Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions

 ,
, 
 ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
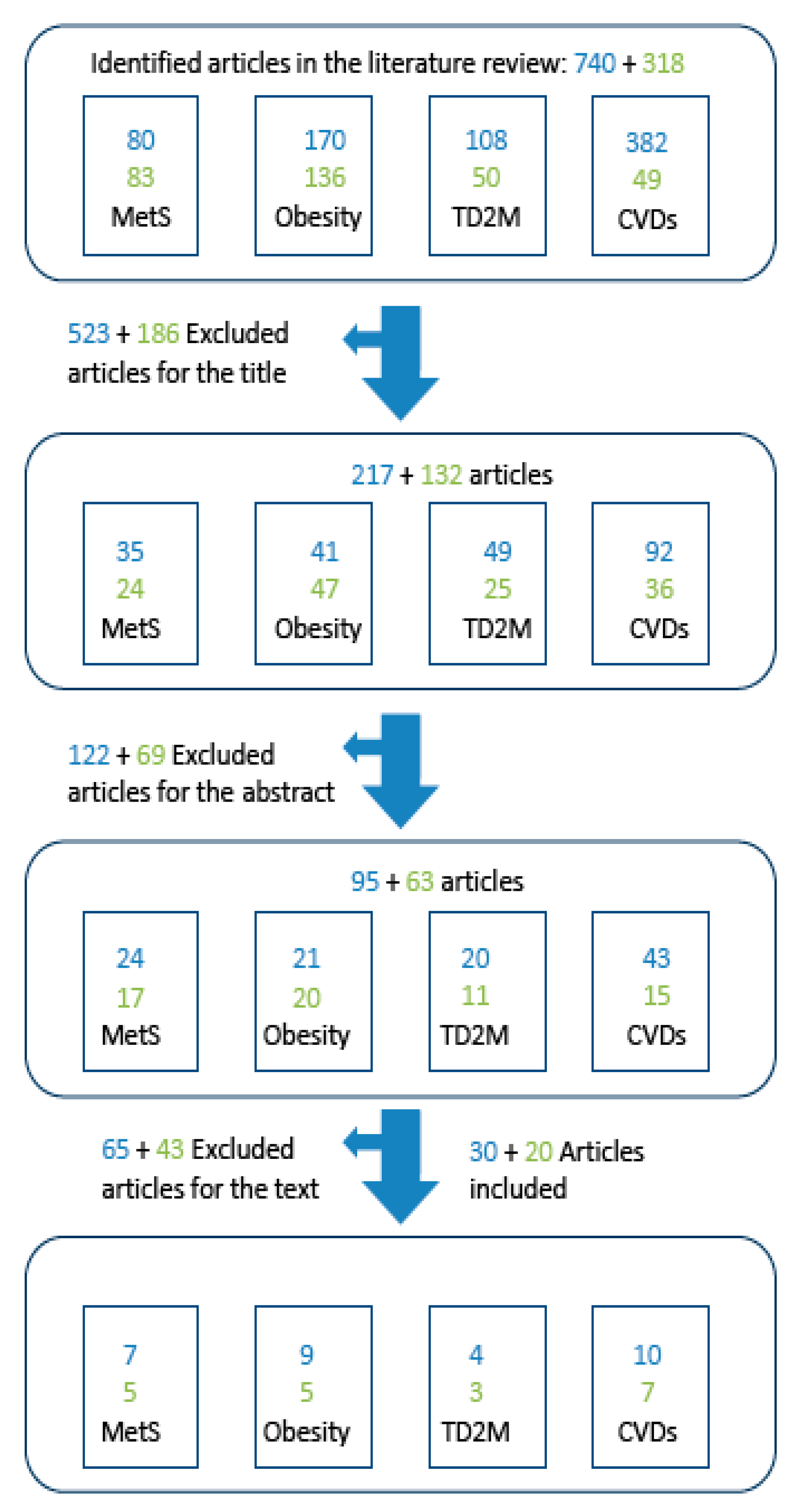
2.1. Literature Search
2.2. Inclusion Criteria
3. Results
3.1. CQ 1: What Effect Does the MedDiet Have on Weight Reduction in Overweight and Obese Patients?
3.2. CQ 2: What Effect Does the MedDiet Have on the Incidence and Prevention of T2DM?
3.3. CQ 3: What Effect Does the MedDiet Have on Established MetS or on the Risk of Developing MetS?
3.4. CQ 4: What Effect Does the MedDiet Have on the Prevention of CVD and the Modulation of Disease Course?
3.5. CQ 5: What Effect Does the MedDiet Have on Weight Gain and Abdominal Adiposity in Healthy Individuals and Individuals Without Overweight?
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-Analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M.; Serra-Majem, L.; Lairon, D.; Estruch, R.; Trichopoulou, A. Mediterranean food pattern and the primary prevention of chronic disease: Recent developments. Nutr. Rev. 2009, 67, S111–S116. [Google Scholar] [CrossRef]
- Trichopoulou, A. From research to education: The Greek experience. Nutrition 2000, 16, 528–531. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health benefits of the Mediterranean diet: Metabolic and molecular mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D. Cardiodiabetes—Is a joint approach the way forward? Br. J. Cardiol. 2008, 15, S8–S10. [Google Scholar]
- Garcia-Fernandez, E.; Rico-Cabanas, L.; Rosgaard, N.; Estruch, R.; Bach-Faig, A. Mediterranean diet and cardiodiabesity: A review. Nutr. Rev. 2014, 6, 3474–3500. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org (accessed on 30 January 2018).
