1. Introduction
Osteoarthritis (OA) is a disease of articular joints induced by increased inflammation. The prevalence of this disease increases with age, and the majority of individuals over the age of 65 are affected by OA [
1]. OA is a primary cause of pain contributing to the immobility of elderly people and is also a leading cause of disability globally [
2]. A previous meta-analysis demonstrated that the overall prevalence of radiographic knee OA is about 35% and that this prevalence increases with age in the USA. Among Korean people, 9.3% of male and 28.5% of female participants were diagnosed with symptomatic OA according to survey criteria in the Fifth Korean National Health and Nutrition Examination Survey (2010–2012) [
3]. In China, the prevalence of symptomatic knee OA is about 8.1% and is much higher in women (10.3%) than in men (5.7%) [
4].
Cartilage loss is considered to be the pathological aspect of OA. However, the disease extends throughout the whole joint, including the bone and soft tissues such as the synovium, menisci, and ligaments [
5]. The main symptoms of OA are a pain, stiffness, and loss of function. The pathophysiology remains unknown although, in general, it is initiated with injury and excessive usage, which induces inflammation causing the removal of articular cartilage. OA decreases quality of life due to pain and the limitation of physical activity [
6]. The risk factors for OA at a personal level include age, gender, weight, skeletal muscle mass, menopausal status, genetics, and diet. The risk factors for OA at the joint level, including injury, misalignment, and abnormal loading of the joints. Personal and joint level risk factors interact in a complex manner to aggregate OA symptoms [
6]. In particular, menopausal women are highly susceptible to OA incidence.
Estrogen deficiency exacerbates energy, glucose, lipid, and bone metabolism. This deficiency also elevates low-grade systematic inflammation with increased levels of pro-inflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor-α (TNF-α) [
7,
8]. Menopausal women are susceptible to OA, as this disease interacts with other metabolic diseases and their symptoms are exacerbated by one another.
These diseases have common pathogenic mechanisms, such as low-grade inflammation and oxidative stress. However, beyond this common etiology, metabolic diseases have direct systemic action on the joints. In addition to the impact of weight, obesity-associated inflammation is associated with OA severity and may modulate OA progression in mouse models. Increased insulin resistance may participate in joint catabolism. Finally, the gut microbiota is also modulated by insulin resistance and inflammation to influence metabolic syndrome and OA [
9,
10].
Medicines available to treat OA are currently limited in their effectiveness. Pharmaceuticals currently used to treat OA primarily focus on reducing pain and inflammation, such as non-steroidal anti-inflammatory drugs (NSAIDs) [
11]. However, NSAIDs are reported to have adverse effects. Glucosamine and chondroitin sulfate are mainly used as functional foods [
11]; however, their effectiveness remains controversial. The roots of
Allium fistulosum (Welsh onion) root (AFR) contain alliin, allicin and diallyl disulfide and have been reported to reduce body fat mass [
12]. Allicin has anti-inflammatory and immune-modulatory properties due to its augmentation of the extracellular signal-regulated kinases (ERK)1/2 signaling pathway [
13,
14]. Gluten may elevate inflammation levels if allergies are present. Rice does not contain gluten, and rice porridge is readily available to the elderly and easy to consume. Therefore, porridge containing AFR could be a beneficial meal for treating OA.
In this study, we hypothesize that the long-term administration of rice porridge containing
Allium fistulosum root water extract prevents or delays the progression of OA and menopausal symptoms in estrogen-deficient animals. This hypothesis was examined in ovariectomized (OVX) rats with OA induced via the intra-articular injection of monoiodoacetate (MIA). The action mechanism was also explored. MIA intra-articular injection into the knees is reported as a useful and relevant pre-clinical model of OA pain [
15].
2. Materials and Methods
2.1. Rice Porridge Containing Allium Fistulosum Root Water Extracts
AFR was extracted with water at 90 °C for 2 h, and the supernatant was filtered using a disposable CA syringe filter unit (pore size; 0.22 µm, diameter; 25 mm, Futecs Co., Ltd., Daejeon, Korea) after centrifuging for 10 min at 4000× g. The supernatant was freeze-dried and stored for further use in the animal study.
Rice porridge was prepared with rice and water by boiling for 2 h followed by freeze-drying. The test meal was prepared by mixing freeze-dried water extracts of AFR and freeze-dried rice porridge (1:13, w/w).
