Different Associations of Socioeconomic Status on Protein Intake in the Korean Elderly Population: A Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Household Income and Education Attainment
2.3. Measurement of Protein Intake
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Characteristics of Study Population According to Protein Intake
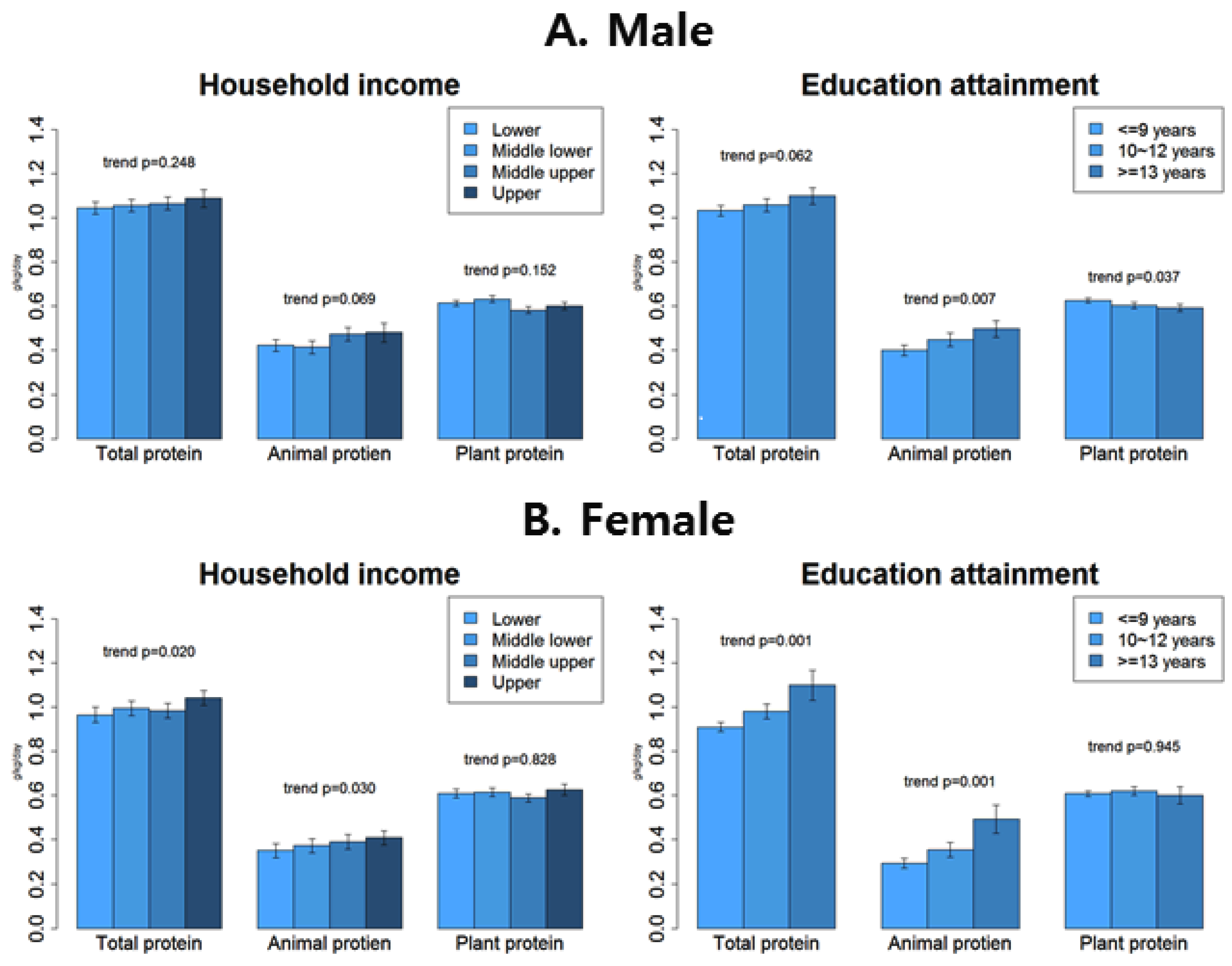
3.3. Total Protein Intake, Animal Protein Intake, and Plant Protein Intake by SES
3.4. Protein Intake Adequacy by SES
4. Discussion
4.1. Differential Influences of SES Status on Animal and Plant Protein
4.2. Mechanisms of SES Affect Protein Intake
4.3. Recommended Protein Intake for Korean Elderly People
4.4. Limitation and Strength
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Malaguarnera, M.; Vacante, M.; Frazzetto, P.M.; Motta, M. What is the frailty in elderly? Value and significance of the multidimensional assessments. Arch. Gerontol. Geriatr. 2013, 56, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Lally, F.; Crome, P. Understanding frailty. Postgrad. Med. J. 2007, 83, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Walrand, S.; Guillet, C.; Salles, J.; Cano, N.; Boirie, Y. Physiopathological mechanism of sarcopenia. Clin. Geriatr. Med. 2011, 27, 365–385. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Kritchevsky, S.B.; Newman, A.B.; Taaffe, D.R.; Nicklas, B.J.; Visser, M.; Lee, J.S.; Nevitt, M.; Tylavsky, F.A.; Rubin, S.M.; et al. Effects of birth cohort and age on body composition in a sample of community-based elderly. Am. J. Clin. Nutr. 2007, 85, 405–410. [Google Scholar]
- Coelho-Júnior, H.J.; Rodrigues, B.; Uchida, M.; Marzetti, E. Low protein intake is associated with frailty in older adults: A systematic review and meta-analysis of observational studies. Nutrients 2018, 10, 1334. [Google Scholar] [CrossRef] [Green Version]
- Beasley, J.M.; LaCroix, A.Z.; Neuhouser, M.L.; Huang, Y.; Tinker, L.; Woods, N.; Michael, Y.; Curb, J.D.; Prentice, R.L. Protein intake and incident frailty in the Women’s Health Initiative observational study. J. Am. Geriatr. Soc. 2010, 58, 1063–1071. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, J.; Ellison, R.C.; Singer, M.R.; Bradlee, M.L.; Kalesan, B.; Holick, M.F.; Moore, L.L. Dietary protein and preservation of physical functioning among middle-aged and older adults in the Framingham Offspring Study. Am. J. Epidemiol. 2018, 187, 1411–1419. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Argiles, J.M.; Evans, W.J.; Bhasin, S.; Cella, D.; Deutz, N.E.; Doehner, W.; Fearon, K.C.; Ferrucci, L.; Hellerstein, M.K.; et al. Nutritional recommendations for the management of sarcopenia. J. Am. Med. Dir. Assoc. 2010, 11, 391–396. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare. Dietary Reference Intakes for Koreans 2015 Sejong: Ministry of Health and Welfare; Korea Nutrition Society: Sejong, Korea, 2015.