- Di Cesare, M.; Bentham, J.; Stevens, G.; Zhou, B.; Danaei, G.; Lu, Y.; Bixby, H.; Cowan, M.J.; Riley, L.M.; Hajifathalian, K.; et al. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Millen, B.E.; Abrams, S.; Adams-Campbell, L.; Anderson, C.A.; Brenna, J.T.; Campbell, W.W.; Clinton, S.; Hu, F.; Nelson, M.; Neuhouser, M.L.; et al. The 2015 Dietary Guidelines Advisory Committee Scientific Report: Development and Major Conclusions. Adv. Nutr. 2016, 7, 438–444. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomized trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Popkin, B.M. The nutrition transition in the developing world. Dev. Policy. Rev. 2003, 21, 581–597. [Google Scholar] [CrossRef]
- Popkin, B.M.; Gordon-Larsen, P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int. J. Obes. 2004, 28, s2. [Google Scholar] [CrossRef]
- Sentenach-Carbo, A.; Batlle, C.; Franquesa, M.; García-Fernandez, E.; Rico, L.; Shamirian-Pulido, L.; Pérez, M.; Deu-Valenzuela, E.; Ardite, E.; Funtikova, A.N.; et al. Adherence of Spanish Primary Physicians and Clinical Practise to the Mediterranean Diet. Eur. J. Clin. Nutr. 2018. [Google Scholar] [CrossRef]
- Popkin, B.M.; Duffey, K.; Gordon Larsen, P. Environmental influences on food choice, physical activity and energy balance. Physiol. Behav. 2005, 86, 603–613. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee to Advise the Public Health Service on Clinical Practice Guidelines. Clinical Practice Guidelines: Directions for a New Program; Field, M.J., Lohr, K.N., Eds.; National Academies Press: Washington, DC, USA, 1990. Available online: https://www.ncbi.nlm.nih.gov/books/NBK235751/doi:10.17226/1626 (accessed on 20 July 2017).
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in healthcare. Can. Med. Assoc. 2010, 182, 839–842. [Google Scholar] [CrossRef]
- Working Group for CPG Updates. Updating Clinical Practice Guidelines in the National Health System: Methodology Handbook. National Health System Quality Plan of the Spanish Ministry of Health and Social Policy. Aragon Health Sciences Institute (I+CS) Clinical Practice Guidelines in the National Health System: I+CS No.2007/02-01. 2009. Available online: http://www.guiasalud.es/emanuales/traduccion/ingles/manual_actualizacion/documentos/MMA_VersionEnglish_DEFINITIVA_10122_FIN.pdf (accessed on 20 July 2017).
- Andreoli, A.; Lauro, S.; di Daniele, N.; Sorge, R.; Celi, M.; Volpe, S.L. Effect of a moderately hypoenergetic Mediterranean diet and exercise program on body cell mass and cardiovascular risk factors in obese women. Eur. J. Clin. Nutr. 2008, 62, 892–897. [Google Scholar] [CrossRef]
- Hadžiabdić, M.O.; Vitali Cepo, D.; Rahelić, D.; Božikov, V. The Effect of the Mediterranean Diet on Serum Total Antioxidant Capacity in Obese Patients: A Randomized Controlled Trial. J. Am. Coll. Nutr. 2015, 35, 224–351. [Google Scholar] [CrossRef]
- Ruiz-Canela, M.; Zazpe, I.; Shivappa, N.; Hébert, J.R.; Sanchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Fito, M.; Lamuela-Raventos, R.M.; Rekondo, J.; et al. Dietary inflammatory index and anthropometric measures of obesity in a population sample at high cardiovascular risk from the PREDIMED (PREvención con DIeta MEDiterránea) trial. Br. J. Nutr. 2015, 113, 984–995. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Pérez, J.; Sánchez-Villegas, A.; Díaz-Benítez, E.M.; Ruano-Rodríguez, C.; Corella, D.; Martínez-González, M.Á.; Estruch, R.; Salas-Salvadó, J.; Serra-Majem, L. Influence of a Mediterranean Dietary Pattern on Body Fat Distribution: Results of the PREDIMED-Canarias Intervention Randomized Trial. J. Am. Coll. Nutr. 2016, 35, 568–580. [Google Scholar] [CrossRef]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status PREDIMED in the randomized trial. CMAJ 2014, 186, 649–657. [Google Scholar] [CrossRef]
- Gómez-Huelgas, R.; Short-Jansen, S.; Baca-Osorio, A.J.; Mancera-Romero, J.; Tinahones, F.J.; Bernal-Lopez, M.R. Effects of long-term lifestyle intervention with Mediterranean diet and exercise program for the Management of Patients with metabolic syndrome in a primary care setting. Eur. J. Intern. Med. 2015, 26, 317–323. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services; US Department of Agriculture. Nutrition and Your Health: Dietary Guidelines for Americans [Internet]. 1st Edition. 1980. Available online: http://health.gov/dietaryguidelines/1980thin.pdf (accessed on 1 August 2017).
