Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Exposure Measures
2.2. Outcome Measures
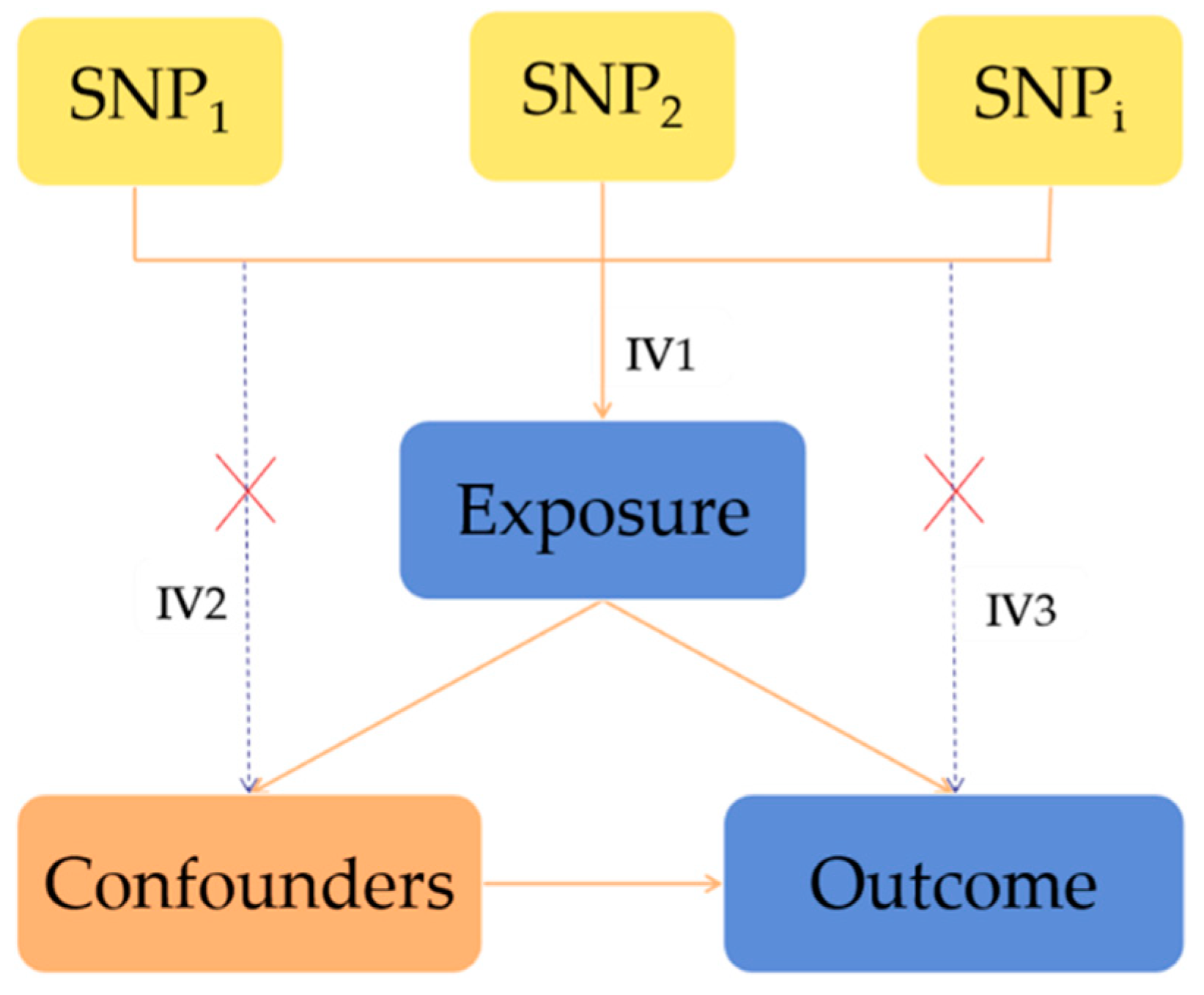
2.3. Statistical Analysis for Mendelian Randomization
3. Results
3.1. Causality between Minerals and Osteoporosis
3.2. Causality between Minerals and Gout
3.3. Causality between Minerals and Rheumatoid Arthritis
3.4. Causality between Minerals and Type 2 Diabetes
3.5. Causality between Minerals and Neurological Diseases
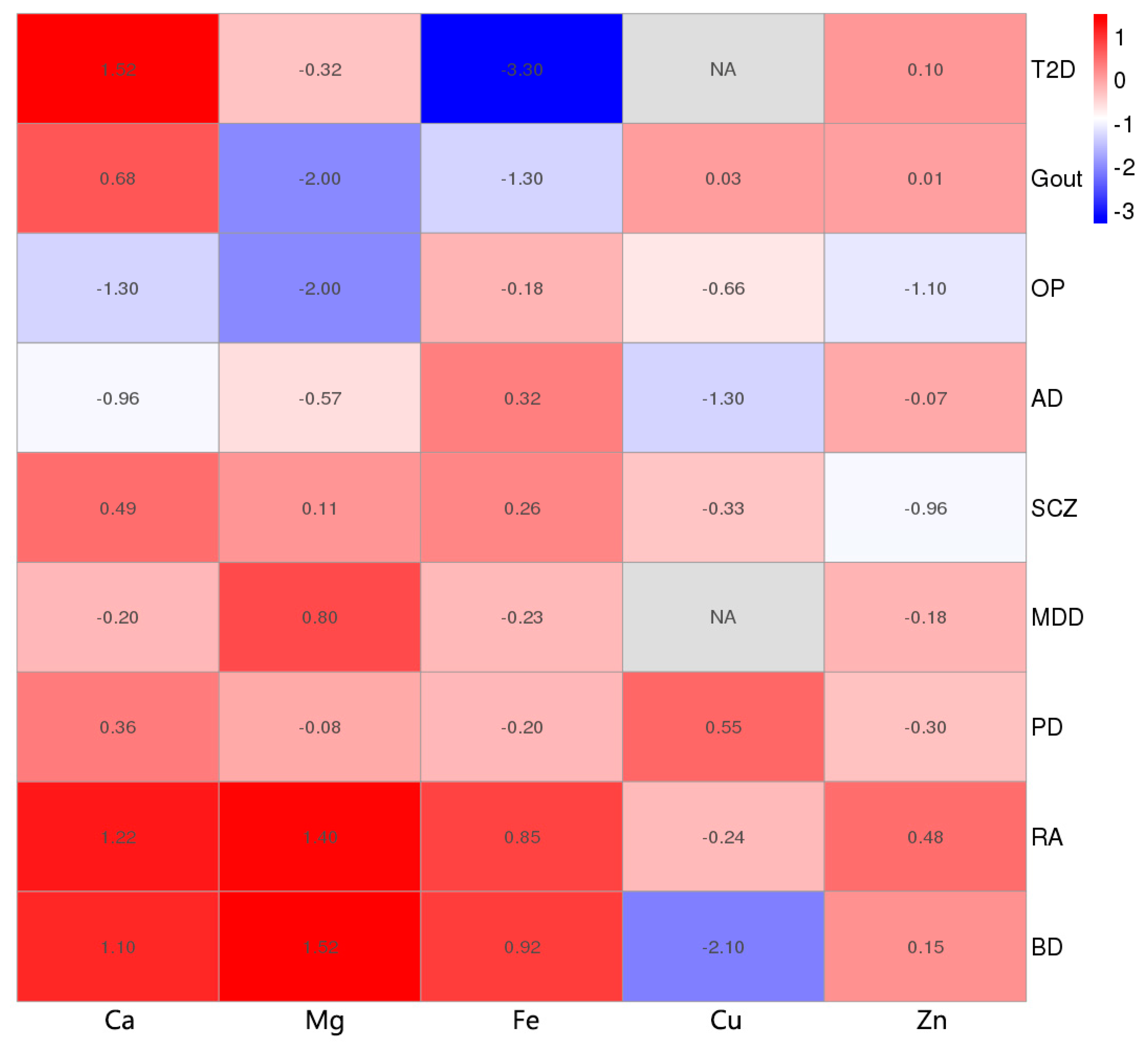
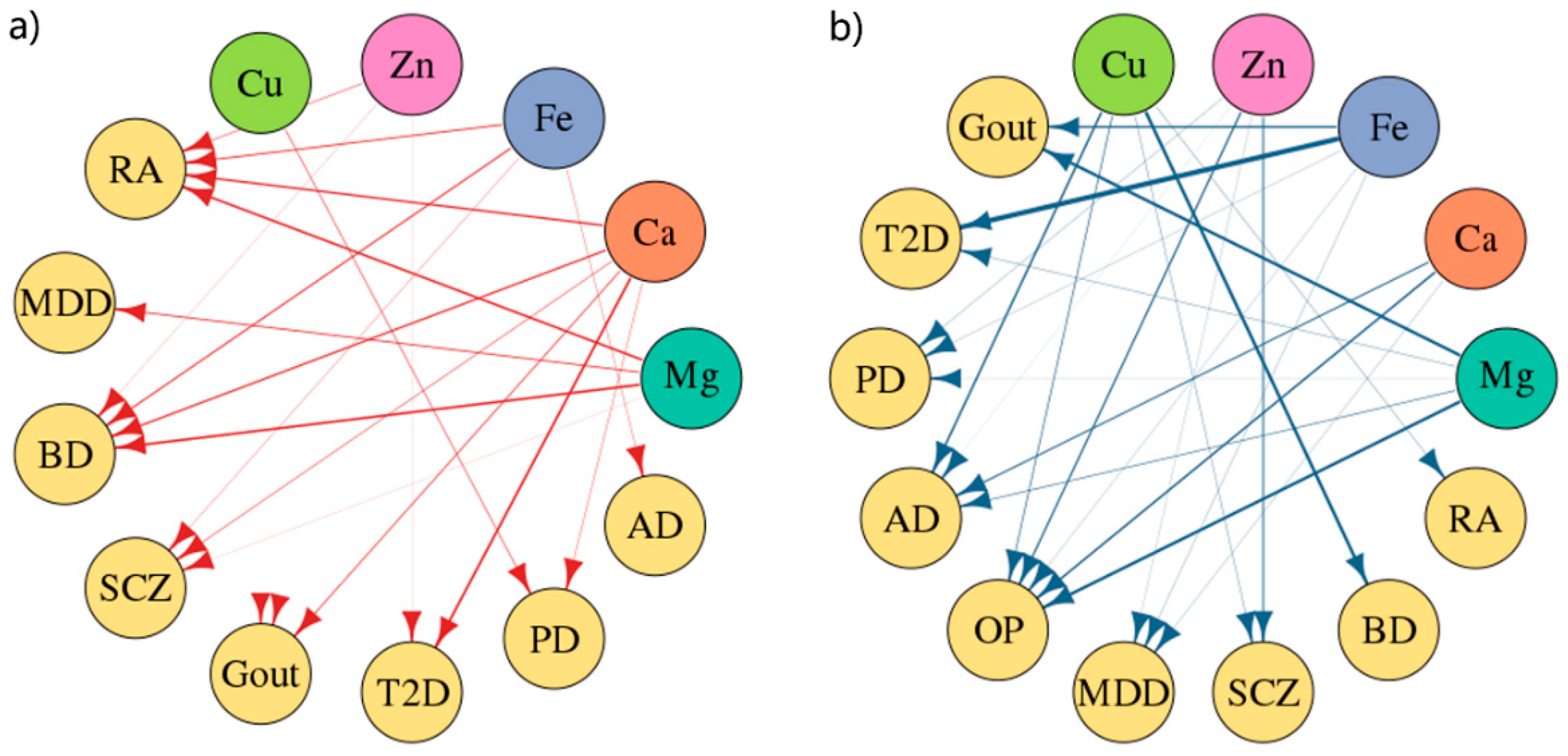
3.6. Causality between Minerals and Nine Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hodgson, N.A.; Gitlin, L.N.; Winter, L.; Czekanski, K. Undiagnosed illness and neuropsychiatric behaviors in community residing older adults with dementia. Alzheimer Dis. Assoc. Disord. 2011, 25, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Quintanilha, B.J.; Reis, B.Z.; Gbs, D.; Smf, C.; Rogero, M.M. Nutrimiromics: Role of microRNAs and Nutrition in Modulating Inflammation and Chronic Diseases. Nutrients 2017, 9, 1168. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Gao, Y.T.; Dai, Q.; Yang, G.; Cai, H.; Li, H.; Zheng, W.; Shu, X.O. Dietary calcium and magnesium intakes and the risk of type 2 diabetes: The Shanghai Women’s Health Study. Am. J. Clin. Nutr. 2009, 89, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Laukkanen, J.A. Low serum magnesium levels are associated with increased risk of fractures: A long-term prospective cohort study. Eur. J. Epidemiol. 2017, 32, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Cherbuin, N.; Kumar, R.; Sachdev, P.S.; Anstey, K.J. Dietary Mineral Intake and Risk of Mild Cognitive Impairment: The PATH through Life Project. Front. Aging Neurosci. 2014, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, B.; Song, X.; Zhang, D. Dietary zinc and iron intake and risk of depression: A meta-analysis. Psychiatry Res. 2017, 251, 41–47. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, A.T.; Assuncao, A.A.Q.; Foschetti, D.A.; Uchoa, F.N.M.; Alves, N.; Aragao, K.S. Assessment of nutritional and biochemical status in patients with rheumatoid arthritis undergoing pharmacological treatment. A pilot study. Int. J. Clin. Exp. Med. 2016, 9, 4282–4290. [Google Scholar]