2.2. Analysis of Index Compounds in RAFR by LC-MS/MS Analysis
The analyses were performed using an Acquity UPLC system (Waters, Milford, MA, USA) equipped with an Acquity UPLC BEH C18 column (2.1 mm × 100 mm, 1.7 µm). The mobile phase included 0.1% formic acid aqueous solution (Solvent A) and 0.1% formic acid in acetonitrile (Solvent B). A gradient elution program was followed: 0–6 min, 100–70% solvent A; 6–9 min, 70–0% solvent A; 9–9.5 min, 0–0 % solvent A; 9.5–10 min, 100% solvent A. The flow rate was set at 0.6 mL/min and the column temperature was maintained at 30 °C. The auto-sampler was conditioned at 10 °C and the injection volume was 5 μL. Mass spectrometric analyses were undertaken using a Waters Xevo TQ triple-quadrupole mass spectrometer equipped with electrospray ionization (ESI) mode. The ESI source was operated by switching between positive and negative ion modes with multiple reaction monitoring modes. Quantification was performed using the positive mode of m/z 147.2→ 84 for lysine, m/z 177.9 → 88 for alliin, m/z 162 → 73 for s-allyl-L-cysteine, and m/z 291 → 145 for γ-glutamyl-(s)-allyl-cysteine and the negative mode of m/z 192.9 → 134 for ferulic acid and m/z 301.4 → 151.1 for quercetin. The detector was operated at a cone voltage of 25 V and a capillary voltage of 3.5 kV. The source temperature was set at 150 °C, the desolvation flow was set at 800 L/h, and the desolvation gas temperature was set at 400 °C.
2.3. Ovariectomy or Sham-Operation
Eight-week-old female Sprague–Dawley rats (weighing 233 ± 19 g) were housed individually in stainless steel cages in a controlled environment (23 °C with a 12 h light/dark cycle). Fifty Sprague–Dawley rats purchased from DBL (Yeumsung-Kun, Korea) were acclimated in our animal facility for one week. Forty rats underwent an OVX, and ten rats had sham operations under anesthesia via the subcutaneous injection of a mixture of ketamine and xylazine (100 and 10 mg/kg body weight, respectively). A mid-ventral incision was made, and each ovary was separated after the ligation of the most proximal portion of the oviduct [
16]. Both ovaries were removed with scissors. In the sham operations, rats underwent the same procedure as the OVX rats, but no ligation and removal of the ovaries were conducted. Thus, sham rats underwent the same surgical procedures as the OVX rats but retained their normal ovary functions. OVX rats were randomized into four groups, and the rats that underwent a sham operation were assigned to the Sham group. The surgery and care of the animals were conducted in accordance with the guidelines of the NIH Guide for the Care and Use of Laboratory Animals, and the International Association for the Study of Pain. The research procedures for the animal study were approved by the Animal Care and Use Committee of Hoseo University, Korea (HSIACUC-18-100).
2.4. Diet Preparation
The diets were high in fat to exacerbate the progression of OA and menopausal symptoms in comparison to a low-fat diet [
17,
18]. The diet consisted of 45% energy (En%) from carbohydrates, 15 En% from protein and 40 En% from fats. This high-fat diet is a semi-purified modified AIN-93 formulation for experimental animals [
19]. The major carbohydrate, protein, and fat sources are starch plus sugar, casein (milk protein), and lard (CJ Co., Seoul, Korea), respectively. The high-fat diet was supplemented with rice porridge containing AFR (0.23% rice + 0.018% AFR) for the OVX-OA-RAFR-L group, 0.69% rice + 0.053% AFR for the OVX-OA-RAFR-H group, and 0.053% cellulose for the control and Sham (normal-control) groups. For the control groups (OVX-OA, OVX, and Sham), the nutrient composition of rice was made equivalent to the OVX-OA-RAFR-H diet with rice protein, starch, and cellulose. Dried rice porridge and ARF powder were homogeneously mixed with a vitamin and mineral mixture and sugar. The dietary components and the mixture were sieved to remove lumps. This mixture was then mixed with the appropriate amounts of starch, casein, and lard and was sieved again. The resulting mixture was then stored at 4 °C, and the food supply was replaced every two days. The amount of the supplement administered (dosage) was calculated based on the food intake.