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2018, 368, 1279–1290, Retraction and republication in 2018, 378, 2441–2442. [Google Scholar] [CrossRef]
- Nissensohn, M.; Viñas-Román, B.; Sánchez-Villegas, A.; Piscopo, S.-; Serra-Majem, L. The Effect of the Mediterranean Diet on Hypertension: A Systematic Review and Meta-Analysis. J. Nutr. Educ. Behav. 2016, 48, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Menotti, A.; Alberti-Fidanza, A.; Fidanza, F.; Lantian, M.; Fruttini, D. Factor analysis in the identification of dietary patterns and their predictive role in morbid and fatal events. Public Health Nutr. 2012, 15, 1232–1239. [Google Scholar] [CrossRef]
- Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Tormo, M.J.; Sánchez, M.J.; Rodríguez, L.; Quirós, J.R.; Navarro, C.; Molina, E.; Martínez, C.; Marín, P.; et al. Major dietary patterns and risk of coronary heart disease in middle-aged persons from a Mediterranean country: The EPIC-Spain cohort study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 192–199. [Google Scholar] [CrossRef]
- Gardener, H.; Wright, C.B.; Gu, Y.; Demmer, R.T.; Boden-Albala, B.; Elkind, M.S.; Sacco, R.L.; Scarmeas, N. Mediterranean-style diet and risk of ischemic stroke, myocardial infarction, and vascular death: The Northern Manhattan Study. Am. J. Clin. Nutr. 2011, 94, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Naska, A.; Orfanos, P.; Trichopoulos, D. Mediterranean diet in relation to body mass index and waist-to-hip ratio: The Greek European Prospective Investigation into Cancer and Nutrition Study. Am. J. Clin. Nutr. 2005, 82, 935–940. [Google Scholar] [CrossRef]
- Kastorini, C.-M.; Panagiotakos, D.B.; Chrysohoou, C.; Georgousopoulou, E.; Pitaraki, E.; Puddu, P.E.; Tousoulis, D.; Stefanadis, C.; Pitsavos, C. Metabolic syndrome, adherence to the Mediterranean diet and 10-year cardiovascular disease incidence: The ATTICA study. Atherosclerosis 2016, 246, 87–93. [Google Scholar] [CrossRef]
- Turati, F.; Dilis, V.; Rossi, M.; Lagiou, P.; Benetou, V.; Katsoulis, M.; Naska, A.; Trichopoulos, D.; La Vecchia, C.; Trichopoulou, A. Glycemic load and coronary heart disease in a Mediterranean population: The Greek EPIC cohort study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.A.; Wallentin, L.; Benatar, J.; Danchin, N.; Hagström, E.; Held, C.; Husted, S.; Lonn, E.; Stebbins, A.; Chiswell, K.; et al. Dietary patterns and the risk of major adverse cardiovascular events in a global study of high-risk Patients with stable coronary heart disease. Eur. Heart J. 2016, 37, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.M.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; Donati, M.B.; De Gaetano, G.; Iacoviello, L. Adherence to the Mediterranean diet is associated with reduced overall mortality in subjects with diabetes. Prospective results from the Moli-sani study. Eur. J. Cardiol. Prev. 2014, 21, S55. [Google Scholar]
- Stefler, D.; Malyutina, S.; Kubinova, R.; Pajak, A.; Peasey, A.; Pikhart, H.; Brunner, E.J.; Bobak, M. Mediterranean diet score and total and cardiovascular mortality in Eastern Europe: The HAPIEE study. Eur. J. Nutr. 2015, 56, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavost, C.; Chrysohoou, C.; Stefanadis, C. The epidemiology of Type 2 diabetes mellitus in adults Greek: The ATTICA study. Diabet. Med. 2005, 22, 1581–1588. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; de la Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.Á.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. PREDIMED Study Investigators. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: Results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care 2011, 34, 14–19. [Google Scholar]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analysis. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of Mediterranean diet in diabetes control and cardiovascular risk modification: A systematic review. Front. Public Health 2015, 3, 69. [Google Scholar] [CrossRef]
- Abiemo, E.E.; Alonso, A.; Nettleton, J.A.; Steffen, L.M.; Bertoni, A.G.; Jain, A.; Lutsey, P.L. Relationships of the Mediterranean dietary pattern with insulin resistance and diabetes incidence in the Multi-Ethnic Study of Atherosclerosis (MESA). Br. J. Nutr. 2013, 109, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Bellastella, G.; Petrizzo, M.; Scappaticcio, L.; Giugliano, D.; Esposito, K. Anti-inflammatory Effect of Mediterranean Diet in Type 2 Diabetes Is Durable: 8-Year Follow-up of a Controlled Trial. Diabetes Care 2016, 39, 44–45. [Google Scholar] [CrossRef]
- Salas-Salvado, J.; Martin, M.; Ruiz-Gutie, V. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status. Arch. Inter. Med. 2013, 168, 2449–2458. [Google Scholar] [CrossRef] [PubMed]
- Alvarez León, E.; Henríquez, P.; Serra-Majem, L. Mediterranean diet and metabolic syndrome: A cross-sectional study in the Canary Islands. Public Health Nutr. 2006, 9, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Steffen, L.M.; Van Horn, L.; Daviglus, M.L.; Zhou, X.; Reis, J.P.; Loria, C.M.; Jacobs, D.R.; Duffey, K.J. A modified Mediterranean diet score is associated with a lower risk of incident metabolic syndrome over 25 years among young adults: The CARDIA (Coronary Artery Risk Development in Young Adults) study. Br. J. Nutr. 2014, 112, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Rumawas, M.E.; Meigs, J.B.; Dwyer, J.T.; McKeown, N.M.; Jacques, P.F. Mediterranean-style dietary pattern, reduced risk of metabolic syndrome traits, and incidence in the Framingham Offspring Cohort. Am. J. Clin. Nutr. 2009, 90, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Ahluwalia, N.; Lassale, C.; Hercberg, S.; Fezeu, L.; Lairon, D. Adherence to Mediterranean diet reduces the risk of metabolic syndrome: A 6-year prospective study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 677–683. [Google Scholar] [CrossRef]
- Mirmiran, P.; Moslehi, N.; Mahmoudof, H.; Sadeghi, M.; Azizi, F. A Longitudinal Study of Adherence to the Mediterranean Dietary Pattern and Metabolic Syndrome in a Mediterranean Non-Population. Int. J. Endocrinol. Metab. 2015, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Polystipioti, A.; Papairakleous, N.; Polychronopoulos, E. Long-Term adoption of a Mediterranean diet is associated with a better health status in elderly people; a cross-sectional survey in Cyprus. Asia Pac. J. Clin. Nutr. 2007, 16, 331–337. [Google Scholar] [PubMed]
