Time and Age Trends in Free Sugar Intake from Food Groups among Children and Adolescents between 1985 and 2016



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Nutrition Assessment
2.3. Definitions of Outcome Variables
2.4. Assessment of Potential Confounding Factors
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
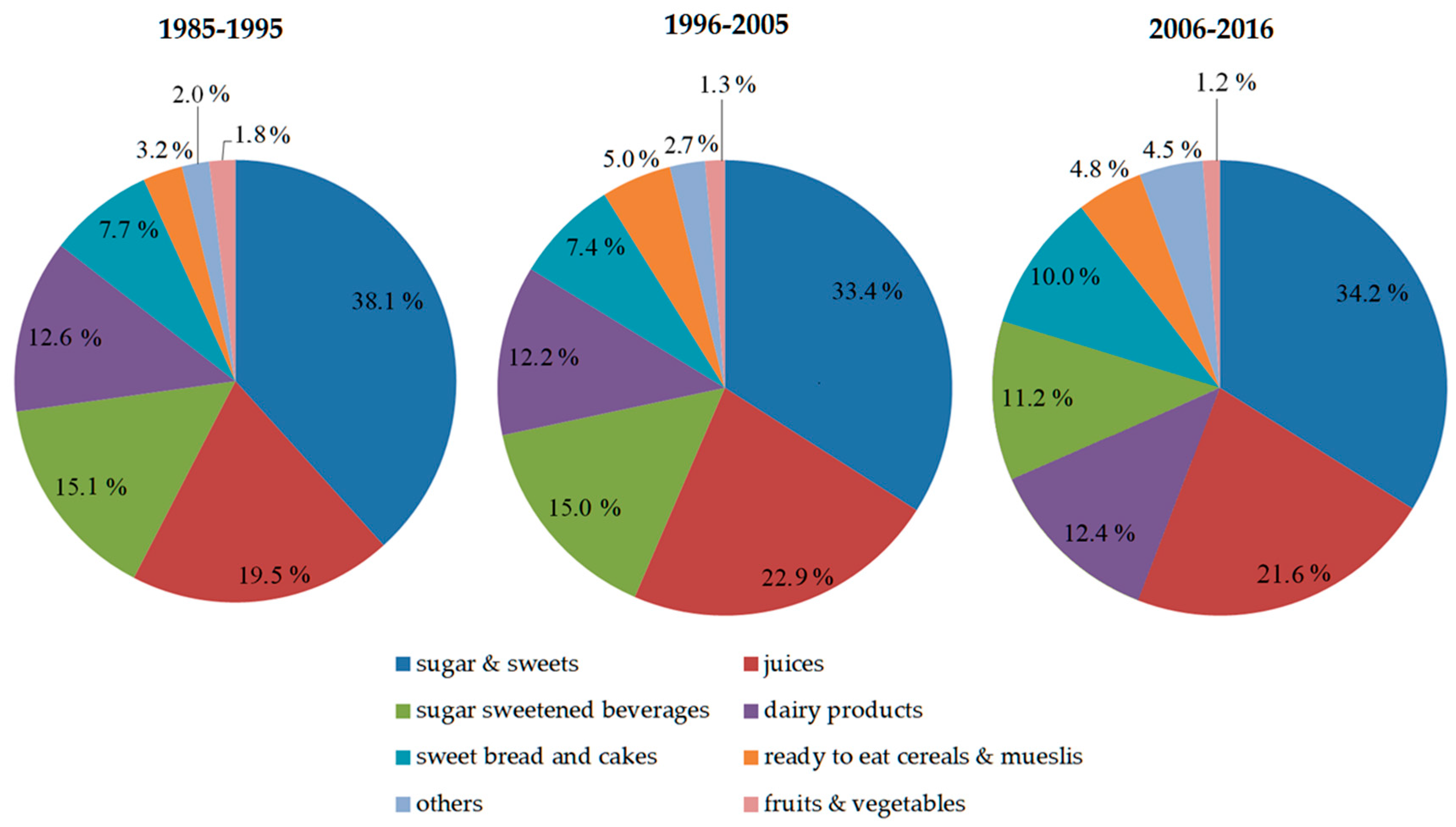
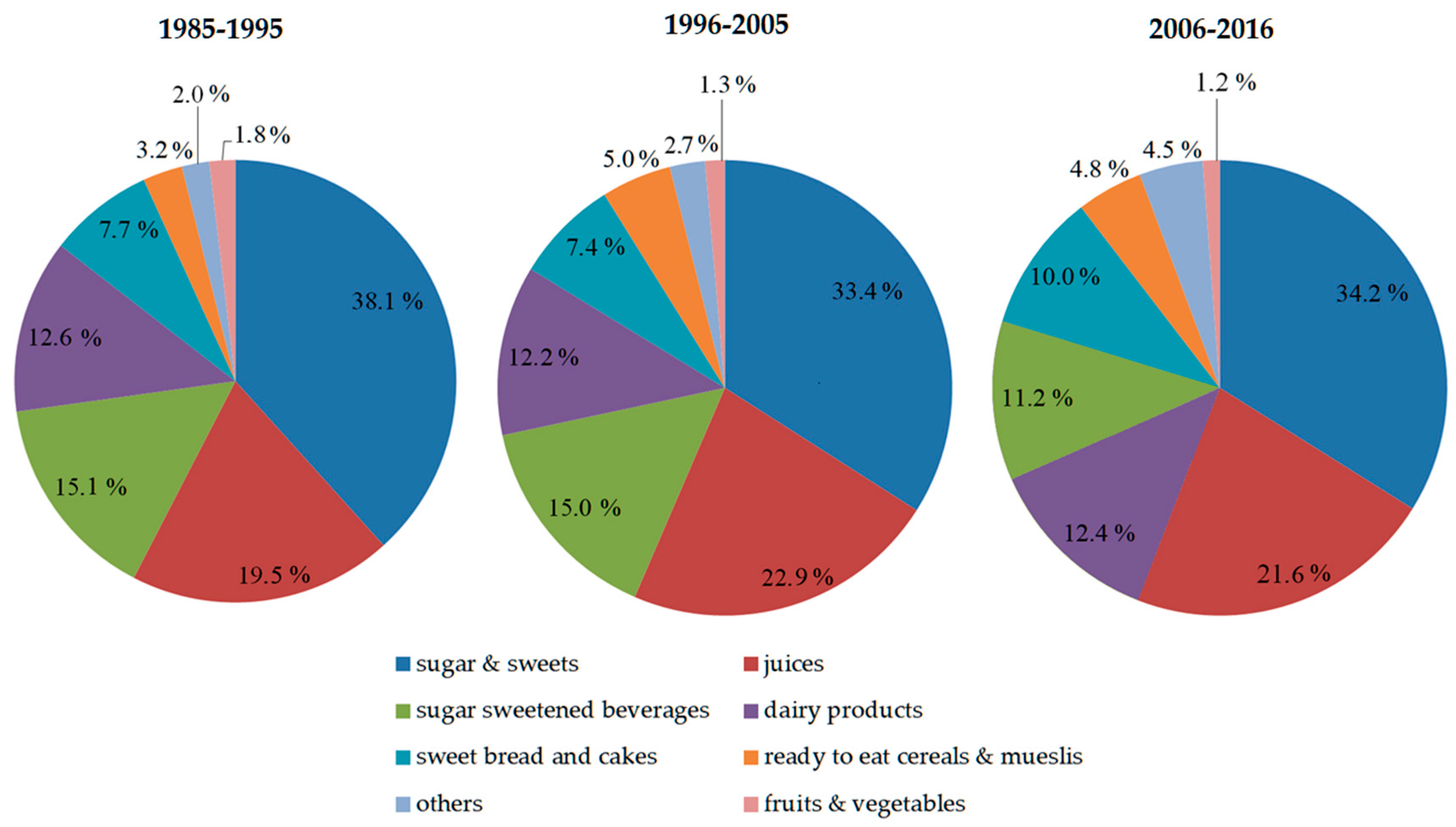
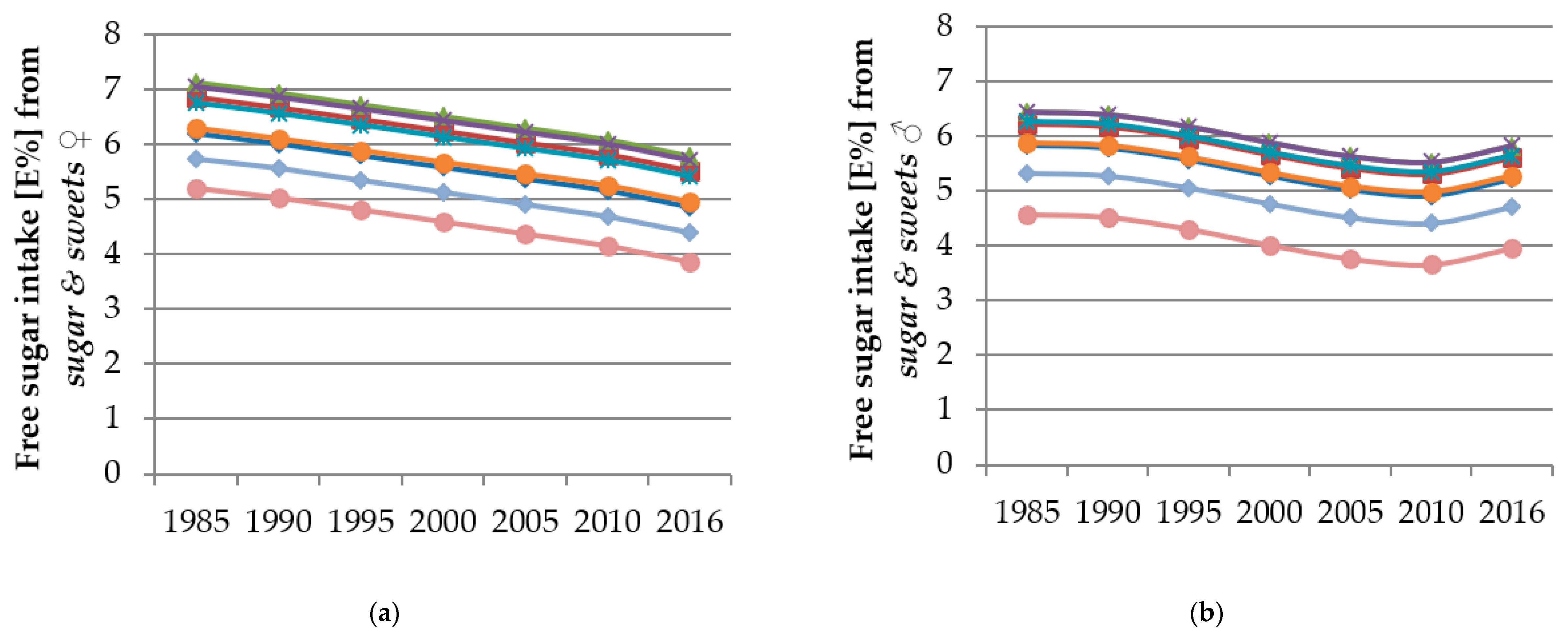
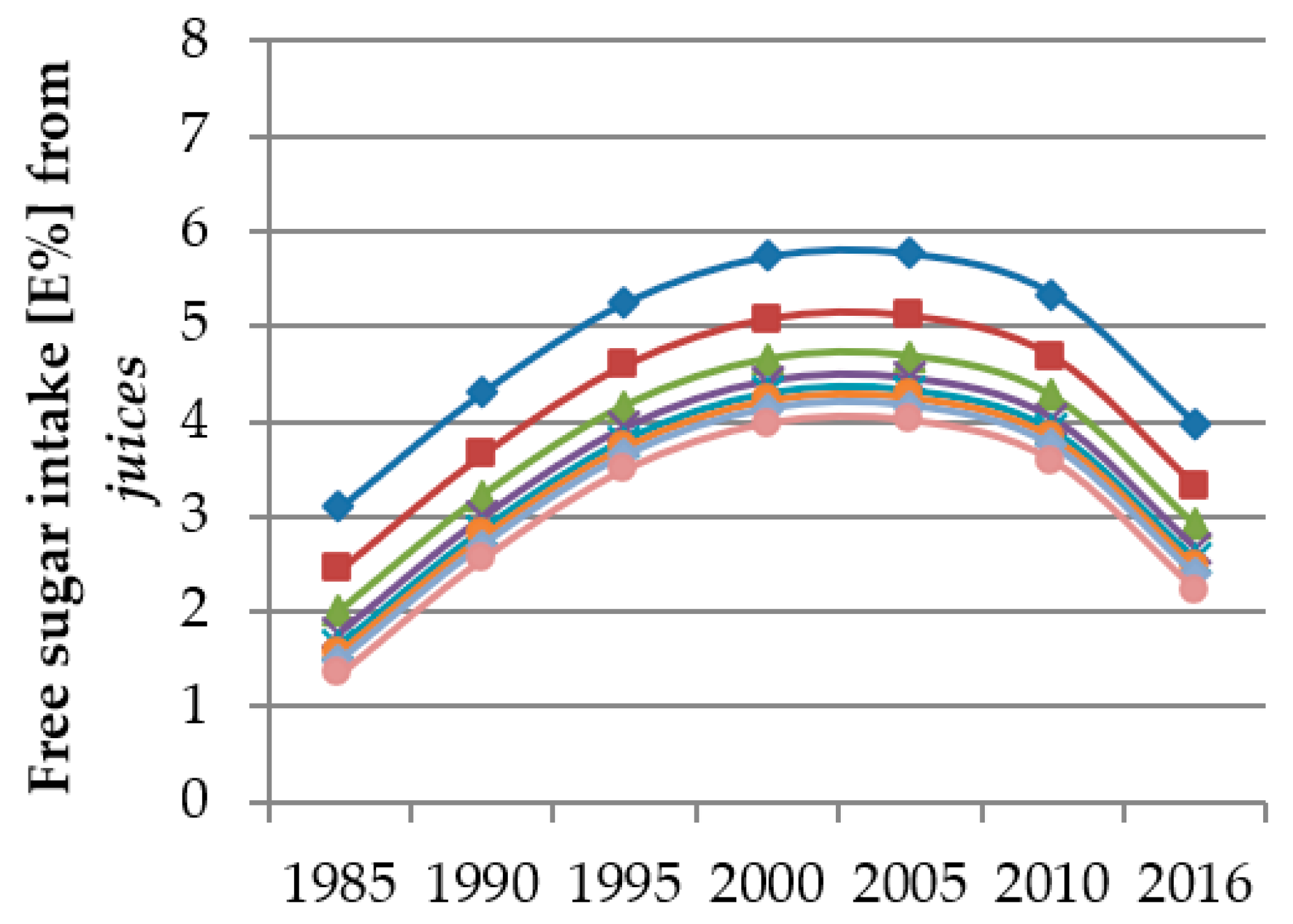
3.2. Time and Age Trends
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moynihan, P.J.; Kelly, S.A.M. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, J.A.; Cunningham, S.A. The role of added sugars in pediatric obesity. Pediatr. Clin. N. Am. 2011, 58, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, M.A.; Sheiham, A.; Liu, P.; Demarco, F.F.; Silva, A.E.R.; Assunção, M.C.; Menezes, A.M.; Barros, F.C.; Peres, K.G. Sugar Consumption and Changes in Dental Caries from Childhood to Adolescence. J. Dent. Res. 2016, 95, 388–394. [Google Scholar] [CrossRef]
- Ludwig, D.S.; Peterson, K.E.; Gortmaker, S.L. Relation between consumption of sugar-sweetened drinks and childhood obesity: A prospective, observational analysis. Lancet 2001, 357, 505–508. [Google Scholar] [CrossRef]
