Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
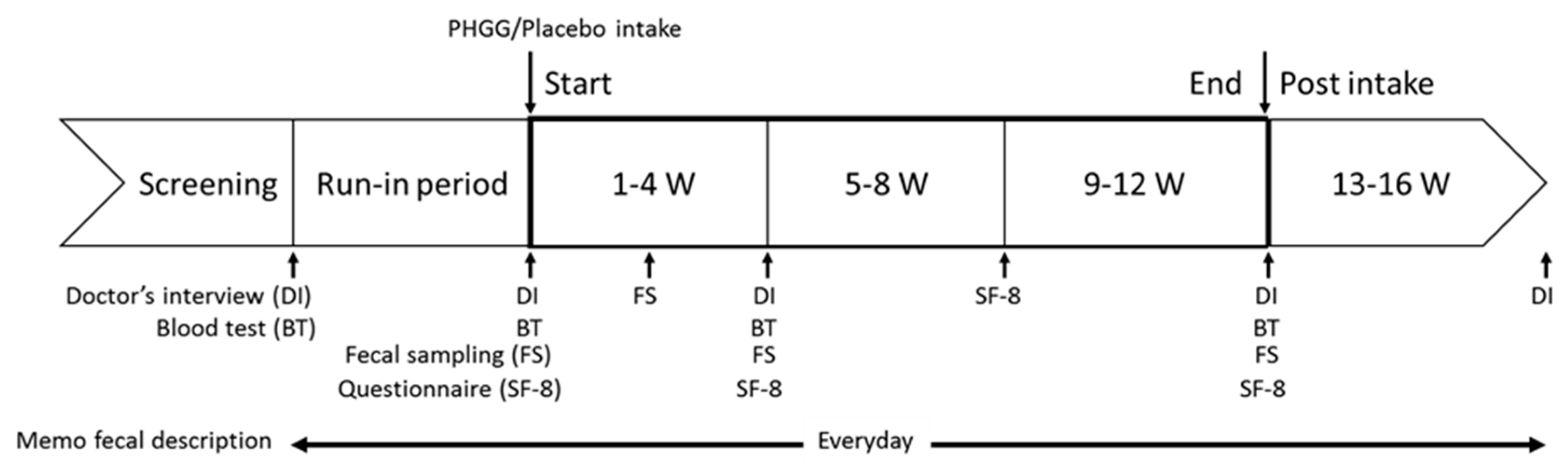
2.1. Study Design
2.2. Ethical Approval of the Study Protocol
2.3. Study Products
2.4. Subjects
2.5. Randomization
2.6. Blinding
2.7. Study Protocol
2.8. Data Collection
2.9. Fecal Sample Collection and DNA Extraction
2.10. Sequencing of 16S rRNA Gene
2.11. Microbiome Analysis
2.12. Safety Assessment
2.13. Sample Size
2.14. Statistical Analysis
3. Results
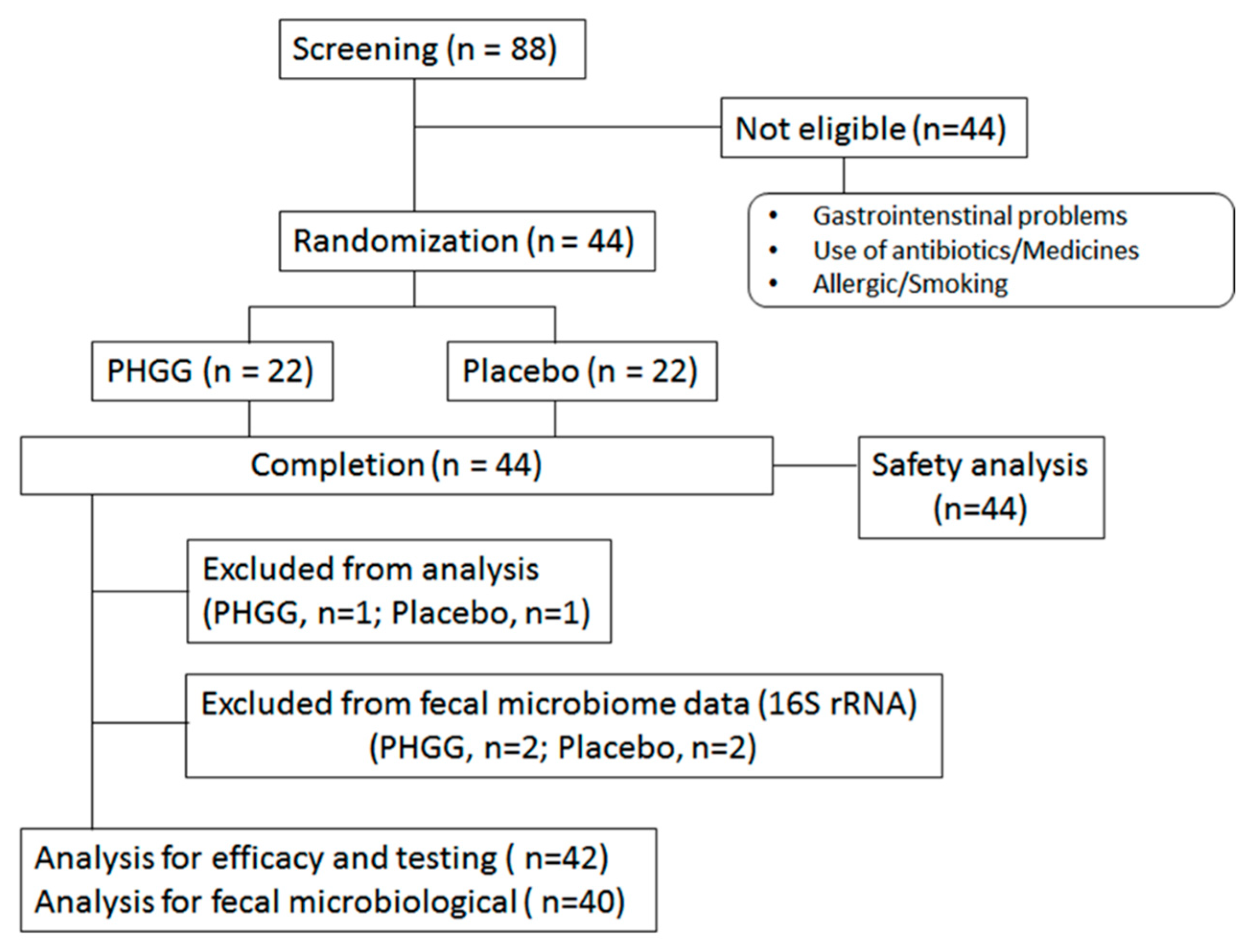
3.1. Subjects and Compliance
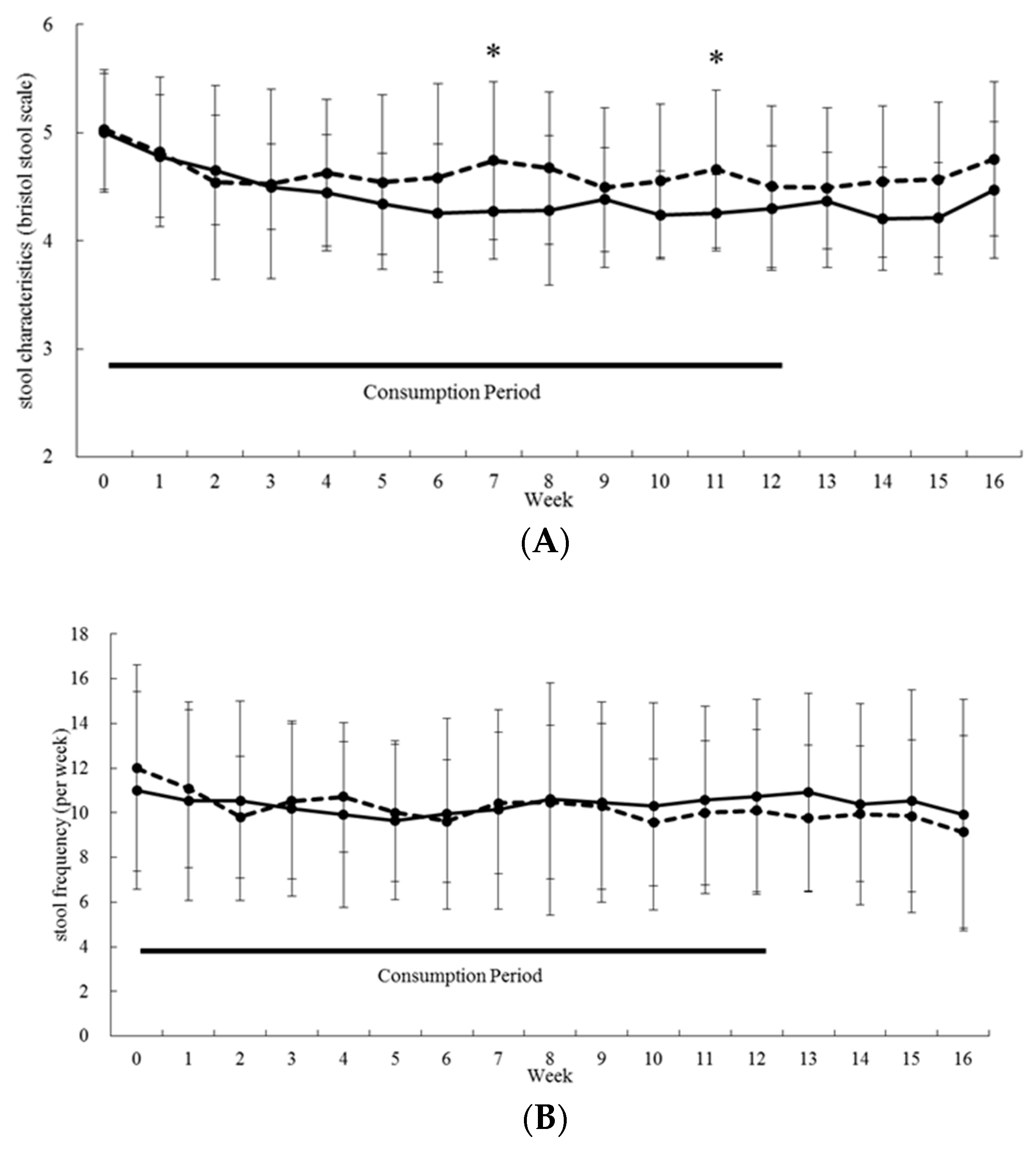
3.2. Gastrointestinal-Related Function
3.3. Quality of Life
3.4. Fecal Microbiological and Serum Bile Acid Analysis
3.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martin, C.R.; Osadchiy, V.; Kalani, A.; Mayer, E.A. The Brain-Gut-Microbiome Axis. Cell. Mol. Gastroenterol. Hepatol. 2018, 6, 133–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, E.A. Gut feelings: The emerging biology of gut–brain communication. Nat. Rev. Neurosci. 2011, 12, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.H.; Pothoulakis, C.; Mayer, E.A. Principles and clinical implications of the brain–gut–enteric microbiota axis. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Park, A.J.; Collins, J.; Blennerhassett, P.A.; Ghia, J.E.; Verdu, E.F.; Bercik, P.; Collins, S.M. Altered colonic function and microbiota profile in a mouse model of chronic depression. Neurogastroenterol. Motil. 2013, 25, 733-e575. [Google Scholar] [CrossRef] [PubMed]
- Vuong, H.E.; Hsiao, E.Y. Emerging roles for the gut microbiome in autism spectrum disorder. Biol. Psychiatry 2017, 81, 411–423. [Google Scholar] [PubMed]
- Sampson, T.R.; Debelius, J.W.; Thron, T.; Janssen, S.; Gauri, G.; Ilhan, Z.E.; Challis, C.; Schretter, C.E.; Rocha, S.; Gradinaru, V.; et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell 2017, 167, 1469–1480. [Google Scholar] [CrossRef] [PubMed]
- Berer, K.; Mues, M.; Koutrolos, M.; Al Rasbi, Z.; Boziki, M.; Johner, C.; Wekerle, H.; Krishnamoorthy, G. Commensal microbiota and myelin autoantigen cooperate to trigger autoimmune demyelination. Nature 2011, 479, 538–541. [Google Scholar] [CrossRef]
- Amaral, F.A.; Sachs, D.; Costa, V.V.; Fagundes, C.T.; Cisalpino, D.; Cunha, T.M.; Ferreira, S.H.; Cunha, F.Q.; Silva, T.A.; Nicoli, J.R.; et al. Commensal microbiota is fundamental for the development of inflammatory pain. Proc. Natl. Acad. Sci. USA 2008, 105, 2193–2197. [Google Scholar] [CrossRef] [Green Version]
