Impact of Strategies for Preventing Obesity and Risk Factors for Eating Disorders among Adolescents: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Data Synthesis
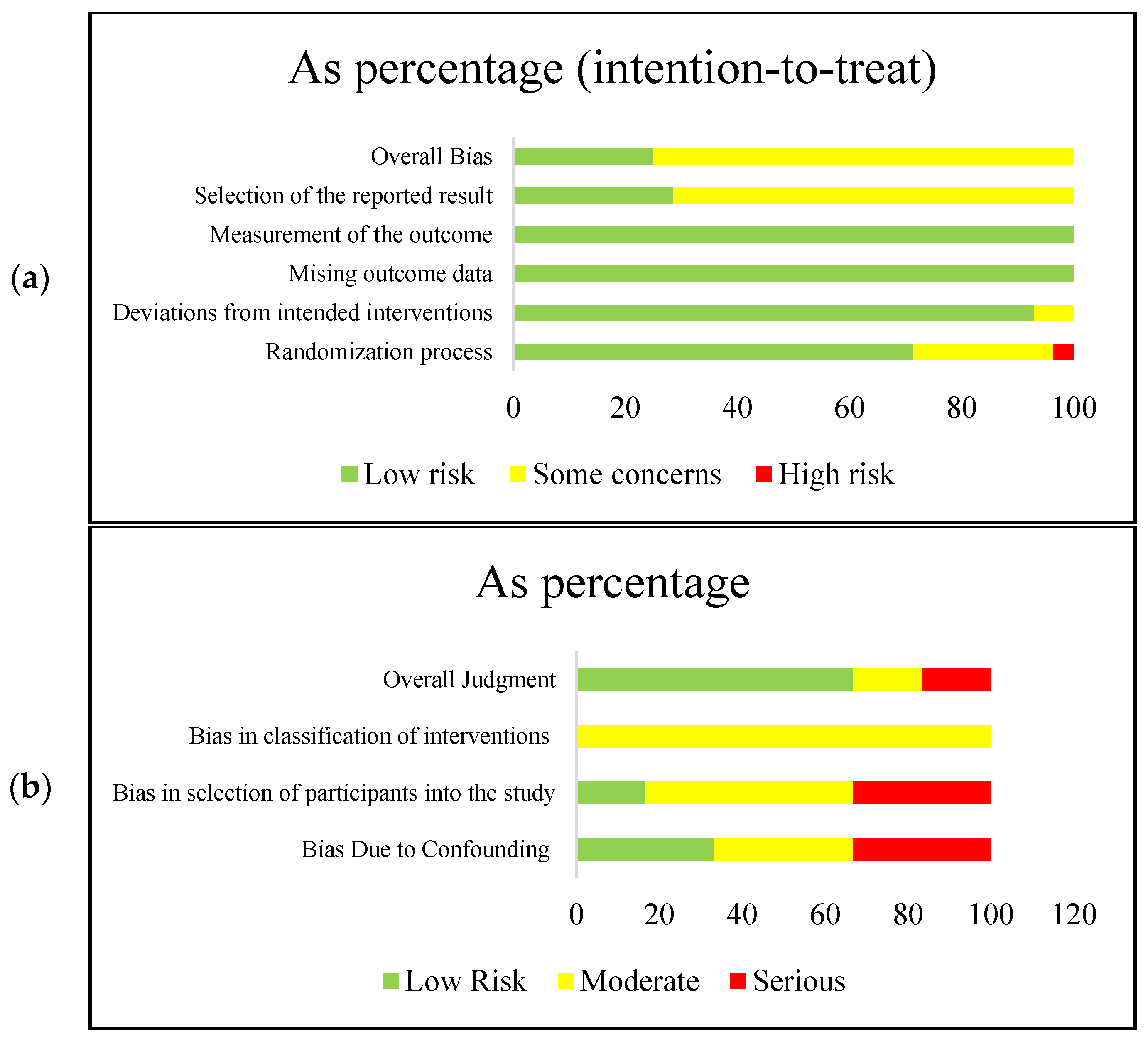
2.5. Quality Assessment and Risk of Bias
3. Results
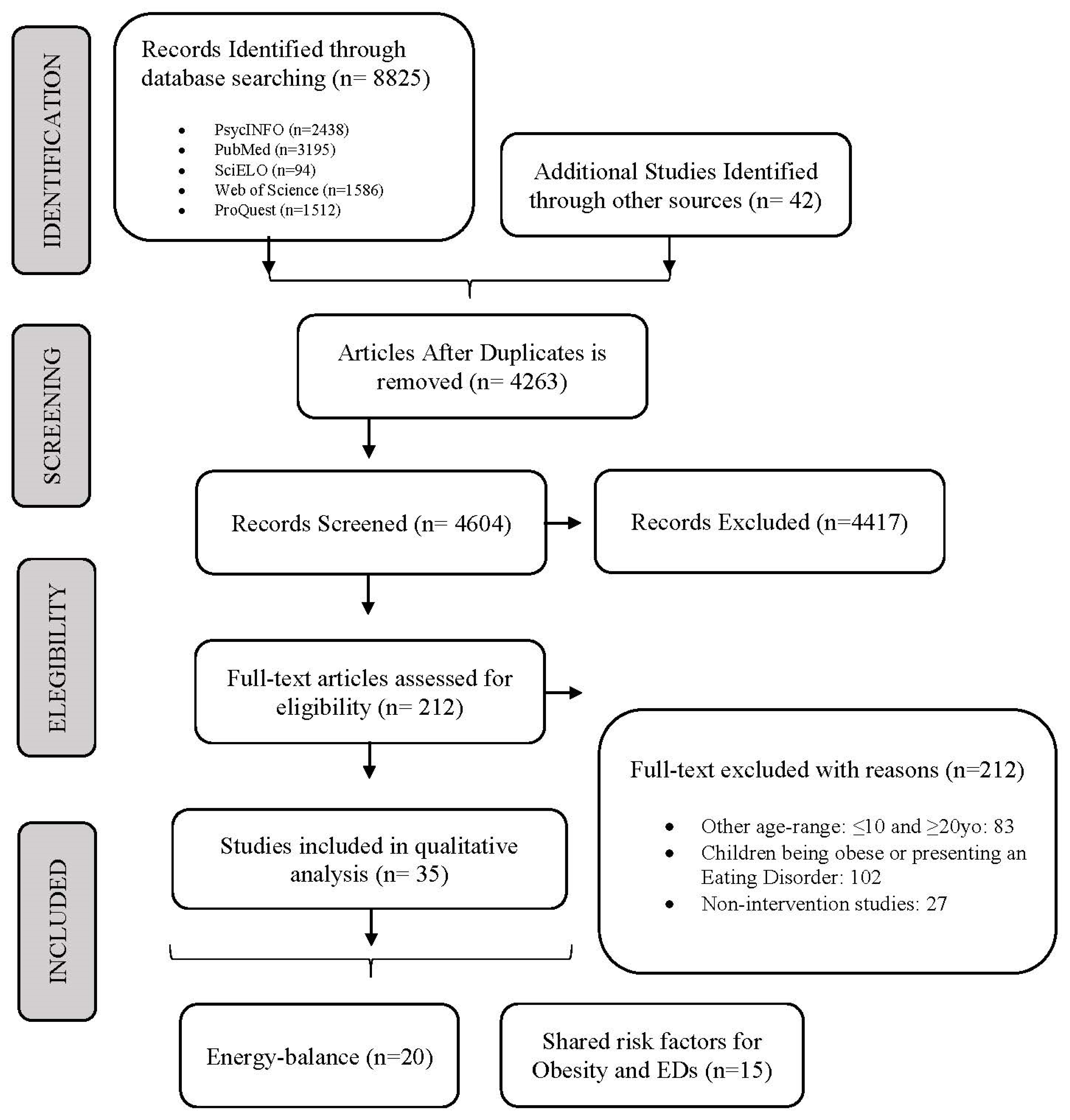
3.1. Overview of Studies
3.2. Study Characteristics
3.2.1. Energy-Balance Programs
3.2.2. Shared Risk Factors for Obesity and Eating Disorders Programs
3.3. The Studies’ Techniques
3.3.1. Energy-Balance Programs
3.3.2. Shared Risk Factors for Obesity and Eating Disorders Programs
3.4. The Studies’ Assessment Tools
3.4.1. Energy-Balance Programs
3.4.2. Shared Risk Factors for Obesity and Eating Disorders Programs
3.5. Outcomes
3.5.1. Energy-Balance Programs
3.5.2. Shared Risk Factors for Obesity and Eating Disorders Programs
4. Discussion
4.1. Combining Diet and Physical Activity Components to Promote Sustainable Lifestyle Behaviors
4.2. Maintaining Healthy Weight through Preventing Eating Disorders Risk Factors
4.3. Other Factors That May Be Associated with an Increased Risk for Eating Disorders and Obesity, Which May Be the Target for Behavioral Interventions
4.4. Caution When Targeting Other Modifiable and Non-Modifiable Risk Factors for Weight-Prevention Programs
4.5. Interventions Should Be Based on Theory and Use of Psychometric Tested Measurements
4.6. Final Thoughts on Effective Behavioral Change Interventions for Youth
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rome, E.S. Obesity prevention and treatment. Pediatr. Rev. 2011, 32, 363–373. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Pont, S.J.; Puhl, R.; Cook, S.R.; Slusser, W. Stigma experienced by children and adolescents with obesity. Pediatrics 2017, 140, e20173034. [Google Scholar] [CrossRef] [Green Version]
- Haines, J.; Neumark-Sztainer, D. Prevention of obesity and eating disorders: A consideration of shared risk factors. Health Educ. Res. 2006, 21, 770–782. [Google Scholar] [CrossRef] [Green Version]