- Welsh, J.A.; Sharma, A.; Cunningham, S.A.; Vos, M.B. Consumption of added sugars and indicators of cardiovascular disease risk among US adolescents. Circulation 2011, 123, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Hu, F.B. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients 2019, 11, 1840. [Google Scholar] [CrossRef] [Green Version]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, L.A.; Madsen, K.A.; Cotterman, C.; Lustig, R.H. Added sugar intake and metabolic syndrome in US adolescents: Cross-sectional analysis of the National Health and Nutrition Examination Survey 2005–2012. Public Health Nutr. 2016, 19, 2424–2434. [Google Scholar] [CrossRef] [Green Version]
- Mourao, D.M.; Bressan, J.; Campbell, W.W.; Mattes, R.D. Effects of food form on appetite and energy intake in lean and obese young adults. Int. J. Obes. 2007, 31, 1688–1695. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar Sweetened Beverages, Obesity, Type 2 Diabetes and Cardiovascular Disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Libuda, L.; Alexy, U.; Sichert-Hellert, W.; Stehle, P.; Karaolis-Danckert, N.; Buyken, A.E.; Kersting, M. Pattern of beverage consumption and long-term association with body-weight status in German adolescents--results from the DONALD study. Br. J. Nutr. 2008, 99, 1370–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, L.; Imamura, F.; Lentjes, M.A.H.; Khaw, K.-T.; Wareham, N.J.; Forouhi, N.G. Prospective associations and population impact of sweet beverage intake and type 2 diabetes, and effects of substitutions with alternative beverages. Diabetologia 2015, 58, 1474–1483. [Google Scholar] [CrossRef] [Green Version]