- Hvas, C.L.; Ott, P.; Paine, P.; Lal, S.; Jørgensen, S.P.; Dahlerup, J.F. Obeticholic acid for severe bile acid diarrhea with intestinal failure: A case report and review of the literature. World J. Gastroenterol. 2018, 24, 2320. [Google Scholar] [CrossRef]
- Krogsgaard, L.R.; Engsbro, A.L.; Bytzer, P. The epidemiology of irritable bowel syndrome in Denmark. A population-based survey in adults ≤50 years of age. Scand. J. Gastroenterol. 2013, 48, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Tinmouth, J.; Rueda, S.; Cooper, C.; Rachlis, A.; O’Neill, T.J.; Raboud, J.M.; Rourke, S.B.; A Hart, T.; Burchell, A.N. Gastrointestinal Symptom Distress is Associated with Worse Mental and Physical Health Related Quality of Life. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 75, 67–76. [Google Scholar]
- Cai, J.; Zhao, C.; Du, Y.; Zhang, Y.; Zhao, M.; Zhao, Q. Comparative efficacy and tolerability of probiotics for antibiotic-associated diarrhea: Systematic review with network meta-analysis. United Eur. Gastroenterol. J. 2018, 6, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Borbély, Y.M.; Osterwalder, A.; Kröll, D.; Nett, P.C.; A Inglin, R. Diarrhea after bariatric procedures: Diagnosis and therapy. World J. Gastroenterol. 2017, 23, 4689. [Google Scholar] [CrossRef] [PubMed]
- Lucak, S.; Chang, L.; Halpert, A.; Harris, L.A. Current and emergent pharmacologic treatments for irritable bowel syndrome with diarrhea: Evidence-based treatment in practice. Therap. Adv. Gastroenterol. 2017, 10, 253–275. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Forsyth, C.B.; Keshavarzian, A. New molecular insights into inflammatory bowel disease-induced diarrhea. Expert Rev. Gastroenterol. Hepatol. 2011, 5, 615–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, T.; Naito, Y.; Inoue, R.; Kashiwagi, S.; Uchiyama, K.; Mizushima, K.; Tsuchiya, S.; Dohi, O.; Yoshida, N.; Kamada, K.; et al. Differences in gut microbiota associated with age, sex, and stool consistency in healthy Japanese subjects. J. Gastroenterol. 2018, 54, 53–63. [Google Scholar] [CrossRef]
- Makki, K.; Deehan, E.C.; Walter, J.; Bäckhed, F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe 2018, 23, 705–715. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, M.P.; Sugita, M.; Fukuzawa, Y.; Okubo, T. Impact of partially hydrolyzed guar gum (PHGG) on constipation prevention: A systematic review and meta-analysis. J. Funct. Foods 2017, 33, 52–66. [Google Scholar] [CrossRef]
