Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Anthropometry
2.4. Body Composition and Resting Energy Expenditure
2.5. Analytical Procedures
2.6. Experimental Protocol
2.7. Statistics
3. Results
3.1. Anthropometry
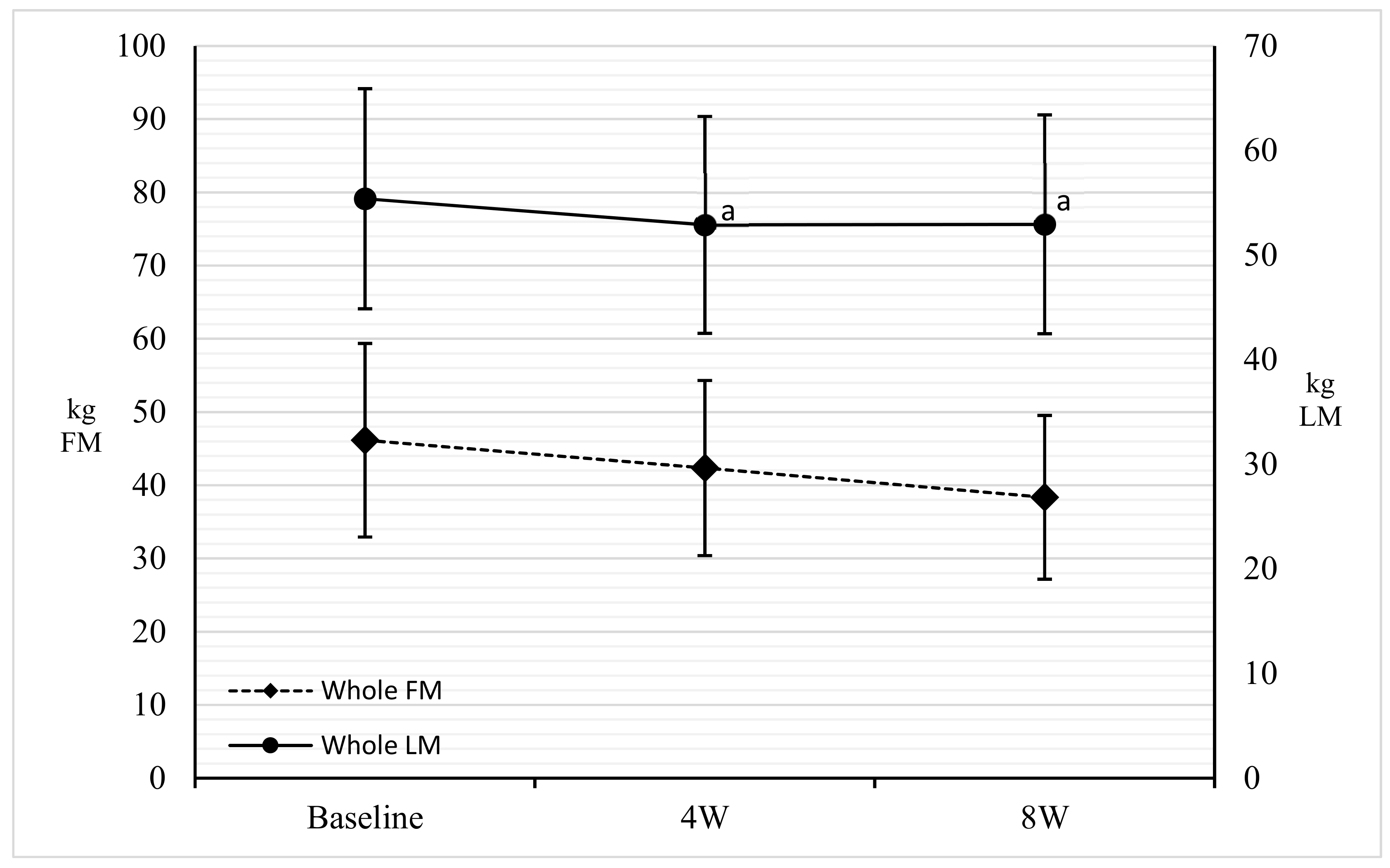
3.2. DXA
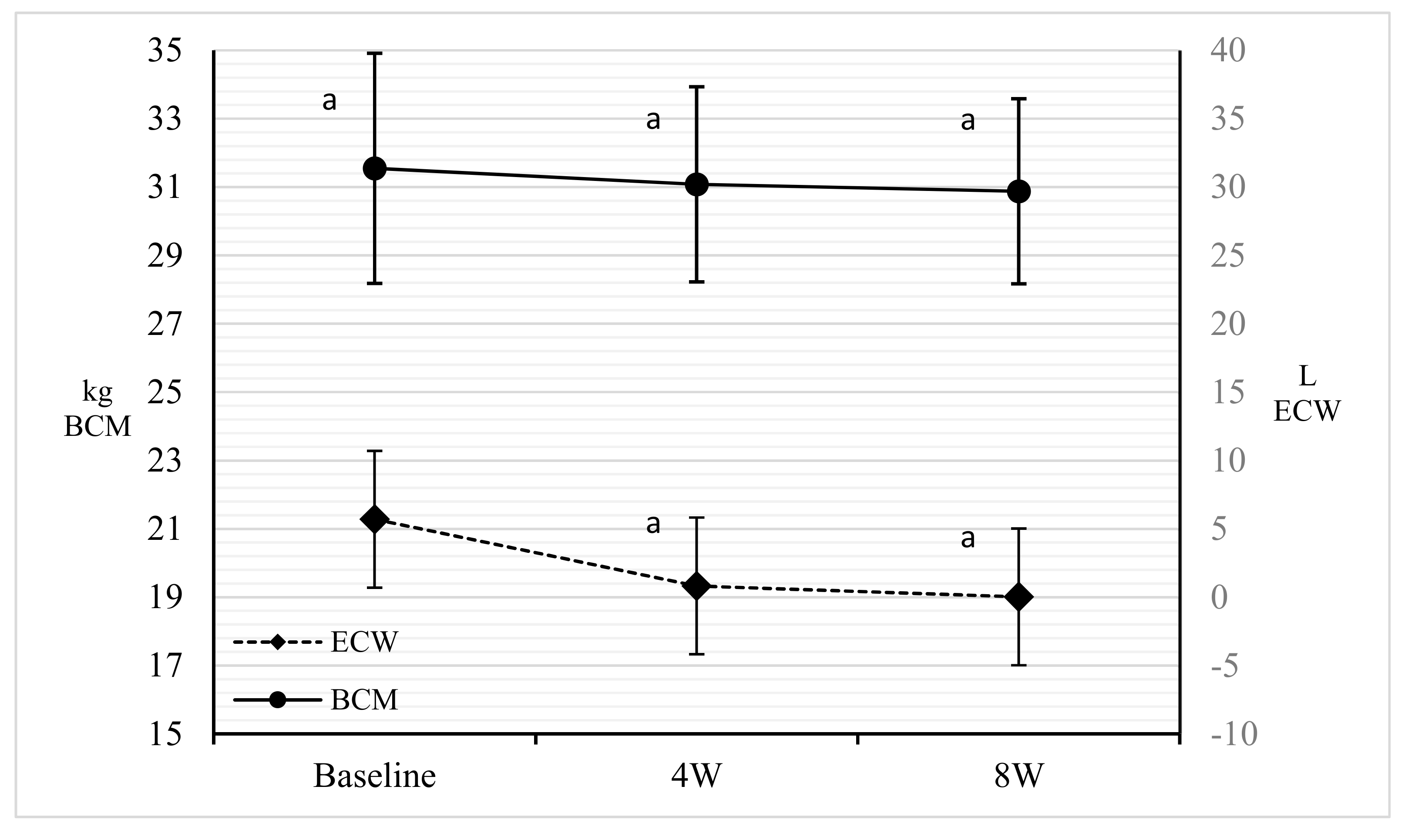
3.3. BIA
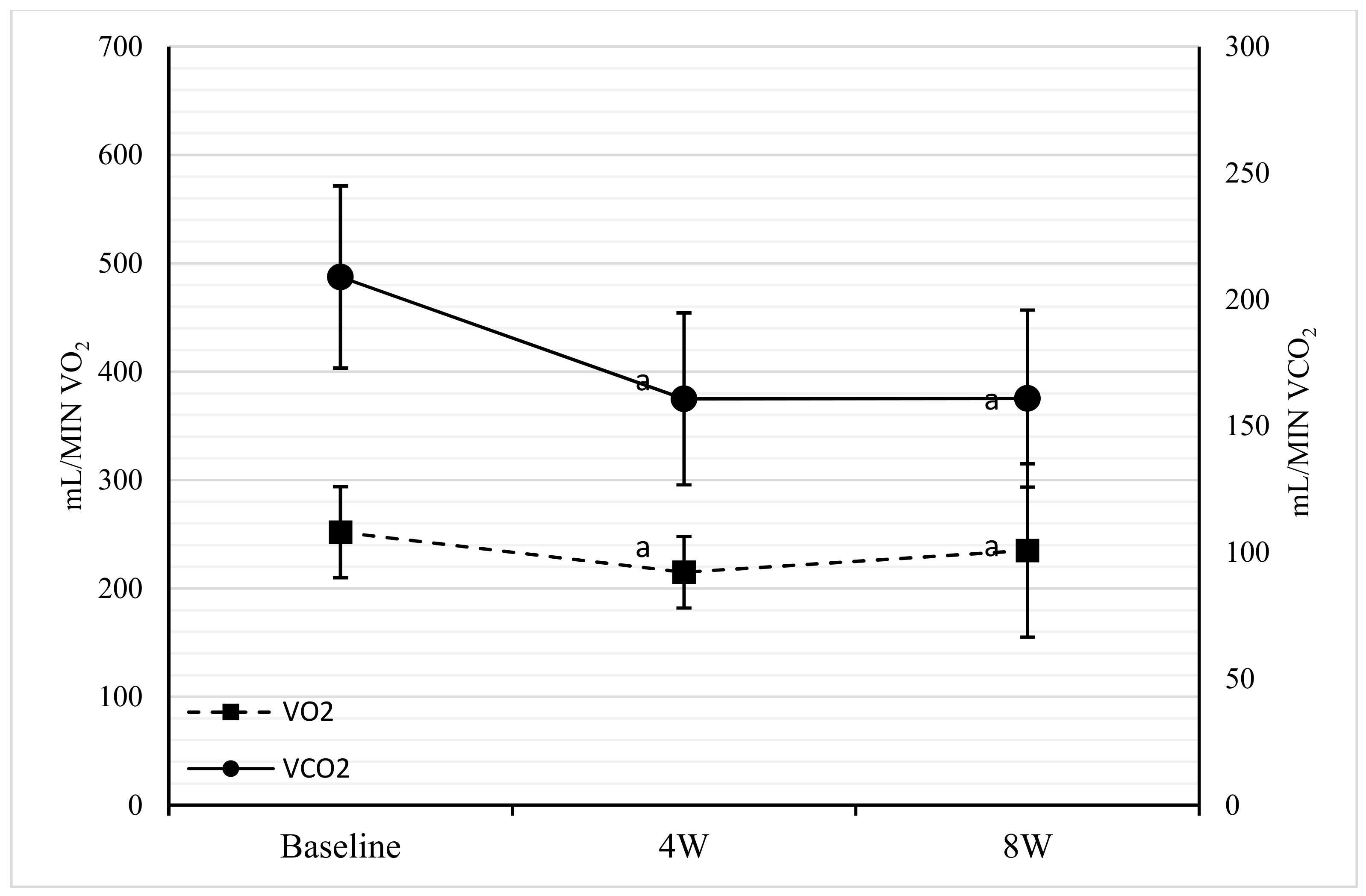
3.4. Indirect Calorimetry
3.5. Blood Tests
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition-barriers to and opportunities for healthier eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- What Is Diabetes. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 10 April 2019).
- Thomas, C.E.; Mauer, E.A.; Shukla, A.P.; Rathi, S.; Aronne, L.J. Low adoption of weight loss medications: A comparison of prescribing patterns of antiobesity pharmacotherapies and SGLT2s. Obesity (Silver Spring) 2016, 24, 1955–1961. [Google Scholar] [CrossRef] [PubMed]
- Avolio, E.; Gualtieri, P.; Romano, L.; Pecorella, C.; Ferraro, S.; Di Renzo, L.; De Lorenzo, A. Obesity and body composition in man and woman: Associated diseases and new role of gut microbiota. Curr. Med. Chem. 2019, 25. [Google Scholar] [CrossRef] [PubMed]
- Lehtisalo, J.; Lindström, J.; Ngandu, T.; Kivipelto, M.; Ahtiluoto, S.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Eriksson, J.G.; Uusitupa, M.; Tuomilehto, J.; et al. Diabetes, glycaemia, and cognition-a secondary analysis of the Finnish Diabetes Prevention Study. Diabetes Metab. Res. Rev. 2016, 32, 102–110. [Google Scholar] [CrossRef]
- Taylor, R.; Al-Mrabeh, A.; Sattar, N. Understanding the mechanisms of reversal of type 2 diabetes. Lancet Diabetes Endocrinol. 2019, 13, S2213–S8587. [Google Scholar] [CrossRef]
- Lim, E.L.; Hollingsworth, K.G.; Aribisala, B.S.; Chen, M.J.; Mathers, J.C.; Taylor, R. Reversal of type 2 diabetes: Normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011, 54, 2506–2514. [Google Scholar] [CrossRef]