- Eguaras, S.; Toledo, E.; Buil-Cosiales, P.; Salas-Salvadó, J.; Corella, D.; Gutierrez-Bedmar, M.; Santos-Lozano, J.M.; Arós, F.; Fiol, M.; Fitó, M.; et al. Does the Mediterranean diet counteract the adverse effects of abdominal adiposity? Nutr. Metabo. Cardiovasc. Dis. 2015, 25, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Urpí-Sardà, M.; Chiva-Blanch, G.; Ros, E.; Martínez-González, M.A.; Covas, M.I.; Lamuela-Raventos, R.M.; Salas-Salvadó, J.; Fiol, M.; et al. The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS ONE 2014, 9, e100084. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2015, 57, 3218–3232. [Google Scholar] [CrossRef]
- Menotti, A.; Alberti-Fidanza, A.; Fidanza, F. The association of the Mediterranean Adequacy Index with fatal coronary events in an Italian middle-aged male population followed for 40 years. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 369–375. [Google Scholar] [CrossRef]
- Menotti, A.; Puddu, P.E.; Maiani, G.; Catasta, G. Lifestyle behaviour and lifetime incidence of heart diseases. Int. J. Cardiol. 2015, 201, 293–299. [Google Scholar] [CrossRef]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef]
- Romaguera, D.; Norat, T.; Vergnaud, A.C.; Mouw, T.; May, A.M.; Agudo, A.; Buckland, G.; Slimani, N.; Rinaldi, S.; Couto, E.; et al. Mediterranean dietary patterns and prospective weight change in participants of the EPIC-PANACEA project. Am. J. Clin. Nutr. 2010, 92, 912–921. [Google Scholar] [CrossRef] [Green Version]
- Schröder, H.; Marrugat, J.; Vila, J.; Covas, M.I.; Elosua, R. Adherence to the traditional Mediterranean diet is inversely associated with body mass index and obesity in a Spanish population. J. Nutr. 2004, 134, 3355–3361. [Google Scholar] [CrossRef]
- Goulet, J.; Lamarche, B.; Nadeau, G.; Lemieux, S. Effect of a nutritional intervention promoting the Mediterranean food pattern on plasma lipids, lipoproteins and body weight in healthy French-Canadian women. Atherosclerosis 2003, 170, 115–124. [Google Scholar] [CrossRef]
- Paletas, K.; Athanasiadou, E.; Sarigianni, M.; Paschos, P.; Kalogirou, A.; Hassapidou, M.; Tsapas, A. The protective role of the Mediterranean diet on the prevalence of metabolic syndrome in a population of Greek obese subjects. J. Am. Coll. Nutr. 2010, 29, 41–45. [Google Scholar] [CrossRef]
- Romaguera, D.; Norat, T.; Mouw, T.; May, A.M.; Bamia, C.; Slimani, N.; Travier, N.; Besson, H.; Luan, J.; Wareham, N. Adherence to the Mediterranean diet is associated with lower abdominal adiposity in European men and women. J. Nutr. 2009, 139, 1728–1737. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2013, 29, 1–14. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Jüni, P.; Altman, D.G.; Egger, M. Systematic reviews in health care: Assessing the quality of controlled clinical trials. BMJ 2001, 323, 42–46. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Mejia, S.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Kendall, C.W.; Sievenpiper, J.L. DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef] [PubMed]
- Onvani, S.; Haghighatdoost, F.; Surkan, P.J.; Larijani, B.; Azadbakht, L. Adherence to the healthy eating index and alternative healthy eating index patterns and mortality from all causes, cardiovascular disease and cancer: A meta-analysis of observational studies. J. Hum. Nutr. Diet. 2017, 30, 216–226. [Google Scholar] [CrossRef]
- Babio, N.; Becerra-Tomás, N.; Martínez-González, M.Á.; Corella, D.; Estruch, R.; Ros, E.; Sayón-Orea, C.; Fitó, M.; Serra-Majem, L.; Arós, F.; et al. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [Green Version]
- Billingsley, H.E.; Carbone, S.; Lavie, C.J. Dietary Fats and Chronic Noncommunicable Diseases. Nutrients 2018, 10, 1385. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Galvano, F.; Pajak, A.; Mistretta, A. factors associated with metabolic syndrome in a Mediterranean population: Role of caffeinated beverages. J. Epidemiol. 2014, 24, 327–333. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Medina-Remón, A.; Lamuela-Raventós, R.M.; Bulló, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Gea, A.; Gómez-Gracia, E.; Lapetra, J.; et al. Moderate red wine consumption is associated with a lower prevalence of the metabolic syndrome in the PREDIMED population. Br. J. Nutr. 2015, 113, S121–S130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ros, E.; Santos-lozano, M. Frequent Consumption of Sugar- and Artificially Sweetened Beverages and Natural and Bottled Fruit Juices Is Associated with an Increased Risk of Metabolic Syndrome in a Mediterranean Population at High Cardiovascular Disease. J. Nutr. 2016, 46, 1528–1536. [Google Scholar]
- Funtikova, A.N.; Subirana, I.; Gomez, S.F.; Fitó, M.; Elosua, R.; Benítez-Arciniega, A.A.; Schröder, H. Soft Drink Consumption Is Positively Associated with Increased Waist Circumference and 10-Year Incidence of Abdominal Obesity in Spanish Adults. J. Nutr. 2014, 145, 328–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef] [PubMed]
- Malmir, H.; Saneei, P.; Larijani, B.; Esmaillzadeh, A. Adherence to Mediterranean diet in relation to bone mineral density and risk of fracture: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2018, 57, 2147–2160. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Medina, F.X. The Mediterranean Diet as an Intangible and Sustainable Food Culture. In The Mediterranean Diet: An Evidence-Based Approach, 1st ed.; Preedy, V.R., Watson, D.R., Eds.; Academic Press-Elsevier: London, UK, 2015; pp. 37–46. [Google Scholar]
- Medina, F.X. Mediterranean Diet, Culture and Heritage: Challenges for a New Conception. Public Health Nutr. 2009, 12, 1618–1620. [Google Scholar] [CrossRef]
- 2015–2020 Dietary Guidelines. Healthy Mediterranean-Style Eating Pattern [Internet]. Available online: https://health.gov/dietaryguidelines/2015/guidelines/chapter-1/examples-of-other-healthy-eating-patterns/ (accessed on 1 February 2019).
