Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action

 ,
,
Abstract
:1. Introduction
2. Clinical Practice Guidelines for the Management of OTRD
3. Review on the Use of Oligomeric Enteral Nutrition Formulas in Malnourish Patients with OTRD
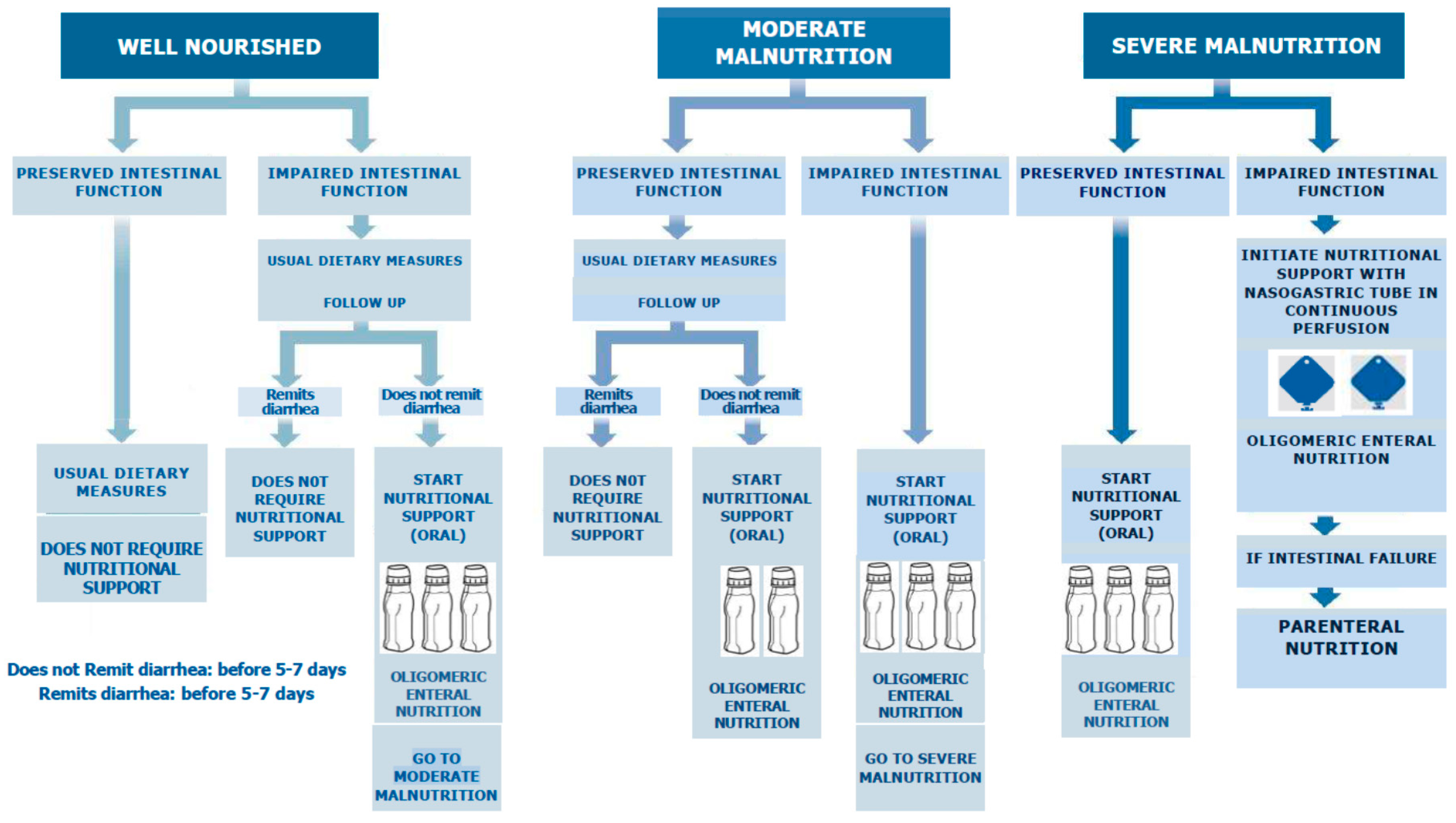
4. Nutritional Support Algorithm in Patients with OTRD
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Henson, C.C.; Davidson, S.E.; Lalji, A. Gastrointestinal symptoms after pelvic radiotherapy: A national survey of gastroenterologists. Support Care Cancer 2012, 20, 2129–2139. Available online: https://doi.org/10.1007/s00520-011-1323-5 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Basile, D.; Di Nardo, P.; Corvaja, C.; Garattini, S.K.; Pelizzari, G.; Lisanti, C.; Bortot, L.; Da Ros, L.; Martoletti, M.; Borghi, M.; et al. Mucosal Injury during Anti-Cancer Treatment: From Pathobiology to Bedside. Cancers 2019, 11, 857. Available online: https://doi.org/10.3390/cancers11060857 (accessed on 13 March 2019). [CrossRef]
- Nugent, B.; Lewis, S.; O’Sullivan, J.M. Enteral feeding methods for nutritional management in patients with head and neck cancers being treated with radiotherapy and/or chemotherapy. Cochrane Database Syst. Rev. 2013, 31. Available online: https://doi.org//10.1002/14651858.CD007904.pub3. (accessed on 18 March 2019).