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Jung, H.W.; Kim, S.W.; Kim, I.Y.; Lim, J.Y.; Park, H.S.; Song, W.; Yoo, H.J.; Jang, H.C.; Kim, K.; Park, Y.; et al. Protein Intake Recommendation for Korean Older Adults to Prevent Sarcopenia: Expert Consensus by the Korean Geriatric Society and the Korean Nutrition Society. Ann. Geriatr. Med. Res. 2018, 22, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Park, H.A. Adequacy of Protein Intake among Korean Elderly: An Analysis of the 2013–2014 Korea National Health and Nutrition Examination Survey Data. Korean J. Fam. Med. 2018, 39, 130–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, K.M.; Olstad, D.L.; Leech, R.M.; Ball, K.; Meertens, B.; Potter, J.; Cleanthous, X.; Reynolds, R.; McNaughton, S.A. Socioeconomic Inequities in Diet Quality and Nutrient Intakes among Australian Adults: Findings from a Nationally Representative Cross-Sectional Study. Nutrients 2017, 9, 1092. [Google Scholar] [CrossRef] [Green Version]
- Van Rossum, C.; Van de Mheen, H.; Witteman, J.; Grobbee, E.; Mackenbach, J. Education and nutrient intake in Dutch elderly people. The Rotterdam Study. Eur. J. Clin. Nutr. 2000, 54, 159. [Google Scholar] [CrossRef]
- Mayen, A.L.; Marques-Vidal, P.; Paccaud, F.; Bovet, P.; Stringhini, S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1520–1531. [Google Scholar] [CrossRef] [Green Version]
- Friel, S.; Kelleher, C.C.; Nolan, G.; Harrington, J. Social diversity of Irish adults nutritional intake. Eur. J. Clin. Nutr. 2003, 57, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, M.; Nakagawa, H.; Kadota, A.; Yoshita, K.; Nakamura, Y.; Okuda, N.; Nishi, N.; Miyamoto, Y.; Arima, H.; Ohkubo, T.; et al. Macronutrient Intake and Socioeconomic Status: NIPPON DATA2010. J. Epidemiol. 2018, 28, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Galobardes, B.; Morabia, A.; Bernstein, M.S. Diet and socioeconomic position: Does the use of different indicators matter? Int. J. Epidemiol. 2001, 30, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Yanagi, N.; Hata, A.; Kondo, K.; Fujiwara, T. Association between childhood socioeconomic status and fruit and vegetable intake among older Japanese: The JAGES 2010 study. Prev. Med. 2018, 106, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Si Hassen, W.; Castetbon, K.; Cardon, P.; Enaux, C.; Nicolaou, M.; Lien, N.; Terragni, L.; Holdsworth, M.; Stronks, K.; Hercberg, S.; et al. Socioeconomic indicators are independently associated with nutrient intake in French adults: A DEDIPAC study. Nutrients 2016, 8, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics 2016: Korea National Health and Nutrition Examination Survey (KNHANES VII-1); Ministry of Health and Welfare: Seoul, Korea, 2017. [Google Scholar]