- Yurrita, L.C.; Martín, I.S.M.; Ciudad-Cabañas, M.J.; Calle-Purón, M.E.; Cabria, M.H. Eficacia de la ingesta de inulina sobre los indicadores del estreñimiento crónico; un meta-análisis de ensayos clínicos aleatorizados controlados. Nutr. Hosp. 2014, 30, 244–252. [Google Scholar]
- Watanabe, N.; Suzuki, M.; Yamaguchi, Y.; Egashira, Y. Effects of resistant maltodextrin on bowel movements: A systematic review and meta-analysis. Clin. Exp. Gastroenterol. 2018, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Ishihara, N.; Takahashi, H.; Fujisawa, T.; Kim, M.; Yamamoto, T.; Mitsuoka, T. Effects of Partially Hydrolyzed Guar Gum Intake on Human Intestinal Microflora and Its Metabolism. Biosci. Biotechnol. Biochem. 1994, 58, 1364–1369. [Google Scholar] [CrossRef] [Green Version]
- Ohashi, Y.; Harada, K.; Tokunaga, M.; Ishihara, N.; Okubo, T.; Ogasawara, Y.; Juneja, L.R.; Fujisawa, T. Faecal fermentation of partially hydrolyzed guar gum. J. Funct. Foods 2012, 4, 398–402. [Google Scholar] [CrossRef]
- Pylkas, A.M.; Juneja, L.R.; Slavin, J.L. Comparison of Different Fiber for in Vitro Production of Short Chain Fatty Acids by Intestinal Microflore.pdf. J. Med. Food. 2005, 8, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Velázquez, M.; Davies, C.; Marett, R.; Slavin, J.L.; Feirtag, J.M. Effect of Oligosaccharides and Fibre Substitutes on Short-chain Fatty Acid Production by Human Faecal Microflora. Anaerobe 2000, 6, 87–92. [Google Scholar] [CrossRef]
- Tokunaga, M.; Yasukawa, Z.; Ozeki, M.; Saito, J. Effect of partially hydrolyzed guar gum on postprandial hyperglycemia. Jpn. Pharmacol. Ther. 2016, 44, 227–235. [Google Scholar]
- Trinidad, T.; Perez, E.; Loyola, A.; Mallillin, A.; Encabo, R.; Yokawa, T.; Aoyama, N.; Juneja, L. Glycemic index of Sunfibre (Cyamoposis tetragonolobus) products in normal and diabetic subjects. Int. J. Food Sci. Technol. 2004, 39, 1093–1098. [Google Scholar] [CrossRef]
- Kajimoto, O.; Xiao, J.; Kondo, S.; Iwatsuki, K.; Kokubo, S.; Sakamoto, A.; Kajimoto, Y.; Togashi, H.; Hirata, H. Suppression of postprandial serum triglyceride elevation by a drinking yogurt supplemented with partially hydrolyzed guar gum. J. Nutr. Food Sci. 2004, 7, 1–17. [Google Scholar]
- Kondo, S.; Xiao, J.-Z.; Takahashi, N.; Miyaji, K.; Iwatsuki, K.; Kokubo, S. Suppressive Effects of Dietary Fiber in Yogurt on the Postprandial Serum Lipid Levels in Healthy Adult Male Volunteers. Biosci. Biotechnol. Biochem. 2004, 68, 1135–1138. [Google Scholar] [CrossRef]