- Leme, A.C.B.; Philippi, S.T.; Thompson, D.; Nicklas, T.; Baranowski, T. “Healthy habits, healthy girls-Brazil”: An obesity prevention program with added focus on eating disorders. Eat. Weight Disord. EWD 2019, 24, 107–119. [Google Scholar] [CrossRef]
- De Giuseppe, R.; Di Napoli, I.; Porri, D.; Cena, H. Pediatric obesity and eating disorders symptoms: The role of the multidisciplinary treatment. A systematic review. Front. Pediatr. 2019, 7, 123. [Google Scholar] [CrossRef] [Green Version]
- Fiechtner, L.; Fonte, M.L.; Castro, I.; Gerber, M.; Horan, C.; Sharifi, M.; Cena, H.; Taveras, E.M. Determinants of binge eating symptoms in children with overweight/obesity. Child. Obes. 2018, 14, 510–517. [Google Scholar] [CrossRef]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Murray, S.B.; Griffiths, S.; Mond, J.M. Evolving eating disorder psychopathology: Conceptualising muscularity-oriented disordered eating. Br. J. Psychiatry 2016, 208, 414–415. [Google Scholar] [CrossRef] [Green Version]
- Leme, A.C.B.; Thompson, D.; Lenz Dunker, K.L.; Nicklas, T.; Tucunduva Philippi, S.; Lopez, T.; Vezina-Im, L.A.; Baranowski, T. Obesity and eating disorders in integrative prevention programmes for adolescents: Protocol for a systematic review and meta-analysis. BMJ Open 2018, 8, e020381. [Google Scholar] [CrossRef] [Green Version]
- Evans, E.H.; Adamson, A.J.; Basterfield, L.; Le Couteur, A.; Reilly, J.K.; Reilly, J.J.; Parkinson, K.N. Risk factors for eating disorder symptoms at 12 years of age: A 6-year longitudinal cohort study. Appetite 2017, 108, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veses, A.M.; Martínez-Gómez, D.; Gómez-Martínez, S.; Vicente-Rodriguez, G.; Castillo, R.; Ortega, F.B.; González-Gross, M.; Calle, M.E.; Veiga, O.L.; Marcos, A. Physical fitness, overweight and the risk of eating disorders in adolescents. The AVENA and AFINOS studies. Pediatr. Obes. 2014, 9, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. Report of the