- Steven, S.; Hollingsworth, K.G.; Al-Mrabeh, A.; Avery, L.; Aribisala, B.; Caslake, M.; Taylor, R. Very Low-Calorie Diet and 6 Months of Weight Stability in Type 2 Diabetes: Pathophysiological Changes in Responders and Nonresponders. Diabetes Care 2016, 39, 808–815. [Google Scholar] [CrossRef] [Green Version]
- McMurray, R.G.; Soares, J.; Caspersen, C.J.; McCurdy, T. Examining variations of resting metabolic rate of adults: A public health perspective. Med. Sci. Sports Exerc. 2014, 46, 1352–1318. [Google Scholar] [CrossRef]
- Müller, M.J.; Bosy-Westphal, A.; Kutzner, D.; Heller, M. Metabolically active components of fat-free mass and resting energy expenditure in humans: Recent lessons from imaging technologies. Obes. Rev. 2002, 3, 113–122. [Google Scholar] [CrossRef]
- Grattan, B.J., Jr.; Connolly-Schoonen, J. Addressing weight loss recidivism: A clinical focus on metabolic rate and the psychological aspects of obesity. ISRN Obes. 2012, 2012, 567530. [Google Scholar] [CrossRef] [PubMed]
- Dulloo, A.G.; Jacquet, J.; Miles-Chan, J.L.; Schutz, Y. Passive and active roles of fat-free mass in the control of energy intake and body composition regulation. Eur. J. Clin. Nutr. 2017, 71, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Dulloo, A.G.; Jacquet, J.; Girardier, L. Poststarvation hyperphagia and body fat overshooting in humans: A role for feedback signals from lean and fat tissues. Am. J. Clin. Nutr. 1997, 65, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Talluri, J.; Peroni, G.; Donelli, C.; Guerriero, F.; Ferrini, K.; Riggi, E.; Sauta, E.; Perna, S.; Guido, D. Beyond Body Mass Index. Is the Body Cell Mass Index (BCMI) a useful prognostic factor to describe nutritional, inflammation and muscle mass status in hospitalized elderly? Body Cell Mass Index links in elderly. Clin. Nutr. 2018, 37, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur. J. Clin. Nutr. 2013, 67, 759. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2003, 102, 1621–1630, Erratum in 2002, 103, 563. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B.; et al. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef]
