Effects of Sucralose Ingestion versus Sucralose Taste on Metabolic Responses to an Oral Glucose Tolerance Test in Participants with Normal Weight and Obesity: A Randomized Crossover Trial


Abstract
1. Introduction
2. Materials and Methods
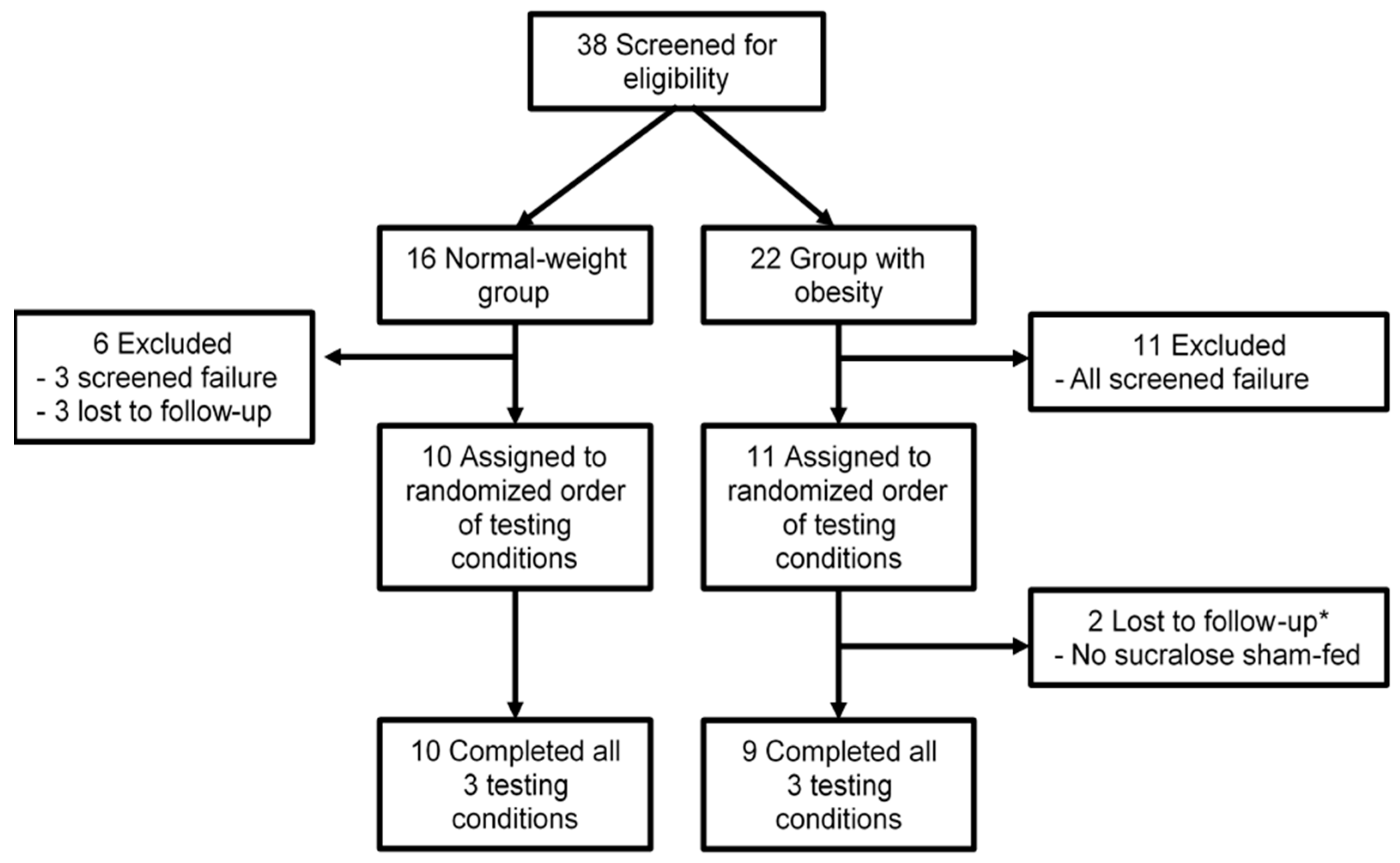
2.1. Study Overview
2.2. Participants
2.3. Laboratory Assessments
2.4. Calculations
2.4.1. Insulin Sensitivity
2.4.2. β-Cell Function and Insulin Clearance
2.4.3. Glucose Kinetics
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
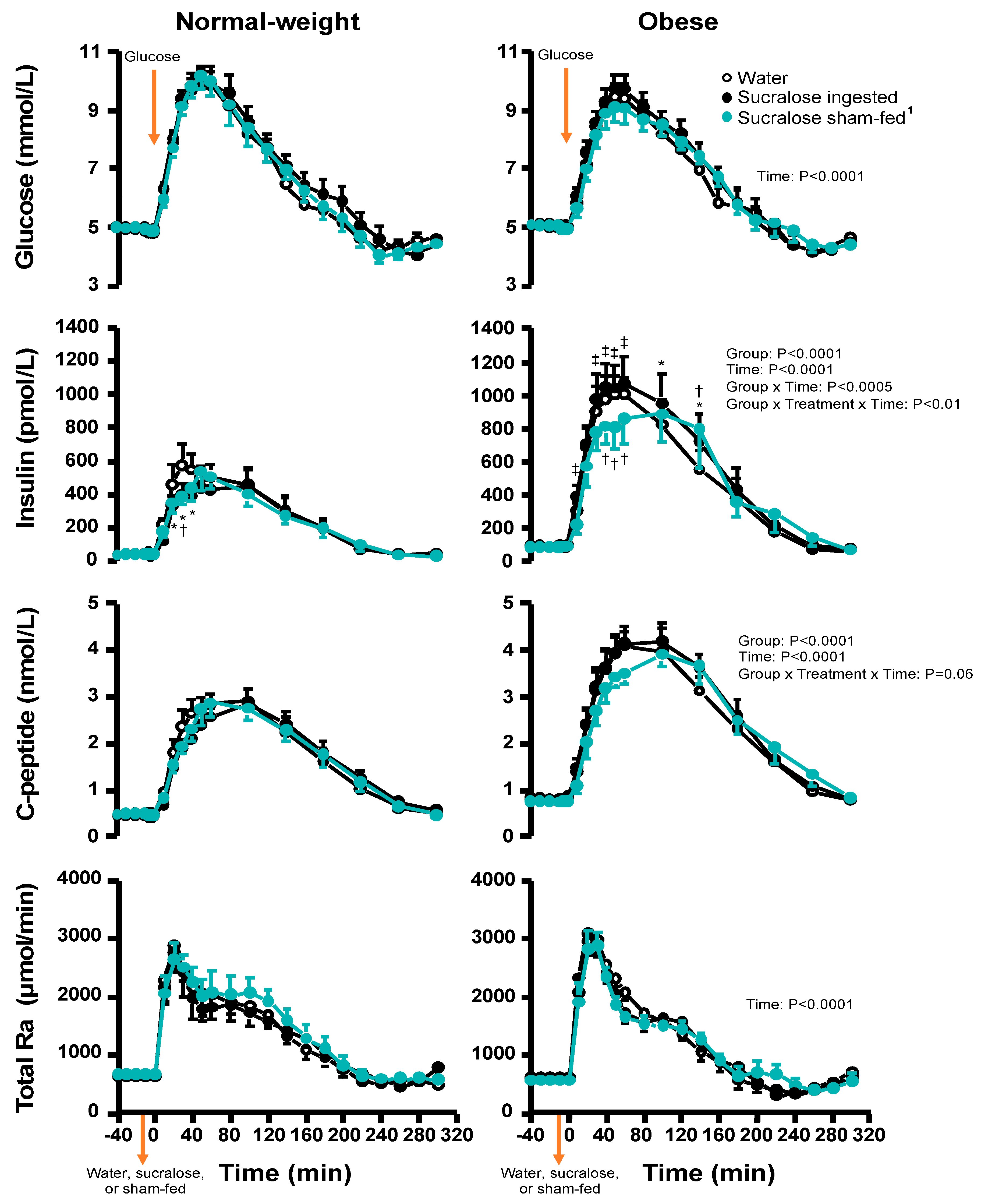
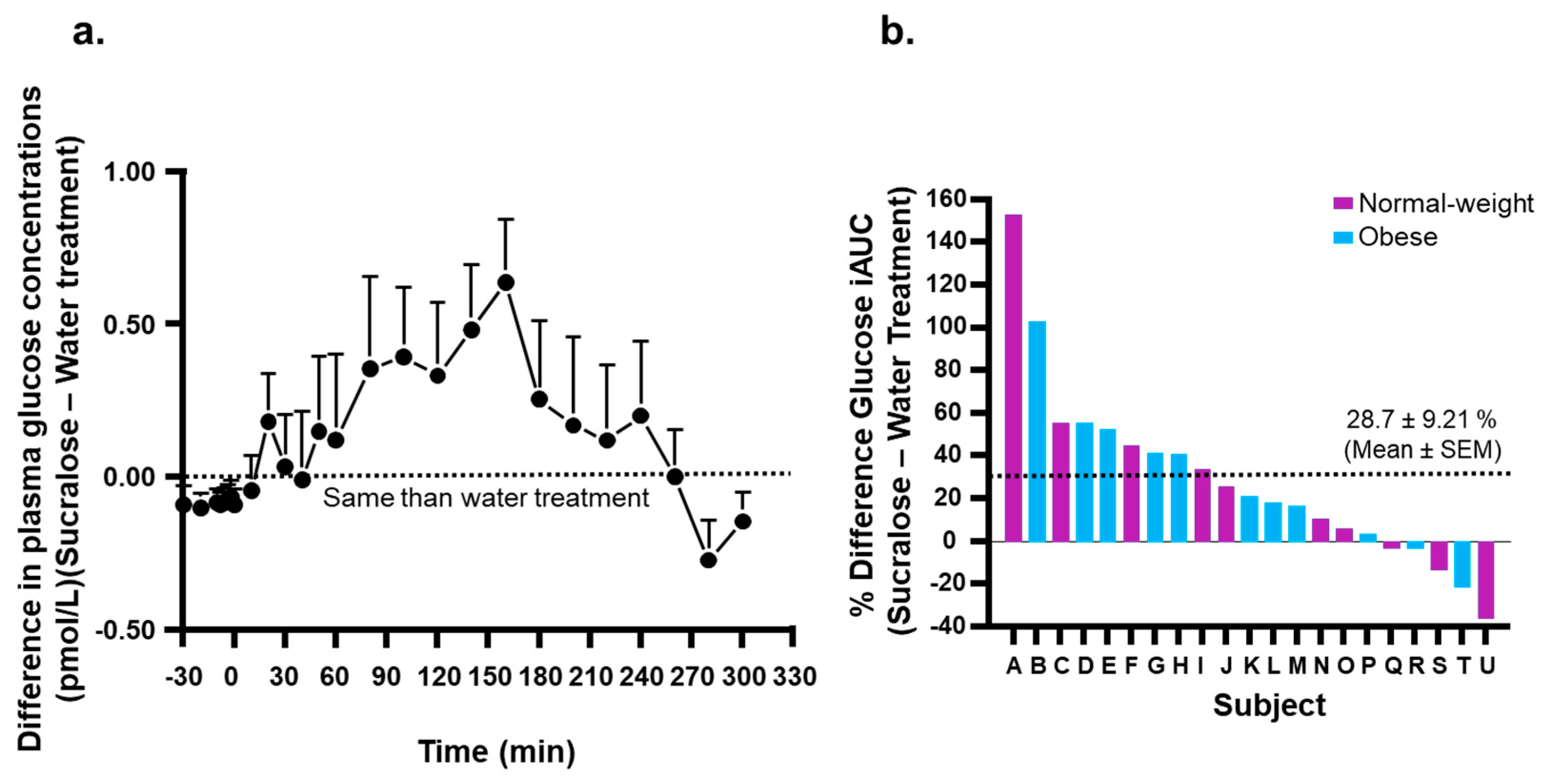
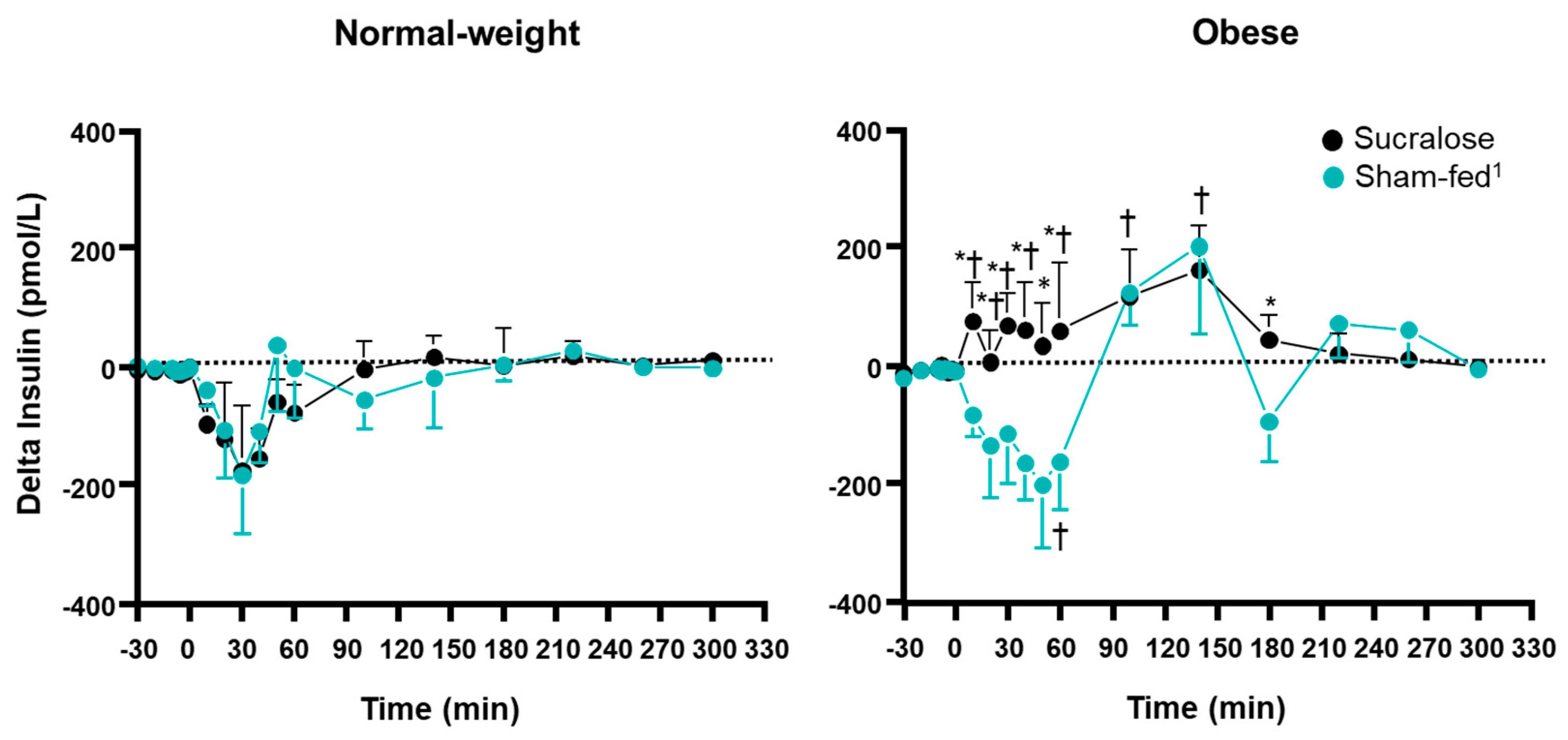
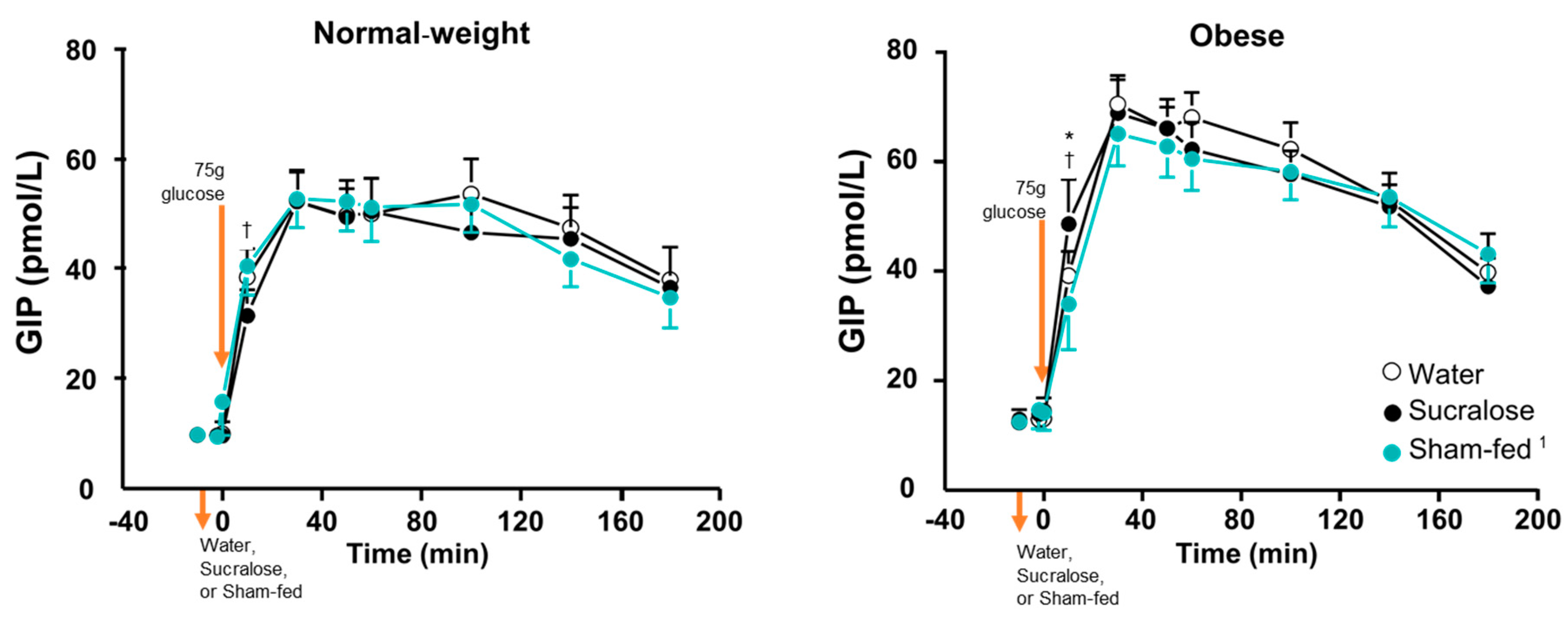
3.2. Plasma Glucose and Hormone Concentrations
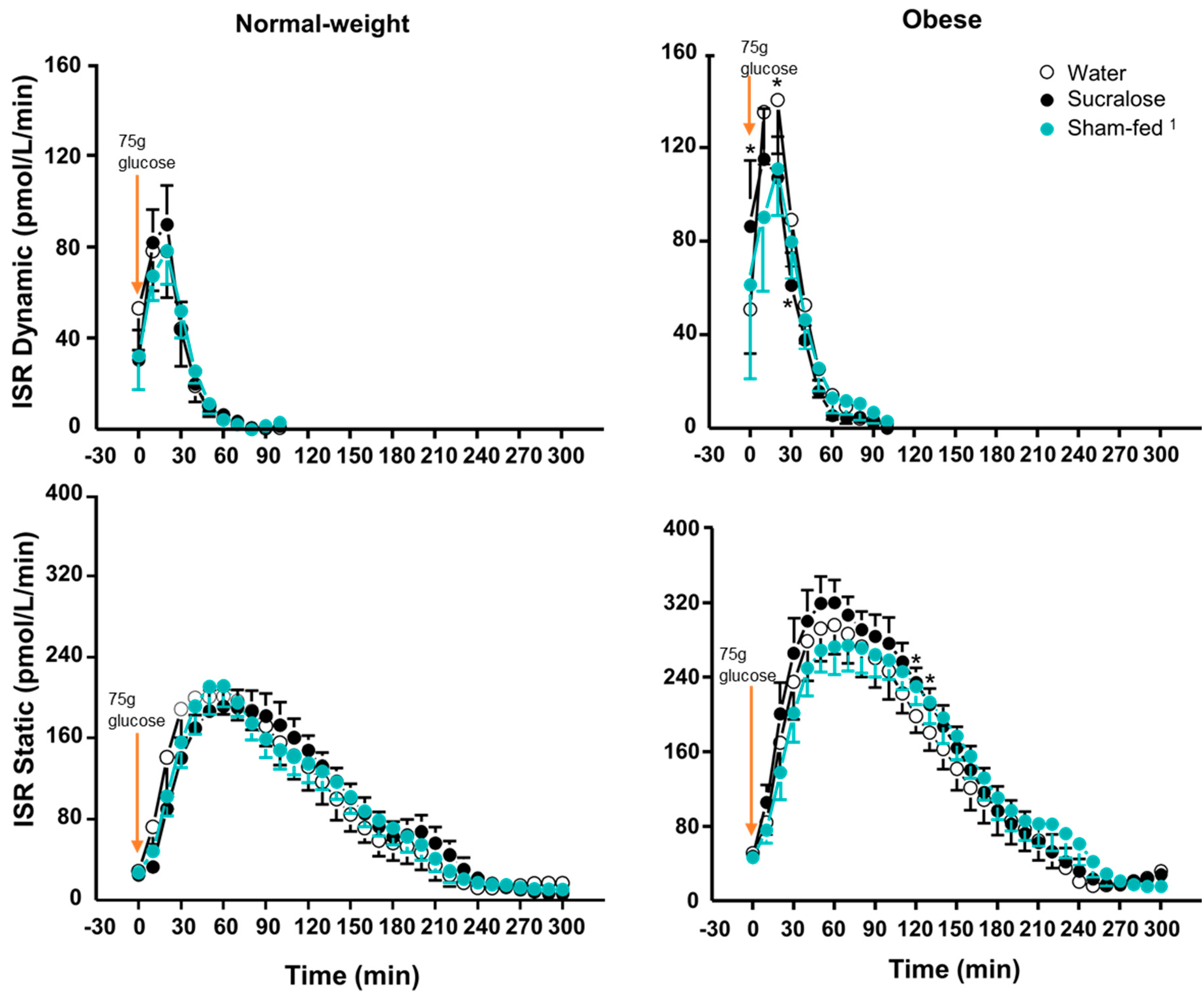
3.3. β-Cell Response
3.4. Insulin Sensitivity and Clearance
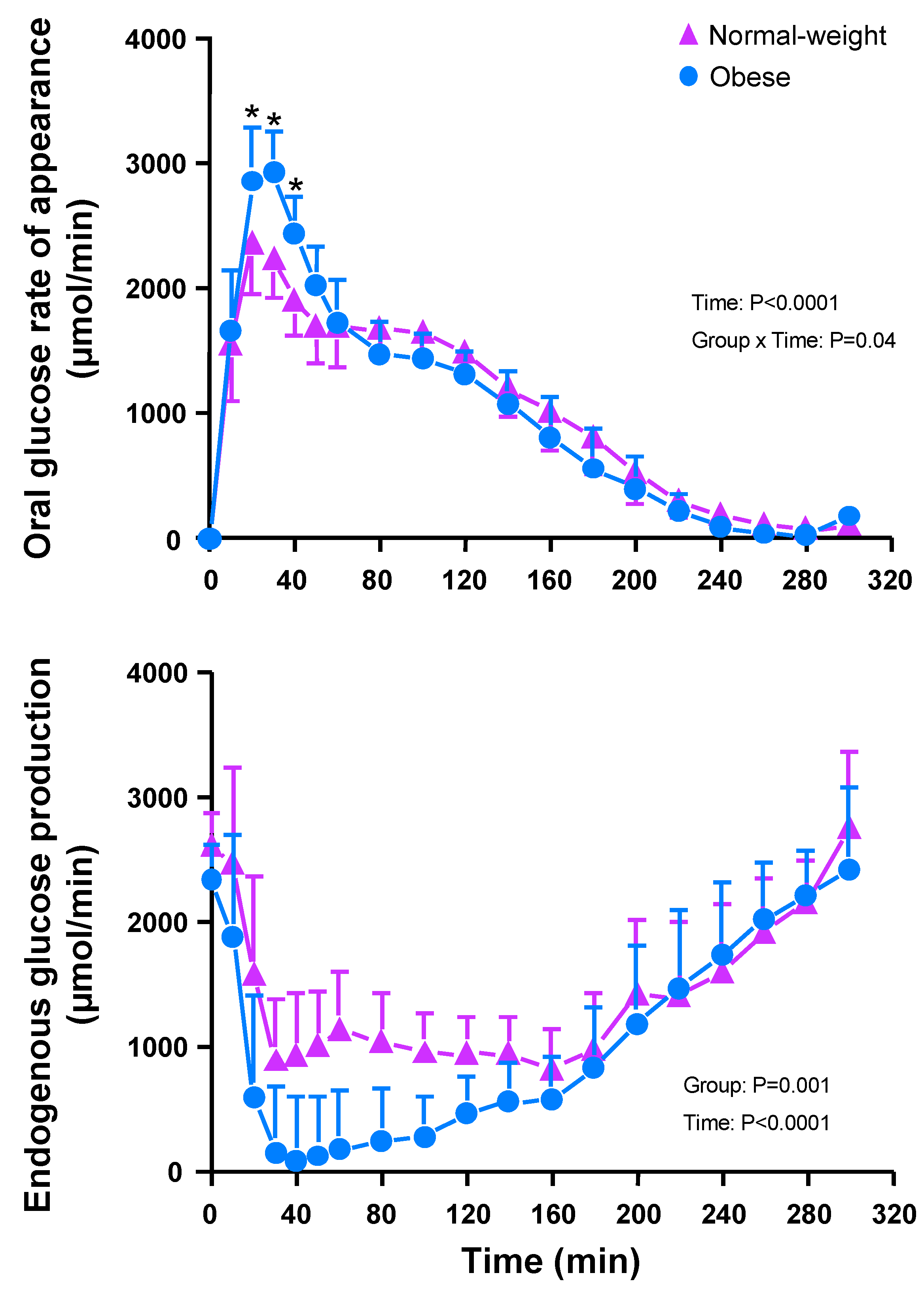
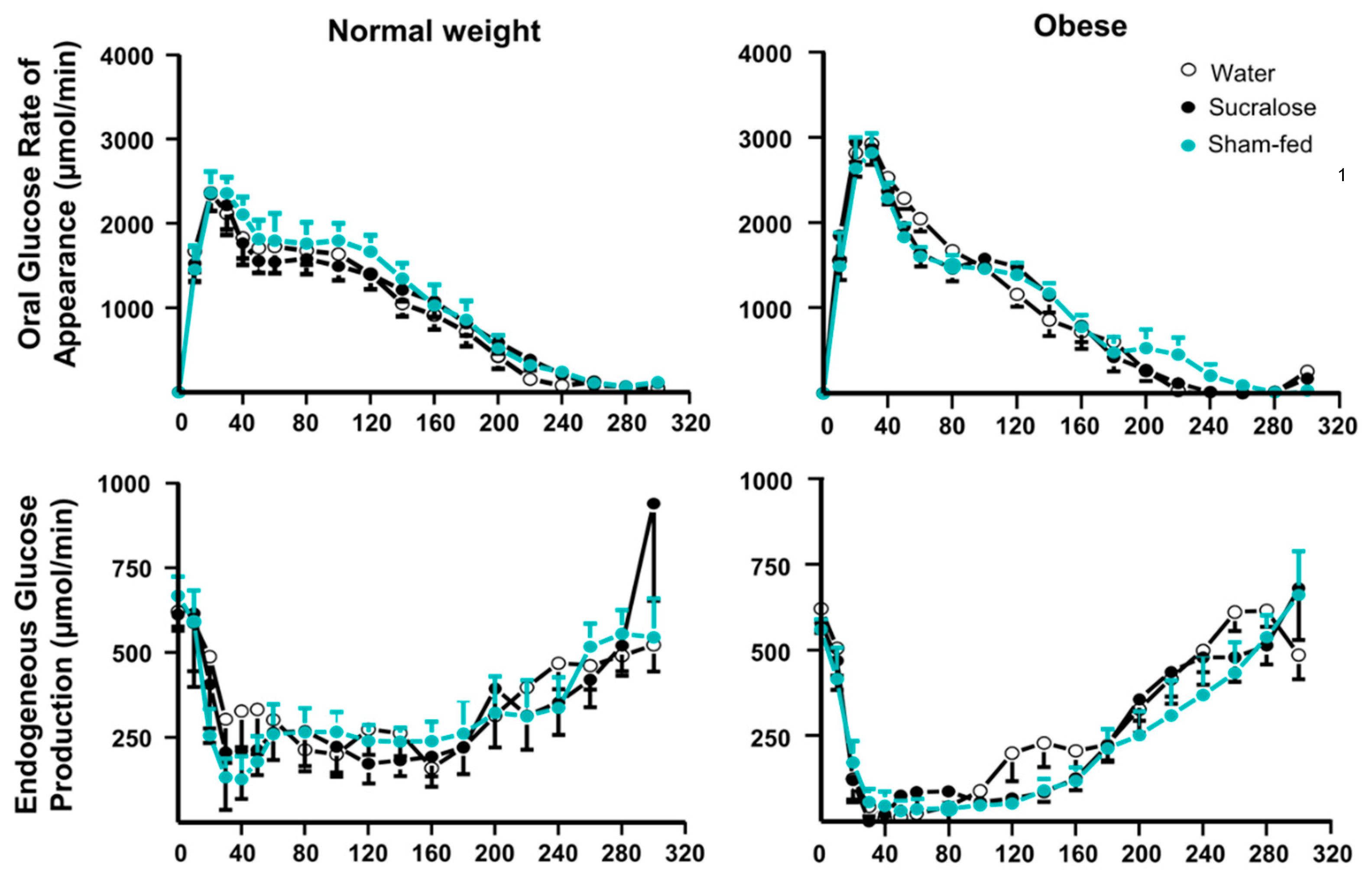
3.5. Glucose Kinetics
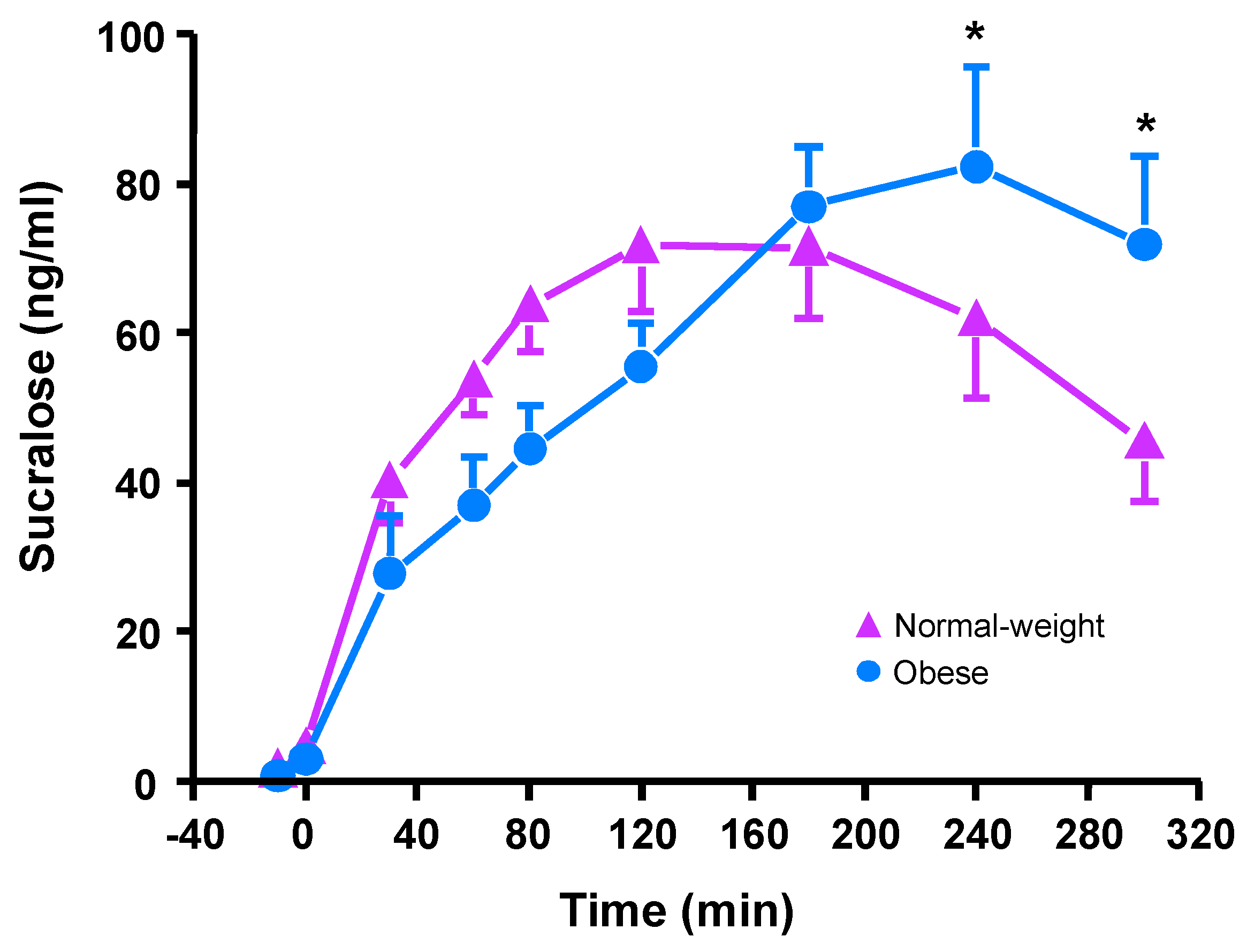
3.6. Plasma Sucralose Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Supplementary Methods
Appendix B





References
- Rippe, J.M.; Angelopoulos, T.J. Relationship between Added Sugars Consumption and Chronic Disease Risk Factors: Current Understanding. Nutrients 2016, 8, 697. [Google Scholar] [CrossRef]
- Hess, J.; Latulippe, M.E.; Ayoob, K.; Slavin, J. The confusing world of dietary sugars: Definitions, intakes, food sources and international dietary recommendations. Food Funct. 2012, 3, 477–486. [Google Scholar] [CrossRef]
- Sylvetsky, A.C.; Jin, Y.C.; Clark, E.J.; Welsh, J.A.; Rother, K.I.; Talegawkar, S.A. Consumption of Low-Calorie Sweeteners among Children and Adults in the United States. J. Acad. Nutr. Diet. 2017, 117, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Rother, K.I.; Conway, E.M.; Sylvetsky, A.C. How Non-nutritive Sweeteners Influence Hormones and Health. Trends Endocrinol. Metab. 2018, 29, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Margolskee, R.F.; Dyer, J.; Kokrashvili, Z.; Salmon, K.S.; Ilegems, E.; Daly, K.; Maillet, E.L.; Ninomiya, Y.; Mosinger, B.; Shirazi-Beechey, S.P. T1R3 and gustducin in gut sense sugars to regulate expression of Na+-glucose cotransporter 1. Proc. Natl. Acad. Sci. USA 2007, 104, 15075–15080. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.W.; Al-Rammahi, M.A.; Arora, D.K.; Batchelor, D.J.; Coulter, E.A.; Daly, K.; Ionescu, C.; Bravo, D.; Shirazi-Beechey, S.P. Expression of Na+/glucose co-transporter 1 (SGLT1) is enhanced by supplementation of the diet of weaning piglets with artificial sweeteners. Brit. J. Nutr. 2010, 104, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Stearns, A.T.; Balakrishnan, A.; Rhoads, D.B.; Tavakkolizadeh, A. Rapid Upregulation of Sodium-Glucose Transporter SGLT1 in Response to Intestinal Sweet Taste Stimulation. Ann. Surg. 2010, 251, 865–871. [Google Scholar] [CrossRef]
- Mace, O.J.; Affleck, J.; Patel, N.; Kellett, G.L. Sweet taste receptors in rat small intestine stimulate glucose absorption through apical GLUT2. J. Physiol.-Lond. 2007, 582, 379–392. [Google Scholar] [CrossRef]
- Jang, H.J.; Kokrashvili, Z.; Theodorakis, M.J.; Carlson, O.D.; Kim, B.J.; Zhou, J.; Kim, H.H.; Xu, X.; Chan, S.L.; Juhaszova, M.; et al. Gut-expressed gustducin and taste receptors regulate secretion of glucagon-like peptide-1. Proc. Natl. Acad. Sci. USA 2007, 104, 15069–15074. [Google Scholar] [CrossRef]
- Kojima, I.; Nakagawa, Y.; Hamano, K.; Medina, J.; Li, L.F.; Nagasawa, M. Glucose-Sensing Receptor T1R3: A New Signaling Receptor Activated by Glucose in Pancreatic beta-Cells. Biol. Pharm. Bull. 2015, 38, 674–679. [Google Scholar] [CrossRef]
- Kyriazis, G.A.; Soundarapandian, M.M.; Tyrberg, B. Sweet taste receptor signaling in beta cells mediates fructose-induced potentiation of glucose-stimulated insulin secretion. Proc. Natl. Acad. Sci. USA 2012, 109, E524–E532. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, Y.; Nagasawa, M.; Yamada, S.; Hara, A.; Mogami, H.; Nikolaev, V.O.; Lohse, M.J.; Shigemura, N.; Ninomiya, Y.; Kojima, I. Sweet taste receptor expressed in pancreatic beta-cells activates the calcium and cyclic AMP signaling systems and stimulates insulin secretion. PLoS ONE 2009, 4, e5106. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Azari, E.K.; LaMoia, T.E.; Hussain, T.; Vargova, V.; Karolyi, K.; Veldhuis, P.; Arnoletti, J.; de la Fuente, S.; Pratley, R.; et al. T1R2 receptor-mediated glucose sensing in the upper intestine potentiates glucose absorption through activation of local regulatory pathways. Mol. Metab. 