- Smith, G.D.; Ebrahim, S. Data dredging, bias, or confounding. BMJ 2002, 325, 1437–1438. [Google Scholar] [CrossRef] [PubMed]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Baird, D.; Borges, M.C.; Bowden, J.; Hemani, G.; Haycock, P.; Evans, D.M.; Smith, G.D. Recent Developments in Mendelian Randomization Studies. Curr. Epidemiol. Rep. 2017, 4, 330–345. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S.; Michaelsson, K. Genetic association between adiposity and gout: A Mendelian randomization study. Rheumatology 2018, 57, 2145–2148. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Traylor, M.; Malik, R.; Dichgans, M.; Burgess, S.; Markus, H.S.; CoSTREAM Consortium, on behalf of the International Genomics of Alzheimer’s Project. Modifiable pathways in Alzheimer’s disease: Mendelian randomisation analysis. BMJ 2017, 359. [Google Scholar] [CrossRef] [PubMed]
- Kodali, H.P.; Pavilonis, B.T.; Schooling, C.M. Effects of copper and zinc on ischemic heart disease and myocardial infarction: A Mendelian randomization study. Am. J. Clin. Nutr. 2018, 108, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Yin, P.; Anttila, V.; Siewert, K.M.; Palotie, A.; Davey Smith, G.; Voight, B.F. Serum calcium and risk of migraine: A Mendelian randomization study. Hum. Mol. Genet. 2017, 26, 820–828. [Google Scholar]
- Lawlor, D.A. Commentary: Two-sample Mendelian randomization: Opportunities and challenges. Int. J. Epidemiol. 2016, 45, 908–915. [Google Scholar] [CrossRef] [PubMed]
- O’Seaghdha, C.M.; Wu, H.; Yang, Q.; Kapur, K.; Guessous, I.; Zuber, A.M.; Kottgen, A.; Stoudmann, C.; Teumer, A.; Kutalik, Z.; et al. Meta-analysis of genome-wide association studies identifies six new Loci for serum calcium concentrations. PLoS Genet. 2013, 9. [Google Scholar] [CrossRef]
- Meyer, T.E.; Verwoert, G.C.; Hwang, S.J.; Glazer, N.L.; Smith, A.V.; van Rooij, F.J.; Ehret, G.B.; Boerwinkle, E.; Felix, J.F.; Leak, T.S.; et al. Genome-wide association studies of serum magnesium, potassium, and sodium concentrations identify six Loci influencing serum magnesium levels. PLoS Genet. 2010, 6. [Google Scholar] [CrossRef]
- Benyamin, B.; Esko, T.; Ried, J.S.; Radhakrishnan, A.; Vermeulen, S.H.; Traglia, M.; Gogele, M.; Anderson, D.; Broer, L.; Podmore, C.; et al. Novel loci affecting iron homeostasis and their effects in individuals at risk for hemochromatosis. Nat. Ccommun. 2014, 5, 4926. [Google Scholar] [CrossRef]
- Evans, D.M.; Zhu, G.; Dy, V.; Heath, A.C.; Madden, P.A.; Kemp, J.P.; McMahon, G.; St Pourcain, B.; Timpson, N.J.; Golding, J.; et al. Genome-wide association study identifies loci affecting blood copper, selenium and zinc. Hum. Mol. Genet. 2013, 22, 3998–4006. [Google Scholar]