- Campbell, W.W.; Trappe, T.A.; Wolfe, R.R.; Evans, W.J. The recommended dietary allowance for protein may not be adequate for older people to maintain skeletal muscle. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M373–M380. [Google Scholar] [CrossRef]
- Geisler, C.; Prado, C.M.; Müller, M.J. Inadequacy of Body Weight-Based Recommendations for Individual Protein Intake-Lessons from Body Composition Analysis. Nutrients 2016, 9, 23. [Google Scholar] [CrossRef]
- Colica, C.; Avolio, E.; Bollero, P.; Costa de Miranda, R.; Ferraro, S.; Sinibaldi Salimei, P.; De Lorenzo, A.; Di Renzo, L. Evidences of a New Psychobiotic Formulation on Body Composition and Anxiety. Mediat. Inflamm. 2017, 2017, 5650627. [Google Scholar] [CrossRef]
- Colica, C.; Merra, G.; Gasbarrini, A.; De Lorenzo, A.; Cioccoloni, G.; Gualtieri, P.; Perrone, M.A.; Bernardini, S.; Bernardo, V.; Di Renzo, L.; et al. Efficacy and safety of very-low-calorie ketogenic diet: A double blind randomized crossover study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2274–2289. [Google Scholar] [PubMed]
- Merra, G.; Gratteri, S.; De Lorenzo, A.; Barrucco, S.; Perrone, M.A.; Avolio, E.; Bernardini, S.; Marchetti, M.; Di Renzo, L. Effects of very-low-calorie diet on body composition, metabolic state, and genes expression: A randomized double-blind placebo-controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 329–345. [Google Scholar] [PubMed]
- Merra, G.; Miranda, R.; Barrucco, S.; Gualtieri, P.; Mazza, M.; Moriconi, E.; Marchetti, M.; Chang, T.F.; De Lorenzo, A.; Di Renzo, L. Very-low-calorie ketogenic diet with aminoacid supplement versus very low restricted-calorie diet for preserving muscle mass during weight loss: A pilot double-blind study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2613–2621. [Google Scholar] [PubMed]