2.5. Experimental Design
The forty OVX rats were randomly assigned to the following four groups: (1) MIA injection into the knee joint and fed a high-fat diet containing 0.23% rice + 0.018% AFR diet (OVX-OA-RAFR-L) to consume about 250 mg/kg body weight. (2) MIA injection into the knee joint and fed a high-fat diet containing 0.69% rice + 0.053% AFR diet (OVX-OA-RAFR-H) to consume about 750 mg/kg bw. (3) MIA injection into the knee joint and fed a high-fat diet containing 0.053% cellulose (OA). (4) Saline injection into the knee joint and fed a high-fat diet containing 0.053% cellulose (OVX). Ten sham rats had the same diet as the control and a saline injection (Sham; normal-control). After the OVX or sham operation, the rats were given free access to water and their assigned diet. Each experimental group consisted of ten rats.
2.6. MIA-Induced OA Animal Models
After eight weeks of consuming their assigned diets, all OVX rats were anesthetized via the intramuscular injection of a ketamine and xylazine mixture (100 and 10 mg, respectively). The rats received a single intra-articular injection of MIA (4 mg/50 μL saline; Sigma Co., St. Louis, MO, USA) through the patellar ligament of the right knee using a 26-gauge needle [
18]. Sham rats received a single intra-articular injection of saline into the right knee as the normal-control (Sham group). The left knees of all rats were administered a saline injection. After the MIA or saline injection, assigned diets were provided for an additional three weeks. The behavior and edema of the knee joints were then carefully observed on days 3, 7, 14, and 21.
2.7. Tail Skin Temperature Measurements
The tail skin temperature was measured using an infrared thermometer (BIO-152-IRB, Bioseb, Chaville, France) designed for small rodents at weeks eight and eleven of the experimental periods during the sleep cycle. Three measurements were taken every 10 min, and the average for each animal was considered as a single data point.
2.8. Bone Mineral Density (BMD) Measurement
A dual-energy X-ray Absorptiometer (DEXA; Norland pDEXA Sabre; Norland Medical Systems Inc., Fort Atkinson, WI, USA) was calibrated with a phantom before use. After anesthetization, the rats were laid in a prone position with posterior legs with 90° flexion of the hip, knee, and ankle. Upon the completion of scanning, BMD was determined in the right femur and knee using the DEXA instrument equipped with the appropriate software for the assessment of bone density in small animals [
18]. Similarly, abdominal fat and lean body mass (LBM) was measured by DEXA.
2.9. Progression of OA and Pain-Related Behavior Evaluation
At 3, 7, 14, and 21 days after MIA injection, the diameters of the knees were measured every week using digital calipers (Mitotoyo, Kawasaki-shi, Japan). All rats were carefully evaluated for knee joint swelling and walking patterns in the cages, where they were able to move freely. Knee joint swelling severity and limping were classified as no change (0), mild (1), moderate (2), and severe (3) [