- Forde, C. Systemic anti-cancer therapy-induced diarrhoea. Br. J. Hosp. Med (Lond.) 2017, 78, C135–C139. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.J.; Keefe, D.M. Cancer chemotherapy-induced diarrhoea and constipation: Mechanisms of damage and prevention strategies. Support Care Cancer 2006, 14, 890–900. Available online: https://doi.org/10.1007/s00520-006-0040-y (accessed on 13 March 2019). [CrossRef] [PubMed]
- Maughan, T.S.; James, R.D.; Kerr, D.J.; Ledermann, J.A.; McArdle, C.; Seymour, M.T.; Cohen, D.; Hopwood, P.; Johnston, C.; Stephens, R.J.; et al. Comparison of survival, palliation, and quality of life with three chemotherapy regimens in metastatic colorectal cancer: A multicentre randomised trial. Lancet 2002, 4, 1555–1563. Available online: https://doi.org/10.1016/S0140-6736(02)08514-8 (accessed on 18 March 2019). [CrossRef]
- Bowen, J.M. Mechanisms of TKI-induced diarrhea in cancer patients. Curr. Opin. Support. Palliat. Care 2013, 7, 162–167. Available online: https://doi.org./10.1097/SPC.0b013e32835ec861 (accessed on 21 March 2019). [CrossRef] [PubMed]
- Zhang, B.; Wu, Q.; Zhou, Y.L.; Guo, X.; Ge, J.; Fu, J. Immune-related adverse events from combination immunotherapy in cancer patients: A comprehensive meta-analysis of randomized controlled trials. Int. Immunopharmacol. 2018, 63, 292–298. Available online: https://doi.org/10.1016/j.intimp.2018.08.014 (accessed on 21 March 2019). [CrossRef]
- Gibsona, R.J.; Stringerb, A.M. Chemotherapy-induced diarrhea. Curr. Opin. Support. Palliat. Care 2009, 3, 31–35. Available online: https//doi.org/10.1097/SPC.0b013e32832531bb (accessed on 18 March 2019). [CrossRef]
- Argilés, J.M. Cancer-associated malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S39–S50. Available online: https://doi.org/10.1016/j.ejon.2005.09.006 (accessed on 18 March 2019). [CrossRef]
- Ding, P.N.; Lord, S.J.; Gebski, V.; Links, M.; Bray, V.; Gralla, R.J.; Yang, J.C.; Lee, C.K. Risk of Treatment-Related Toxicities from EGFR Tyrosine Kinase Inhibitors: A Meta-analysis of Clinical Trials of Gefitinib, Erlotinib, and Afatinib in Advanced EGFR-Mutated Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 633–643. Available online: https://doi.org/10.1016/j.jtho.2016.11.2236 (accessed on 21 March 2019). [CrossRef]
- Gupta, A.; De Felice, K.M.; Loftus Jr, E.V.; Khanna, S. Systematic review: Colitis associated with anti-CTLA-4 therapy. Aliment. Pharmacol. Ther. 2015, 42, 406–417. Available online: https://doi.org/10.1111/apt.13281 (accessed on 21 March 2019). [CrossRef] [PubMed]
- Boussios, S.; Pentheroudakis, G.; Katsanos, K.; Pavlidis, N. Systemic treatment-induced gastrointestinal toxicity: Incidence, clinical presentation and management. Ann. Gastroenterol. 2012, 25, 106–118. [Google Scholar] [PubMed]
- Capuano, G.; Grosso, A.; Gentile, P.C.; Battista, M.; Bianciardi, F.; Di Palma, A.; Pavese, I.; Satta, F.; Tosti, M.; Palladino, A.; et al. Influence of weight loss on outcomes in patients with head and neck cancer undergoing concomitant chemoradiotherapy. Head Neck 2008, 30, 503. Available online: https://doi.org/10.1002/hed.20737 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. Available online: https://doi.org/10.1016/j.clnu.2016.07.015 (accessed on 18 March 2019). [CrossRef] [PubMed]
- Elia, M.; Van Bokhorst-de van der Schueren, M.A.; Garvey, J.; Goedhart, A.; Lundholm, K.; Nitenberg, G.; Stratton, R.J. Enteral (oral or tube administration) nutritional support and eicosapentaenoic acid in patients with cancer: A systematic review. Int. J. Oncol. 2006, 28, 5–23. Available online: https://doi.org/10.3892/ijo.28.1.5 (accessed on 20 March 2019). [CrossRef] [PubMed] [Green Version]
- Chow, R.; Bruera, E.; Chiu, L.; Chow, S.; Chiu, N.; Lam, H.; McDonald, R.; DeAngelis, C.; Vuong, S.; Ganesh, V.; et al. Enteral and parenteral nutrition in cancer patients: A systematic review and meta-analysis. Ann. Palliat Med. 2016, 5, 30–41. Available online: https://doi.org/10.3978/j.issn.2224-5820.2016.01.01 (accessed on 7 August 2019). [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. Available online: https://doi.org/10.1016/j.clnu.2016.09.004. (accessed on 18 March 2019). [CrossRef] [PubMed]
- Saltz, L.B. Understanding and managing chemotherapy-induced diarrhea. J. Support Oncol. 2003, 1, 35–46. Available online: https://www.supportiveoncology.net (accessed on 13 March 2019). [PubMed]
- Benson, A.L.B.; Ajani, J.A.; Catalano, R.; Engelking, C.; Kornblau, S.; Martenson, J.; McCallum, R.; Mitchell, E.P.; O’Dorisio, T.M.; Vokes, E.E.; et al. Recommended Guidelines for the Treatment of Cancer Treatment-Induced Diarrhea. J. Clin. Oncol. 2004, 22, 2918–2926. Available online: https://doi:10.1200/JCO.2004.04.132 (accessed on 13 March 2019). [CrossRef] [PubMed] [Green Version]
- Maroun, J.A.; Anthony, L.B.; Blais, N.; Burkes, R.; Dowden, S.D.; Dranitsaris, G.S.B.; Shah, A.; Thirlwell, M.P.; Vincent, M.D.; wong, R.; et al. Prevention and management of chemotherapy-induced diarrhea in patients with colorectal cancer: A consensus statement by the Canadian Working Group on Chemotherapy-Induced Diarrhea. Curr. Oncol. 2007, 14, 13–20. Available online: https://doi:10.3747/co.2007.96 (accessed on 18 March 2019). [CrossRef]
- Lupiañez, Y. Enteritis Rádica. Prevención y tratamiento. Enfermería Docente 2008, 89, 31–32. Available online: http://www.juntadeandalucia.es/servicioandaluzdesalud/huvvsites/default/files/revistas/ED-89-10.pdf (accessed on 18 March 2019).
- Symptom Management Guideline: Cancer-Related Diarrea. BC Cancer Agency, 2010. Available online: http://www.bccancer.bc.ca/nursing-site/Documents/Symptom%20Management%20Guidelines/3Diarrhea.pdf (accessed on 20 March 2019).
- Stein, A.; Voigt, W.; Jordan, K. Chemotherapy-induced diarrhea: Pathophysiology, frequency and guideline-based management. Ther. Adv. Med. Oncol. 2010, 2, 51–63. Available online: https://doi.org/10.1177/1758834009355164 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Guideline for the Management of Chemotherapy Induced Diarrhoea in Adult Patients. University Hospitals Birmigham, 2012. Available online: https://www.uhb.nhs.uk/chemotherapy.htm (accessed on 13 March 2019).