- Steven, S.; Taylor, R. Restoring normoglycaemia by use of a very low calorie diet in long- and short-duration Type 2 diabetes. Diabet. Med. 2015, 32, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Siclari, M.; Gratteri, S.; Romano, L.; Gualtieri, P.; Marchetti, M.; Merra, G.; Colica, C. Developing and cross-validation of new equations to estimate fat mass in Italian population. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 2513–2524. [Google Scholar] [PubMed]
- Costa de Miranda, R.; Di Lorenzo, N.; Andreoli, A.; Romano, L.; De Santis, G.L.; Gualtieri, P.; De Lorenzo, A. Body composition and bone mineral density in Huntington’s disease. Nutrition 2019, 59, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Colica, C.; Di Renzo, L.; Trombetta, D.; Smeriglio, A.; Bernardini, S.; Cioccoloni, G.; Costa de Miranda, R.; Gualtieri, P.; Sinibaldi Salimei, P.; De Lorenzo, A. Antioxidant Effects of a Hydroxytyrosol-Based Pharmaceutical Formulation on Body Composition, Metabolic State, and Gene Expression: A Randomized Double-Blinded, Placebo-Controlled Crossover Trial. Oxid. Med. Cell. Longev. 2017, 2017, 2473495. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Di Renzo, L.; Morini, P.; de Miranda, R.C.; Romano, L.; Colica, C. New equations to estimate resting energy expenditure in obese adults from body composition. Acta Diabetol. 2018, 55, 59–66. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol. 2019, 7, 344–355. [Google Scholar] [CrossRef] [Green Version]
- Westerterp-Plantenga, M.S.; Nieuwenhuizen, A.; Tome, D.; Soenen, S.; Westerterp, K.R. Dietary protein, weight loss, and weight maintenance. Annu. Rev. Nutr. 2009, 29, 21–41. [Google Scholar] [CrossRef]