2018, 17, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Wölnerhanssen, B.K.; Cajacob, L.; Keller, N.; Doody, A.; Rehfeld, J.F.; Drewe, J.; Peterli, R.; Beglinger, C.; Meyer-Gerspach, A.C. Gut hormone secretion, gastric emptying, and glycemic responses to erythritol and xylitol in lean and obese subjects. Am. J. Physiol.Endocrinol. Metab. 2016, 310, E1053–E1061. [Google Scholar] [CrossRef]
- Wu, T.; Zhao, B.R.; Bound, M.J.; Checklin, H.L.; Bellon, M.; Little, T.J.; Young, R.L.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Effects of different sweet preloads on incretin hormone secretion, gastric emptying, and postprandial glycemia in healthy humans. Am. J. Clin. Nutr. 2012, 95, 78–83. [Google Scholar] [CrossRef]
- Powley, T.L.; Berthoud, H.R. Diet and cephalic phase insulin responses. Am. J. Clin. Nutr. 1985, 42, 991–1002. [Google Scholar] [CrossRef]
- Teff, K. Nutritional implications of the cephalic-phase reflexes: Endocrine responses. Appetite 2000, 34, 206–213. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Tiemann, C.D.; Patterson, B.W.; Wice, B.M.; Klein, S. Sucralose affects glycemic and hormonal responses to an oral glucose load. Diabetes Care 2013, 36, 2530–2535. [Google Scholar] [CrossRef]
- Brown, A.W.; Bohan Brown, M.M.; Onken, K.L.; Beitz, D.C. Short-term consumption of sucralose, a nonnutritive sweetener, is similar to water with regard to select markers of hunger signaling and short-term glucose homeostasis in women. Nutr. Res. 2011, 31, 882–888. [Google Scholar] [CrossRef]
- Ford, H.E.; Peters, V.; Martin, N.M.; Sleeth, M.L.; Ghatei, M.A.; Frost, G.S.; Bloom, S.R. Effects of oral ingestion of sucralose on gut hormone response and appetite in healthy normal-weight subjects. Eur. J. Clin. Nutr. 2011, 65, 508–513. [Google Scholar] [CrossRef]
- Wu, T.; Bound, M.J.; Standfield, S.D.; Bellon, M.; Young, R.L.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Artificial sweeteners have no effect on gastric emptying, glucagon-like peptide-1, or glycemia after oral glucose in healthy humans. Diabetes Care 2013, 36, e202–e203. [Google Scholar] [CrossRef] [PubMed]