- Korea agriculture and Fisheries Food Circulation Construction; National Agricultural Cooperative Federation; National Federation of Fishers Cooperatives. Agricultural Fishery and Livestock Products by Item Details Irradiation Price. Available online: https://www.data.go.kr/dataset/15012298/fileData.do (accessed on 20 August 2019).
- Korea Health Industry Development Institue. National Food & Nutrition Statistics I: Based on 2014 Korea National Health and Nutrition Examination Survey 2016; Korea Health Industry Development Institue: Cheongju, Korea, 2016. [Google Scholar]
- Turrell, G.; Kavanagh, A.M. Socio-economic pathways to diet: Modelling the association between socio-economic position and food purchasing behaviour. Public Health Nutr. 2006, 9, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilcox, S.; Sharpe, P.A.; Liese, A.D.; Dunn, C.G.; Hutto, B. Socioeconomic factors associated with diet quality and meeting dietary guidelines in disadvantaged neighborhoods in the Southeast United States. Ethn. Health 2018, 1–17. [Google Scholar] [CrossRef]
- Lin, Y.; Bolca, S.; Vandevijvere, S.; De Vriese, S.; Mouratidou, T.; De Neve, M.; Polet, A.; Van Oyen, H.; Van Camp, J.; De Backer, G. Plant and animal protein intake and its association with overweight and obesity among the Belgian population. Br. J. Nutr. 2011, 105, 1106–1116. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; Volume 40. [Google Scholar]
- Park, H.A. Rate of missing socioeconomic factors in the 4th KNHANES. Korean J. Fam. Med. 2012, 33, 406. [Google Scholar] [CrossRef] [Green Version]
- Bingham, S.A. Urine nitrogen as a biomarker for the validation of dietary protein intake. J. Nutr. 2003, 133, 921–924. [Google Scholar] [CrossRef]
- Murayama, N. Effects of socioeconomic status on nutrition in Asia and future nutrition policy studies. J. Nutr. Sci. Vitaminol. 2015, 61, 66–68. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Mean (SE) Or Proportion (SE) 1 | Male | Female | Total |
|---|---|---|---|
| 43.6 (0.8) | 56.4 (0.8) | ||
| Age (year) | 70.0 (0.2) | 70.3 (0.2) | 70.1 (0.2) |
| BMI (kg/m2) | 23.4 (0.1) | 24.4 (0.1) | 24.0 (0.1) |
| Having chronic diseases 2 (vs. none) | 62.3 (1.5) | 75.5 (1.2) | 69.7 (1.0) |
| Alcohol consumption frequency per week | |||
| 0 | 30.8 (1.3) | 60.6 (1.3) | 47.6 (1.0) |
| 1 | 38.8 (1.5) | 34.4 (1.2) | 36.3 (1.0) |
| 2≤ | 30.4 (1.4) | 5.0 (0.6) | 16.1 (0.8) |