17]. All assessments were conducted by the same trained inspector who was blinded to their treatments throughout the study period.
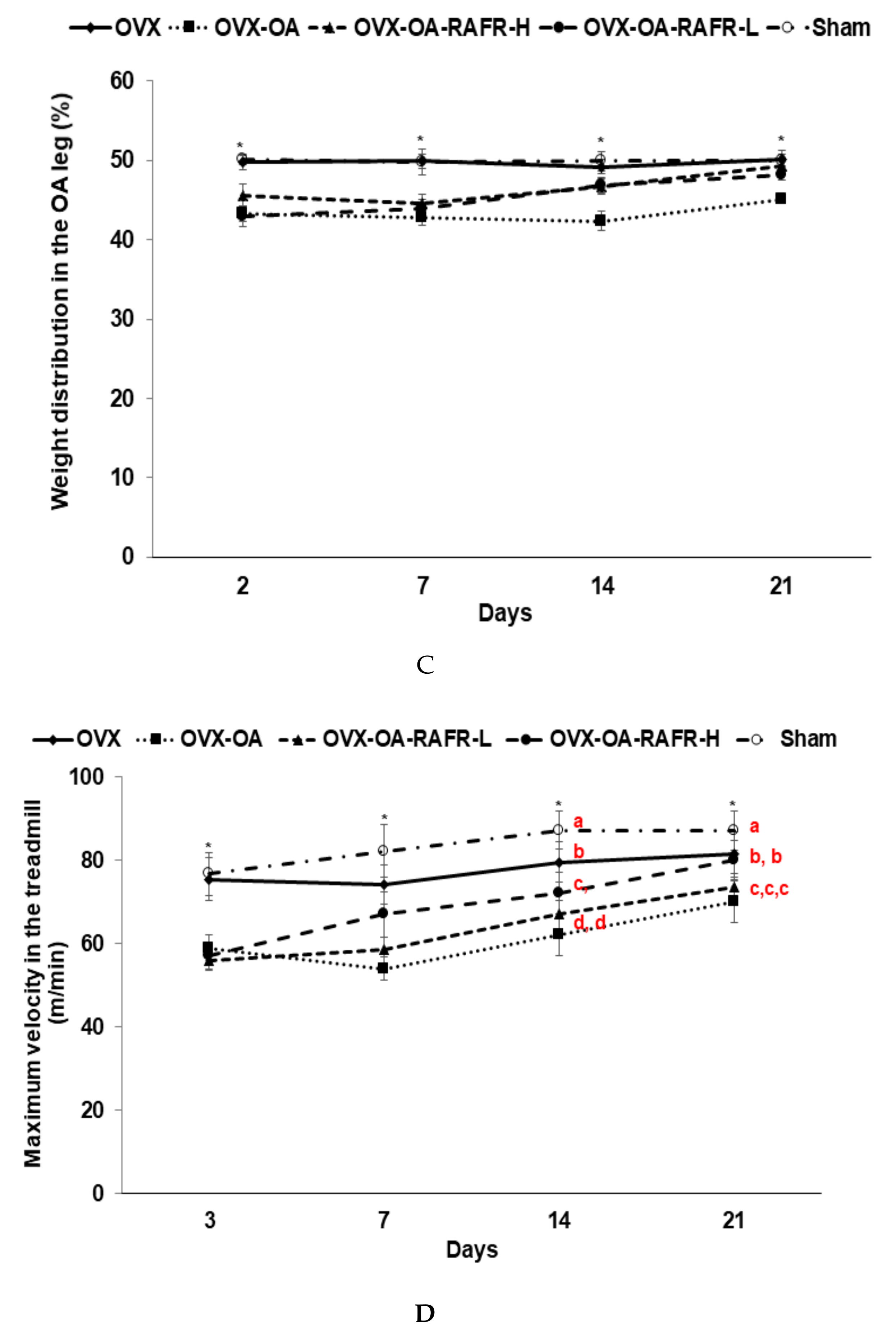
Pain-related behaviors were assessed using an incapacitance test via a hind paw limb weight-bearing apparatus (Linton Incapacitance Tester, Linton Instruments, Palgrave Diss, UK), the maximum running speed on a treadmill, and locomotive activity. These assessments occurred on the same days as OA progression was assessed. These tests have been utilized as indices of joint discomfort and may be useful for the discovery of novel pharmacological agents for treating human OA [
17]. Rats were acclimatized for 30 min before the incapacitance test. The hind paw weight distribution between the right (osteoarthritis) and left (control) limbs were assessed using an incapacitance tester. The assessments were performed five times for each rat, and the average of their values was calculated. The percent weight distribution of the right hind paw was calculated by dividing the right paw weight by the sum of the left and right paw weights [
18].
The maximum running speed of the rats was used as a parameter to assess the severity of their OA, as rats with OA cannot run as fast as rats without OA. The rats walked on a treadmill at 40 cm/s for 1 min, which then increased to 50 cm/sec for 1 min. Subsequently, the speed of the treadmill increased by 5 cm/s every min until the rats could not continue to run and instead slid to the back of the treadmill. The maximum running speed for each rat was determined by them running for 20 s at that speed. Each rat was subjected to the treadmill test for under 5 min.
The locomotive activity was measured using a Linton AM1053 Activity Monitor system to mount a three-dimensional array of infrared beams around clear Perspex cages with AmLogger software (Linton Instruments). The total locomotive activity was calculated through the sum of the rearing, mobility, and activities measured by the infrared beams. The activity was measured for 30 min during the dark phase of the light/dark cycle when the rats were most active after they were adapted to the clear Perspex cage for 30 min.
2.10. Glucose Homeostasis and Sample Collection at the end of the Experiment
An oral glucose tolerance test (OGTT) was performed via the overnight fasting of rats for 16 h, followed by administering 2 g glucose/kg bw orally at week eleven. Post-glucose loading, tail blood was collected to measure serum glucose levels using a Glucose Analyzer II (Beckman, Palo Alto, CA, USA) at 10 min intervals from 0 to 90 min and at 120 min. At 0, 20, 40, 90, and 120 min serum insulin concentrations were determined using an Ultrasensitive ELISA kit (Linco Research, Billerica, MA, USA). The average of the areas under the curves (AUC) of the serum glucose and insulin concentrations was calculated using the trapezoidal rule.