- Pepin, A.; Stanhope, K.L.; Imbeault, P. Are Fruit Juices Healthier Than Sugar-Sweetened Beverages? A Review. Nutrients 2019, 11, 1006. [Google Scholar] [CrossRef] [Green Version]
- DiMeglio, D.P.; Mattes, R.D. Liquid versus solid carbohydrate: Effects on food intake and body weight. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 794–800. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef]
- Expert Consultation on Diet, Nutrition, and the Prevention of Chronic Diseases; WHO; FAO; Joint WHO-FAO Expert Consultation on Diet, Nutrition, and the Prevention of Chronic Diseases. Diet, Nutrition, and the Prevention of Chronic Diseases. Report of a WHO-FAO Expert Consultation; [Joint WHO-FAO Expert Consultation on Diet, Nutrition, and the Prevention of Chronic Diseases, 2002, Geneva, Switzerland; World Health Organization: Geneva, Switzerland, 2003; ISBN 92-4-120916-X. [Google Scholar]
- Swan, G.E.; Powell, N.A.; Knowles, B.L.; Bush, M.T.; Levy, L.B. A definition of free sugars for the UK. Public Health Nutr. 2018, 21, 1636–1638. [Google Scholar] [CrossRef] [Green Version]
- Scientific Advisory Committee on Nutrition. Minutes of the 48th Meeting. Available online: https://app.box.com/s/ivrivaemf7fgeo9a17xdmv167c4uvteu/file/106585193169 (accessed on 18 December 2019).