- Shaw, C.; Taylor, T. Treatment-related diarrhea in patients with cancer. Clin. J. Oncol. Nurs. 2012, 6, 413–417. Available online: https://doi.org/10.1188/12.CJON.413-417 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Wedlake, L.J.; Shaw, C.; Whelan, K.; Andreyev, H.J. Systematic review: The efficacy of nutritional interventions to counteract acute gastrointestinal toxicity during therapeutic pelvic radiotherapy. Aliment. Pharmacol. Ther. 2013, 37, 1046–1056. Available online: https://doi.org/10.1111/apt.12316 (accessed on 18 March 2019). [CrossRef] [PubMed]
- McQuade, R.M.; Bornstein, J.C.; Nurgali, K. Anti-Colorectal Cancer Chemotherapy-Induced Diarrhoea: Current Treatments and Side-Effects. Int. J. Clin. Med. 2014, 5, 393–406. Available online: http://dx.doi.org/10.4236/ijcm.2014.57054 (accessed on 18 March 2019). [CrossRef] [Green Version]
- Andreyev, J.; Ross, P.; Donnellan, C.; Lennan, E.; Leonard, P.; Waters, C.; Wedlake, L.; Bridgewater, J. Guidance on the management of diarrhoea during cancer chemotherapy. Lancet Oncol. 2014, 15, 447–460. Available online: https://doi.org/10.1016/S1470-2045(14)70006-3 (accessed on 13 March 2019). [CrossRef]
- Peterson, D.E.; Boers-Doets, C.B.; Bensadoun, R.J.; Herrstedt, J. Management of oral and gastrointestinal mucosal injury: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, 139–151. Available online: https://doi.org/10.1093/annonc/mdv202 (accessed on 18 March 2019). [CrossRef] [PubMed]
- Guidelines for Management of Systemic Anti-Cancer Therapy Induced Diarrhoea in Adult Haematology and Oncology Patients. NOSCAN, 2015. Available online: https://www.noscan.scot.nhs.uk/guidelinesandprotocols/SACT/SACT%20SOPs/Documents/NOSCAN%20Diarrhoea%20Guidelines%201015.pdf (accessed on 18 March 2019).
- Guideline on Prevention and Management of Chemotherapy-Associated Diarrhoea. Oxford University Hospital NHS Foundation Trust, 2015. Available online: http://tvscn.nhs.uk/wp-content/uploads/2014/09/Cancer-Children-Diarrhoea-Guidelines-v2.1-Nov-2015.pdf (accessed on 18 March 2019).
- Grabenbauer, G.G.; Holger, G. Management of radiation and chemotherapy related acute toxicity in gastrointestinal cancer. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 655–664. Available online: http://dx.doi.org/10.1016/j.bpg.2016.06.001 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Mardas, M.; Radoslaw, M. Link between diet and chemotherapy related gastrointestinal side effects. Contemp. Oncol. (Pozn) 2017, 21, 162–167. Available online: https://doi.org/10.5114/wo.2017.66896. (accessed on 20 March 2019). [CrossRef] [PubMed]
- Jomar, R.; Gomes, R.; Leite, D.; Gomes, H.; Peres, E.; Junior, E. Nursing diagnoses in adult/elderly patients undergoing outpatient antineoplastic chemotherapy: A review. Ecancermedicalscience 2017, 11, 736. Available online: https://doi:10.3332/ecancer.2017.736 (accessed on 20 March 2019). [CrossRef]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.M.; Voss, A.C.; Piemonte, T. Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310. Available online: https://doi.org/10.1016/j.jand.2016.05.010. (accessed on 20 March 2019). [CrossRef] [PubMed]
- Karin, J.; Feyer, P.; Höller, U.; Link, L.; Wörmann, B.; Jahn, F. Supportive Treatments for Patients with Cancer. Dtsch Arztebl Int. 2017, 114, 481–487. Available online: https://doi.org/10.3238/arztebl.2017.0481 (accessed on 20 March 2019).[Green Version]
- PDQ Supportive and Palliative Care Editorial Board. Gastrointestinal Complications: Health Professional Version. In PDQ Cancer Information Summaries [Internet]; National Cancer Institute: Bethesda, MD, USA, 28 November 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK65768/ (accessed on 20 March 2019).
- Thomsen, M.; Vitetta, L. Adjunctive Treatments for the Prevention of Chemotherapy- and Radiotherapy-Induced Mucositis. Integr. Cancer Ther. 2018, 17, 1027–1047. Available online: https://doi.org/10.1177/1534735418794885 (accessed on 21 March 2019). [CrossRef] [PubMed] [Green Version]
- Management of Chemotherapy-Induced Diarrhea. Oncolink, 2018. Available online: https://www.oncolink.org/support/side-effects/gastrointestinal-side-effects/diarrhea (accessed on 21 March 2019).
- Bossi, P.; Antonuzzo, A.; Cherny, N.I.; Rosengarten, O.; Pernot, S.; Trippa, F.; Schuler, U.; Snegovoy, A. Diarrhoea in adult cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, 126–142. Available online: https://doi.org/10.1093/annonc/mdy145 (accessed on 21 March 2019). [CrossRef] [PubMed]
- Bossola, M. Nutritional interventions in head and neck cancer patients undergoing chemoradiotherapy: A narrative review. Nutrients 2015, 7, 265–276. Available online: https://doi.org/10.3390/nu7010265 (accessed on 20 March 2019). [CrossRef] [PubMed]
- Ravasco, P.; Monteiro-Grillo, I.; Camilo, M. Individualized nutrition intervention is of major benefit to colorectal cancer patients: long-term follow-up of a randomized controlled trial of nutritional therapy. Am. J. Clin. Nutr. 2012, 96, 1346–1353. Available online: https://doi.org/10.3945/ajcn.111.018838 (accessed on 20 March 2019). [CrossRef] [PubMed] [Green Version]
- Ohkura, Y.; Ueno, M.; Shindoh, J.; Iizuka, T.; Udagawa, H. Randomized controlled trial on efficacy of oligomeric formula (HINE E-GEL) versus polymeric formula (MEIN) enteral nutrition after esophagectomy for esophageal cancer with gastric tube reconstruction. Dis. Esophagus 2019, 32. Available online: https://doi.org/10.1093/dote/doy084 (accessed on 20 March 2019).
- O’Keefe, S.J.; Lee, R.B.; Anderson, F.P.; Gennings, C.; Abou-Assi, S.; Clore, J.; Heuman, D.; Chey, W. Physiological effects of enteral and parenteral feeding on pancreaticobiliary secretion in humans. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 284, 27–36. Available online: https://doi.org/10.1152/ajpgi.00155.2002 (accessed on 21 March 2019). [CrossRef] [PubMed]
- O’Sullivan, M.; O’Morain, C. Nutritional therapy in inflammatory bowel disease. Curr. Treat. Options Gastroenterol. 2004, 7, 191–1988. Available online: https://doi.org/10.1007/s11938-004-0040-2 (accessed on 21 March 2019). [CrossRef]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Kitagawa, T.; Matsumoto, K. Impact of elemental diet on mucosal inflammation in patients with active Crohn’s disease: Cytokine production and endoscopic and histological findings. Inflamm. Bowel Dis. 2005, 11, 580–588. Available online: https://doi.org/10.1097/01.MIB.0000161307.58327.96 (accessed on 21 March 2019). [CrossRef]
- Elting, L.S.; Cooksley, C.; Chambers, M.; Cantor, S.B.; Manzullo, E.; Rubenstein, E.B. The burdens of cancer therapy. Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer 2003, 98, 1531–1539. Available online: https://doi.org/10.1002/cncr.11671 (accessed on 18 March 2019). [CrossRef]
- Kawashima, R.; Kawakami, F.; Maekawa, T.; Yamamoto, H.; Koizumi, W.; Ichikawa, T. Elemental diet moderates 5-fluorouracil-induced gastrointestinal mucositis through mucus barrier alteration. Cancer Chemother. Pharmacol. 2015, 76, 269–277. Available online: https://doi.org/10.1007/s00280-015-2790-z (accessed on 18 March 2019). [CrossRef] [PubMed]
- Gwede, C.K. Overview of radiation- and chemoradiation-induced diarrhea. Semin. Oncol. Nurs. 2003, 19, 6–10. Available online: https://doi.org/10.1053/j.soncn.2003.09.008 (accessed on 18 March 2019). [CrossRef]
- Henson, C.C.; Burden, S.; Davidson, S.E.; Lal, S. Nutritional interventions for reducing gastrointestinal toxicity in adults undergoing radical pelvic radiotherapy. Cochrane Database Syst. Rev. 2013, 11. Available online: https://doi.org/10.1002/14651858.CD009896.pub2 (accessed on 18 March 2019).