| Smoker (vs. nonsmoker) | 24.0 (1.3) | 2.9 (0.4) | 12.1 (0.7) |
| Urban dwelling (vs. rural) | 75.9 (2.6) | 76.5 (2.5) | 76.2 (2.5) |
| Familial type | |||
| Living alone | 7.5 (0.8) | 21.9 (1.0) | 15.6 (0.8) |
| Living with spouse | 49.2 (1.6) | 29.8 (1.1) | 38.3 (1.2) |
| Living with others | 43.3 (1.6) | 48.3 (1.4) | 46.1 (1.3) |
| Household income quartiles | |||
| Lower | 37.5 (1.6) | 46.1 (1.6) | 42.3 (1.4) |
| Middle lower | 28.3 (1.4) | 27.0 (1.3) | 27.5 (1.1) |
| Middle upper | 19.3 (1.2) | 15.1 (1.0) | 17.0 (0.9) |
| Upper | 14.9 (1.2) | 11.8 (1.1) | 13.2 (1.0) |
| Educational attainment (year) | |||
| ≤9 | 59.5 (1.6) | 83.5 (1.2) | 73.0 (1.2) |
| 10–12 | 24.9 (1.3) | 11.7 (0.9) | 17.5 (0.8) |
| 13≤ | 15.6 (1.3) | 4.8 (0.6) | 9.5 (0.8) |
| Total Energy Intake, kcal/day | Total Protein Intake, (g/day) | %Energy from Protein, (%) | Protein Intake Per Weight, (g/kg/day) | Total, Animal Protein Intake, (g/kg/day) | Total Plant Protein Intake, (g/kg/day) | |
|---|---|---|---|---|---|---|
| Male | ||||||
| Total | 1986.0 (21.9) | 65.3 (1.0) | 13.1 (0.1) | 1.03 (0.02) | 0.40 (0.01) | 0.63 (0.01) |
| Household income quartiles | ||||||
| Lower | 1858.9 (27.6) | 58.7 (1.4) | 12.6 (0.2) | 0.95 (0.02) | 0.34 (0.02) | 0.61 (0.01) |
| Middle lower | 2012.4 (39.4) | 65.6 (1.6) | 13.0 (0.2) | 1.05 (0.03) | 0.38 (0.02) | 0.65 (0.02) |
| Middle upper | 2079.1 (51.5) | 70.0 (2.2) | 13.4 (0.3) | 1.09 (0.03) | 0.46 (0.03) | 0.61 (0.02) |
| Upper | 2134.7 (52.9) | 75.4 (2.8) | 14.1 (0.3) | 1.14 (0.05) | 0.49 (0.04) | 0.63 (0.02) |
| Trend p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.563 |
| Educational attainment (year) | ||||||
| ≤9 | 1929.2 (27.5) | 61.4 (1.1) | 12.7 (0.2) | 0.99 (0.02) | 0.35 (0.02) | 0.63 (0.01) |
| 10–12 | 2057.2 (39.9) | 68.8 (1.8) | 13.3 (0.2) | 1.07 (0.03) | 0.44 (0.02) | 0.63 (0.01) |
| 13≤ | 2089.0 (59.7) | 74.9 (2.8) | 14.3 (0.3) | 1.15 (0.05) | 0.51 (0.04) | 0.62 (0.02) |
| Trend p | 0.003 | <0.001 | <0.001 | <0.001 | <0.001 | 0.896 |
| Female | ||||||
| Total | 1560.9 (17.0) | 49.7 (0.7) | 12.6 (0.1) | 0.90 (0.01) | 0.29 (0.01) | 0.60 (0.01) |
| Household income quartiles | ||||||
| Lower | 1472.8 (19.7) | 45.1 (0.9) | 12.1 (0.1) | 0.83 (0.02) | 0.25 (0.01) | 0.58 (0.01) |
| Middle lower | 1547.0 (30.3) | 49.4 (1.1) | 12.8 (0.2) | 0.89 (0.02) | 0.29 (0.01) | 0.60 (0.01) |
| Middle upper | 1697.1 (46.9) | 56.0 (1.9) | 13.1 (0.3) | 0.97 (0.03) | 0.35 (0.02) | 0.62 (0.02) |
| Upper | 1762.0 (49.1) | 60.5 (2.0) | 13.6 (0.2) | 1.09 (0.04) | 0.41 (0.03) | 0.68 (0.03) |
| Trend p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Educational attainment (year) | ||||||
| ≤9 | 1527.7 (18.0) | 47.5 (0.7) | 12.4 (0.1) | 0.86 (0.01) | 0.26 (0.01) | 0.59 (0.01) |