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-154902-8. [Google Scholar]
- Ernst, J.B.; Arens-Azevêdo, U.; Bitzer, B.; Bosy-Westphal, A.; de Zwaan, M.; Egert, S.; Fritsche, A.; Gerlach, S.; Hauner, H.; Heseker, H.; et al. für die Deutsche Adipositas-Gesellschaft, Deutsche Diabetes Gesellschaft und Deutsche Gesellschaft für Ernährung. Quantitative Empfehlung zur Zuckerzufuhr in Deutschland. Available online: https://www.dge.de/fileadmin/public/doc/ws/stellungnahme/Konsensuspapier_Zucker_DAG_DDG_DGE_2018.pdf (accessed on 18 December 2019).
- Perrar, I.; Alexy, U. Comments on: “The role of dietary sugars in health: Molecular composition or just calories?”. Eur. J. Clin. Nutr. 2019, 73, 1323–1324. [Google Scholar] [CrossRef]
- Prinz, P. The role of dietary sugars in health: Molecular composition or just calories? Eur. J. Clin. Nutr. 2019, 73, 1216–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, A.K.; Mennella, J.A. Innate and learned preferences for sweet taste during childhood. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Mennella, J.A.; Johnson, S.L.; Bellisle, F. Sweetness and food preference. J. Nutr. 2012, 142, 1142S–1148S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaf, C.; Zandstra, E. Sweetness intensity and pleasantness in children, adolescents, and adults. Physiol. Behav. 1999, 67, 513–520. [Google Scholar] [CrossRef]
- Graffe, M.I.M.; Pala, V.; de Henauw, S.; Eiben, G.; Hadjigeorgiou, C.; Iacoviello, L.; Intemann, T.; Jilani, H.; Molnar, D.; Russo, P.; et al. Dietary sources of free sugars in the diet of European children: The IDEFICS Study. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Perrar, I.; Schmitting, S.; Della Corte, K.W.; Buyken, A.E.; Alexy, U. Age and time trends in sugar intake among children and adolescents: Results from the DONALD study. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Heuer, T. Estimation of “Free” Sugar Intake in Germany Based on the Data of the German National Nutrition Survey II. Available online: https://www.openagrar.de/receive/openagrar_mods_00030594 (accessed on 22 July 2019).
- Dietz, W.H. Critical periods in childhood for the development of obesity. Am. J. Clin. Nutr. 1994, 59, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, L.T.; Burns, T.L.; Stanford, W.; Thompson, B.H.; Witt, J.D.; Rost, C.A.; Lauer, R.M. Coronary risk factors measured in childhood and young adult life are associated with coronary artery calcification in young adults: The Muscatine Study. J. Am. Coll. Cardiol. 1996, 27, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Buyken, A.E.; Mitchell, P.; Ceriello, A.; Brand-Miller, J. Optimal dietary approaches for prevention of type 2 diabetes: A life-course perspective. Diabetologia 2010, 53, 406–418. [Google Scholar] [CrossRef] [Green Version]
- The, N.; Suchindran, C.; North, K.E.; Popkin, B.M.; Gordon-Larsen, P. Association of adolescent obesity with risk of severe obesity in adulthood. JAMA 2010, 304, 2042–2047. [Google Scholar] [CrossRef] [Green Version]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Kroke, A.; Manz, F.; Kersting, M.; Remer, T.; Sichert-Hellert, W.; Alexy, U.; Lentze, M.J. The DONALD Study. History, current status and future perspectives. Eur. J. Nutr. 2004, 43, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Buyken, A.E.; Alexy, U.; Kersting, M.; Remer, T. Die DONALD Kohorte: Ein aktueller Überblick zu 25 Jahren Forschung im Rahmen der Dortmund Nutritional and Anthropometric Longitudinally Designed Study. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Sichert-Hellert, W.; Kersting, M.; Chahda, C.; Schäfer, R.; Kroke, A. German food composition database for dietary evaluations in children and adolescents. J. Food Compos. Anal. 2007, 20, 63–70. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [Green Version]
- Libuda, L.; Alexy, U.; Kersting, M. Time trends in dietary fat intake in a sample of German children and adolescents between 2000 and 2010: Not quantity, but quality is the issue. Br. J. Nutr. 2014, 111, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Diethelm, K.; Bolzenius, K.; Cheng, G.; Remer, T.; Buyken, A.E. Longitudinal associations between reported sleep duration in early childhood and the development of body mass index, fat mass index and fat free mass index until age 7. Int. J. Pediatr. Obes. 2011, 6, e114–e123. [Google Scholar] [CrossRef]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar]
- Sichert-Hellert, W.; Kersting, M.; Schöch, G. Underreporting of energy intake in 1 to 18 year old German children and adolescents. Z. Ernahrungswiss. 1998, 37, 242–251. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poppitt, S.D.; Swann, D.; Black, A.E.; Prentice, A.M. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 303–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armfield, J.M.; Spencer, A.J.; Roberts-Thomson, K.F.; Plastow, K. Water fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am. J. Public Health 2013, 103, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, K. Reformulierte Lebensmittel in Deutschland-Bestandsaufnahme, Barrieren, Handlungsfelder. Ernährungsumschau 2019, 30–40. [Google Scholar] [CrossRef]
- Bundesministerium für Ernährung und Landwirtschaft. Nationale Reduktions-und Innovationsstrategie für Zucker, Fette und Salz in Fertigprodukten. Available online: https://www.bmel.de/SharedDocs/Downloads/Ernaehrung/NationaleReduktionsInnovationsstrategie-Kabinett.pdf?__blob=publicationFile (accessed on 14 December 2019).
- Bagus, T.; Roser, S.; Watzl, B. Reformulierung von Verarbeiteten Lebensmitteln. Bewertungen und Empfehlungen zur Reduktion des Zuckergehalts. Available online: https://www.mri.bund.de/fileadmin/MRI/Themen/Reformulierung/Reformulierung_Thema-Zucker.pdf (accessed on 13 December 2019).
- Krug, S.; Finger, J.D.; Lange, C.; Richter, A.; Mensink, G.B.M. Sport-und Ernährungsverhalten bei Kindern und Jugendlichen in Deutschland—Querschnittergebnisse Aus KiGGS Welle 2 und Trends. 2018. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/Journal-of-Health-Monitoring_02_2018_KiGGS-Welle2_Gesundheitsverhalten.pdf?__blob=publicationFile (accessed on 11 December 2019).