The rats were anesthetized with a ketamine/xylazine mixture, and the peri-uterine and retroperitoneal fat masses and uterine were weighed after excision. The uterus index (uterus weight divided by body weight) was calculated. Insulin resistance was determined using the homeostasis model assessment estimate of insulin resistance (HOMA-IR). HOMA-IR was calculated by fasting insulin (µIU/mL) × fasting glucose (mM)/22.5. The serum was prepared from blood collected from the inferior vena cava by centrifuging at 3000 rpm for 20 min. Serum and tissues were then stored at −70 °C for future use. Serum IL-6 and TNF-α concentrations were determined using a commercially available ELISA (Rat IL-6 and Rat TNF-α Quantikine (R&D Systems, Minneapolis, MN, USA). Serum 17β-estradiol levels and serum alkaline phosphatase (ALP) activities were measured by ELISA kits (Enzo Life Sciences, Farmingdale, NY, USA) and colorimetry kit (Asan Pharmaceutical, Seoul, Korea).
2.11. Isolation of Total RNA from Articular Cartilage and Real-Time PCR
Articular cartilage samples from five rats of each group were collected at the end of the experiment. Each cartilage was individually powdered with a cold steel mortar and pestle and then mixed with a monophasic solution of phenol and guanidine isothiocyanate (TRIzol reagent, Life Technologies, Rockville, MD, USA) for total RNA extraction. The RNA concentration was determined using a Lambda 850 spectrophotometer (Perkin Elmer, Waltham, MA, USA) and cDNA was synthesized from 1 μg total RNA extracted from individual rats using a Superscript III reverse transcriptase kit (Life Technology, Carlsbad, CA, USA). Five different cDNA were formed from each group, and each cDNA was used for real-time PCR. Equal amounts of cDNA and primers for the gene of interest were mixed with SYBR Green mix (Bio-Rad, Richmond, CA, USA) in duplicate and amplified using a real-time PCR instrument (Bio-Rad). Thermal cycling conditions were 55 °C for 2 min and 95 °C for 10 min, followed by 40 cycles of 94 °C for 20 s, 65 °C for 30 s, and 72 °C for 20 seconds. Primers were used to detect the genes related to the inflammation and degradation of articular cartilage, such as TNF-α, IL-1β, IL-6, matrix metalloproteinase (MMP)-3, and MMP-13 genes. The primers were described previously [
18]. The cycle of threshold (CT) for each sample was determined via real-time PCR. The gene expression levels in the cartilage of each rat were quantitated using the CT method (ΔΔCT method). ΔCT was calculated via subtracting CT (target gene) to CT (endogenous reference gene, β-actin). The relative fold-change in gene expression was calculated by the equation ΔΔCt = ΔCt
treatment − ΔCt
control. The results are presented as 2
−ΔΔCT [
16].
2.12. Histopathological Analysis of Rat Knees
After scarifying rats, the right knee was histologically examined for chronic morphological changes, including narrowing knee articular bones, the loss of joint regions, cartilage erosion, and osteophyte formation. For the histological analysis, knee joints were excised and fixed in phosphate-buffered formalin. The joints were subsequently decalcified in 10% nitric acid for 72 h and embedded in paraffin. Five-micrometer sections were stained with hematoxylin and eosin (H-E) and safranin-O fast green to evaluate morphological changes. The histopathological changes in each rat were quantitatively expressed according to the depth and extent of the damage by the following scoring system [
17,
18]: The depth was scored on a scale of 0–5 where 0 = normal; 1 = minimal, affecting the superficial zone only; 2 = mild invasion into the upper middle zone only; 3 = moderate invasion well into the middle zone; 4 = marked invasion into the deep zone but not to the tidemark; and 5 = severe full-thickness degradation to the tidemark. The extent of the tibial plateau involvement and proteoglycan loss were scored as 1 (minimal), 2 (mild), 3 (moderate), and 4 (severe).