- Zheng, H.F.; Forgetta, V.; Hsu, Y.H.; Estrada, K.; Rosello-Diez, A.; Leo, P.J.; Dahia, C.L.; Park-Min, K.H.; Tobias, J.H.; Kooperberg, C.; et al. Whole-genome sequencing identifies EN1 as a determinant of bone density and fracture. Nature 2015, 526, 112–117. [Google Scholar] [CrossRef]
- Kottgen, A.; Albrecht, E.; Teumer, A.; Vitart, V.; Krumsiek, J.; Hundertmark, C.; Pistis, G.; Ruggiero, D.; O’Seaghdha, C.M.; Haller, T.; et al. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations. Nat. Genet. 2013, 45, 145–154. [Google Scholar] [CrossRef]
- Okada, Y.; Wu, D.; Trynka, G.; Raj, T.; Terao, C.; Ikari, K.; Kochi, Y.; Ohmura, K.; Suzuki, A.; Yoshida, S.; et al. Genetics of rheumatoid arthritis contributes to biology and drug discovery. Nature 2014, 506, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Xue, A.; Wu, Y.; Zhu, Z.; Zhang, F.; Kemper, K.E.; Zheng, Z.; Yengo, L.; Lloyd-Jones, L.R.; Sidorenko, J.; Wu, Y.; et al. Genome-wide association analyses identify 143 risk variants and putative regulatory mechanisms for type 2 diabetes. Nat. Commun. 2018, 9, 2941. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.C.; Ibrahim-Verbaas, C.A.; Harold, D.; Naj, A.C.; Sims, R.; Bellenguez, C.; DeStafano, A.L.; Bis, J.C.; Beecham, G.W.; Grenier-Boley, B.; et al. Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s disease. Nat. Genet. 2013, 45, 1452–1458. [Google Scholar] [CrossRef] [PubMed]
- Bipolar Disorder and Schizophrenia Working Group of the Psychiatric Genomics Consortium. Genomic Dissection of Bipolar Disorder and Schizophrenia, Including 28 Subphenotypes. Cell 2018, 173, 1705–1715. [Google Scholar]
- Pankratz, N.; Beecham, G.W.; DeStefano, A.L.; Dawson, T.M.; Doheny, K.F.; Factor, S.A.; Hamza, T.H.; Hung, A.Y.; Hyman, B.T.; Ivinson, A.J.; et al. Meta-analysis of Parkinson’s disease: Identification of a novel locus, RIT2. Ann. Neurol. 2012, 71, 370–384. [Google Scholar] [CrossRef] [PubMed]
- CONVERGE Consortium. Sparse whole-genome sequencing identifies two loci for major depressive disorder. Nature 2015, 523, 588–591. [Google Scholar] [CrossRef]
- Pierce, B.L.; Burgess, S. Efficient design for Mendelian randomization studies: Subsample and 2-sample instrumental variable estimators. Am. J. Epidemiol. 2013, 178, 1177–1184. [Google Scholar] [CrossRef]