- Dernini, S.; Berry, E.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Trichopoulou, A. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef]
- Medina, F.X.; Aguilar, A.; Solé-Sedeno, J.M. Aspectos sociales y culturales sobre la obesidad: Reflexiones necesarias desde la salud pública. Nutr. Clin. Diet. Hosp. 2014, 34, 67–71. [Google Scholar]


{kind=link}
{kind=link}
| P: Who Are the Patients/Participants in the Study? | I: What Intervention Is Being Examined? | C: Against What is the Intervention of Interest Being Compared? | O: What Are the Measured Results (Outcomes)? | CQs |
|---|---|---|---|---|
| Men and women with overweight or obesity and/or MetS | Application of MedDiet and/or monitoring of MedDiet adherence | Epidemiologically similar control group that does not follow the MedDiet | Reduction in weight, BMI, and/or WC | CQ 1: What effect does the MedDiet have on weight reduction in overweight and obese patients? |
| Men and women with or at risk of T2DM | Application of MedDiet and/or monitoring of MedDiet adherence | Epidemiologically similar control group that does not follow the MedDiet | Reduction in risk of all-cause mortality and mortality due to CVD, heart attack, or T2DM | CQ 2: What effect does the MedDiet have on the incidence and prevention of T2DM? |
| Healthy men and women with MetS or risk factors for MetS | Application of MedDiet and/or monitoring of MedDiet adherence | Epidemiologically similar control group that does not follow the MedDiet | Reduction in incidence or severity of MetS | CQ 3: What effect does the MedDiet have on established MetS or on the risk of developing MetS? |
| Men and women | Application of MedDiet and/or monitoring of MedDiet adherence | Epidemiologically similar control group that does not follow the MedDiet | Reduction in CVD incidence or mortality | CQ 4: What effect does the MedDiet have on the prevention of CVD and the modulation of disease course? |
| Men and women | Application of MedDiet and/or monitoring of MedDiet adherence | Epidemiologically similar control group that does not follow the MedDiet | Reduction in weight gain, BMI, or WC | CQ 5: What effect does the MedDiet have on weight gain and abdominal adiposity in healthy individuals and individuals without overweight? |
| Item | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Adults (>18 years old) | Children Experimental animal studies |
| Intervention | Dietary interventions with the pure MedDiet (defined in the study) or the MedDiet with reinforcement of one of the food components (e.g., olive oil or nuts) No intervention (analysis of MedDiet adherence [defined in the study]) | Other food interventions and interventions involving specific foods even though they form part of the MedDiet. Other non-dietary interventions (e.g., pharmacological or surgical). |
| Comparator | Non-dietary intervention, prudent diet, Westernized diet, or any type of diet other than the MedDiet Non-adherence to the MedDiet | |
| Results (outcomes) | Weight reduction measured as weight (kg, lb, %), WC, hip-waist ratio, percentage of body fat, maintenance of weight loss Cardiovascular events: MI, heart failure, hospitalization for MI or heart failure Cardiovascular risk factors: total cholesterol factors, HDL-C, LDL-C, non-HDL-C, triglycerides, diabetes, smoking, CRP Morbidity: cardiovascular damage, chronic renal failure, non-alcoholic steatohepatitis, depression Mortality: CVD, all causes Changes in body composition: improved quality of life, functionality, disability | Self-reported weight |
| Time | No time limits Minimum 6-month follow-up | Fewer than 6 months of follow-up * |
| Study design | Systematic reviews and clinical trials | Other |
| Language | English | Other (despite availability of an English abstract) |
| Publication type | Systematic reviews and meta-analyses | Other |
| Publication date | From October 2013 to July 2016 | All others |
| Study Characteristics | Level of Evidence |
|---|---|
| • Well-designed, well-executed RCTs with assessment of health outcomes, representative of the populations to which the results apply • Meta-analyses of the aforementioned RCTs • High level of certainty about the estimated effects and very little likelihood that more research on the subject would alter this certainty | High |
| • RCTs with minor limitations affecting applicability of or confidence in the results • Meta-analysis of the aforementioned RCTs • Moderate certainty about the estimated effects and likelihood that more research on the subject would alter this certainty | Moderate |
| • RCTs with major limitations • Non-RCTs and observational studies with major constraints affecting applicability of or confidence in the results • Uncontrolled clinical studies without an adequate comparison group • Psychological studies in humans and meta-analyses of these • Low certainty about the estimated effects and strong likelihood that more research on the subject would alter this certainty | Low |