- Gummesson, A.; Carlsson, L.M.S.; Storlien, L.H.; Backhed, F.; Lundin, P.; Lofgren, L.; Stenlof, K.; Lam, Y.Y.; Fagerberg, B.; Carlsson, B. Intestinal Permeability Is Associated with Visceral Adiposity in Healthy Women. Obesity 2011, 19, 2280–2282. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.A.; Boudreau, G.S.; Devlin, M.J.; Walsh, B.T. Artificial sweetener use among individuals with eating disorders. Int. J. Eat. Disorder. 2006, 39, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Sylvetsky, A.C.; Walter, P.J.; Garraffo, H.M.; Robien, K.; Rother, K.I. Widespread sucralose exposure in a randomized clinical trial in healthy young adults. Am. J. Clin. Nutr. 2017, 105, 820–823. [Google Scholar] [CrossRef]
- Allison, D.B.; Paultre, F.; Maggio, C.; Mezzitis, N.; Pisunyer, F.X. The Use of Areas under Curves in Diabetes Research. Diabetes Care 1995, 18, 245–250. [Google Scholar] [CrossRef]
- Dalla Man, C.; Caumo, A.; Basu, R.; Rizza, R.; Toffolo, G.; Cobelli, C. Minimal model estimation of glucose absorption and insulin sensitivity from oral test: Validation with a tracer method. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E637–E643. [Google Scholar] [CrossRef]
- Breda, E.; Cavaghan, M.K.; Toffolo, G.; Polonsky, K.S.; Cobelli, C. Oral glucose tolerance test minimal model indexes of beta-cell function and insulin sensitivity. Diabetes 2001, 50, 150–158. [Google Scholar] [CrossRef]
- Gastaldelli, A.; Casolaro, A.; Pettiti, M.; Nannipieri, M.; Ciociaro, D.; Frascerra, S.; Buzzigoli, E.; Baldi, S.; Mari, A.; Ferrannini, E. Effect of Pioglitazone on the Metabolic and Hormonal Response to a Mixed Meal in Type II Diabetes. Clin. Pharmacol. Ther. 2007, 81, 205–212. [Google Scholar] [CrossRef]
- Steele, R. Influences of Glucose Loading and of Injected Insulin on Hepatic Glucose Output. Ann. N. Y. Acad. Sci. 1959, 82, 420–430. [Google Scholar] [CrossRef]
- Teff, K.L.; Engelman, K. Oral sensory stimulation improves glucose tolerance in humans: Effects on insulin, C-peptide, and glucagon. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1996, 270, R1371–R1379. [Google Scholar] [CrossRef]
