in public health forums.
In contrast, five public health respondents identified a lack of awareness and knowledge of Codex by the NCD-related public health community as a reason for their limited influence. Unlike industry, relevant public health actors were not familiar with Codex governance structures and avenues for engagement. In fact, two of these respondents suggested that many public health practitioners and researchers were not even aware of discussions in Codex regarding FoP nutrition labelling. Public health actors were thus not well organized to participate and exert influence on the discussions.
Respondents from multilateral organizations emphasized the strong scientific basis that underpinned Codex guidance. Respondents suggested that public health influence was constrained by the limited and only emerging evidence base for the effect of FoP nutrition labelling. However, three public health respondents also identified industry funded research as casting doubt on public health research findings, similar to experiences with tobacco control. While a range of countries have conducted their own research to adopt context specific approaches, it was unclear how Codex processes would take this evidence into account in developing guidance.
Different levels of financial resources available to different actors were also identified by respondents as another source of actor influence on decisions at Codex, but one which was strongly inter-related with relational influence and knowledge.
Three respondents highlighted that development of standards and guidelines require a high level of human resources and technical capacity to develop and implement. As a result, LMICs and small countries can be more influenced by global guidance, because of their low capacity, whereas high-income countries have relatively less need for international guidance, as they have resources and expertise. In the case of FoP nutrition labelling, several respondents pointed out that LMICs are also differentially affected by NCDs, because of insufficient resources within health systems, and due to this may have a greater desire to adopt FoP nutrition labelling schemes as part of NCD prevention strategies.
However, respondents from multilateral institutions and academia pointed out that financial resources also dictate the scale of participation in Codex by member states and observers due to the multiple (in-person) meetings and long time frames for decision-making, which span multiple meetings. LMICs are thus less likely to participate consistently. This leads to an imbalance between influence on, and outcomes of, standards development: countries with fewer resources are more likely to want Codex guidance, but also less likely to have the technical expertise and ability to be present for discussion and development of such guidance.
Respondents from public health also commented on an imbalance between industry and public health participation at Codex. A few respondents noted that industry actors have a significant business motive to be engaged in Codex discussions and devote funding to participate. They also have extensive technical expertise in their particular interest area. In contrast, several respondents noted that public health actors from both government and non-government have a fraction of the resources and are spread very thin, across all Codex issues. There is thus an imbalance of power in both knowledge and in the requirement for engagement. As one public health respondent put it, “industry can pick and choose” the issues they engage on, whereas the Ministry of Health must be across a wide range of food-related public health issues.


{kind=link}