| Author, Year | Type of Study | Country | Sex, Age (y) and Number of Participants | Initial Disease | Follow-Up (y) | Components of MedDiet Index | Object of Study | Results | Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Ruiz-Canela et al., 2015 [21] | Multicenter parallel-group RCT (PREDIMED) | Spain | 3111 men (ages 55–80) 4125 women (ages 60–80) N total = 7236 | No CVD or T2DM but three risk factors for CVD: smoking, hypertension, high LDL-C, low HDL-C, BMI ≥ 25 kg/m2, family history of premature CVD | - | PREDIMED [26] | Obesity | Adjusted difference in WHtR for women and men between the highest and lowest quintiles of DII: 1.60% (95% CI, 0.87–2.33) and 1.04% (95% CI, 0.35–1.74), respectively | |
| Nissensohn et al., 2015 [27] | Systematic review and meta-analysis | Spain | Men and women (age not specified) N total > 7000 | Different depending on the study | >2 | Different depending on the study | Cardiodiabesity | MedDiet vs. low-fat diet: decrease in systolic and diastolic blood pressure | |
| Eguaras et al., 2015 [54] | RCT (PREDIMED) | Spain | 3241 men (ages 55–80) 4297 women (ages 60–80) N total = 7538 | High risk of CVD due to T2DM or presence of three risk factors for CVD | 4.8 | PREDIMED [26] | Obesity and CVD | Increased risk of CVD events was apparent for the highest vs. the lowest quartiles of WHtR (HR, 1.98; 95% CI, 1.10–3.57; linear trend: p = 0.019) only in control diet group | Age, sex, multivariate |
| Hadziabdic et al., 2016 [20] | Parallel-group RCT | Croatia | Men and women (ages 18–69) N total = 84 | Obesity (≥30 kg/m2) | 1 | (+) vegetables, fruit, whole grains, (-) red meat (+) fish and poultry. 1573 kcal/day 33 g of olive oil/day and 56 g of nuts/week | Obesity | MedDiet vs. low-fat diet: tendency towards high weight loss (kg) | |
| Alvarez-Perez et al., 2016 [22] | Multicenter, parallel-group RCT (PREDIMED) | Spain | Men (ages 55–80) and women (ages 60–80) N total = 305 | No CVD or T2DM but three risk factors for CVD: smoking, hypertension, high LDL-C, low HDL-C, overweight/obesity, family history of premature CVD | 1 | PREDIMED [26] | Obesity | Low-fat diet decreased total body weight but increased total body fat. MedDiet + nuts decreased total body weight. MedDiet + extra-virgin olive oil decreased total body weight, BMI, and WC. | Sex and age |
| Casas et al., 2014 [55] | Parallel-group RCT (PREDIMED) | Spain | 77 men and 87 women (average age 67.7) N total = 164 | No CVD or T2DM but three risk factors for CVD: smoking, hypertension, high LDL-C, low HDL-C, BMI ≥ 25 kg/m2, family history of premature CVD | 1 | PREDIMED [26] | CVD | MedDiet reduced systolic (p = 0.02) and diastolic (p = 0.02) blood pressure, total cholesterol (p = 0.04) and LDL-C by 5–9% (p = 0.04). MedDiet significantly reduced inflammatory markers (e.g., VCAM and ICAM) and adhesion molecules (e.g., CD40). | |
| Grosso et al., 2015 [56] | Systematic review and meta-analysis (20 studies) | Several | Men and women (ages 20–70) N total = 888,257 | Established CVD, risk factors for CVD, elderly | - | MedDiet | CVD | Higher MedDiet adherence was associated with a 40% relative risk reduction in CVD incidence and mortality. Reduced CVD risk for consumption of olive oil, vegetables, fruit, and pulses, and increased CVD risk for consumption of dairy products. No difference for consumption of fish, alcohol, cereals, or red meat. | |
| Bonaccio et al., 2014 [38] | Cohort study | Italy | 139 men and 643 women (average age 62.6) N total = 1995 | T2DM at the beginning of the study | 4 | EPIC-Trichopoulou score [65] | CVD and mortality | Higher MedDiet adherence was associated with a 37% relative risk reduction in CVD mortality and a 34% relative risk reduction in cerebrovascular-event mortality. Adherence to consumption of vegetables and olive oil reduced mortality by 21%. A reduction was observed only when CVD mortality was considered (HR, 0.66; 0.46–0.95). The MedDiet was associated with a reduced risk of death overall (HR, 0.81; 0.62–1.07). | Age, sex, education, oil intake, blood glucose |
| Menotti 2015 [59] | Prospective study of MedDiet adherence and lifestyle in Seven Countries CVD study | Italy | Men and women (age up to 90) N total = 1677 | General rural population | ≤50 | MedDiet: 18 food groups [29] | CVD | MedDiet adherence was associated with lower CVD incidence. Cox proportional HRs for CHD: 1.45 (95%, CI, 1.11–1.90) for heavy smokers vs. non-smokers; 0.67 (95% CI, 0.50–0.89) for vigorous activity vs. sedentary habits, and 0.62 (95% CI, 0.47–0.83) for MedDiet vs. non-MedDiet. | Smokers and physical activity |