- Teff, K.L.; Townsend, R.R. Early phase insulin infusion and muscarinic blockade in obese and lean subjects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1999, 277, R198–R208. [Google Scholar] [CrossRef] [PubMed]
- Veldhuizen, M.G.; Babbs, R.K.; Patel, B.; Fobbs, W.; Kroemer, N.B.; Garcia, E.; Yeomans, M.R.; Small, D.M. Integration of Sweet Taste and Metabolism Determines Carbohydrate Reward. Curr. Biol. 2017, 27, 2476–2485. [Google Scholar] [CrossRef] [PubMed]
- Proietto, J.; Rohner-Jeanrenaud, F.; Ionescu, E.; Jeanrenaud, B. Role of the oropharynx in regulation of glycemia. Diabetes 1987, 36, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Azari, E.K.; Smith, K.R.; Yi, F.C.; Osborne, T.F.; Bizzotto, R.; Mari, A.; Pratley, R.E.; Kyriazis, G.A. Inhibition of sweet chemosensory receptors alters insulin responses during glucose ingestion in healthy adults: A randomized crossover interventional study. Am. J. Clin. Nut. 2017, 105, 1001–1009. [Google Scholar] [CrossRef]
- Gerspach, A.C.; Steinert, R.E.; Schönenberger, L.; Graber-Maier, A.; Beglinger, C. The role of the gut sweet taste receptor in regulating GLP-1, PYY, and CCK release in humans. Am. J. Physiol. Endocrinol. Metab. 2011, 301, E317–E325. [Google Scholar] [CrossRef]
- Lertrit, A.; Srimachai, S.; Saetung, S.; Chanprasertyothin, S.; Chailurkit, L.O.; Areevut, C.; Katekao, P.; Ongphiphadhanakul, B.; Sriphrapradang, C. Effects of sucralose on insulin and glucagon-like peptide-1 secretion in healthy subjects: A randomized, double-blind, placebo-controlled trial. Nutrition 2018, 55–56, 125–130. [Google Scholar] [CrossRef]
- Romo-Romo, A.; Aguilar-Salinas, C.A.; Brito-Cordova, G.X.; Gomez-Diaz, R.A.; Almeda-Valdes, P. Sucralose decreases insulin sensitivity in healthy subjects: A randomized controlled trial. Am. J. Clin. Nut. 2018, 108, 485–491. [Google Scholar] [CrossRef]
- Peper, A. Aspects of the Relationship between Drug Dose and Drug Effect. Dose Response 2009, 7, 172–192. [Google Scholar] [CrossRef]
- Nguyen, N.Q.; Debreceni, T.L.; Bambrick, J.E.; Chia, B.; Wishart, J.; Deane, A.M.; Rayner, C.K.; Horowitz, M.; Young, R.L. Accelerated Intestinal Glucose Absorption in Morbidly Obese Humans: Relationship to Glucose Transporters, Incretin Hormones, and Glycemia. J. Clin. Endocr. Metab. 2015, 100, 968–976. [Google Scholar] [CrossRef]