- Rao, T.P.; Hayakawa, M.; Minami, T.; Ishihara, N.; Kapoor, M.P.; Ohkubo, T.; Juneja, L.R.; Wakabayashi, K. Post-meal perceivable satiety and subsequent energy intake with intake of partially hydrolysed guar gum. Br. J. Nutr. 2015, 113, 1489–1498. [Google Scholar] [CrossRef] [Green Version]
- Homann, H.-H.; Kemen, M.; Fuessenich, C.; Senkal, M.; Zumtobel, V. Reduction in Diarrhea Incidence by Soluble Fiber in Patients Receiving Total or Supplemental Enteral Nutrition. J. Parenter. Enter. Nutr. 1994, 18, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Rushdi, T.A.; Pichard, C.; Khater, Y.H. Control of diarrhea by fiber-enriched diet in ICU patients on enteral nutrition: A prospective randomized controlled trial. Clin. Nutr. 2004, 23, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.H.; Meier, R.; Schneider, H.; Sarker, S.A.; Bardhan, P.K.; Mahalanabis, D.; Fuchs, G.J.; Gyr, N. Partially Hydrolyzed Guar Gum–Supplemented Oral Rehydration Solution in the Treatment of Acute Diarrhea in Children. J. Pediatr. Gastroenterol. Nutr. 2000, 31, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.H.; Meier, R.; Sarker, S.; Bardhan, P.K.; Schneider, H.; Gyr, N. Partially hydrolysed guar gum supplemented comminuted chicken diet in persistent diarrhoea: A randomised controlled trial. Arch. Dis. Child. 2005, 90, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S.; Hongo, R.; Moji, K.; Oku, T. Suppressive effect of partially hydrolyzed guar gum on transitory diarrhea induced by ingestion of maltitol and lactitol in healthy humans. Eur. J. Clin. Nutr. 2007, 61, 1086–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, L.; Slavin, J.L. Dietary Fiber and Other Alternative Therapies and Irritable Bowel Syndrome. Top. Clin. Nutr. 2009, 24, 262–271. [Google Scholar] [CrossRef]
- Higashimura, Y.; Naito, Y.; Takagi, T.; Uchiyama, K.; Mizushima, K.; Ushiroda, C.; Ohnogi, H.; Kudo, Y.; Yasui, M.; Inui, S.; et al. Protective effect of agaro-oligosaccharides on gut dysbiosis and colon tumorigenesis in high-fat diet-fed mice. Am. J. Physiol. Liver Physiol. 