- Hartwig, F.P.; Davies, N.M.; Hemani, G.; Davey Smith, G. Two-sample Mendelian randomization: Avoiding the downsides of a powerful, widely applicable but potentially fallible technique. Int. J. Epidemiol. 2016, 45, 1717–1726. [Google Scholar] [CrossRef]
- Bowden, J.; Davey Smith, G.; Haycock, P.C.; Burgess, S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet. Eepidemiol. 2016, 40, 304–314. [Google Scholar] [CrossRef]
- Burgess, S.; Thompson, S.G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Eepidemiol. 2017, 32, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Bowden, J.; Davey Smith, G.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Siwek, M.; Styczen, K.; Sowa-Kucma, M.; Dudek, D.; Reczynski, W.; Szewczyk, B.; Misztak, P.; Opoka, W.; Topor-Madry, R.; Nowak, G. The serum concentration of magnesium as a potential state marker in patients with diagnosis of bipolar disorder. Psychiatr. Pol. 2015, 49, 1277–1287. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.A.; Skinner, J.; Hickson, M. Dietary Magnesium May Be Protective for Aging of Bone and Skeletal Muscle in Middle and Younger Older Age Men and Women: Cross-Sectional Findings from the UK Biobank Cohort. Nutrients 2017, 9, 1189. [Google Scholar] [CrossRef] [PubMed]
- Smorgon, C.; Mari, E.; Atti, A.R.; Nora, E.D. Trace elements and cognitive impairment: An elderly cohort study. Arch. Gerontol. Geriatr. 2004, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Styczen, K.; Sowa-Kucma, M.; Dudek, D.; Siwek, M.; Reczynski, W.; Szewczyk, B.; Misztak, P.; Topor-Madry, R.; Opoka, W.; Nowak, G. Zinc and copper concentration do not differentiate bipolar disorder from major depressive disorder. Psychiatr. Pol. 2018, 52, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Siwek, M.; Styczen, K.; Sowa-Kucma, M.; Dudek, D.; Reczynski, W.; Szewczyk, B.; Misztak, P.; Opoka, W.; Topor-Madry, R.; Nowak, G.; et al. The serum concentration of copper in bipolar disorder. Psychiatr. Pol. 2017, 51, 469–481. [Google Scholar] [CrossRef]
- Kim, K.N.; Oh, S.Y.; Hong, Y.C. Associations of serum calcium levels and dietary calcium intake with incident type 2 diabetes over 10 years: The Korean Genome and Epidemiology Study (KoGES). Diabetol. Metab. Syndr. 2018, 10. [Google Scholar] [CrossRef]
