Consumption and Sources of Saturated Fatty Acids According to the 2019 Canada Food Guide: Data from the 2015 Canadian Community Health Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Data Collection
2.3. Statistical Analyses
3. Results
3.1. CCHS Sample
3.2. Saturated Fatty Acids Consumption
4. Discussion
4.1. Saturated Fatty Acids Consumption in Canadian Adults
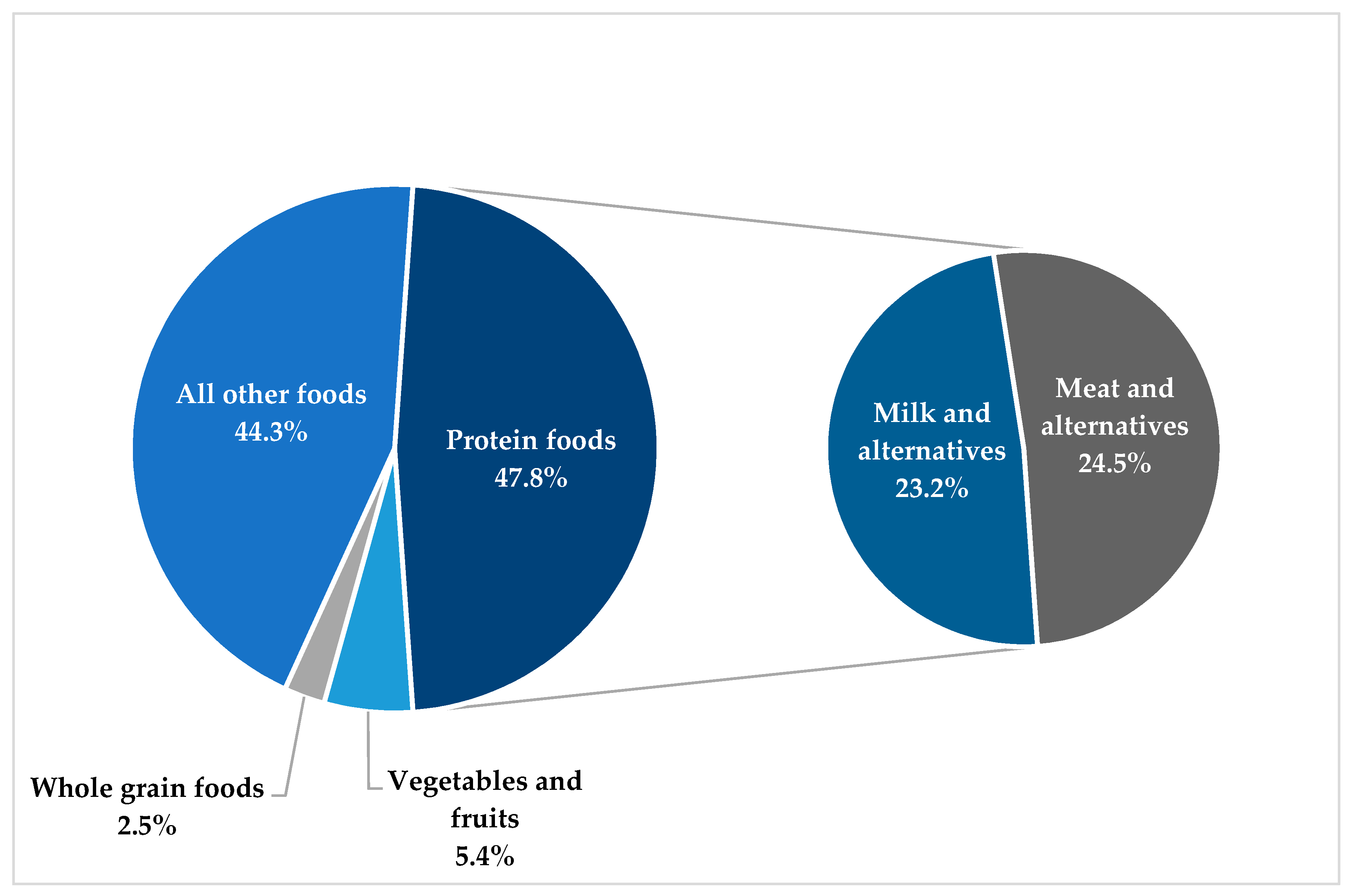
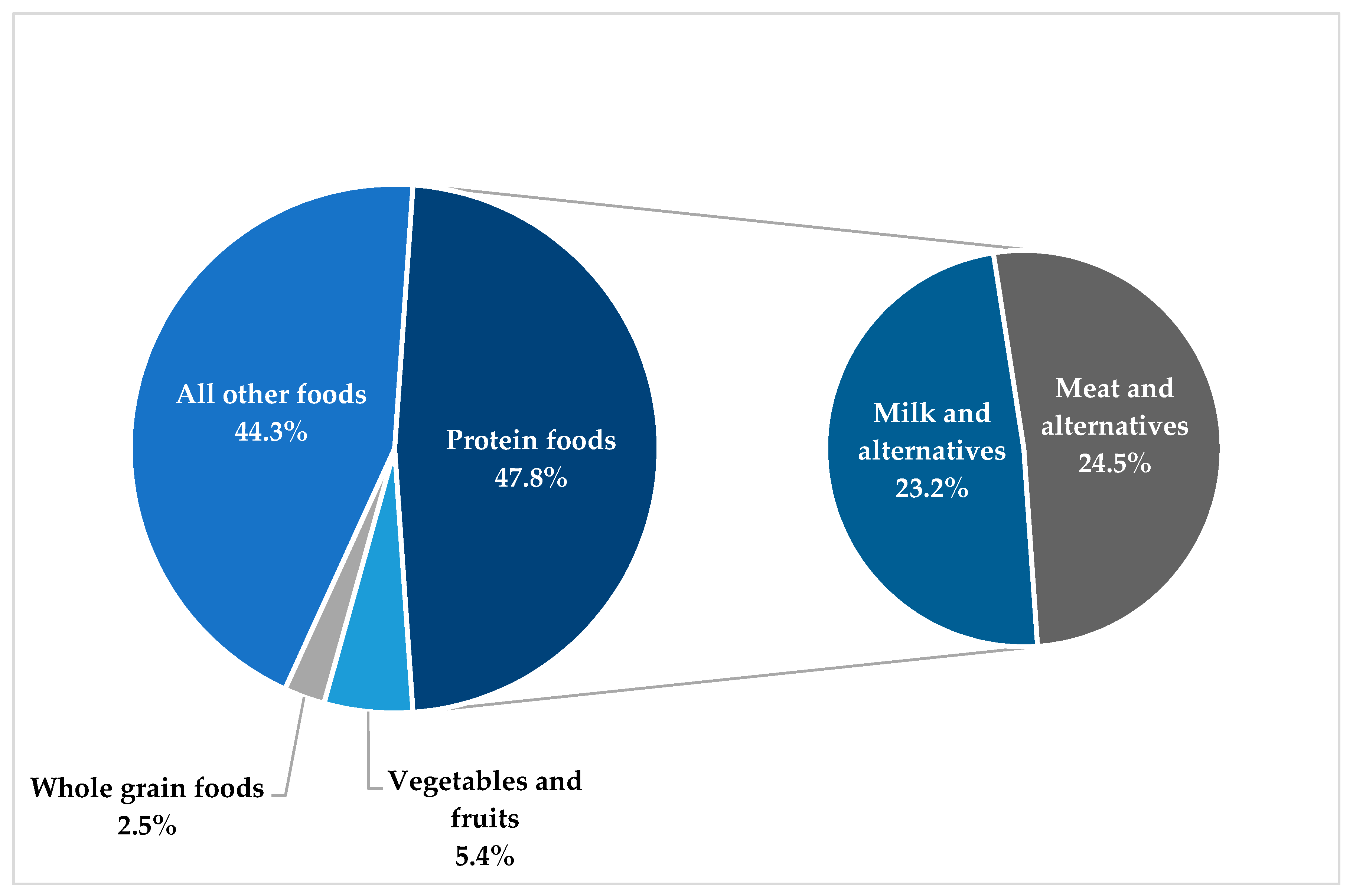
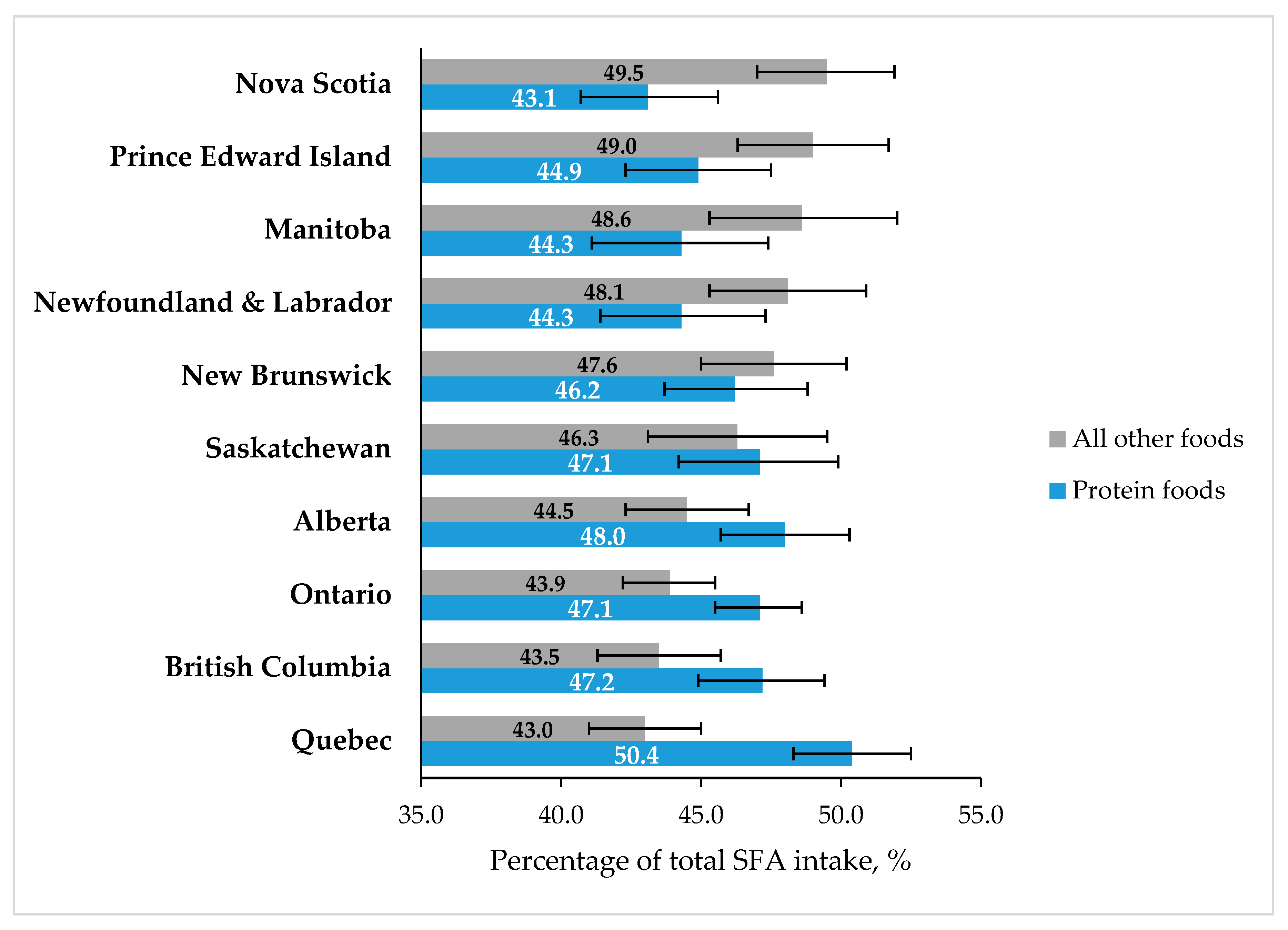
4.2. Contribution of 2019 CFG Food Categories to Total Saturated Fatty Acids Intake
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mensink, R.P.; Zock, P.L.; Kester, A.D.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: A meta-analysis of 60 controlled trials. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Martin, N.; Abdelhamid, A.; Davey Smith, G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst. Rev. 2015, 6, Cd011737. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A.; Bertram, H.C.; Bonjour, J.P.; De Groot, L.C.; de Oliveira Otto, M.C.; Feeney, E.L.; Garg, M.L.; Givens, I.; Kok, F.J.; Krauss, R.M.; et al. WHO draft guidelines on dietary saturated and trans fatty acids: Time for a new approach? BMJ (Clin. Res. Ed.) 2019, 366, l4137. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Otto, M.C.; Mozaffarian, D.; Kromhout, D.; Bertoni, A.G.; Sibley, C.T.; Jacobs, D.R., Jr.; Nettleton, J.A. Dietary intake of saturated fat by food source and incident cardiovascular disease: The Multi-Ethnic Study of Atherosclerosis. Am. J. Clin. Nutr. 2012, 96, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.P.; Brassard, D.; Tessier-Grenier, M.; Cote, J.A.; Labonte, M.E.; Desroches, S.; Couture, P.; Lamarche, B. Systematic Review of the Association between Dairy Product Consumption and Risk of Cardiovascular-Related Clinical Outcomes. Adv. Nutr. (Bethesda Md.) 2016, 7, 1026–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Canada. Canada’s Dietary Guidelines for Health Professionals and Policy Makers; Health Canada: Ottawa, ON, Canada, 2019; p. 57. [Google Scholar]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Nutrient File; Health Canada: Ottawa, ON, Canada, 2015.
- World Health Organization. Draft Guidelines on Saturated Fatty Acid and Trans-Fatty Acid Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2018; p. 103. [Google Scholar]
- Gray-Donald, K.; Jacobs-Starkey, L.; Johnson-Down, L. Food Habits of Canadians: Reduction in Fat Intake Over a Generation. Can. J. Public Health 2000, 91, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Community Health Survey, Cycle 2.2, Nutrition (2004). Nutrient Intakes from Food: Provincial, Regional and National Summary Tables; Health Canada: Ottawa, ON, Canada, 2009; Volume 1, p. 224.
- Huth, P.J.; Fulgoni, V.L.; Keast, D.R.; Park, K.; Auestad, N. Major food sources of calories, added sugars, and saturated fat and their contribution to essential nutrient intakes in the U.S. diet: Data from the national health and nutrition examination survey (2003–2006). Nutr. J. 2013, 12, 116. [Google Scholar] [CrossRef]
- Eilander, A.; Harika, R.K.; Zock, P.L. Intake and sources of dietary fatty acids in Europe: Are current population intakes of fats aligned with dietary recommendations? Eur. J. Lipid Sci. Technol. EJLST 2015, 117, 1370–1377. [Google Scholar] [CrossRef] [Green Version]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5, e008705. [Google Scholar] [CrossRef]
- Hiza, H.A.B.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet Quality of Americans Differs by Age, Sex, Race/Ethnicity, Income, and Education Level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Nadon, S.; Godin, C.; Ferland, G. Diet Quality of Montreal-Area Adults Needs Improvement: Estimates from a Self-Administered Food Frequency Questionnaire Furnishing a Dietary Indicator Score. J. Am. Diet. Assoc. 2005, 105, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Raatz, S.K.; Conrad, Z.; Picklo, M.J.; Jahns, L. Relationship of the Reported Intakes of Fat and Fatty Acids to Body Weight in US Adults. Nutrients 2017, 9, 438. [Google Scholar] [CrossRef] [PubMed]
- Langlois, K.; Garriguet, D.; Findlay, L. Diet composition and obesity among Canadian adults. Health Rep. 2009, 20, 11–20. [Google Scholar] [PubMed]
- Department for Environment Food and Rural Affairs. Family Food 2015. Statistics; Department for Environment Food and Rural Affairs: London, UK, 2017.