- Veldhorst, M.; Smeets, A.; Soenen, S.; Hochstenbach-Waelen, A.; Hursel, R.; Diepvens, K.; Lejeune, M.; Luscombe-Marsh, N.; Westerterp-Plantenga, M. Protein-induced satiety: Effects and mechanisms of different proteins. Physiol. Behav. 2008, 94, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Cenci, L.; Fancelli, M.; Parmagnani, A.; Fratter, A.; Cucchi, A.; Bianco, A. Ketogenic diet and phytoextracts. Comparison of the efficacy of mediterranean, zone and tisanoreica diet on some health risk factors. Agro Food Ind. Hi-Tech 2010, 21, 24–29. [Google Scholar]
- Acconcia, M.C.; Caretta, Q.; Romeo, F.; Borzi, M.; Perrone, M.A.; Sergi, D.; Chiarotti, F.; Calabrese, C.M.; Sili Scavalli, A.; Gaudio, C. Meta-analyses on intra-aortic balloon pump in cardiogenic shock complicating acute myocardial infarction may provide biased results. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2405–2414. [Google Scholar] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, N.; Runyan, J.W.; Clark, G.; Marvin, O. Carbohydrate Intake and Respiratory Quotient. Nutr. Rev. 1964, 22, 105–107. [Google Scholar]
- Steven, S.; Carey, P.E.; Small, P.K.; Taylor, R. Reversal of Type 2 diabetes after bariatric surgery is determined by the degree of achieved weight loss in both short- and long-duration diabetes. Diabet. Med. 2015, 32, 47–53. [Google Scholar] [CrossRef]
- Di Renzo, L.; Carbonelli, M.G.; Bianchi, A.; Iacopino, L.; Fiorito, R.; Di Daniele, N.; De Lorenzo, A. Body composition changes after laparoscopic adjustable gastric banding: What is the role of -174G>C interleukin-6 promoter gene polymorphism in the therapeutic strategy? Int. J. Obes. (Lond.) 2012, 36, 369–378. [Google Scholar] [CrossRef]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Ordoñez-Mayan, L.; Carreira, J.; Galban, C.; Martinez-Olmos, M.A.; Crujeiras, A.B.; Sajoux, I.; Casanueva, F.F. Body Composition Changes After Very-Low-Calorie Ketogenic Diet in Obesity Evaluated by 3 Standardized Methods. J. Clin. Endocrinol. Metab. 2017, 102, 488–498. [Google Scholar] [CrossRef]
- Overweight and Obesity. Available online: https://www.who.int/gho/ncd/risk_factors/overweight_obesity/obesity_adults/en/ (accessed on 10 April 2019).