- Mensink, G.B.M.; Schienkiewitz, A.; Rabenberg, M.; Borrmann, A.; Richter, A.; Haftenberger, M. Konsum zuckerhaltiger Erfrischungsgetränke bei Kindern und Jugendlichen in Deutschland—Querschnittergebnisse aus KiGGS Welle 2 und Trends. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/FactSheets/JoHM_01_2018_zuckerhaltige_Getraenke_KiGGS-Welle2.pdf?__blob=publicationFile (accessed on 11 December 2019).
- Welsh, J.A.; Sharma, A.J.; Grellinger, L.; Vos, M.B. Consumption of added sugars is decreasing in the United States. Am. J. Clin. Nutr. 2011, 94, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Stahl, A.; Vohmann, C.; Richter, A.; Heseker, H.; Mensink, G.B.M. Changes in food and nutrient intake of 6- to 17-year-old Germans between the 1980s and 2006. Public Health Nutr. 2009, 12, 1912–1923. [Google Scholar] [CrossRef] [Green Version]
- Lytle, L.A.; Seifert, S.; Greenstein, J.; McGovern, P. How do children’s eating patterns and food choices change over time? Results from a cohort study. Am. J. Health Promot. 2000, 14, 222–228. [Google Scholar] [CrossRef]
- Cheng, G.; Libuda, L.; Karaolis-Danckert, N.; Alexy, U.; Bolzenius, K.; Remer, T.; Buyken, A.E. Trends in dietary carbohydrate quality during puberty from 1988 to 2007: A cause for concern? Br. J. Nutr. 2010, 104, 1375–1383. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Zhu, H.; Gutin, B.; Dong, Y. Race, Gender, Family Structure, Socioeconomic Status, Dietary Patterns, and Cardiovascular Health in Adolescents. Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef]
- Mazarello Paes, V.; Hesketh, K.; O’Malley, C.; Moore, H.; Summerbell, C.; Griffin, S.; van Sluijs, E.M.F.; Ong, K.K.; Lakshman, R. Determinants of sugar-sweetened beverage consumption in young children: A systematic review. Obes. Rev. 2015, 16, 903–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kranz, S.; Siega-Riz, A.M. Sociodemographic determinants of added sugar intake in preschoolers 2 to 5 years old. J. Pediatr. 2002, 140, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Desbouys, L.; de Ridder, K.; Rouche, M.; Castetbon, K. Food Consumption in Adolescents and Young Adults: Age-Specific Socio-Economic and Cultural Disparities (Belgian Food Consumption Survey 2014). Nutrients 2019, 11, 1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuer, T. Zuckerkonsum in Deutschland. Aktuel Ernahr. 2018, 43, S8–S11. [Google Scholar] [CrossRef]
- Mensink, G.B.M.; Kleiser, C.; Richter, A. Lebensmittelverzehr bei Kindern und Jugendlichen in Deutschland. Ergebnisse des Kinder- und Jugendgesundheitssurveys (KiGGS). Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 609–623. [Google Scholar] [CrossRef] [Green Version]
- Sluik, D.; van Lee, L.; Engelen, A.I.; Feskens, E.J.M. Total, Free, and Added Sugar Consumption and Adherence to Guidelines: The Dutch National Food Consumption Survey 2007–2010. Nutrients 2016, 8, 70. [Google Scholar] [CrossRef]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [Green Version]