- Brown, M.S.; Buchanan, R.B.; Karran, S.J. Clinical observations on the effects of elemental diet supplementation during irradiation. Clin. Radiol. 1980, 31, 19–20. Available online: https://doi.org/10.1016/S0009-9260(80)80075-4 (accessed on 18 March 2019). [CrossRef]
- Foster, K.J.; Brown, M.S.; Alberti, K.G.; Buchanan, R.B.; Dewar, P.; Karran, S.J.; Price, C.P.; Wood, P.J. The metabolic effects of abdominal irradiation in man with and without dietary therapy with an elemental diet. Clin. Radiol. 1980, 31, 13–17. Available online: https://doi.org/10.1016/S0009-9260(80)80073-0 (accessed on 20 March 2019). [CrossRef]
- Beer, W.H.; Fan, A.; Halsted, C.H. Clinical and nutritional implications of radiation enteritis. Am. J. Clin. Nutr. 1985, 41, 85–91. Available online: https://doi.org/10.1093/ajcn/41.1.85 (accessed on 18 March 2019). [CrossRef] [PubMed] [Green Version]
- McArdle, A.H.; Reid, E.C.; Laplante, M.P.; Freeman, C.R. Prophylaxis Against Radiation Injury: The Use of Elemental Diet Prior to and During Radiotherapy for Invasive Bladder Cancer and in Early Postoperative Feeding Following Radical Cystectomy and Heal Conduit. Arch. Surg. 1986, 121, 879–885. Available online: https://doi.org/10.1001/archsurg.1986.01400080021003 (accessed on 18 March 2019). [CrossRef]
- Craighead, P.S.; Young, S. Phase II study assessing the feasibility of using elemental supplements to reduce acute enteritis in patients receiving radical pelvic radiotherapy. Am. J. Clin. Oncol. 1998, 21, 573–578. [Google Scholar] [CrossRef]
- Capirci, C.; Polico, C.; Mondoliti, G.; Zorat, P.L.; Gava, A.; Turcato, G. Diet prevention of radiation acute enteric toxicity: Multicentric randomised study. Radiother. Oncol. 2000, 56, 44, (published data only unpublished sought but not used). [Google Scholar]
- McGough, C.; Wedlake, L.; Baldwin, C.; Hackett, C.; Norman, A.R.; Blake, P.; Harrington, K.; Tait, D.; Kho, V.; Frost, G.; et al. Clinical trial: Normal diet vs. partial replacement with oral E028 formula for the prevention of gastrointestinal toxicity in cancer patients undergoing pelvic radiotherapy. Alimen. Pharmacol. Ther. 2008, 27, 1132–1139. Available online: https://doi.org/10.1111/j.1365-2036.2008.03665.x (accessed on 13 March 2019). [CrossRef]
- Shao, F.; Xin, F.Z.; Yang, C.G.; Yang, D.G.; Mi, Y.T.; Yu, J.X.; Li, G.Y. The impact of microbial immune enteral nutrition on the patients with acute radiation enteritis in bowel function and immune status. Cell Biochem. Biophys. 2014, 69, 357–361. Available online: https://doi.org/10.1007/s12013-013-9807-1. (accessed on 20 March 2019). [CrossRef]
- Ishikawa, T.; Yasuda, T.; Doi, T.; Okayama, T.; Sakamoto, N.; Gen, Y.; Dohi, O.; Yoshida, N. The amino acid-rich elemental diet Elental preserves lean body mass during chemo- or chemoradiotherapy for esophageal cancer. Oncol. Rep. 2016, 36, 1093–1100. Available online: https://doi.org/10.3892/or.2016.4877 (accessed on 20 March 2019). [CrossRef] [PubMed]
- Tanaka, Y.; Takahashi, T.; Yamaguchi, K.; Osada, S.; Shimokawa, T.; Yoshida, K. Elemental diet plus glutamine for the prevention of mucositis in esophageal cancer patients receiving chemotherapy: A feasibility study. Support Care Cancer 2016, 24, 933–941. Available online: https://doi.org/10.1007/s00520-015-2864-9. (accessed on 20 March 2019). [CrossRef] [PubMed]
- Morishita, T.; Tsushita, N.; Imai, K.; Sakai, T.; Miyao, K.; Sakemura, R.; Kato, T.; Niimi, K.; Ono, Y.; Sawa, M. The Efficacy of an Oral Elemental Diet in Patients Undergoing Hematopoietic Stem Cell Transplantation. Intern. Med. 2016, 55, 3561–3569. Available online: https://doi.org/10.2169/internalmedicine.55.7310 (accessed on 20 March 2019). [CrossRef] [PubMed] [Green Version]
- Ogata, Y.; Ishibashi, N.; Yamaguchi, K.; Uchida, S.; Kamei, H.; Nakayama, G.; Hirakawa, H.; Tanigawa, M.; Akagi, Y. Preventive effects of amino-acid-rich elemental diet Elental on chemotherapy-induced oral mucositis in patients with colorectal cancer: A prospective pilot study. Support Care Cancer 2016, 24, 783–789. Available online: https://doi.org/10.1007/s00520-015-2844-0 (accessed on 20 March 2019). [CrossRef] [PubMed]
- Harada, K.; Ferdous, T.; Horinaga, D.; Uchida, K.; Mano, T.; Mishima, K.; Park, S.; Hanazawa, H.; Takahashi, S.; Okita, A.; et al. Efficacy of elemental diet on prevention for chemoradiotherapy-induced oral mucositis in patients with oral squamous cell carcinoma. Support Care Cancer 2016, 24, 953–959. Available online: https://doi.org/10.1007/s00520-015-2866-7. (accessed on 13 March 2019). [CrossRef]
- Okada, T.; Nakajima, Y.; Nishikage, T.; Ryotokuji, T.; Miyawaki, Y.; Hoshino, A.; Tokairin, Y.; Kawada, K.; Nagai, K.; Kawano, T. A prospective study of nutritional supplementation for preventing oral mucositis in cancer patients receiving chemotherapy. Asia Pac. J. Clin. Nutr. 2017, 26, 42–48. Available online: https://doi.org/10.6133/apjcn.112015.03 (accessed on 13 March 2019). [PubMed]
- Tanaka, Y.; Ueno, T.; Yoshida, N.; Akutsu, Y.; Takeuchi, H.; Baba, H.; Matsubara, H.; Kitagawa, Y.; Yoshida, K. The effect of an elemental diet on oral mucositis of esophageal cancer patients treated with DCF chemotherapy: A multi-center prospective feasibility study (EPOC study). Esophagus 2018, 15, 239–248. Available online: https://doi.org/10.1007/s10388-018-0620-1. (accessed on 13 March 2019). [CrossRef]
- Harada, K.; Minami, H.; Ferdous, T.; Kato, Y.; Umeda, H.; Horinaga, D.; Uchida, K.; Park, S.C.; Hanazawa, H.; Takahashi, S.; et al. The Elental elemental diet for chemoradiotherapy-induced oral mucositis: A prospective study in patients with oral squamous cell carcinoma. Mol. Clin. Oncol. 2019, 10, 159–167. Available online: https://doi.org/10.3892/mco.2018.1769 (accessed on 13 March 2019). [CrossRef]
- Toyomasu, Y.; Mochiki, E.; Yanai, M.; Suzuki, M.; Yanoma, T.; Kimura, A.; Kogure, N.; Ogata, K.; Kuwano, H. A prospective pilot study of an elemental nutritional supplement for prevention of oral mucositis during S-1 adjuvant chemotherapy for gastric cancer. Surg. Oncol. 2019, 29, 97–101. Available online: https://doi.org/10.1016/j.suronc.2019.04.003 (accessed on 13 March 2019).