| Stefler et al., 2015 [39] | Prospective study of HAPIEE cohort | Poland, Russia, and Czech Republic | 8787 men and 10,546 women (age not specified) N total = 19,333 | Absence of CVD and diabetes | 7 | MedDiet recommendations [66] with categorization of 17 points | CVD | One SD increase in MDS inversely associated with all-cause mortality (HR, 0.93; 95% CI, 0.88–0.98) and CVD (HR, 0.90; 95% CI, 0.81–0.99). Inverse but non-significant link found for CHD (HR, 0.90; 95% CI, 0.78–1.03) and stroke (HR, 0.87; 95% CI, 0.71–1.07). | |
| Turati et al., 2015 [36] | Prospective cohort study (EPIC) | Greece | 8246 men and 12,029 women (ages 20–86) N total = 20,275 | Absence of CVD, cancer, and diabetes | 10.4 | MedDiet defined according to Trichopoulou [65] | CVD | Significant positive association between glycemic load and CHD incidence (HR for highest vs. lowest tertiles, 1.41; 95% CI, 1.05–1.90). High MedDiet adherence with low/moderate glycemic load associated with lower risk of CHD incidence (HR, 0.61; 95% CI, 0.39–0.95) and mortality (HR, 0.47; 95% CI, 0.23–96). | Sex, BMI |
| Stewart et al., 2016 [37] | RCT | 30 countries | 12,556 men and 2926 women (average age 64.2) N total = 15,482 | Previous MI with a risk factor: > 60 years, DM under treatment, HDL-C < 1.03 mmol/L, smoker or ex-smoker, glomerular filtration rate > 30 < 60 mL/min or albuminuria or polyvascular disease | 3.7 | MedDiet defined according to Turati [36]. Eggs and dairy products not included. | CVD | MedDiet adherence (MDS > 12) associated with lower CVD incidence and mortality. One-unit increase in MDS > 12 associated with lower MACE after adjusting for all covariates (+1 category HR, 0.95; 95% CI, 0.91– 0.98, p = 0.002). No association between Western diet score (adjusted model +1 category HR, 0.99; 95% CI, 0.97– 1.01) and MACE. | Geography, education |
| Esposito et al., 2015 [43] | Systematic review and meta-analysis | Several | Men and women (age not specified) N total = 1266 | Overweight or obesity with T2DM | >0.5 | MedDiet defined according to PREDIMED [26] | T2DM | Higher MedDiet adherence lowered HbA1c. MedDiet reduced incidence of T2DM. | |
| Sleiman et al., [44] | Systematic review | Several | Men and women (age not specified) N total = 1266 | Obesity with T2DM and non-high-risk diabetes | 0.5–2 | Different depending on study | T2DM | Fasting glucose increased and HbA1c decreased in individuals following the MedDiet. No differences for MedDiet and control diet in non-diabetic patients. | |
| Maiorino et al., 2016 [46] | Parallel-group RCT (MEDITA) | Italy | Men and women (age not specified) N total = 215 | Recent diagnosis of T2DM | 8.1 | MedDiet | T2DM | MedDiet decreased CRP and increased adiponectin | |
| Babio et al., 2014 [23] | Multicenter, parallel-group RCT (PREDIMED) | Spain | 2437 men (ages 55–80) and 3364 women (ages 60–80) N total = 5801 | No CVD or T2DM but three risk factors for CVD: smoking, hypertension, high LDL-C, low HDL-C, BMI ≥ 25 kg/m2, family history of premature CVD | 4.8 | PREDIMED [26] | MetS | The risk of MetS was higher in MedDiet vs. control diet (control vs. olive oil: HR, 1.10; 95% CI, 0.94–1.30, p = 0.231; control vs. nuts: HR, 1.08; 95% CI 0.92–1.27, p = 0.3). Compared against control group, participants on either MedDiet were more likely to undergo reversion (control vs. olive oil: HR, 1.35; 95% CI: 1.15–1.58, p < 0.001; control vs. nuts: HR, 1.28; 95% CI, 1.08–1.51; p < 0.001). | |
| Steffen et al., 2014 [49] | Prospective study of MedDiet adherence and CVD (CARDIA) | USA | 2140 men and 2573 women (ages 18–30 at the beginning of the study) N total = 4713 | Absence of MetS | 25 | Modified by Trichopoulou [65] | MetS | Incidence of MetS inversely proportional to MedDiet adherence. Lower adherence → higher abdominal adiposity and % low HDL-C. The HRs and 95% CI from category 1 to category 5 were 1.0; 0.94 (0.76, 1.15); 0.84 (0.68, 1.04); 0.73 (0.58, 0.92); and 0.72 (0.54, 0.96), respectively (p = 0.005). | Age, education, physical activity, and race |
| Gomez-Huelgas 2015 [24] | Cross-sectional study to determine prevalence of MetS | Spain | 55.1% men and 44.9% women (average age 53.8) N total = 406 | MetS as defined by the International Society of Diabetes | 3 | MedDiet (14 points) according to PREDIMED | MetS | MedDiet → greater decrease in WC and blood pressure and higher HDL than the control group. | |
| Mirmiran et al., 2015 [52] | Prospective study to identify and prevent non-communicable diseases | Iran | 44.8% men and 55.2% women (average age 39.1) N total = 2241 | Healthy individuals without T2DM or MetS | 3 | MedDiet defined according to Trichopoulou [65]. MUFA/PUFA ratio; no olive oil intake | MetS | In the multivariable model, the adjusted odds ratio (OR) for developing MetS did not differ significantly between participants in the highest MDS tertile (OR, 0.88; 95% CI, 0.62–1.23) or Sofi-MDS (OR, 1.12; 95% CI, 0.77–1.62) and those in the lowest tertiles. | Age, sex, intake, physical activity, smoker, BMI |