2.13. Statistical Analysis
Statistical analysis was performed using SAS software version 7 (SAS Institute, Cary, NC, USA), and all results are expressed as a mean±SD. The variables measured at different time points were analyzed via two-way repeated measures ANOVA with the time and group as independent variables and an interaction term between the time and group. A one-way ANOVA was used to determine the metabolic effects of the OVX (OVX rats with a saline injection), OA (OVA rats with an MIA injection), OVX-OA-RAFR-L, OVX-OA-RAFR-H, and Sham (Sham rats with a saline injection; normal-control). Significant differences in the effects between groups were identified through Tukey’s test at p < 0.05.
4. Discussion
Estrogen deficiency during menopause exacerbates bone, energy, glucose, and lipid metabolism by increasing insulin resistance. These effects are accompanied by elevated oxidative stress and inflammation. Women experiencing menopause have a high susceptibility to OA. Moreover, hyperglycemia exacerbates the symptoms of OA. In the present study, we examined whether RAFR ameliorated bone and glucose metabolism involved in OA progression as well as menopausal symptoms in OVX rats. RAFR did not decrease tail skin temperature, uterine weight, or serum 17β-estradiol concentrations compared to OVX-control rats. However, RAFR ameliorated BMD and LBM, but not to the same extent as the Sham.
Furthermore, OVX-OA-RAFR improved glucose and insulin tolerance to a similar degree as the Sham. This improvement is associated with the exacerbation of the activation of MMPs to reduce collagen and stimulate proinflammatory cytokines due to an estrogen deficiency. This study shows that OVX-OA-RAFR reduced the disturbance of glucose and bone metabolism but did not significantly decrease tail skin temperatures in OVX-OA rats. MIA is known to disrupt glycolysis in the knee joints resulting in the eventual death of chondrocytes by inhibiting glyceraldehyde-3-phosphate dehydrogenase activity with increased inflammation [