- Peterson, D.E.; Bensadoun, R.J.; Roila, F. Management of oral and gastrointestinal mucositis: ESMO clinical practice guidelines. Ann. Oncol. 2011, 22, 78–84. Available online: https://doi.org/10.1093/annonc/mdr391 (accessed on 20 March 2019). [CrossRef]
- Gibson, R.J.; Keefe, D.M.; Lalla, R.V.; Bateman, E.; Blijlevens, N.; Fijlstra, M.; King, E.E.; Stringer, A.M.; van der Velden, W.J.; Yazbeck, R.; et al. Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/ International Society of Oral Oncology (MASCC/ISOO). Systematic review of agents for the management of gastrointestinal mucositis in cancer patients. Support Care Cancer 2013, 21, 313–326. Available online: https://doi.org/10.1007/s00520-012-1644-z (accessed on 18 March 2019). [CrossRef]
- Bossi, P.; Locati, L.D.; Licitra, L. Palifermin in prevention of head and neck cancer radiation-induced mucositis: not yet a definitive word on safety and efficacy profile. J. Clin. Oncol. 2012, 30, 565–567. Available online: https://doi.org/10.1200/JCO.2011.39.1136 (accessed on 13 March 2019). [CrossRef] [PubMed]
- Harada, K.; Ferdous, T.; Mizukami, Y.; Mishima, K. Elemental diet inhibits proinflammatory cytokine production in keratinocytes through the suppression of NF-κB activation. Oncol. Rep. 2018, 40, 361–368. Available online: https://doi.org/10.3892/or.2018.6440 (accessed on 18 March 2019). [PubMed]
- Harada, K.; Ferdous, T.; Kobayashi, H.; Ueyama, Y. Elemental diet accelerates the recovery from oral mucositis and dermatitis induced by 5 Fluorouracil through the induction of fibroblast growth factor 2. Integr. Cancer Ther. 2018, 17, 423–430. Available online: https://doi.org/10.1177/1534735417721014 (accessed on 18 March 2019). [CrossRef] [PubMed]
- Andou, A.; Hisamatsu, T.; Okamoto, S.; Chinen, H.; Kamada, N.; Kobayashi, T.; Hashimoto, M.; Okutsu, T.; Shimno, K.; Takeda, T.; et al. Dietary histidine ameliorates murine colitis by inhibition of proinflammatory cytokine production from macrophages. Gastroenterology 2009, 136, 564–574. Available online: https://doi.org/10.1053/j.gastro.2008.09.062 (accessed on 21 March 2019). [CrossRef] [PubMed]
- Fijlstra, M.; Schierbeek, H.; Voortman, G.; Dorst, K.Y.; van Goudoever, J.B.; Rings, E.H.; Tissing, W.J. Continuous enteral administration can enable normal amino acid absorption in rats with methotrexate-induced gastrointestinal mucositis. J. Nutr. 2012, 142, 1983–1990. Available online: https://doi.org/10.3945/jn.112.165209 (accessed on 21 March 2019). [CrossRef] [PubMed]
- McLaughlin, S.D.; Culkin, A.; Cole, J.; Clark, S.K.; Tekkis, P.P.; Ciclitira, P.J.; Nicholls, R.J.; Whelan, K. Exclusive elemental diet impacts on the gastrointestinal microbiota and improves symptoms in patients with chronic pouchitis. J. Crohn’s Colitis 2013, 7, 460–466. Available online: https://doi.org/10.1016/j.crohns.2012.07.009 (accessed on 20 March 2019). [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Jensen, G.; Correia, M.I.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. Available online: https://doi.org.10.1016/j.clnu.2018.08.002 (accessed on 20 March 2019). [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year | Oral HidratatIon | LowF | Low Fiber | Soluble Fiber | Small, Frequent Meals | Avoid Spicy, Fried Foods | Avoid Insoluble Fiber | Avoid Very Hot or Cold Foods/Fluids | Avoid Sorbitol-coNtaining Substances | Avoid Alcohol, Caffeine | Limiting Lactose-coNtaining Products | Enteralor ParenteraLnutrition |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Saltz, LB (2003) [19] | 3–4 L water, clear soup, noncarbonated soft drinks | x | x | x | x | x | Supplementation with the amino acid glutamine | |||||
| Benson, Al B. (artículo especial) (2004) [20] | 8–10 glasses of clear liquids at day | x | x | x | x | Avoid high-osmolar supplements | ||||||
| Canadian Working Group (2007) [21] | Hydration oral | x | x | x | ||||||||
| Lupiañez Y. (2008). [22] | Fluids noncarbonated, nor irritants | x | x | x | x | x | Indicated in diarrhea (oligomeric formula) | |||||
| BC Cancer Agency (2010) [23] | 10–12 cups of fluids throughout the day | x | x | x | x | x | x | x | x | x | x | May be indicated in GRADE 3 or 4 diarrhea |
| Stein, A (2010) [24] | Drink 8–10 large glasses of clear liquids a day (eg, Gatorade or broth) | x | x | x | ||||||||
| Pan Birmingham Cancer Network (2012) [25] | Drink plenty of fluids. | x | x | x | x | Temporarily to see if this improves symptoms | ||||||
| Shaw, C (2012) [26] | three to four liters of fluid per day | x | x | x | x | |||||||
| Wedlake, L.J. (2013) [27] | should not be recommended | should not be recommended | Should not be recommended | Total replacement of diet with elemental formula may be appropriate in severe toxicity. | ||||||||
| McQuade, RM (2014) [28] | Drink 8–10 large glasses of clear liquids a day | x | x | |||||||||
| Andreyev, J (2014) [29] | Five sachets in 1 L water (consider 8–10 sachets in 1 L is for replacing electrolyte deficits) | x | Especially if the diarrhea is accompanied by marked bloating | |||||||||
| ESMO Clinical Practice Guidelines (2015) [30] | x | x | x | Probiotics to prevent diarrhea in a pelvic malignancy | ||||||||
| North of Scotland Cancer Network (2015) [31] | Increase oral fluids (2–3 L per day), | x | x | x | x | x | ||||||
| Oxford University hospital NHS foundation trust (2015) [32] | Fluids appropriate for weight/age | x | ||||||||||
| Grabenbauer, G (2016) [33] | x | x | x | Enteral nutrition with severe malnutrition or no enteral food intake for >7 days or insufficient intake | ||||||||
| Mardas, M. (2017) [34] | Fluids isotonic | x | x | x | x | x | x | x | Avoid high osmolar dietary supplements | |||
| Ecancer medical science (2017) [35] | Fluids | |||||||||||
| Thompson, KL (2017) [36] | Hydration oral | Dietary supplements containing EPA or MFS (fish oil), glutamic, vitamins | ||||||||||
| Karin, J. (2017) [37] | High fluid intake | x | x | x | ||||||||
| PDQ Supportive and Palliative Care. NCI (2018) [38] | Liquid intake to at least 3 L per day (e.g., water, sports drinks..)avoid beverages. | x | x | x | x | x | x | x | x | x | x | |