| Kastorini et al., 2016 [35] | ATTICA | Greece | 50% men and 50% women (ages 18–89) N total = 2020 | Absence of CVD | 8.41 | MedDiet | MetS and CVD | 10% increase in MedDiet adherence associated with 15% less probability of developing CVD. Individuals with low MedDiet adherence were twice as likely to develop MetS. MetS associated with two-fold increased odds of CVD incidence (OR, 2.04; 95% CI, 1.31–3.17) in participants with low MedDiet adherence. | Age, sex, family history, smoker, history of MetS |
| CQs | Scientific Evidence | References |
|---|---|---|
| CQ 1: What effect does the MedDiet have on weight reduction in overweight and obese patients? | MedDiet adherence reduces obesity and abdominal adiposity. | Andreoli et al., 2008 [19]; Hadžiabdić et al., 2015 [20]; Ruiz-Canela et al., 2015 [21]; Álvarez Pérez et al., 2016 [22]; Babio et al., 2016 [23]; Gómez-Huelgas et al., 2015 [24]. |
| The MedDiet reduces CVD incidence and mortality. | US Department of Health and Human Services et al., 1980 [25]; Estruch et al., 2013 [26]; Nissensohn et al., 2016 [27]; Martínez-Gónzalez et al., 2011 [28]; Menotti et al., 2012 [29]; Gullar-Castillón et al., 2012 [30]; Gardener et al., 2011 [31]; Fung et al., 2009 [32]; Buckland et al., 2009 [33]; Trichopoulou et al., 2005 [34]; Kastorini et al., 2016 [35]; Turati et al., 2015 [36]; Stewart et al., 2016 [37]; Bonaccio et al., 2014 [38]; Stefler et al., 2015 [39]. | |
| CQ 2: What effect does the MedDiet have on the incidence and prevention of T2DM? | The MedDiet reduces the incidence of T2DM in healthy individuals. | Panagiotakos et al., 2005 [40]; Martínez-González et al., 2008 [41]; Salas-Salvado et al., 2011 [42]; Esposito et al., 2015 [43]; Sleiman et al., 2015 [44]; Abiemo et al., 2012 [45]. |
| The MedDiet reduces the symptoms of T2DM and modulates disease course. | Esposito et al., 2015 [43]; Sleiman et al., 2015 [44]; Maiorino et al., 2016 [46]. | |
| CQ 3: What effect does the MedDiet have on established MetS or on the risk of developing MetS? | High MedDiet adherence reduces some of the risk factors for MetS in patients with the disease. | Gómez-Huelgas et al., 2015 [24]; Salas-Salvado et al., 2013 [47]; Alvarez Leon et al., 2006 [48]. |
| The MedDiet reduces some of the risk factors for MetS in healthy individuals. | Alvarez Leon et al., 2006 [48]; Steffen et al., 2014 [49]; Rumawas et al., 2009 [50]; Kesse-Guyot et al., 2013 [51]; Mirmiran et al., 2015 [52]. | |
| CQ 4: What effect does the MedDiet have on the prevention of CVD and the modulation of disease course? | MedDiet adherence reduces the incidence of CVD in individuals with high cardiovascular risk. | Martínez-González et al., 2011 [28]; Gullar-Castillón et al., 2012 [30]; Kastorini et al., 2016 [35]; Stewart et al., 2016 [37]; Stefler et al., 2015 [39]; Panagiotakos et al., 2007 [53]; Eguaras et al., 2015 [54]; Casas et al., 2014 [55]; Estruch et al., 2013 [26]; Grosso et al., 2015 [56]. |
| MedDiet adherence reduces CVD mortality in individuals without CVD but with high cardiovascular risk. | Stewart et al., 2016 [37]; Bonaccio et al., 2014 [38]; Stefler et al., 2015 [39]. | |
| MedDiet adherence reduces CVD incidence and mortality in the general population. | Gardener et al., 2011 [31]; Fung et al., 2009 [32]; Buckland et al., 2009 [33]; Turati et al., 2015 [36]; Stewart et al., 2016 [37]; Menotti et al., 2012 [57]; Menotti, 2015 [58]; Knoops et al., 2004 [59]. | |
| CQ 5: What effect does the MedDiet have on weight gain and abdominal adiposity in healthy individuals and individuals without overweight? | MedDiet adherence decreases weight gain and/or BMI in the general population. | Romaguera et al., 2010 [60]; Schröder et al., 2004 [61]; Goulet et al., 2003 [62]; Paletas et al., 2010 [63]. |
| MedDiet adherence reduces WC in the general population. | Rumawas et al., 2009 [50]; Steffen et al., 2014 [49]; Romaguera et al., 2009 [64]. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franquesa, M.; Pujol-Busquets, G.; García-Fernández, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martínez, A.; Medina, F.X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients 2019, 11, 655. https://doi.org/10.3390/nu11030655
Franquesa M, Pujol-Busquets G, García-Fernández E, Rico L, Shamirian-Pulido L, Aguilar-Martínez A, Medina FX, Serra-Majem L, Bach-Faig A. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients. 2019; 11(3):655. https://doi.org/10.3390/nu11030655
Chicago/Turabian StyleFranquesa, Marcella, Georgina Pujol-Busquets, Elena García-Fernández, Laura Rico, Laia Shamirian-Pulido, Alicia Aguilar-Martínez, Francesc Xavier Medina, Lluís Serra-Majem, and Anna Bach-Faig. 2019. "Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions" Nutrients 11, no. 3: 655. https://doi.org/10.3390/nu11030655
APA StyleFranquesa, M., Pujol-Busquets, G., García-Fernández, E., Rico, L., Shamirian-Pulido, L., Aguilar-Martínez, A., Medina, F. X., Serra-Majem, L., & Bach-Faig, A. (2019). Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients, 11(3), 655. https://doi.org/10.3390/nu11030655