- Svensson, A.; Larsson, C.; Eiben, G.; Lanfer, A.; Pala, V.; Hebestreit, A.; Huybrechts, I.; Fernández-Alvira, J.M.; Russo, P.; Koni, A.C.; et al. European children’s sugar intake on weekdays versus weekends: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 822–828. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Group | Components |
|---|---|
| Sugar & sweets | Sugars and other sweeteners (including syrups), sweet spreads, sweets and marshmallows, chocolate and bars, ice cream, jelly desserts, sweet sauces, sweet baking ingredients (e.g., marzipan) |
| Dairy products | unfermented (e.g., milk, cream, pudding) and fermented dairy products (e.g., yoghurt, buttermilk) all types of cheese (e.g., cream, soft, hard and processed cheese), dairy powder, vegan milk and cheese substitutes, instant milk beverages (e.g., cocoa) |
| Fruits & vegetables | Fresh, frozen, canned and dried fruits and vegetables |
| Juices | Fruits and vegetable juices, juice spritzers and smoothies |
| Sugar sweetened beverages (SSB) | Sweetened fruit juice drinks and nectars, soft drinks/sodas, sweetened teas and waters, instant beverages (except dairy drinks), sweetened sport drinks |
| Sweet bread & cakes | Sweet breads, pastries, cakes, pies, baking mixtures |
| Ready to eat breakfast cereals (RTC) | Ready to eat cereals and mueslis |
| Others | Eggs and egg meals (e.g., pancakes), meat and meat products, fish and fish products, vegetarian/vegan meat substitutes and spreads, fats and oils, flours, grains, breads, doughs, salty snacks, noodles, pasta, potatoes and potato products, nuts and seeds, legumes, alcoholic drinks, unsweetened teas, ready to eat meals, instant soups, sauces and dressings, spices, formula and baby food |
| Female | 652 (49.7) |
| Anthropometrics | |
| Overweight 1 | 161 (12.3) |
| Maternal characteristics | |
| Overweight 2 | 432 (32.9) |
| High educational status 3 | 817 (62.3) |
| Employment | 784 (59.8) |
| Girls | Boys | |||||
|---|---|---|---|---|---|---|
| 1985–1995 | 1996–2005 | 2006–2016 | 1985–1995 | 1996–2005 | 2006–2016 | |
| nrecords | 1348 | 1977 | 1953 | 1375 | 1945 | 2163 |
| Age | 7.0 (4.7; 10.1) | 9.0 (6.0; 13.0) | 10.0 (6.0; 14.0) | 7.0 (4.9; 10.3) | 9.1 (6.0; 13.1) | 9.3 (6.0; 14.0) |
| TEI [kcal] | 1390 (1156; 1680) | 1495 (1238; 1785) | 1524 (1265; 1821) | 1596 (1307; 1917) | 1742 (1409; 2162) | 1731 (1372; 2139) |
| TEI/BMR | 1.4 (1.2; 1.6) | 1.4 (1.2; 1.5) | 1.4 (1.2; 1.5) | 1.5 (1.3; 1.6) | 1.4 (1.2; 1.6) | 1.4 (1.2; 1.6) |
| Carbohydrates [%E] | 49.8 (46.1; 53.5) | 52.1 (48.3; 55.8) | 52.3 (48.4; 56.3) | 49.8 (46.0; 53.9) | 51.9 (47.9; 55.9) | 52.1 (48.1; 55.9) |
| Total sugar [%E] | 27.5 (23.6; 31.7) | 27.5 (23.1; 32.0) | 25.5 (21.0; 30.6) | 27.1 (23.2; 31.9) | 27.6 (22.9; 32.1) | 25.6 (21.0; 30.1) |
| Added sugar [%E] | 12.5 (8.8; 16.4) | 12.9 (9.4; 16.9) | 11.8 (8.7; 15.5) | 12.8 (9.3; 16.6) | 13.0 (9.7; 17.3) | 12.0 (8.9; 15.4) |
| Free sugar intake [%E] | 16.5 (12.3; 20.6) | 17.3 (13.2; 21.9) | 16.0 (11.6; 20.4) | 16.3 (12.3; 20.7) | 17.9 (13.8; 22.4) | 16.1 (12.1; 20.8) |
| FS from sugar & sweets | 5.8 (3.7; 8.2) | 5.5 (3.5; 8.0) | 5.0 (3.0; 7.6) | 5.5 (3.6; 7.8) | 4.9 (2.9; 7.7) | 4.7 (2.8; 7.2) |
| FS from juices | 2.5 (0.0; 5.7) | 3.2 (0.0; 6.5) | 2.8 (0.0; 6.2) | 2.1 (0.0; 5.1) | 3.4 (0.7; 6.9) | 2.9 (0.0; 6.2) |
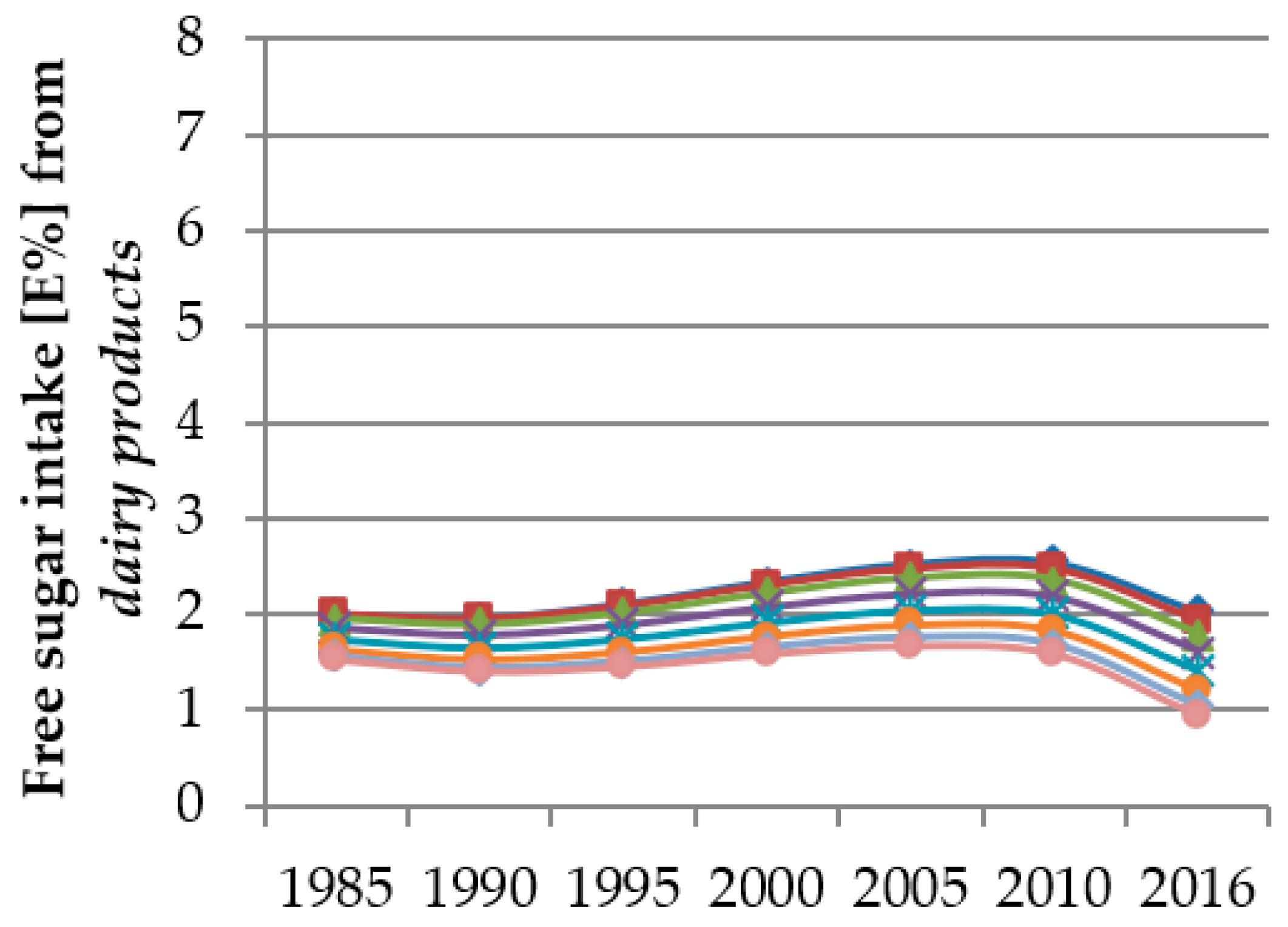