| Thomsen, M (2018) [39] | Fluids | Activated charcoal, glutamine, and probiotics | ||||||||||
| Oncolink (2018) [40] | 8–10 glasses of clear liquids per day | x | x | x | x | |||||||
| ESMO Clinical Practice Guidelines (2018) [41] | Diluted fruit juices and flavored soft drinks along with saltine crackers and broths or soups | x | x | x | There is insufficient evidence | Glutamine and omega fatty acids. Requires more studies. |
| Author, Year | Type of Study | Number Patients, Sex, Age (y) | Disease | Intervention | Follow-Up | Component Diet | Object of Study | Results | Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Brown [52] 1980 | One single-centre parallel group unblinded RCT | 68 patients (16 in control group, 30 who adhered to the ON diet and 21 who did not adhere to the full period of supplementation). Men 70%, 69–29y. | Mainly urological tumours, with many other types of primary tumours. | Compare reduced fibre diet (control) versus three sachets of ON with a reduced fibre diet. | During irradiation | Vivonex HN (Eaton Lab): 900 kcal and 40 g of mixed amino acids, simple sugars, fats, vitamins and mineral. | Reported weight and stool frequency. | Mean stool frequency 4/d for all three groups. Mean weight loss was 1.6 kg, 0.5 kg and 1.7 kg respectively. | Heterogeneous group. Only means were reported with no measurement of variance given |
| Foster [53] 1980 | One single-centre parallel group unblinded RCT | 32 patients (12 control and 20 intervention). 75% male, 66y, | Carcinoma bladder, prostate, uterus and testis | Compare reduced fibre diet (control) versus three sachets of Vivonex HN with a reduced fibre diet. | During irradiation | Vivonex HN (Eaton Lab): 900 kcal and 40 g of mixed amino acids, simple sugars, fats, vitamins and mineral. | Investigate the metabolic effects of therapeutic irradiation in different diet planning | Weight loss similar (1.4 vs. 1 Kg). No differences in metabolic and hormonal determinations. | Few of the patients were underweight at the start of treatment. |
| Beer [54] 1985 | One single-centre, prospective cohort study | 8 patients (7 female, 1 male). 3 control and 5 intervention. | Gynecologic or testicular malignancy | Compare oral diet versus vivonex-HN and Criticare-HN | Five days | Vivonex HN (Eaton Lab): 900 kcal and 40 g of mixed amino acids, simple sugars, fats, vitamins and mineral. Criticare HN: 900 kcal and 38 g of protein hydrolyzed casein, amino acids | Investigate weight and stool frequency | The mean daily fecal weight and energy were decreased | Few patients, The follow-up is very short |
| McArle [55] 1986 | One single-centre parallel group unblinded RCT | 56 patients (32 control and 24 intervention). 75% men, 65y | Invasive bladder cancer | Control: regular hospital diet or TPN during RT. Intervention: 1600–2000 Kcal during 3 days before RT and during RT supplementation with ON continuous feeding nasoduodenal tube or by mouth. | During irradiation | Vital HNR (Ross Lab): Partially hy drolyzed whey, meat, soy, hydrolyzed cornstarch and sucrose, safflower oil and MCT. | Investigate whether elemental diet could prophylaxis intestinal injury by radiotherapy. | The severity of the diarrhea in control was significantly greater. No bloody diarrhea. Positive nitrogen balance. Biopsy ileal normal mucosa morphologia and maintenance enzyme activity. | Control group is retrospective dates. |
| Craighead [56] 1998 | One single-centre uncontrolled phase II prospective cohort study | 61 patients (16 intervention group and a cohort of 45 patients (control) | primary cervical and endometrial cancer patients | Intervention with ON. Both cohorts diet restricted lactose, low fibre (12g daily), moderate fat intake (< 30% calories), adequate protein and carbohydrate. Intake of fruits, caffeine and other bowel stimulants restricted. | From three days before the start of radiotherapy to the last day of radiotherapy | Vital HNR: Partially hy drolyzed whey, meat, soy, hydrolyzed cornstarch and sucrose, safflower oil and MCT. | Assess compliance elemental supplements and preliminary assess of the efficacy. | Intervention vs. control: RTOG grade (55% vs. 15%, p < 0.001); Mean (SD) duration of diarrhoea during treatment was 5.85 days (4.44) vs. 12.2 days (6.95). | The study was small and not powered for GI symptoms or weight. Neither randomised nor controlled. Diarrhoea was not clearly defined. It was not clear whether there were any differences between baseline characteristics of the cohorts. |
| Capirci [57] 2000 | Conference abstract of a multicentre RCT | 677 patients (332 intervention group and 345 control group). | 439 with primary rectal cancer, 228 primary uterine cancer and 10 prostate cancer. | Natural diet plus elemental diet compared with standard diet (control) | Not defined | OD Not defined. | The outcomes were RTOG score and change in weight pre- and post-radiotherapy. | Toxicity significantly less in intervention group. 12 vs. 44 patients required a break in radiotherapy due to GI toxicity in the intervention and control group. The total numbers with each grade of diarrhoea were not reported. Weight response significant differences intervention vs. control: grade 1 toxicity (+1 vs. 0 Kg ), grade 2 (0 vs. −1.3 Kg) and grade 3–4 (−5.5 vs. −4 Kg) | There is no full report. Available data limited. It was not clear whether change in weight reported was mean change in weight and no measure of variance was reported. The statistical methods not described. Heterogeneous group. |
| McGough [58] 2008 | One single-centre parallel group unblinded RCT | 50 patients (29 women and 21 men). Intervention (25 people), Control (25 people) | Gynaecological, urological or lower GI malignancy | Control: habitual diet. Intervention: Replace one meal per day (33% of daily calories) with ON. | The first three weeks of radiotherapy. | EO28 Extra (SHS Lab): 85 Kcal, 14% protein, 35% fats (MCT 35%), 52% carbohydrate. | Primary outcome was GI symptoms at week five using IBDQB index. Other outcomes: GI symptoms using VIQ and RTOG toxicity grade, Weight and BMI, and Faecal Calprotectin | GI symptoms increased between baseline and both weeks three and five (P value < 0.001) in both groups. VIQ scores improved for patients in the intervention group comparing week 10 versus week five (P value < 0.001) but not in the control group (P value = 0.06). there was poor compliance with the intervention (6/25, 24%) and no improvement was seen in terms of GI symptoms or nutritional status. | Different baseline characteristics in terms of primary tumour and treatment regimen, The median intake of elemental diet, was lower than the prescribed volume required to provide 33% of caloric requirement. Six patients were non-compliant |