- Kirkpatrick, S.I.; Raffoul, A.; Lee, K.M.; Jones, A.C. Top dietary sources of energy, sodium, sugars, and saturated fats among Canadians: Insights from the 2015 Canadian Community Health Survey. Appl. Physiol. Nutr. Metab. 2019, 44, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Tugault-Lafleur, C.N.; Black, J.L. Differences in the Quantity and Types of Foods and Beverages Consumed by Canadians between 2004 and 2015. Nutrients 2019, 11, 526. [Google Scholar] [CrossRef] [PubMed]
- Daniel, C.R.; Cross, A.J.; Koebnick, C.; Sinha, R. Trends in meat consumption in the USA. Public Health Nutr. 2011, 14, 575–583. [Google Scholar] [CrossRef]
- Nardocci, M.; Leclerc, B.S.; Louzada, M.L.; Monteiro, C.A.; Batal, M.; Moubarac, J.C. Consumption of ultra-processed foods and obesity in Canada. Can. J. Public Health = Revue Canadienne de Sante Publique 2019, 110, 4–14. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B. Prevalence and characteristics of misreporting of energy intake in US adults: NHANES 2003–2012. Br. J. Nutr. 2015, 114, 1294–1303. [Google Scholar] [CrossRef]
- Jessri, M.; Lou, W.Y.; L′Abbe, M.R. Evaluation of different methods to handle misreporting in obesity research: Evidence from the Canadian national nutrition survey. Br. J. Nutr. 2016, 115, 147–159. [Google Scholar] [CrossRef]
- National Cancer Institute. National Cancer Institute. Dietary Assessment Primer. Available online: https://dietassessmentprimer.cancer.gov (accessed on 11 July 2019).
- Garriguet, D. Accounting for misreporting when comparing energy intake across time in Canada. Health Rep. 2018, 29, 3–12. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| % of Total Energy Intake ‡ | 95% CI | p-value * | ||
|---|---|---|---|---|
| Canadian adults | 10.4 | 10.2 | 10.5 | – |
| Sex | 0.49 | |||
| Women | 10.4 | 10.2 | 10.6 | |
| Men | 10.3 | 10.1 | 10.5 | |
| Age | 0.05 | |||
| 19–30 years | 10.6 | 10.2 | 10.9 | |
| 31–50 years | 10.5 | 10.2 | 10.7 | |
| 51–70 years | 10.2 | 10.0 | 10.4 | |
| Body mass index | 0.07 | |||
| Normal | 10.3 | 10.0 | 10.5 | |
| Overweight | 10.4 | 10.1 | 10.7 | |
| Obesity | 10.8 | 10.4 | 11.2 | |
| Education level | 0.002 | |||
| High School/No diploma | 10.2 a | 10.0 | 10.4 | |
| CEGEP †/Trade certificate/college | 10.8 b | 10.6 | 11.1 | |
| University | 10.2 a | 9.9 | 10.4 | |
| Unknown | 9.3 a,b | 7.6 | 11.1 | |
| Province of residence | <0.0001 | |||
| Newfoundland & Labrador | 10.1 | 9.7 | 10.5 | |
| Prince Edward Island | 11.0 | 10.6 | 11.4 | |
| Nova Scotia | 10.9 | 10.5 | 11.3 | |
| New Brunswick | 10.8 | 10.2 | 11.3 | |
| Quebec | 10.6 | 10.2 | 11.0 | |
| Ontario | 10.2 | 10.0 | 10.5 | |
| Manitoba | 10.7 | 10.2 | 11.2 | |
| Saskatchewan | 10.5 | 9.9 | 11.1 | |
| Alberta | 10.6 | 10.2 | 11.0 | |
| British Columbia | 10.0 | 9.7 | 10.4 | |