2016, 310, G367–G375. [Google Scholar] [CrossRef]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing Items on the SF-8 Japanese Version for Health-Related Quality of Life: A Psychometric Analysis Based on the Nominal Categories Model of Item Response Theory. Value Heal. 2009, 12, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Inoue, R.; Ohue-Kitano, R.; Tsukahara, T.; Tanaka, M.; Masuda, S.; Inoue, T.; Yamakage, H.; Kusakabe, T.; Hasegawa, K.; Shimatsu, A.; et al. Prediction of functional profiles of gut microbiota from 16S rRNA metagenomic data provides a more robust evaluation of gut dysbiosis occurring in Japanese type 2 diabetic patients. J. Clin. Biochem. Nutr. 2017, 61, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Roberfroid, M.B. Prebiotics and probiotics: Are they functional foods? Am. J. Clin. Nutr. 2000, 71, 1682S–1687S. [Google Scholar] [CrossRef]
- Shah, E.; Pimentel, M. Evaluating the functional net value of pharmacologic agents in treating irritable bowel syndrome. Aliment. Pharmacol. Ther. 2014, 39, 973–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Tito, R.Y.; Joossens, M.; Raes, J. Stool consistency is strongly associated with gut microbiota richness and composition, enterotypes and bacterial growth rates. Gut 2016, 65, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Hotta, M.; Sato, Y.; Iwata, S.; Yamashita, N.; Sunakawa, K.; Oikawa, T.; Tanaka, R.; Watanabe, K.; Takayama, H.; Yajima, M.; et al. Clinical Effects of Bifidobacterium Preparations Intractable Diarrhea. Keio J. Med. 1987, 36, 298–314. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.-B.; Jiang, R.-H.; Sheng, H.-B. Meta-analysis of the effects of Bifidobacterium preparations for the prevention and treatment of pediatric antibiotic-associated diarrhea in China. Complement. Ther. Med. 2017, 33, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Wick, E.C.; Sears, C.L. Bacteroides spp. and diarrhea. Curr. Opin. Infect. Dis. 2010, 23, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Shukla, R.; Ghoshal, U.; Dhole, T.N.; Ghoshal, U.C. Fecal Microbiota in Patients with Irritable Bowel Syndrome Compared with Healthy Controls Using Real-Time Polymerase Chain Reaction: An Evidence of Dysbiosis. Dig. Dis. Sci. 2015, 60, 2953–2962. [Google Scholar] [CrossRef] [PubMed]
- Carroll, I.M.; Chang, Y.-H.; Park, J.; Sartor, R.B.; Ringel, Y. Luminal and mucosal-associated intestinal microbiota in patients with diarrhea-predominant irritable bowel syndrome. Gut Pathog. 2010, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Giaccari, S.; Grasso, G.; Tronci, S.; Allegretta, L.; Sponziello, G.; Montefusco, A.; Siciliano, I.G.; Guarisco, R.; Candiani, C.; Chiri, S. [Partially hydrolyzed guar gum: A fiber as coadjuvant in the irritable colon syndrome]. La Clin. Ter. 2001, 152, 21–25. [Google Scholar]