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Gualtieri, P.; Salimei, C.; Carrano, E.; Rampello, T.; de Miranda, R.C. Triponderal mass index rather than body mass index: An indicator of high adiposity in Italian children and adolescents. Nutrition 2019, 60, 41–47. [Google Scholar] [CrossRef]
- Kolanowski, J.; Bodson, A.; Desmecht, P.; Bemelmans, S.; Stein, F.; Crabbe, J. On the relationship between ketonuria and natriuresis during fasting and upon refeeding in obese patients. Eur. J. Clin. Investig. 1978, 8, 277–282. [Google Scholar] [CrossRef]
- Frigolet, M.E.; Ramos Barragán, V.E.; Tamez González, M. Low-carbohydrate diets: A matter of love or hate. Ann. Nutr. Metab. 2011, 58, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Chen, K.Y.; Guo, J.; Lam, Y.Y.; Leibel, R.L.; Mayer, L.E.; Reitman, M.L.; Rosenbaum, M.; Smith, S.R.; Walsh, B.T.; et al. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am. J. Clin. Nutr. 2016, 104, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, F.X.; Becker, D.M.; Bouchard, C.; Carleton, R.A.; Colditz, G.A.; Dietz, W.H.; Foreyt, J.P.; Garrison, R.J.; Grundy, S.M.; Hansen, B.C.; et al. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: Executive summary. Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Am. J. Clin. Nutr. 1998, 68, 899–917. [Google Scholar]
- National Institute for Health and Care Excellence. Obesity: Identification, assessment and management of overweight and obesity in children, young people and adults. In NICE Clinical Guidelines; Puo, C., Ed.; 2014. Available online: https://www.nice.org.uk/guidance/cg189 (accessed on 10 April 2016).
- Goodpaster, B.H.; Sparks, L.M. Metabolic Flexibility in Health and Disease. Cell Metab. 2017, 25, 1027–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leibel, R.L.; Rosenbaum, M.; Hirsch, J. Changes in energy expenditure resulting from altered body weight. N. Engl. J. Med. 1995, 332, 621–628, Erratum in 1995, 333, 999. [Google Scholar] [CrossRef]
- Carrasco, F.; Papapietro, K.; Csendes, A.; Salazar, G.; Echenique, C.; Lisboa, C.; Díaz, E.; Rojas, J. Changes in resting energy expenditure and body composition after weight loss following Roux-en-Y gastric bypass. Obes. Surg. 2007, 17, 608–616, Erratum in 2007, 17, 996. [Google Scholar] [CrossRef]
- Lim, E.L.; Hollingsworth, K.G.; Smith, F.E.; Thelwall, P.E.; Taylor, R. Inhibition of lipolysis in Type 2 diabetes normalizes glucose disposal without change in muscle glycogen synthesis rates. Clin. Sci. (Lond.) 2011, 121, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef]
- Giordani, I.; Malandrucco, I.; Donno, S.; Picconi, F.; Di Giacinto, P.; Di Flaviani, A.; Chioma, L.; Frontoni, S. Acute caloric restriction improves glomerular filtration rate in patients with morbid obesity and type 2 diabetes. Diabetes Metab. 2014, 40, 158–160. [Google Scholar] [CrossRef]
- Garlick, P.J. The nature of human hazards associated with excessive intake of amino acids. J. Nutr. 2004, 134, 1633S–1639S. [Google Scholar] [CrossRef] [PubMed]
- Imamura, W.; Yoshimura, R.; Takai, M.; Yamamura, J.; Kanamoto, R.; Kato, H. Adverse effects of excessive leucine intake depend on dietary protein intake: A transcriptomic analysis to identify useful biomarkers. J. Nutr. Sci. Vitaminol. 2013, 59, 45–55. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | 20 |