- Zhao, Z.; Li, S.; Liu, G.; Yan, F.; Ma, X.; Huang, Z.; Tian, H. Body iron stores and heme-iron intake in relation to risk of type 2 diabetes: A systematic review and meta-analysis. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Podmore, C.; Meidtner, K.; Schulze, M.B.; Scott, R.A.; Ramond, A.; Butterworth, A.S.; Di Angelantonio, E.; Danesh, J.; Arriola, L.; Barricarte, A.; et al. Association of Multiple Biomarkers of Iron Metabolism and Type 2 Diabetes: The EPIC-InterAct Study. Diabetes care 2016, 39, 572–581. [Google Scholar] [CrossRef]
- Burgess, S.; Scott, R.A.; Timpson, N.J.; Smith, G.D.; Thompson, S.G.; Consortium, E.I. Using published data in Mendelian randomization: A blueprint for efficient identification of causal risk factors. Eur. J. Epidemiol. 2015, 30, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Neeland, I.J.; Kozlitina, J. Mendelian Randomization: Using Natural Genetic Variation to Assess the Causal Role of Modifiable Risk Factors in Observational Studies. Circulation 2017, 135, 755–758. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Tchetgen Tchetgen, E.J.; Cornelis, M.; Kraft, P. Methodological challenges in mendelian randomization. Epidemiology 2014, 25, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.R.; Minelli, C.; Bowden, J.; Del Greco, F.M.; Gill, D.; Jones, E.M.; Shapland, C.Y.; Sheehan, N.A. Mendelian randomization incorporating uncertainty about pleiotropy. Stat. Med. 2017, 36, 4627–4645. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.D.; Ebrahim, S. Mendelian randomization: Prospects, potentials, and limitations. Int. J. Epidemiol. 2004, 33, 30–42. [Google Scholar] [CrossRef]
- Burgess, S.; Thompson, S.G.; Collaboration, C.C.G. Avoiding bias from weak instruments in Mendelian randomization studies. Int. J. Epidemiol. 2011, 40, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, D.I.; Kuchenbaecker, K.B.; Shah, S.; Sofat, R.; Holmes, M.V.; White, J.; Mindell, J.S.; Kivimaki, M.; Brunner, E.J.; Whittaker, J.C.; et al. Selecting instruments for Mendelian randomization in the wake of genome-wide association studies. Int. J. Epidemiol. 2016, 45, 1600–1616. [Google Scholar] [CrossRef]
- Burgess, S.; Dudbridge, F.; Thompson, S.G. Combining information on multiple instrumental variables in Mendelian randomization: Comparison of allele score and summarized data methods. Stat. Med. 2016, 35, 1880–1906. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure | Number of SNPs | Number of Independent SNPs | Sample Size | Race |
|---|---|---|---|---|
| Ca | 8 | 8 | 39,400 | Mix + Europe |
| Mg | 5 | 5 | 15,366 | Europe |
| Fe | 14 | 11 | 48,972 | Europe |
| Cu | 2 | 2 | 2603 | Australia |
| Zn | 3 | 2 | 2603 | Australia |