| FS from dairy products | 1.6 (0.4; 3.0) | 1.6 (0.4; 2.9) | 1.5 (0.3; 2.8) | 1.6 (0.4; 3.0) | 1.6 (0.4; 3.2) | 1.5 (0.1; 3.1) |
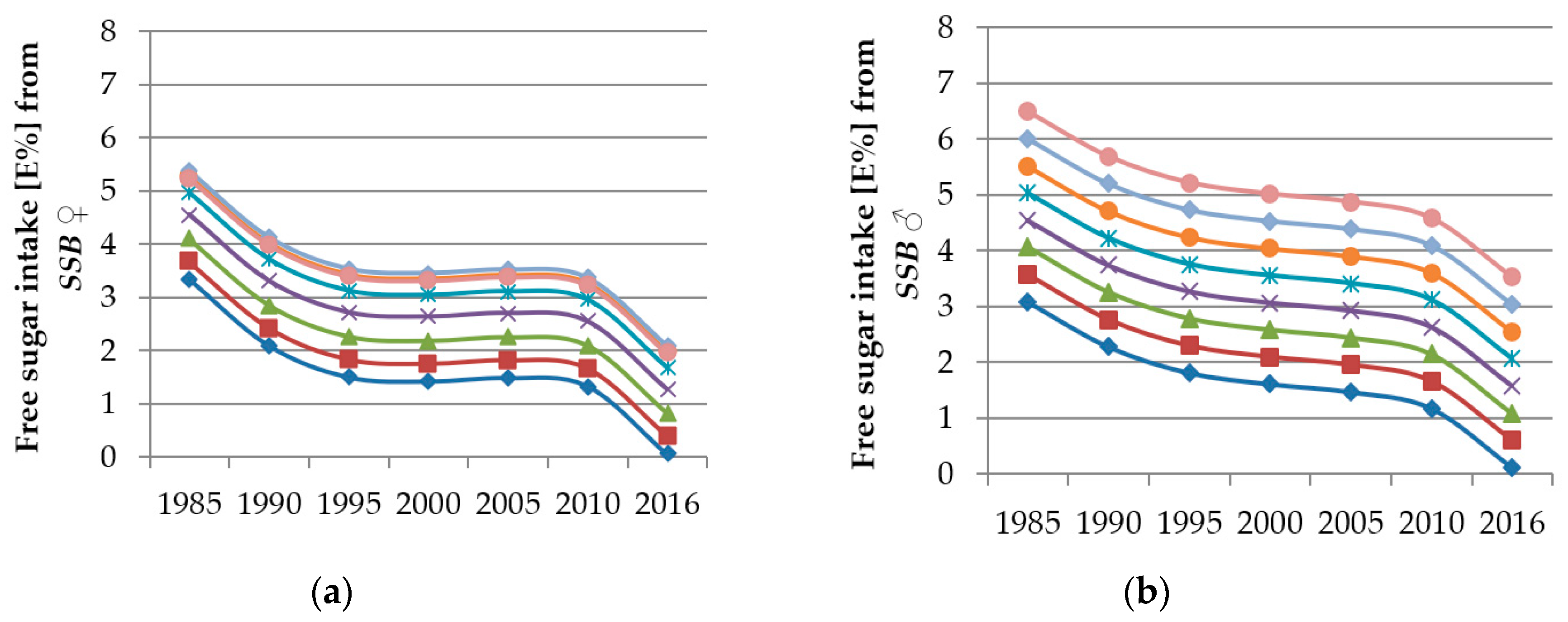
| FS from SSB | 1.9 (0.0; 5.0) | 1.5 (0.0; 4.9) | 0.0 (0.0; 3.3) | 2.2 (0.0; 5.6) | 2.1 (0.0; 4.9) | 0.9 (0.0; 3.8) |
| FS from sweet breads & cakes | 0.8 (0.1; 1.7) | 0.9 (0.1; 2.0) | 1.1 (0.2; 2.3) | 0.7 (0.0; 1.8) | 0.7 (0.0; 1.8) | 1.0 (0.0; 2.3) |
| FS from RTC | 0.0 (0.0; 0.3) | 0.0 (0.0; 1.0) | 0.0 (0.0; 0.8) | 0.0 (0.0; 0.5) | 0.0 (0.0; 1.5) | 0.0 (0.0; 1.1) |
| FS from others | 0.1 (0.0; 0.3) | 0.2 (0.1; 0.5) | 0.4 (0.2; 0.8) | 0.1 (0.0; 0.3) | 0.2 (0.0; 0.5) | 0.4 (0.2; 0.8) |
| FS from fruits & vegetables | 0.0 (0.0; 0.2) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.2) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) |
| Girls | Boys | |||||||
|---|---|---|---|---|---|---|---|---|
| 3–5 Years | 6–10 Years | 11–14 Years | 15–18 Years | 3–5 Years | 6–10 Years | 11–14 Years | 15–18 Years | |
| nrecords | 1382 | 1895 | 1163 | 838 | 1428 | 1978 | 1216 | 861 |
| TEI [kcal] | 1133 | 1497 | 1772 | 1771 | 1242 | 1673 | 2010 | 2452 |
| (1003; 1274) | (1309; 1685) | (1529; 2021) | (1498; 2056) | (1091; 1402) | (1466; 1884) | (1743; 2319) | (2100; 2819) | |
| TEI/BMR | 1.36 (1.23; 1.51) | 1.43 (1.28;1.59) | 1.35 (1.15; 1.52) | 1.19 (1.00; 1.40) | 1.39 (1.24; 1.54) | 1.49 (1.32; 1.64) | 1.36 (1.17; 1.54) | 1.31 (1.11; 1.51) |
| Carbohydrates [%E] | 51.4 (47.4; 55.3) | 51.8 (48.2; 55.7) | 51.4 (47.5; 55.5) | 51.4 (47.2; 55.6) | 51.8 (47.9; 56.1) | 51.8 (47.9; 55.6) | 51.3 (47.6; 55.1) | 50.1 (45.9; 54.5) |
| Total sugar [%E] | 28.1 (24.0; 32.7) | 27.4 (23.3; 31.6) | 25.6 (21.3; 30.3) | 25.0 (19.8; 30.0) | 28.5 (24.4; 33.5) | 26.9 (23.0; 31.2) | 25.7 (21.3; 30.3) | 23.5 (19.5; 28.7) |
| Added sugar [%E] | 11.6 (8.6; 14.9) | 13.3 (9.9; 16.8) | 12.8 (8.9; 15.6) | 11.6 (7.9; 15.8) | 11.7 (8.5; 15.3) | 13.0 (9.7; 16.6) | 13.2 (9.7; 17.2) | 12.2 (8.5; 16.5) |
| Free sugar intake [%E] | 16.3 (12.1; 20.6) | 17.5 (13.4; 21.5) | 16.7 (12.4; 21.3) | 15.2 (10.8; 20.0) | 16.9 (12.6; 21.7) | 17.0 (13.1; 21.4) | 16.9 (13.0; 21.4) | 15.8 (11.7; 20.7) |
| FS from sugar & sweets | 5.4 (3.4; 7.9) | 6.0 (3.9; 8.6) | 5.3 (3.3; 7.9) | 4.0 (2.2; 6.5) | 5.2 (3.3; 7.6) | 5.5 (3.5; 7.8) | 4.9 (3.0; 7.6) | 3.8 (1.8; 6.1) |
| FS from juices | 3.6 (0.7; 7.1) | 3.0 (0.0; 6.4) | 2.4 (0.0; 5.5) | 1.8 (0.0; 5.2) | 4.0 (1.1, 7.6) | 2.8 (0.0; 6.2) | 2.2 (0.0; 5.2) | 2.2 (0.0; 5.2) |
| FS from dairy products | 1.8 (0.5; 3.3) | 1.7 (0.6; 3.1) | 1.4 (0.2; 2.6) | 1.1 (0.0; 2.4) | 1.8 (0.5; 3.4) | 1.7 (0.5; 3.3) | 1.4 (0.2; 2.8) | 1.0 (0.0; 2.5) |
| FS from SSB | 0.0 (0.0; 2.7) | 1.2 (0.0; 4.1) | 1.9 (0.0; 5.6) | 1.9 (0.0; 5.9) | 0.0 (0.0; 2.8) | 1.6 (0.0; 4.4) | 2.5 (0.0; 6.5) | 3.2 (0.0; 7.6) |
| FS from sweet breads & cakes | 1.1 (0.3; 2.2) | 1.1 (0.2; 2.2) | 0.8 (0.0; 1.9) | 0.7 (0.0; 1.9) | 1.0 (0.0; 2.2) | 1.0 (0.1; 2.2) | 0.6 (0.0; 1.8) | 0.3 (0.0; 1.4) |
| FS from RTC | 0.0 (0.0; 0.5) | 0.0 (0.0; 0.9) | 0.0 (0.0; 0.9) | 0.0 (0.0; 0.9) | 0.0 (0.0; 0.6) | 0.1 (0.0; 1.4) | 0.0 (0.0; 1.3) | 0.0 (0.0; 1.1) |