- Parisi, G.; Zilli, M.; Miani, M.; Carrara, M.; Bottona, E.; Verdianelli, G.; Battaglia, G.; Desideri, S.; Faedo, A.; Marzolino, C.; et al. High-Fiber Diet Supplementation in Patients with Irritable Bowel Syndrome (IBS): A Multicenter, Randomized, Open Trial Comparison Between Wheat Bran Diet and Partially Hydrolyzed Guar Gum (PHGG). Dig. Dis. Sci. 2002, 47, 1697–1704. [Google Scholar] [CrossRef]
- Parisi, G.; Bottona, E.; Carrara, M.; Cardin, F.; Faedo, A.; Goldin, D.; Marino, M.; Zilli, M.; Leandro, G. Treatment Effects of Partially Hydrolyzed Guar Gum on Symptoms and Quality of Life of Patients with Irritable Bowel Syndrome. A Multicenter Randomized Open Trial. Dig. Dis. Sci. 2005, 50, 1107–1112. [Google Scholar] [CrossRef]
- Ohashi, Y.; Sumitani, K.; Tokunaga, M.; Ishihara, N.; Okubo, T.; Fujisawa, T. Consumption of partially hydrolysed guar gum stimulates Bifidobacteria and butyrate-producing bacteria in the human large intestine. Benef. Microbes 2015, 6, 451–455. [Google Scholar] [CrossRef]
- Inoue, R.; Sakaue, Y.; Kawada, Y.; Tamaki, R.; Yasukawa, Z.; Ozeki, M.; Ueba, S.; Sawai, C.; Nonomura, K.; Tsukahara, T.; et al. Dietary supplementation with partially hydrolyzed guar gum helps improve constipation and gut dysbiosis symptoms and behavioral irritability in children with autism spectrum disorder. J. Clin. Biochem. Nutr. 2019, 64, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Slavin, J. Fiber and Prebiotics: Mechanisms and Health Benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, H.M.; Jonkers, D.; Venema, K.; Vanhoutvin, S.; Troost, F.J.; Brummer, R.J. The role of butyrate on colonic function. Aliment. Pharmacol. Ther. 2008, 27, 104–119. [Google Scholar]
- Menees, S.; Saad, R.; Chey, W.D. Agents that act luminally to treat diarrhoea and constipation. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 661–674. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | PHGG | Placebo | p Value | |
|---|---|---|---|---|
| Number of subjects (male; female) | 44 (22; 22) | 22 (11; 11) | 22 (11; 11) | |
| Age (years) | 41.9 ± 6.3 | 41.8 ± 7.0 | 42.1 ± 5.6 | 0.906 |
| Height (cm) | 166.7 ± 8.4 | 167.0 ± 6.2 | 166.3 ± 10.3 | 0.773 |
| Weight (kg) | 62.7 ± 10.9 | 63.4 ± 8.2 | 62.0 ± 13.2 | 0.685 |
| BMI (kg m−2) | 22.4 ± 2.5 | 22.7 ± 2.5 | 22.2 ± 2.6 | 0.511 |