| Men | 10 |
| Women | 10 |
| Age (years) | 56.13 ± 9.27 |
| Diabetes Duration (years) | 5.85 ± 1.73 |
| Diabetes Treatment | |
| Diet (n) | 8 |
| Metformin (n) | 15 |
| Sulphonylurea (n) | 5 |
| Insulin (n) | 10 |
| Anti-Hypertensives (n) | 15 |
| Statins (n) | 18 |
| Parameters | Basal | Four Weeks | Eight Weeks | Δ Base–Four Weeks | Δ Four Weeks–Eight Weeks | Δ Base–Eight Weeks | p Base–Four Weeks | p Four Weeks–Eight Weeks | p Base–Eight Weeks |
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||||||
| ANTHROPOMETRY | |||||||||
| Weight (kg) | 104.43 ± 18.85 | 92.85 ± 27.61 | 89.07 ± 26.17 | −11.07 | −4.04 | −15.77 | 0.000 * | 0.000 * | 0.000 * |
| BMI (kg/m2) | 37.09 ± 6.83 | 34.75 ± 6.50 | 33.25 ± 5.99 | −6.42 | −4.12 | −10.27 | 0.000 * | 0.000 * | 0.000 * |
| Neck circumference (cm) | 43.08 ± 3.36 | 41.59 ± 3.22 | 40.92 ± 3.0’ | −3.99 | −1.35 | −4.92 | 0.000 * | 0.070 | 0.000 * |
| Waist circumference (cm) | 113.56± 12.71 | 109.33 ± 9.86 | 101.65 ± 11.23 | −4.87 | −5.98 | −10.37 | 0.000 * | 0.000 * | 0.000 * |
| Abdomen circumference (cm) | 123.79 ± 12.96 | 119.21 ± 13.14 | 110.99 ± 12.52 | −4.82 | −6.12 | −10.31 | 0.000 * | 0.000 * | 0.000 * |
| Hip circumference (cm) | 118.65 ± 14.5 | 114.09 ± 12.58 | 108.32 ± 11.57 | −3.38 | −5.15 | −8.38 | 0.000 * | 0.000 * | 0.000 * |
| Handgrip (dominant hand) (kg) | 26.81 ± 8.03 | 27.34 ± 7.73 | 29.00 ± 7.32 | 1.60 | 2.23 | 3.39 | 0.640 | 0.070 | 0.050 |
| DXA | |||||||||
| Arm FM (kg) | 4.74 ± 1.30 | 4.36 ± 1.14 | 4.16 ± 1.17 | −7.58 | −7.39 | −10.26 | 0.070 | 0.230 | 0.010 * |
| Leg FM (kg) | 11.6 ± 4.18 | 10.97 ± 4.16 | 10.05 ± 3.75 | −4.52 | −8.21 | −12.37 | 0.010 * | 0.000 * | 0.000 * |
| Trunk FM (kg) | 28.35 ± 9.47 | 24.33 ± 6.68 | 21.33 ± 6.04 | −9.64 | −12.28 | −20.72 | 0.000 * | 0.000 * | 0.000 * |
| Android FM (kg) | 5.12 ± 1.87 | 4.28 ± 1.29 | 3.66 ± 1.23 | −11.46 | −14.96 | −24.80 | 0.000 * | 0.000 * | 0.000 * |
| Gynoid FM (kg) | 6.53 ± 2.05 | 5.97 ± 1.92 | 5.34 ± 1.63 | −6.86 | −10.13 | −16.33 | 0.000 * | 0.000 * | 0.000 * |
| Whole FM (kg) | 46.15 ± 13.22 | 42.35 ± 11.96 | 38.04 ± 11.18 | −8.20 | −10.36 | −17.75 | 0.000 * | 0.000 * | 0.000 * |
| Arm FM (%) | 43.26 ± 9.9 | 42.55 ± 9.24 | 42.22 ± 9.11 | −2.41 | −3.74 | −6.36 | 0.010 * | 0.000 * | 0.000 * |
| Leg FM (%) | 36.39 ± 9.56 | 36.64 ± 10.22 | 35.94 ± 10.41 | −0.34 | −4.87 | −4.98 | 0.980 | 0.000 * | 0.000 * |
| Trunk FM (%) | 49.92 ± 6.6 | 48.32 ± 6.68 | 46.3 ± 7.18 | −2.52 | −6.13 | −8.31 | 0.000 * | 0.000 * | 0.000 * |
| Android FM (%) | 53.15 ± 6.34 | 51.48 ± 6.66 | 49.29 ± 7.52 | −2.57 | −6.10 | −8.22 | 0.010 * | 0.000 * | 0.000 * |
| Gynoid FM (%) | 42.51 ± 8.69 | 42.27 ± 9.24 | 41.19 ± 9.09 | −1.13 | −5.33 | −6.38 | 0.200 | 0.000 * | 0.000 * |
| Whole FM (%) | 43.87 ± 7.38 | 42.89 ± 7.42 | 40.67 ± 7.59 | −2.29 | −6.13 | −8.10 | 0.000 * | 0.000 * | 0.000 * |
| Arm LM (kg) | 5.96 ± 1.84 | 5.74 ± 1.49 | 5.74 ± 1.69 | −5.77 | −1.78 | −1.71 | 0.130 | 0.780 | 0.260 |
| Leg LM (kg) | 18.95 ± 4.26 | 17.97 ± 4.22 | 17.79 ± 4.46 | −5.17 | −1.37 | −6.53 | 0.000 * | 0.120 | 0.000 * |
| Trunk LM (kg) | 26.56 ± 4.81 | 24.85 ± 4.69 | 24.54 ± 4.90 | −5.30 | −0.54 | −6.09 | 0.000 * | 0.490 | 0.000 * |