| 10–12 | 1666.8 (38.5) | 57.4 (1.9) | 13.7 (0.3) | 1.01 (0.04) | 0.37 (0.03) | 0.64 (0.02) |
| 13≤ | 1878.2 (77.9) | 68.8 (3.8) | 14.7 (0.6) | 1.26 (0.09) | 0.56 (0.06) | 0.70 (0.05) |
| Trend p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.016 |
| Adequacy (%) | Model 1 OR (CI 95%) | Model 2 OR (CI 95%) | ||
|---|---|---|---|---|
| Male | ||||
| Household income quartiles | ||||
| Lower | 45.8 (2.4) | ref | ref | |
| Middle lower | 53.4 (2.7) | 1.04 (0.70, 1.55) | 0.99 (0.66, 1.49) | |
| Middle upper | 57.1 (3.2) | 1.09 (0.70, 1.69) | 1.05 (0.67, 1.66) | |
| Upper | 59.1 (4.1) | 1.02 (0.59, 1.75) | 0.99 (0.56, 1.77) | |
| Trend p | 0.863 | 0.951 | ||
| Educational attainment (year) | ||||
| ≤9 | 47.9 (2.1) | ref | ref | |
| 10~12 | 56.8 (3.0) | 1.19 (0.83, 1.70) | 1.23 (0.85, 1.77) | |
| 13≤ | 60.7 (4.3) | 1.74 (1.00, 3.05) | 1.74 (0.99, 3.06) | |
| Trend p | 0.044 | 0.042 | ||
| Female | ||||
| Household income quartiles | ||||
| Lower | 32.5 (1.7) | ref | ref | |
| Middle lower | 40.0 (2.3) | 1.43 (1.04, 1.97) | 1.45 (1.04, 2.02) | |
| Middle upper | 45.3 (3.2) | 1.13 (0.74, 1.74) | 1.17 (0.75, 1.83) | |
| Upper | 61.4 (3.7) | 2.41 (1.49, 3.90) | 2.50 (1.50, 4.17) | |
| Trend p | 0.002 | 0.002 | ||
| Educational attainment (year) | ||||
| ≤9 | 36.7 (1.5) | ref | ref | |
| 10–12 | 48.8 (4.0) | 1.26 (0.80, 1.99) | 1.29 (0.80, 2.06) | |
| 13≤ | 72.5 (4.6) | 3.30 (1.70, 6.40) | 3.21 (1.67, 6.17) | |
| Trend p | 0.001 | 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, D.H.; Park, H.A.; Cho, Y.G.; Kim, K.W.; Kim, N.H. Different Associations of Socioeconomic Status on Protein Intake in the Korean Elderly Population: A Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey. Nutrients 2020, 12, 10. https://doi.org/10.3390/nu12010010
Kwon DH, Park HA, Cho YG, Kim KW, Kim NH. Different Associations of Socioeconomic Status on Protein Intake in the Korean Elderly Population: A Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey. Nutrients. 2020; 12(1):10. https://doi.org/10.3390/nu12010010
Chicago/Turabian StyleKwon, Du Ho, Hyun Ah Park, Young Gyu Cho, Kyoung Woo Kim, and Na Hee Kim. 2020. "Different Associations of Socioeconomic Status on Protein Intake in the Korean Elderly Population: A Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey" Nutrients 12, no. 1: 10. https://doi.org/10.3390/nu12010010
APA StyleKwon, D. H., Park, H. A., Cho, Y. G., Kim, K. W., & Kim, N. H. (2020). Different Associations of Socioeconomic Status on Protein Intake in the Korean Elderly Population: A Cross-Sectional Analysis of the Korea National Health and Nutrition Examination Survey. Nutrients, 12(1), 10. https://doi.org/10.3390/nu12010010