| Sample Size | ||||
|---|---|---|---|---|
| Outcome | Total | Cases | Controls | Race |
| OP | 561,489 | 508,253 | 53,236 | Europe |
| GOUT | 69,374 | 2115 | 67,259 | Europe |
| RA | 103,638 | 29,880 | 73,758 | Europe |
| T2D | 659,316 | 62,892 | 596,424 | Europe |
| AD | 54,162 | 17,008 | 37,154 | Europe |
| BD | 41,653 | 20,129 | 21,524 | Mix |
| SCZ | 65,967 | 33,426 | 32,541 | Europe |
| PD | 14,326 | 7976 | 6350 | Mix |
| MDD | 10,640 | 5303 | 5337 | Asia |
| MR-Egger | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 6 | IVW | 0.39 | 0.15, 1.07 | 0.068 | 8.02 (0.16) | ||
| MR-Egger | 27.00 | 0.13, 5581.5 | 0.292 | 4.94 (0.29) | −0.080 | 0.190 | ||
| WM | 0.37 | 0.14, 1.02 | 0.054 | |||||
| Mg | 4 | IVW | 0.10 | 0.02, 0.63 | 0.014 | 3.43 (0.33) | ||
| WM | 0.10 | 0.01, 0.82 | 0.032 | |||||
| Fe | 9 | IVW | 0.98 | 0.81, 1.19 | 0.815 | 14.78 (0.06) | ||
| MR-Egger | 1.71 | 0.68, 1.69 | 0.781 | 14.39 (0.04) | −0.008 | 0.680 | ||
| WM | 0.96 | 0.80, 1.15 | 0.661 | |||||
| Cu | 2 | IVW | 0.93 | 0.83, 1.04 | 0.221 | 1.25 (0.26) | ||
| Zn | 2 | IVW | 0.91 | 0.82, 1.01 | 0.077 | 0.03 (0.86) | ||
| MR-Egger | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 7 | IVW | 2.84 | 0.45, 17.92 | 0.267 | 20.76 (0.002) | ||
| MR-Egger | 1.24 | 0.04, 38.29 | 0.908 | 19.47 (0.002) | 0.029 | 0.589 | ||
| WM | 2.12 | 0.66, 6.83 | 0.206 | |||||
| Mg | 5 | IVW | 0.33 | 0.05, 2.08 | 0.236 | 15.29 (0.004) | ||
| MR-Egger | 0.15 | 0.01, 2.09 | 0.253 | 12.36 (0.006) | 0.038 | 0.461 | ||
| WM | 0.26 | 0.09, 0.76 | 0.013 | |||||
| Fe | 11 | IVW | 0.86 | 0.71, 1.04 | 0.117 | 6.34 (0.786) | ||
| MR-Egger | 0.71 | 0.53, 0.95 | 0.047 | 3.50 (0.941) | 0.027 | 0.126 | ||
| WM | 0.81 | 0.63, 1.03 | 0.091 | |||||
| Cu | 2 | IVW | 1.01 | 0.80, 1.28 | 0.928 | 0.26 (0.607) | ||
| Zn | 2 | IVW | 1.01 | 0.69. 1.47 | 0.971 | 2.77 (0.096) | ||
| MR-Egger | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 6 | IVW | 1.83 | 0.99, 3.41 | 0.055 | 3.40 (0.638) | ||
| MR-Egger | 2.42 | 0.80, 7.35 | 0.194 | 3.05 (0.549) | −0.01 | 0.59 | ||
| WM | 1.93 | 0.94, 3.94 | 0.073 | |||||
| Mg | 4 | IVW | 3.07 | 0.16, 58.62 | 0.457 | 8.11 (0.044) | ||
| WM | 8.94 | 1.06, 75.70 | 0.044 | |||||
| Fe | 11 | IVW | 1.01 | 0.82, 1.25 | 0.913 | 42.22 (6.84 × 10−6) | ||
| MR-Egger | 1.19 | 0.90, 1.57 | 0.262 | 33.21 (1.23 × 10−4) | −0.03 | 0.15 | ||
| WM | 1.12 | 0.97, 1.29 | 0.138 | |||||
| Cu | 2 | IVW | 0.94 | 0.77, 1.16 | 0.579 | 2.26 (0.13) | ||