- Wisen, O.; Johansson, C. Gastrointestinal Function in Obesity - Motility, Secretion, and Absorption Following a Liquid Test Meal. Metab. Clin. Exp. 1992, 41, 390–395. [Google Scholar] [CrossRef]
- Conte, C.; Fabbrini, E.; Kars, M.; Mittendorfer, B.; Patterson, B.W.; Klein, S. Multiorgan Insulin Sensitivity in Lean and Obese Subjects. Diabetes Care 2012, 35, 1316–1321. [Google Scholar] [CrossRef] [PubMed]
- Jani, R.; Molina, M.; Matsuda, M.; Balas, B.; Chavez, A.; DeFronzo, R.A.; Abdul-Ghani, M. Decreased Non-Insulin-Dependent Glucose Clearance Contributes to the Rise in Fasting Plasma Glucose in the Nondiabetic Range. Diabetes Care 2008, 31, 311–315. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Swithers, S.E.; Laboy, A.F.; Clark, K.; Cooper, S.; Davidson, T.L. Experience with the high-intensity sweetener saccharin impairs glucose homeostasis and GLP-1 release in rats. Behav. Brain Res. 2012, 233, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A.; et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Brener, W.; Hendrix, T.R.; McHugh, P.R. Regulation of the gastric emptying of glucose. Gastroenterology 1983, 85, 76–82. [Google Scholar] [PubMed]
- Phillips, W.T.; Schwartz, J.G.; Blumhardt, R.; McMahan, C.A. Linear gastric emptying of hyperosmolar glucose solutions. J. Nucl. Med. 1991, 32, 377–381. [Google Scholar] [PubMed]
- Jones, K.L.; O’Donovan, D.; Russo, A.; Meyer, J.H.; Stevens, J.E.; Lei, Y.; Horowitz, M. Effects of drink volume and glucose load on gastric emptying and postprandial blood pressure in healthy older subjects. Am. J. Physiol. Gastrointest. Liver Physiol. 2005, 289, G240–G248. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Normal Weight (n = 10) | Obese (n = 11) |
|---|---|---|
| Age (years) | 27.0 (4.2) | 29.5 (4.0) |
| Weight (kg) | 66.0 (10.7) | 102.9 (15.3) * |
| BMI (kg/m2) | 22.8 (0.9) | 37.7 (5.5) * |
| Female/male | 7/3 | 10/1 |
| Race | ||
| White | 7 (70%) | 5 (45%) |
| Black | 2 (20%) | 5 (45%) |
| Other | 1 (10%) | 1 (10%) |
| Plasma concentrations | ||
| Fasting glucose (mmol/L) | 5.0 (0.3) | 5.1 (0.3) |