| Feng Shao [59] 2013 | One single-centre parallel group unblinded RCT | 46 patients (24 treatment group and 22 control group,). (22 males and 24 females), 60.2y. | Abdominal tumor with post-radiation enteritis | Intervention: Peptisorb plus triple live microorganismal tablets, L-Glutamine enteric capsule and fish oil capsule. Control: Peptisorb only | Whenrceiving radiotherapy or within 3 weeks post-radiotherapy | Peptisorb: ON 16 % protein (85 % small peptides and 15 % amino acid peptide), 9 % fat and 75 % carbohydrates. Microorganismal agent comprised Bifidobacterium, lactobacillus and Streptococcus thermophilus. | Investigate the effect of microbial immune enteral nutrition by microecopharmaceutics and deep sea fish oil and glutamine and Peptisorb on the patients with acute radiation enteritis in bowel function and immune status. | Intervention group: Abdominal pain, bloating and diarrhea was better than the control group (P values were 0.018, 0.04 and 0.008 after 7 days; P values were 0.018, 0.015 and 0.002 after 14 days); and the cellular immune parameters were better than the control group(P = 0.008, P = 0.039, P = 0.032); | Heterogeneous group. Difficult know if the results are because, mirocoorganism, glutamin o or fish oil. Both use ON. |
| Author, Year | Type of Study | Numbrer patientes, Sex, Age (y). | Disease | Intervention | Follow-Up | Component Diet | Object of Study | Results | Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Ishikawa [60] 2016 | Randomized, open label, phase 2 clinical trial | 33 patients (17 azulene and 16 OD) | Primarysquamous cell carcinoma of the esophagus who were scheduled to undergo chemotherapy or chemoradiotherapy | Randomized to receive either azulene oral rinse (Arm 1) or OD (Arm 2) | During the treatment cycle (4 weeks). | Elental® (Ajinomoto Pharmaceutical) (80 g/ 300 kcal amino-acid-rich, fat free, elemental diet) | Examine the preventive effects of OD on oral mucositis and sarcopenia progression during chemo (chemoradio) therapy for esophageal cancer | OD tended to reduce the incidence of oral mucositis (Arm 1, 23.5% and Arm 2, 12.5%), but there was no statistically significant difference. The average body mass index and body fat mass decreased significantly in both groups. Lean body mass was reduced in Arm 1, but was increased in Arm; the relative change of lean body mass after the treatment was significant between Arm 1 and Arm 2 (p = 0.007). The incidence of diarrhea was greater in Arm 2 than in Arm 1 (31.3 and 11.8%, respectively), and was grade 2 or less. | Single institution, small patient number |
| Tanaka [61] 2016 | One single-centre parallel group unblinded RCT | 30 patients (10 control, 10 Glutamin group and 10 Glutamin plus OD). 90% female. Age 68–75y. | Esophageal cancer | Control (no treatment), Gln group (oral 8910 mg Gln/day), Gln plus OD group. | Oral administration of Glutamin and OD began 1 week before chemotherapy and continued during treatment. | Elental® (Ajinomoto Pharmaceutical) (80 g/ 300 kcal amino-acid-rich, fat free, elemental diet) | Investigate the effect of glutamine and OD chemotherapy-inducOD oral mucositis in esophageal cancer patients | The incidence of grade ≥2 oral mucositiswas 60% in control group, 70 % in Glutamin group, and 10 % in Glutamin plus OD group. The percentage of change in body weight and diamine oxidase activity from before chemotherapy was higher in Glutamin plus OD group than control group. | Small number of patients. Effects not well explained. |
| Morishita [62] 2016 | One single-centre prospective cohort study | 73 patients (23 autologous HSCT and 50 allogeneic). 21 Control and 52 intervention. Age 47y (17–67). Male 50% intervention and 70% control. | hematopoietic stem cell transplantation (HSCT) | The first 21 patients did not receive OD and in the successive 52 patients received OD | Oral OD was started before conditioning and was continued until 28 days after transplantation | Elental® (Ajinomoto Pharmaceutical) (80 g/ 300 kcal amino-acid-rich, fat free, elemental diet) | The primary endpoint: hospitalization period. The secondary endpoint: occurrence of oral mucositis, nausea, diarrhea and fever. | The median hospitalization period was significantly shorter in intervention group compared to control (34 days vs. 50 days; p = 0.007). Grade 3–4 oral mucositis occurred less in intervention than control (25% vs. 48%; p = 0.06). There were no significant differences in the use of opioid agents, grade 3–4 diarrhea, or grade 3–4 nausea, for both frequency and duration | Single institution, small patient number, prospective cohort study and included both autologous and allogeneic patients. |
| Ogata [63] 2016 | One single-centre prospective pilot study | 22 patients (10 male and 12 Female) 67y | Metastatic colorectal cancer patients after developing grade 1–3 oral mucositis. | The OD Elental® (80 g/300 kcal or more per day) was given perorally in addition to normal oral ingestion, together with chemotherapy in each course lasting 2 to 3 weeks (on days 1–14 or days 1–21). | Introduction of OD after developing grade 1–3 oralmucositis | Elental® (Ajinomoto Pharmaceutical) (80 g/ 300 kcal amino-acid-rich, fat free, OD) | Evaluate the preventive effects of Elental®, on chemotherapy-induced oral mucositis in colorectal cáncer. | The maximum grade of oral mucositis decreased in 18 of the 22 patients during the first treatment course with Elental® (p = 0.0002) and in 20 of the 22 patients in the second course (p < 0.0001). | Single institution, small simple size, no control group. |