| Vegetables and Fruits * | Whole Grain Foods | Protein Foods (All) | Milk and Alternatives | Meats and Alternatives | All Other Foods | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Women | 5.6 (5.2–6.0) | 2.7 (2.4–3.0) | 46.0 (44.8–47.1) a | 23.6 (22.6–24.6) | 22.4 (21.4–23.3) a | 45.7 (44.5–46.9) a |
| Men | 5.2 (4.8–5.6) | 2.4 (2.1–2.6) | 49.5 (48.0–50.9) b | 22.7 (21.6–23.9) | 26.7 (25.5–28.0) b | 42.8 (41.4–44.1) b |
| Age | ||||||
| 19–30 years | 5.0 (4.4–5.7) | 2.1 (1.7–2.6) a | 48.3 (46.1–50.4) | 26.4 (24.3–28.6) a | 21.8 (20.1–23.6) a | 44.5 (42.3–46.7) |
| 31–50 years | 5.6 (5.1–6.1) | 2.5 (2.1–2.8) a,b | 47.9 (46.5–49.4) | 22.8 (21.6–24.0) b | 25.2 (23.9–26.4) b | 43.9 (42.4–45.4) |
| 51–70 years | 5.3 (4.9–5.7) | 2.8 (2.4–3.2) b | 47.1 (45.9–48.4) | 22.0 (20.9–23.1) b | 25.2 (24.0–26.3) b | 44.4 (43.2–45.7) |
| BMI | ||||||
| Normal (<25 kg/m2) | 5.1 (4.5–5.7) | 2.8 (2.3–3.2) | 46.3 (44.4–48.3) | 27.7 (21.1–24.4) | 23.6 (22.1–25.0) | 45.7 (43.8–47.7) |
| Overweight (25–30 kg/m2) | 5.2 (4.7–5.7) | 2.5 (2.0–3.0) | 48.7 (46.9–50.5) | 23.9 (22.4–25.4) | 24.8 (22.9–26.7) | 43.6 (41.9–45.3) |
| Obesity (≥30 kg/m2) | 5.8 (5.1–6.5) | 2.2 (1.7–2.6) | 46.9 (44.7–49.0) | 22.2 (20.5–23.9) | 24.7 (23.0–26.4) | 45.1 (42.9–47.3) |
| Education level | ||||||
| High School/No diploma | 4.8 (4.4–5.3) | 2.6 (2.2–2.9) a | 47.0 (45.6–48.4) | 22.5 (21.2–23.7) | 24.5 (23.2–25.9) | 45.5 (44.0–47.0) |
| CEGEP †/Trade certificate/College | 5.6 (5.0–6.1) | 1.8 (1.6–2.1) b | 48.7 (47.0–50.4) | 23.6 (22.2–25.1) | 25.1 (23.8–26.4) | 43.8 (42.1–45.5) |
| University | 5.7 (5.2–6.3) | 3.2 (2.7–3.6) a | 47.6 (46.0–49.2) | 23.6 (22.2–24.9) | 24.1 (22.6–25.5) | 43.4 (41.8–44.9) |
| Unknown | 7.2 (3.7–1.1) | 1.4 (0.7–2.1) b,c | 44.0 (36.3–51.8) | 18.2 (11.1–25.3) | 25.8 (19.7–31.9) | 47.4 (38.7–56.1) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harrison, S.; Brassard, D.; Lemieux, S.; Lamarche, B. Consumption and Sources of Saturated Fatty Acids According to the 2019 Canada Food Guide: Data from the 2015 Canadian Community Health Survey. Nutrients 2019, 11, 1964. https://doi.org/10.3390/nu11091964
Harrison S, Brassard D, Lemieux S, Lamarche B. Consumption and Sources of Saturated Fatty Acids According to the 2019 Canada Food Guide: Data from the 2015 Canadian Community Health Survey. Nutrients. 2019; 11(9):1964. https://doi.org/10.3390/nu11091964
Chicago/Turabian StyleHarrison, Stéphanie, Didier Brassard, Simone Lemieux, and Benoît Lamarche. 2019. "Consumption and Sources of Saturated Fatty Acids According to the 2019 Canada Food Guide: Data from the 2015 Canadian Community Health Survey" Nutrients 11, no. 9: 1964. https://doi.org/10.3390/nu11091964
APA StyleHarrison, S., Brassard, D., Lemieux, S., & Lamarche, B. (2019). Consumption and Sources of Saturated Fatty Acids According to the 2019 Canada Food Guide: Data from the 2015 Canadian Community Health Survey. Nutrients, 11(9), 1964. https://doi.org/10.3390/nu11091964