| Fasting insulin (pmol/L) | 38.1 (15.8) | 87.0 (35.6) * |
| HOMA-IR2 | 0.7 (0.1) | 1.7 (0.2) * |
| Prediabetes 1 | 3 (30%) | 5 (45%) |
| Measure | Normal Weight | Obese | p Value | ||||
|---|---|---|---|---|---|---|---|
| Water (n = 10) | Sucralose (n = 10) | Sham-Fed (n = 10) | Water (n = 11) | Sucralose (n = 11) | Sham-Fed (n = 9) 1 | Group X Treatment | |
| Metabolic Response | |||||||
| Incremental Peak Response | |||||||
| Glucose (mmol/L) | 5.7 ± 0.4 | 5.4 ± 0.5 | 5.5 ± 0.4 | 4.4 ± 0.4 | 4.7 ± 0.4 | 4.5 ± 0.4 | 0.27 |
| Insulin (pmol/L) * | 683 ± 130 | 548 ± 91 | 590 ± 115 | 1062 ± 124 | 1193 ± 171 | 1041 ± 184 | 0.12 |
| C-peptide (nmol/L) * | 2.8 ± 0.3 | 2.6 ± 0.3 | 2.8 ± 0.3 | 3.7 ± 0.4 | 3.9 ± 0.4 | 3.6 ± 0.3 | 0.20 |
| GIP (pmol/L) | 49.5 ± 6.8 | 45.0 ± 5.9 | 48.5 ± 5.5 | 61.9 ± 4.0 | 59.6 ± 5.2 | 56.0 ± 4.4 | 0.53 |
| iAUC | |||||||
| Glucose (mmol/L)·300 min † | 470 ± 56 | 560 ± 66 | 491 ± 60 | 380 ± 55 | 455 ± 48 | 455 ± 59 | 0.81 |
| Insulin (102 pmol/L)·300 min * | 654 ± 131 | 607 ± 102 | 597 ± 106 | 1195 ± 177 | 1400 ± 241 | 1282 ± 257 | 0.10 |
| C-peptide (nmol/L)·300 min * | 375 ± 40 | 394 ± 43 | 375 ± 45 | 502 ± 54 | 565 ± 47 | 541 ± 43 | 0.37 |
| GIP (102 pmol/L)·300 min | 67 ± 11 | 62 ± 10 | 64± 7 | 79 ± 6 | 74 ± 5 | 72 ± 7 | 0.91 |
| Glucose Kinetics | |||||||
| Peak Response | |||||||
| Total Ra (µmol/min) | 2274 ± 147 | 2313 ± 242 | 2071 ± 253 | 2576 ± 206 | 2672 ± 198 | 2552 ± 229 | 0.88 |
| Oral Ra (µmol/min) * | 2565 ± 109 | 2436 ± 154 | 2482 ± 203 | 3159 ± 217 | 3169 ± 225 | 3094 ± 244 | 0.67 |
| AUC | |||||||
| Total Ra (102 mol/min)·300 min | 3947 ± 269 | 3920 ± 296 | 4348 ± 315 | 3664 ± 85 | 3580 ± 91 | 3436 ± 95 | 0.10 |
| Oral Ra(102 mol/min)·300 min | 2884 ± 143 | 2967 ± 69 | 3405 ± 185 | 2910 ± 90 | 2928 ± 98 | 2780 ± 87 | 0.16 |
| %Total oral glucose appearing in circulation (out of 75 g) | 69.6 ± 3.5 | 71.3 ± 1.7 | 78.9 ± 4.7 | 69.7 ± 2.5 | 71.2 ± 2.8 | 71.3 ± 3.1 | 0.21 |
| Measure | Normal Weight | Obese | p Value | ||||
|---|---|---|---|---|---|---|---|
| Water (n = 10) | Sucralose (n = 10) | Sham-Fed (n = 10) | Water (n = 11) | Sucralose (n = 11) | Sham-Fed Water (n = 9) 1 | Group X Treatment | |