| Zn | 2 | IVW | 1.07 | 0.94, 1.22 | 0.328 | 0.54 (0.46) | ||
| MR-Egger | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 7 | IVW | 0.88 | 0.34, 2.27 | 0.80 | 99.35 (3.43 × 10−19) | ||
| MR-Egger | 2.82 | 0.75, 10.58 | 0.19 | 52.98 (3.40 × 10−10) | −0.040 | 0.090 | ||
| WM | 1.36 | 1.03, 1.79 | 0.03 | |||||
| Mg | 3 | IVW | 1.55 | 0.26, 9.24 | 0.63 | 7.99 (0.02) | ||
| WM | 0.64 | 0.18, 2.22 | 0.48 | |||||
| Fe | 10 | IVW | 0.89 | 0.81, 0.98 | 0.01 | 41.06 (4.87 × 10−6) | ||
| MR-Egger | 0.93 | 0.82, 1.07 | 0.36 | 35.87 (1.85 × 10−5) | −0.008 | 0.310 | ||
| WM | 0.91 | 0.86, 0.96 | 5.32 × 10−4 | |||||
| Zn | 2 | IVW | 1.01 | 0.92, 1.12 | 0.79 | 3.77 (0.05) | ||
| Outcome: AD | ||||||||
| MR-Egger | ||||||||
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’sQ Statistic(p Value) | Intercept | Intercept p Value |
| Ca | 6 | IVW | 0.74 | 0.45, 1.22 | 0.23 | 4.08 (0.54) | ||
| MR-Egger | 0.46 | 0.19, 1.14 | 0.17 | 2.62 (0.62) | 0.020 | 0.29 | ||
| WM | 0.64 | 0.37, 1.10 | 0.11 | |||||
| Mg | 4 | IVW | 0.43 | 0.08, 2.44 | 0.34 | 1.16 (0.76) | ||
| WM | 0.30 | 0.04, 2.53 | 0.27 | |||||
| Fe | 11 | IVW | 1.04 | 0.94, 1.14 | 0.48 | 8.35 (0.59) | ||
| MR-Egger | 1.02 | 0.88, 1.17 | 0.82 | 8.24 (0.51) | 0.005 | 0.75 | ||
| WM | 1.03 | 0.92, 1.15 | 0.62 | |||||
| Cu | 2 | IVW | 0.87 | 0.75, 1.00 | 0.05 | 1.72 (0.20) | ||
| Zn | 2 | IVW | 0.99 | 0.85, 1.14 | 0.85 | 1.96 (0.16) | ||
| Outcome: BD | ||||||||
| MR-Egger | ||||||||
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 7 | IVW | 1.85 | 0.74, 4.65 | 0.19 | 23.99 (5.25 × 10−4) | ||
| MR-Egger | 1.27 | 0.22, 7.29 | 0.80 | 22.79 (3.70 × 10−4) | 0.013 | 0.63 | ||
| WM | 1.63 | 0.94, 2.82 | 0.08 | |||||
| Mg | 4 | IVW | 8.78 | 1.16, 66.26 | 0.04 | 4.66 (0.198) | ||
| WM | 8.02 | 0.91, 70.43 | 0.06 | |||||
| Fe | 11 | IVW | 1.07 | 0.89, 1.29 | 0.45 | 41.0 (1.13 × 10−5) | ||
| MR-Egger | 1.07 | 0.8, 1.43 | 0.66 | 40.99 (5.01 × 10−6) | 0.0005 | 0.97 | ||
| WM | 1.10 | 0.98, 1.23 | 0.12 | |||||
| Cu | 2 | IVW | 0.87 | 0.79, 0.97 | 0.01 | 0.15 (0.70) | ||
| Zn | 2 | IVW | 1.02 | 0.91, 1.14 | 0.70 | 1.24 (0.27) | ||
| Outcome: SCZ | ||||||||
| MR-Egger | ||||||||
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 7 | IVW | 0.81 | 0.53, 1.23 | 0.32 | 7.48 (0.28) | ||
| MR-Egger | 1.05 | 0.49, 2.25 | 0.91 | 6.63 (0.25) | −0.009 | 0.46 | ||
| WM | 0.93 | 0.6, 1.45 | 0.75 | |||||
| Mg | 4 | IVW | 0.87 | 0.24, 3.19 | 0.83 | 2.31 (0.51) | ||
| WM | 0.79 | 0.15, 4.07 | 0.77 | |||||