20]. RAFR dose-dependently ameliorated OA symptoms induced by MIA in the knee joint by decreasing the degradation of articular cartilage and the mRNA expression of proinflammatory cytokines. Therefore, it may be beneficial for elderly women who are at risk of OA to consume RAFR daily.
AFR, a part of RAFR, contains Allium sulfides such as alliin and allicin [
21]. AFR inhibits cholesterol synthesis, consists of arterial smooth muscle cells, and exhibits platelet aggregation as well as anti-oxidant, anti-inflammatory, and vasodilatory activities [
21]. Previous studies have reported that AFR reduces body fat and liver fat in non-alcoholic fatty livers [
22,
23]. However, no previous studies have reported the impact of AFR on OA and menopausal symptoms. Allium sulfide compounds have a great potential to contribute towards treatments for OA. Allium sulfide has been demonstrated to repress the expression of matrix-degrading proteases in chondrocyte-like cells, meaning that it may have the potential to reduce OA incidence [
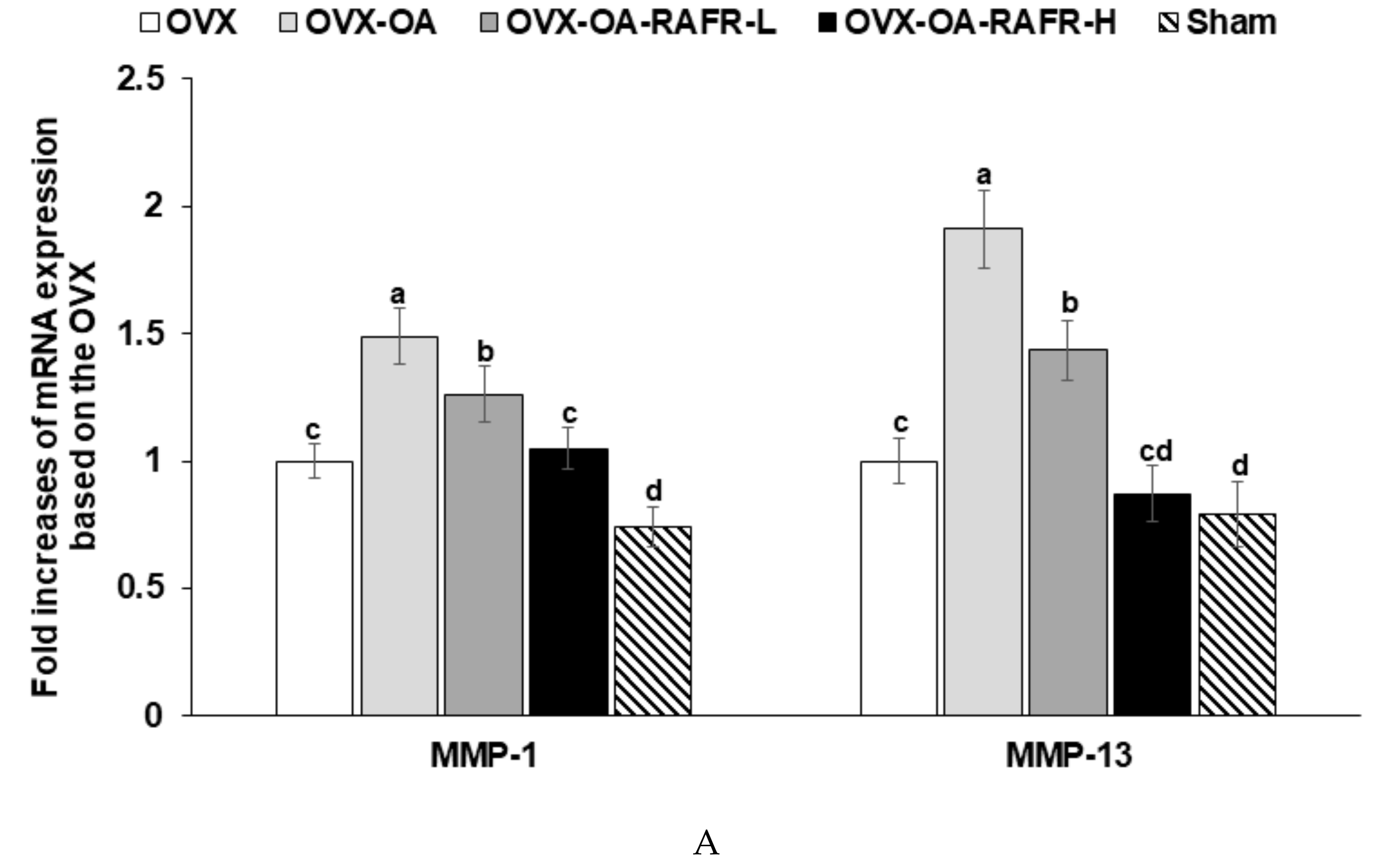
24]. The present study found that OVX-OA-RAFR decreases the mRNA expression of MMP-1 and MMP-13, which are involved with the matrix-degrading proteases, and TNF-α and IL-13 in the articular matrix compared to the OVX-OA. These effects may be associated with allium sulfide in RAFR.
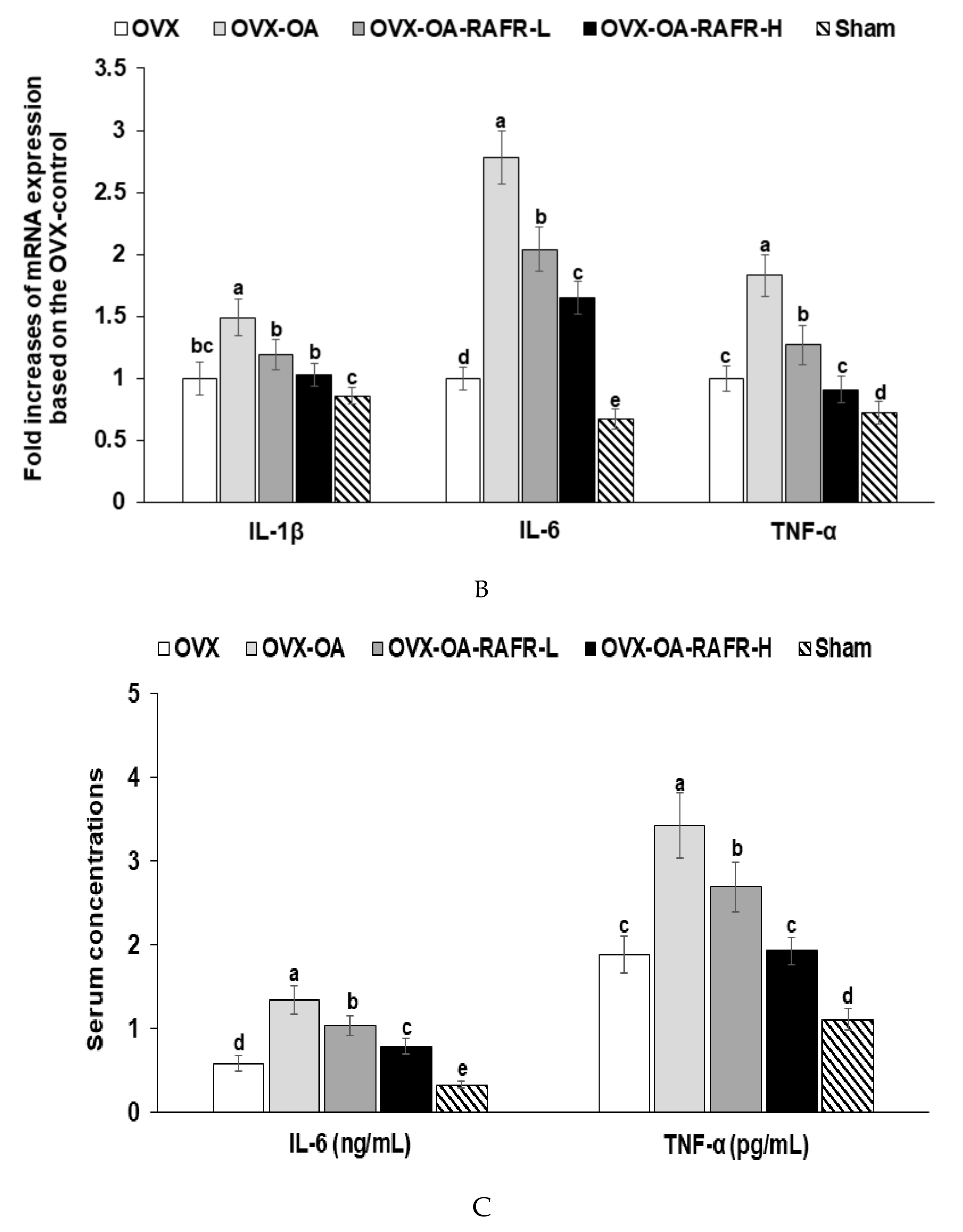
A decline in ovarian function is associated with a spontaneous increase in proinflammatory cytokines along with oxidative stress. This outcome is associated with the exacerbation of osteoarthritis symptoms in menopausal women. In the estrogen-deficient state, nuclear factor kappa B is activated, which increases the production of IL-1β, IL-6, and TNF-α. In OVX rats, their concentrations and mRNA expression are elevated, which suggests the exacerbation of OA due to estrogen deficiency [
25]. The present study showed consistent results; OVX rats decreased BMD and LBM with increasing serum TNF-α concentrations. The serum TNF-α concentrations were elevated in OVX-OA rats compared to OVX rats.