| Systolic blood pressure (mmHg) | 109.5 ± 11.3 | 110.3 ± 11.2 | 108.6 ± 11.6 | 0.636 |
| Diastolic blood pressure (mmHg) | 64.3 ± 9.5 | 64.1 ± 9.1 | 64.6 ± 10.1 | 0.876 |
| Pulse (per minute) | 69.7 ± 9.1 | 69.8 ± 8.5 | 69.7 ± 10.0 | 0.974 |
| Waist circumference (cm) | 80.6 ± 8.1 | 81.6 ± 6.5 | 79.7 ± 9.5 | 0.446 |
| Physical Component Summary | Mental Component Summary | |||
|---|---|---|---|---|
| PHGG | Placebo | PHGG | Placebo | |
| Baseline (0 W) | 50.65 ± 4.82 | 51.77 ± 4.56 | 50.87 ± 4.94 | 48.61 ± 7.52 |
| p = 0.443 | p = 0.257 | |||
| Intake period 1 (4 W) | 52.41 ± 4.34 | 52.79 ± 4.44 | 50.89 ± 4.65 | 47.15 ± 7.96 |
| p = 0.782 | p = 0.072 | |||
| Intake period 2 (8 W) | 51.13 ± 4.29 | 51.27 ± 5.03 | 51.53 ± 4.38 | 48.19 ± 8.54 |
| p = 0.920 | p = 0.121 | |||
| Intake period 3 (12 W) | 51.59 ± 3.88 | 52.12 ± 4.75 | 50.89 ± 3.64 | 47.84 ± 9.46 |
| p = 0.692 | p = 0.179 | |||
| Phylum | Class | Oder | Family | Genus | Group | Consumption Period (Week) | |||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 2 | 4 | 12 | ||||||
| Actinobacteria | Actinobacteria | Bifidobacteriales | Bifidobacteriaceae | Bifidobacterium | Placebo | 8.82% ± 7.94% | 5.65% ± 5.17% | 7.14% ± 6.42% | 7.98% ± 7.27% |
| PHGG | 8.02% ± 6.35% | 12.24% ± 8.54% | 10.96% ± 8.15% | 11.40% ± 10.45% | |||||
| Bacteroidetes | Bacteroidia | Bacteroidales | Bacteroidaceae | Bacteroides | Placebo | 16.56% ± 9.82% | 16.23% ± 8.94% | 18.99% ± 10.35% | 16.96% ± 10.55% |
| PHGG | 13.21% ± 7.69% | 12.93% ± 6.16% | 13.12% ± 8.80% | 14.85% ± 9.23% | |||||
| Firmicutes | Bacilli | Lactobacillales | Streptococcaceae | Streptococcus | Placebo | 0.46% ± 0.40% | 0.47% ± 0.31% | 0.82% ± 0.91% | 0.54% ± 0.95% |
| PHGG | 0.61% ± 0.47% | 0.92% ± 1.44% | 1.17% ± 1.65% | 1.60% ± 2.17% | |||||
| Firmicutes | Clostridia | Clostridiales | Clostridiaceae | Clostridium | Placebo | 0.74% ± 0.95% | 0.58% ± 0.56% | 1.24% ± 3.15% | 0.58% ± 0.62% |
| PHGG | 0.38% ± 0.44% | 0.27% ± 0.23% | 0.24% ± 0.26% | 0.22% ± 0.22% | |||||
| Firmicutes | Clostridia | Clostridiales | Lachnospiraceae | Unclassified | Placebo | 6.41% ± 2.65% | 7.56% ± 3.87% | 6.76% ± 4.02% | 6.54% ± 2.22% |
| PHGG | 5.56% ± 2.87% | 4.96% ± 2.55% | 5.26%± 3.03% | 4.91% ± 2.85% | |||||
| Firmicutes | Clostridia | Clostridiales | Lachnospiraceae | [Ruminococcus] | Placebo | 3.84% ± 3.58% | 4.02% ± 3.22% | 4.57% ± 5.72% | 3.71% ± 2.76% |
| PHGG | 2.93% ± 2.29% | 3.08% ± 3.49% | 2.57% ± 1.72% | 2.35% ± 1.57% | |||||