| β-Cell Function | |||||||
| Φtotal (109·min−1) * | 13.9 ± 0.8 | 13.6 ± 1.1 | 14.0 ± 1.0 | 23.3 ± 1.9 | 23.9 ± 1.9 | 24.1 ± 2.0 | 0.74 |
| Φdynamic (109) * | 513 ± 114 | 571±117 | 483 ± 75 | 1269 ± 201 | 936 ±148 | 977 ± 200 | 0.12 |
| Φstatic (109·min−1) * | 45.6 ± 8.3 | 43.3 ± 5.4 | 40.7 ± 5.9 | 70.2 ± 12.7 | 70.8 ± 10.4 | 63.4 ± 7.2 | 0.58 |
| Insulin Sensitivity * | |||||||
| SI [10−5 dl·kg−1·min−1/(pmol/L)] | 16.3 ± 3.0 a | 25.5 ± 6.1 b | 19.7 ± 2.9 a | 5.6 ± 0.8 c | 4.8 ± 0.7 c | 5.6 ± 0.5 c | 0.02 |
| Insulin Clearance | |||||||
| Clearance rate (L·min−1) | 1.7 ± 0.2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 1.5 ± 0.1 | 1.5 ± 0.1 | 1.5 ± 0.1 | 0.10 |
| Sucralose Kinetics | Normal-Weight | Obese |
|---|---|---|
| Peak Response (ng/mL) | 78.6 ± 8.4 | 93.2 ± 11.1 |
| Time to Peak (min) | 143 ± 19 | 194 ± 24 |
| AUC (102 ng/L·300 min) | 175 ± 19 | 176 ± 145 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nichol, A.D.; Salame, C.; Rother, K.I.; Pepino, M.Y. Effects of Sucralose Ingestion versus Sucralose Taste on Metabolic Responses to an Oral Glucose Tolerance Test in Participants with Normal Weight and Obesity: A Randomized Crossover Trial. Nutrients 2020, 12, 29. https://doi.org/10.3390/nu12010029
Nichol AD, Salame C, Rother KI, Pepino MY. Effects of Sucralose Ingestion versus Sucralose Taste on Metabolic Responses to an Oral Glucose Tolerance Test in Participants with Normal Weight and Obesity: A Randomized Crossover Trial. Nutrients. 2020; 12(1):29. https://doi.org/10.3390/nu12010029
Chicago/Turabian StyleNichol, Alexander D., Clara Salame, Kristina I. Rother, and M. Yanina Pepino. 2020. "Effects of Sucralose Ingestion versus Sucralose Taste on Metabolic Responses to an Oral Glucose Tolerance Test in Participants with Normal Weight and Obesity: A Randomized Crossover Trial" Nutrients 12, no. 1: 29. https://doi.org/10.3390/nu12010029
APA StyleNichol, A. D., Salame, C., Rother, K. I., & Pepino, M. Y. (2020). Effects of Sucralose Ingestion versus Sucralose Taste on Metabolic Responses to an Oral Glucose Tolerance Test in Participants with Normal Weight and Obesity: A Randomized Crossover Trial. Nutrients, 12(1), 29. https://doi.org/10.3390/nu12010029