| FS from others | 0.2 (0.0; 0.4) | 0.2 (0.0; 0.5) | 0.3 (0.1; 0.7) | 0.4 (0.1; 0.8) | 0.2 (0.0; 0.5) | 0.2 (0.1; 0.6) | 0.3 (0.1; 0.7) | 0.4 (0.1; 0.9) |
| FS from fruits & vegetables | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) |
| Age Trend Per Year of Age (3–18 Years) a | Time Trend Per Study Year (1985–2016) b | Interaction of Time and Age | |||||
|---|---|---|---|---|---|---|---|
| Age β (p) | Age2 β (p) | Age3 β (p) | Time β (p) | Time2 β (p) | Time3 β (p) | Age × Time β (p) | |
| FS from sugar & sweets | |||||||
| Girls c Unadjusted model | 0.9268 (<0.0001) | −0.07895 (<0.0001) | 0.001717 (0.0029) | −0.04032 (<0.0001) | |||
| Adjusted model | 0.9330 (<0.0001) | −0.07851 (<0.0001) | 0.001697 (0.0033) | −0.04294 (<0.0001) | |||
| Boys d Unadjusted model | 0.3994 (<0.0001) | −0.02390 (<0.0001) | 0.01535 (0.8293) | −0.00605 (0.2198) | 0.000156 (0.1144) | ||
| Adjusted model | 0.4158 (<0.0001) | −0.02409 (<0.0001) | 0.01052 (0.8833) | −0.00548 (0.2700) | 0.000144 (0.1482) | ||
| FS from juicese | |||||||
| Unadjusted model | −0.7443 (0.0001) | 0.05349 (0.0009) | −0.00136 (0.0084) | 0.3250 (<0.0001) | −0.00895 (<0.0001) | ||
| Adjusted model | −0.7304 (0.0001) | 0.05339 (0.0009) | −0.00136 (0.0082) | 0.3150 (<0.0001) | −0.00892 (<0.0001) | ||
| FS from dairy productsf | |||||||
| Unadjusted model | 0.1192 (0.0699) | −0.01531 (0.0273) | 0.000471 (0.0352) | −0.03703 (0.1907) | 0.006421 (0.0009) | −0.00017 (<0.0001) | −0.00149 (0.0489) |
| Adjusted model | 0.1159 (0.0780) | −0.01604 (0.0207) | 0.000492 (0.0280) | −0.02873 (0.3094) | 0.006435 (0.0009) | −0.00017 (<0.0001) | −0.00140 (0.0634) |
| FS from SSB | |||||||
| Girls g Unadjusted model | −0.04422 (0.8096) | 0.03543 (0.0715) | −0.00144 (0.0241) | −0.4051 (<0.0001) | 0.02430 (<0.0001) | −0.00049 (<0.0001) | |
| Adjusted model | −0.07104 (0.6987) | 0.03659 (0.0629) | −0.00148 (0.0211) | −0.3789 (<0.0001) | 0.02412 (<0.0001) | −0.00049 (<0.0001) | |
| Boys h Unadjusted model | 0.2649 (<0.0001) | −0.2793 (0.0004) | 0.01462 (0.0085) | −0.00030 (0.0072) | |||
| Adjusted model | 0.2433 (<0.0001) | −0.2359 (0.0028) | 0.01329 (0.0165) | −0.00028 (0.0135) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrar, I.; Schadow, A.M.; Schmitting, S.; Buyken, A.E.; Alexy, U. Time and Age Trends in Free Sugar Intake from Food Groups among Children and Adolescents between 1985 and 2016. Nutrients 2020, 12, 20. https://doi.org/10.3390/nu12010020
Perrar I, Schadow AM, Schmitting S, Buyken AE, Alexy U. Time and Age Trends in Free Sugar Intake from Food Groups among Children and Adolescents between 1985 and 2016. Nutrients. 2020; 12(1):20. https://doi.org/10.3390/nu12010020
Chicago/Turabian StylePerrar, Ines, Alena M. Schadow, Sarah Schmitting, Anette E. Buyken, and Ute Alexy. 2020. "Time and Age Trends in Free Sugar Intake from Food Groups among Children and Adolescents between 1985 and 2016" Nutrients 12, no. 1: 20. https://doi.org/10.3390/nu12010020
APA StylePerrar, I., Schadow, A. M., Schmitting, S., Buyken, A. E., & Alexy, U. (2020). Time and Age Trends in Free Sugar Intake from Food Groups among Children and Adolescents between 1985 and 2016. Nutrients, 12(1), 20. https://doi.org/10.3390/nu12010020