| Android LM (kg) | 4.28 ± 0.89 | 3.91 ± 0.83 | 3.84 ± 0.85 | −6.76 | −1.59 | −8.36 | 0.000 * | 0.340 | 0.050 |
| Gynoid LM (kg) | 8.37 ± 1.63 | 7.85 ± 1.63 | 7.72 ± 1.71 | −5.70 | −1.54 | −7.28 | 0.000 * | 0.110 | 0.000 * |
| Whole LM (kg) | 55.39 ± 10.52 | 52.9 ± 10.37 | 52.94 ± 10.46 | −4.58 | 0.25 | −4.49 | 0.000 * | 0.790 | 0.000 * |
| Bone Mass (kg) | 2.78 ± 0.59 | 2.80 ± 0.58 | 2.77 ± 0.59 | −0.45 | −1.02 | −1.45 | 0.240 | 0.050 | 0.060 |
| BIA | |||||||||
| Rz (Ohm) | 471.89 ± 69.35 | 516.71 ± 75.68 | 508.00 ± 62.24 | 8.88 | −0.75 | 8.56 | 0.000 * | 0.730 | 0.040 |
| Xc (Ohm) | 47.84 ± 13.45 | 52.94 ± 10.38 | 51.86 ± 7.44 | 15.51 | 0.57 | 14.89 | 0.010 * | 0.690 | 0.110 |
| TBW (kg) | 44.98 ± 7.88 | 41.65 ± 7.43 | 41.08 ± 7.03 | −5.71 | −1.57 | −6.43 | 0.000 * | 0.280 | 0.000 * |
| ECW (kg) | 21.28 ± 4.37 | 19.33 ± 3.22 | 19.01 ± 2.87 | −8.05 | −2.11 | −7.99 | 0.000 * | 0.110 | 0.010 * |
| BCM (kg) | 31.37 ± 8.42 | 30.2 ± 7.14 | 29.69 ± 6.77 | 0.67 | 1.36 | −0.11 | 0.900 | 0.600 | 0.570 |
| PA (°) | 5.81 ± 1.58 | 5.89 ± 1.06 | 5.89 ± 0.90 | 6.09 | 1.43 | 6.26 | 0.180 | 0.940 | 0.730 |
| CALORIMETRY | |||||||||
| VO2 (mL/min) | 251.88 ± 42.7 | 214.92 ± 33.56 | 235.03 ± 88.42 | −14.85 | 0.56 | −6.27 | 0.040 * | 0.970 | 0.410 |
| VCO2 (mL/min) | 208.88 ± 36.52 | 160.67 ± 34.26 | 160.81 ± 35.50 | −20.49 | −2.08 | −23.80 | 0.040 * | 0.510 | 0.000 * |
| RQ | 0.83 ± 0.03 | 0.73 ± 0.04 | 0.73 ± 0.04 | −12.37 | 0.07 | −12.01 | 0.000 * | 1.000 | 0.000 * |
| REE (kcal) | 1784.50 ± 313.18 | 1435.33 ± 223.71 | 1498.00 ± 316.65 | −16.83 | 1.94 | −16.59 | 0.010 * | 0.810 | 0.000 * |
| Parameters | Basal | Eight Weeks | p | ∆ Base–Eight Weeks |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Glycemia (mg/dL) | 170.06 ± 11.18 | 99.67 ± 9.4 | 0.000 * | −39.70 |
| HbA1c (%) | 7.33 ± 0.35 | 6.16 ± 0.07 | 0.000 * | −15.73 |
| HbA1c (mmol/L) | 57.06 ± 3.2 | 44.06 ± 2.08 | 0.000 * | −21.83 |
| Insulin (uU/mL) | 17.89 ± 4.71 | 8.66 ± 3.64 | 0.000 * | −51.54 |
| Homa Index | 7.47 ± 2.07 | 2.13 ± 0.88 | 0.000 * | −71.39 |
| AST (U/L) | 36.75 ± 5.06 | 21.21 ± 4.49 | 0.030 * | −29.37 |
| ALT (U/L) | 45.08 ± 6.97 | 24.07 ± 5.69 | 0.000 * | −41.09 |
| Creatinine (mg/dl) | 0.81 ± 0.16 | 0.77 ± 0.14 | 0.040 | −4.50 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, L.; Marchetti, M.; Gualtieri, P.; Di Renzo, L.; Belcastro, M.; De Santis, G.L.; Perrone, M.A.; De Lorenzo, A. Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications. Nutrients 2019, 11, 1526. https://doi.org/10.3390/nu11071526
Romano L, Marchetti M, Gualtieri P, Di Renzo L, Belcastro M, De Santis GL, Perrone MA, De Lorenzo A. Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications. Nutrients. 2019; 11(7):1526. https://doi.org/10.3390/nu11071526
Chicago/Turabian StyleRomano, Lorenzo, Marco Marchetti, Paola Gualtieri, Laura Di Renzo, Meriann Belcastro, Gemma Lou De Santis, Marco Alfonso Perrone, and Antonino De Lorenzo. 2019. "Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications" Nutrients 11, no. 7: 1526. https://doi.org/10.3390/nu11071526
APA StyleRomano, L., Marchetti, M., Gualtieri, P., Di Renzo, L., Belcastro, M., De Santis, G. L., Perrone, M. A., & De Lorenzo, A. (2019). Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications. Nutrients, 11(7), 1526. https://doi.org/10.3390/nu11071526