| Firmicutes | Clostridia | Clostridiales | Ruminococcaceae | Ruminococcus | Placebo | 2.45% ± 2.64% | 2.39% ± 3.18% | 1.97% ±3.02% | 2.53% ± 2.98% |
| PHGG | 4.05% ± 4.06% | 3.08% ± 4.40% | 4.43% ± 4.94% | 3.77% ± 4.86% | |||||
| Firmicutes | Clostridia | Clostridiales | Veillonellaceae | Megasphaera | Placebo | 0.74% ± 2.34% | 0.54% ± 1.68% | 0.89% ± 2.77% | 0.90% ± 3.66% |
| PHGG | 2.52% ± 3.70% | 2.97% ± 3.65% | 3.41% ± 4.89% | 3.75% ± 4.94% | |||||
| Firmicutes | Clostridia | Clostridiales | Veillonellaceae | Phascolarctobacterium | Placebo | 3.36% ± 2.96% | 4.85% ± 4.38% | 3.23% ± 2.77% | 4.13% ± 4.18% |
| PHGG | 2.18% ± 2.29% | 3.06% ± 3.22% | 1.94% ± 2.05% | 2.20% ± 2.63% | |||||
| PHGG (n = 21) | Placebo (n = 21) | ||||||
|---|---|---|---|---|---|---|---|
| Outcome | Initial | Final | Within Group p Value | Initial | Final | Within Group p Value | Between Groups p Value |
| Bile Acids Primary | |||||||
| CA % | 8.29 ± 4.96 | 8.63 ± 5.34 | 0.71 | 7.82 ± 5.30 | 8.79 ± 6.77 | 0.41 | 0.94 |
| CDCA % | 11.21 ± 10.71 | 13.11 ± 12.02 | 0.37 | 7.39 ± 6.03 | 10.92 ± 8.57 | 0.05 | 0.51 |
| Bile Acids Secondary | |||||||
| DCA % | 16.79 ± 11.41 | 13.74 ± 12.38 | 0.23 | 14.20 ± 10.64 | 14.37 ± 11.03 | 0.92 | 0.87 |
| LCA % | 1.34 ± 0.91 | 1.25 ± 1.24 | 0.70 | 1.40 ± 1.17 | 1.19 ± 0.96 | 0.27 | 0.85 |
| DCA/(CA+DCA) | 0.6081 ± 0.2343 | 0.5108 ± 0.2685 | 0.03* | 0.5798 ± 0.2370 | 0.5771 ± 0.2596 | 0.91 | 0.43 |
| LCA/(CDCA+LCA) | 0.2009 ± 0.1982 | 0.1840 ± 0.2354 | 0.71 | 0.2301 ± 0.2345 | 0.1762 ± 0.2072 | 0.29 | 0.91 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasukawa, Z.; Inoue, R.; Ozeki, M.; Okubo, T.; Takagi, T.; Honda, A.; Naito, Y. Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial. Nutrients 2019, 11, 2170. https://doi.org/10.3390/nu11092170
Yasukawa Z, Inoue R, Ozeki M, Okubo T, Takagi T, Honda A, Naito Y. Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial. Nutrients. 2019; 11(9):2170. https://doi.org/10.3390/nu11092170
Chicago/Turabian StyleYasukawa, Zenta, Ryo Inoue, Makoto Ozeki, Tsutomu Okubo, Tomohisa Takagi, Akira Honda, and Yuji Naito. 2019. "Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial" Nutrients 11, no. 9: 2170. https://doi.org/10.3390/nu11092170
APA StyleYasukawa, Z., Inoue, R., Ozeki, M., Okubo, T., Takagi, T., Honda, A., & Naito, Y. (2019). Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial. Nutrients, 11(9), 2170. https://doi.org/10.3390/nu11092170