Moreover, the mRNA expressions of IL-1β, IL-6, and TNF-α in the articular matrix in the knee were elevated in OVX-OA rats compared to OVX rats. No studies have been conducted on the effects of AFR or RAFR on bone metabolism. However, previous studies have found that the garlic extract maintains bone health in OVX rats. The reduction of estrogen production increases bone turnover by increasing the production of proinflammatory cytokines and oxidative stress to induce osteoporosis [
25]. Garlic extracts protect against BMD loss [
25]. The effect of RAFR on BMD may be similar to that of garlic, as RAFR contains allium sulfide compounds which may be effective components. This present study showed that RAFR protected against a decrease of BMD and LBM by decreasing the mRNA expression of IL-1β, IL-6, and TNF-α in the articular matrix of the knee joint.
OA changes the morphology of the knee joints, and these changes can be scored to assess OA severity. The induction of OA increases chondrocyte hypertrophy and decreases the articular cartilage matrix with the loss of proteoglycans and surface fibrillation [
26]. In addition, the early stages of OA increase bone remodeling and bone loss, and the late-stage slows down remodeling and subchondral densification. Therefore, OA bone atrophy arises from an increase in bone resorption or a decrease in bone formation during OA [
27]. In this present study, MIA reduces the articular cartilage matrix via the upregulation of matrix-degrading enzymes such as MMP-1 and MMP-13 and bone loss. Bone loss was indicated via a higher serum ALP concentration and lower BMD in the legs of the OA-control group compared to that in the OVX-control group. OVX-OA-RAFR reduced proteoglycan loss in the articular cartilage matrix as well as bone atrophy and BMD loss compared to OVX-OA. RAFR partly protected against the loss of the articular cartilage matrix and bone remodeling in MIA-induced OA rats.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}