| Harada [64] 2016 | One single-centre retrospective study | 74 patients (37 intervention and 37 control group) | Oral squamous cell carcinoma (OSCC) patients who underwent radiation with/without chemotherapy | Recorded data on a daily basis and compared the data from 37 patients who received OD (intervention group) with those from 37 patients who did not receive OD (the control group) | During the treatment period (6 weeks). | Elental® (Ajinomoto Pharmaceutical) (80 g/300 kcal amino-acid-rich, fat free, elemental diet) | Evaluate the preventive effects of Elental®, on radiotherapy- or chemoradiotherapy-induced mucositis in OSCC patients. | Most of the patients who consumed OD suffered from a lower degree of mucositis compared to control group. OD was associated with a significantly improved rate of completion of chemoradiation (no interruption). There was no significant difference between OD group and control group in terms of mean change of body weight or total protein and albumin levels in blood serum before and after chemoradiation. | Single institution. Retrospective |
| Okada [65] 2017 | RCT | 22 patients (11 intervention and 11 control) | Esophageal cancer undergoing chemotherapy | Intervention: Elental (one pack per day) for 14 days and control not receiving Elental during chemotherapy | During chemotherapy | Elental® (Ajinomoto Pharmaceutical) (80 g/300 kcal amino-acid-rich, fat free, elemental diet) | Evaluate the influence of elemental diet on chemotherapy-induced oral mucositis and diarrhea. | The distribution of the maximum severity of oral mucositis showed a statistically significant reduction in the Elental group (p = 0.020). Regarding diarrhea, no difference was observed between the two groups. | Single institution, small sample size, most patients in the Elental group did not receive the same dose of Elental. |
| Tanaka [66] 2018 | Prospective multi-center feasibility study | 19 patients (males 100%), 68y (37–75y). | Stage II/III esophageal squamous cell carcinoma or adenocarcinoma | Orally administerOD OD 2 packs (160 g/day) during chemotherapy. | 2 cycles of chemotherapy | Elental® (Ajinomoto Pharmaceutical) (80 g/300 kcal amino-acid-rich, fat free, elemental diet) | The primary was the compliance of an orally administerOD OD 2 packs. The secondary endpoints were the incidence of oral mucositis; the rate of weight fluctuation; plasma diamine oxidase activity; the turnover rate of plasma proteins and adverse events. | 70% patients were able to complete the orally administered OD (160 g/day). The incidence of grade ≥ 2 oral mucositis in the OD completion group (15.4%:, 2 of 13 patients) was significantly lower than that in the non-completion group (66.7%, 4 of 6 patients) (p = 0.046). The grade 3 adverse events were: fatigue (15%), fever (15%), anorexia (15%); diarrhea (10%). | Small sample size, No control group, |
| Harada [67] 2019 | One single-centre prospective study | 50 patients (25 with OD and 25 control without). Males 70%. | Oral squamous cell carcinoma patients, who received radiation (60-70 Gy) with/without chemotherapy. | Intervention: 1 bottle/day of OD (80 g, 300 kcal) orally. Control without OD. | The median follow up period was 23 (8–37) months | Elental® (Ajinomoto Pharmaceutical) (80 g/300 kcal amino-acid-rich, fat free, elemental diet) | Evaluate the preventive effects of OD on radiotherapy- or chemoradiotherapy–induced mucositis in oral squamous cell carcinoma patients | Multivariate analysis indicated that most of the patients who received Elental® suffered from a lower degree of mucositis and showed significantly improved rate of completion of chemoradiation (no interruption) compared to the control group. There was a significant difference between the Elental® group and the control group in mean change of C-reactive protein levels in blood serum; however, there was no significant difference in mean change of body weight and total protein level in blood serum before and after chemoradiation. Diarrhea were no determinated. | Single institution, |
| Toyomasu [68] 2019 | One single-centre randomizOD open-label study | 22 patients (11 control and 11 intervention). Ages ranged from 59 to 80y. | Patients who underwent adjuvant chemotherapy for gastric cancer | One pack of OD per day | During adjuvant chemotherapy | Elental® (Ajinomoto Pharmaceutical) (80 g/300 kcal amino-acid-rich, fat free, elemental diet) | Whether an oral OD prevents chemotherapy associated oral mucositis and body weight loss. | The incidence of oral mucositis was significantly lower in the treatment group (9.1 %) than in the control group (27.3%). The median body weight loss in the treatment group was significantly smaller than that in the control group (P = 0.015). The treatment group was significantly associated with high cumulative S-1 continuation rates (log-rank p = 0.047). No differences in diarrhea between groups. | Single-institutional study with a small sample size |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanz-Paris, A.; Martinez-García, M.; Martinez-Trufero, J.; Lambea-Sorrosal, J.; Calvo-Gracia, F.; López-Alaminos, M.E. Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action. Nutrients 2019, 11, 1888. https://doi.org/10.3390/nu11081888
Sanz-Paris A, Martinez-García M, Martinez-Trufero J, Lambea-Sorrosal J, Calvo-Gracia F, López-Alaminos ME. Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action. Nutrients. 2019; 11(8):1888. https://doi.org/10.3390/nu11081888
Chicago/Turabian StyleSanz-Paris, Alejandro, María Martinez-García, Javier Martinez-Trufero, Julio Lambea-Sorrosal, Fernando Calvo-Gracia, and María Elena López-Alaminos. 2019. "Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action" Nutrients 11, no. 8: 1888. https://doi.org/10.3390/nu11081888
APA StyleSanz-Paris, A., Martinez-García, M., Martinez-Trufero, J., Lambea-Sorrosal, J., Calvo-Gracia, F., & López-Alaminos, M. E. (2019). Oligomeric Enteral Nutrition in Undernutrition, due to Oncology Treatment-Related Diarrhea. Systematic Review and Proposal of An Algorithm of Action. Nutrients, 11(8), 1888. https://doi.org/10.3390/nu11081888