| Fe | 10 | IVW | 1.04 | 0.92, 1.18 | 0.55 | 12.6 (0.18) | ||
| MR-Egger | 0.91 | 0.69, 1.22 | 0.55 | 11.27 (0.19) | 0.01 | 0.36 | ||
| WM | 1.01 | 0.88, 1.16 | 0.85 | |||||
| Cu | 2 | IVW | 0.96 | 0.85, 1.08 | 0.47 | 2.22 (0.14) | ||
| Zn | 2 | IVW | 0.94 | 0.86, 1.02 | 0.11 | 1.02 (0.31) | ||
| Outcome: PD | ||||||||
| MR-Egger | ||||||||
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 7 | IVW | 1.57 | 0.49, 5.02 | 0.44 | 8.05 (0.23) | ||
| MR-Egger | 1.34 | 0.14, 12.65 | 0.81 | 8.01 (0.16) | 0.005 | 0.87 | ||
| WM | 1.53 | 0.47, 4.95 | 0.48 | |||||
| Mg | 5 | IVW | 0.92 | 0.35, 2.42 | 0.86 | 1.32 (0.86) | ||
| MR-Egger | 0.96 | 0.26, 3.59 | 0.95 | 1.31 (0.73) | −0.002 | 0.93 | ||
| WM | 0.90 | 0.32, 2.52 | 0.84 | |||||
| Fe | 11 | IVW | 0.95 | 0.78, 1.16 | 0.63 | 10.17 (0.43) | ||
| MR-Egger | 0.99 | 0.72, 1.35 | 0.94 | 10.06 (0.35) | −0.005 | 0.76 | ||
| WM | 1.06 | 0.82, 1.36 | 0.65 | |||||
| Cu | 2 | IVW | 1.13 | 0.91,1.41 | 0.28 | 0.39 (0.53) | ||
| Zn | 2 | IVW | 0.92 | 0.71,1.18 | 0.50 | 1.36 (0.24) | ||
| Outcome: MDD | ||||||||
| MR-Egger | ||||||||
| Mineral | Number of SNPs | MR Method | OR | 95% CI | p Value | Cochran’s Q Statistic (p Value) | Intercept | Intercept p Value |
| Ca | 6 | IVW | 0.92 | 0.67, 1.28 | 0.63 | 3.54 (0.62) | ||
| MR-Egger | 1.16 | 0.56, 2.38 | 0.71 | 3.06 (0.55) | −0.005 | 0.53 | ||
| WM | 1.01 | 0.68, 1.51 | 0.95 | |||||
| Mg | 3 | IVW | 1.19 | 0.22, 6.61 | 0.84 | 7.06 (0.03) | ||
| WM | 2.25 | 0.72, 7.06 | 0.17 | |||||
| Fe | 9 | IVW | 0.98 | 0.91, 1.05 | 0.60 | 1.57 (0.99) | ||
| MR-Egger | 0.98 | 0.83, 1.02 | 0.85 | 1.57 (0.98) | −0.0002 | 0.97 | ||
| WM | 0.98 | 0.9, 1.07 | 0.72 | |||||
| Zn | 2 | IVW | 0.99 | 0.95, 1.03 | 0.66 | 0.004 (0.95) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, W.-W.; Zhu, Q.; Zhang, H.-Y. Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study. Nutrients 2019, 11, 378. https://doi.org/10.3390/nu11020378
Cheng W-W, Zhu Q, Zhang H-Y. Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study. Nutrients. 2019; 11(2):378. https://doi.org/10.3390/nu11020378
Chicago/Turabian StyleCheng, Wen-Wen, Qiang Zhu, and Hong-Yu Zhang. 2019. "Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study" Nutrients 11, no. 2: 378. https://doi.org/10.3390/nu11020378
APA StyleCheng, W.-W., Zhu, Q., & Zhang, H.-Y. (2019). Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study. Nutrients, 11(2), 378. https://doi.org/10.3390/nu11020378