Commission on Ending Childhood Obesity: Implementation Plan: Executive Summary; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Rubino, F.; Puhl, R.M.; Cummings, D.E.; Eckel, R.H.; Ryan, D.H.; Mechanick, J.I.; Nadglowski, J.; Ramos Salas, X.; Schauer, P.R.; Twenefour, D.; et al. Joint international consensus statement for ending stigma of obesity. Nat. Med. 2020, 26, 485–497. [Google Scholar] [CrossRef] [Green Version]
- Pegington, M.; French, D.P.; Harvie, M.N. Why young women gain weight: A narrative review of influencing factors and possible solutions. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2020, 21, e13002. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D. Integrating messages from the eating disorders field into obesity prevention. Adolesc. Med. State Art Rev. 2012, 23, 529–543. [Google Scholar]
- Neumark-Sztainer, D.; Levine, M.P.; Paxton, S.J.; Smolak, L.; Piran, N.; Wertheim, E.H. Prevention of body dissatisfaction and disordered eating: What next? Eat. Disord. 2006, 14, 265–285. [Google Scholar] [CrossRef]
- Jebeile, H.; Gow, M.L.; Baur, L.A.; Garnett, S.P.; Paxton, S.J.; Lister, N.B. Treatment of obesity, with a dietary component, and eating disorder risk in children and adolescents: A systematic review with meta-analysis. Obes Rev. 2019, 20, 1287–1298. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Health Topics—Adolescent Health. Available online: https://www.who.int/health-topics/adolescent-health#tab=tab_1 (accessed on 11 October 2020).
- Schoenberg, N.E.; Tarasenko, Y.N.; Snell-Rood, C. Are evidence-based, community-engaged energy balance interventions enough for extremely vulnerable populations? Transl. Behav. Med. 2018, 8, 733–738. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ (Clin. Res. Ed.) 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Clin. Res. Ed.) 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malakellis, M.; Hoare, E.; Sanigorski, A.; Crooks, N.; Allender, S.; Nichols, M.; Swinburn, B.; Chikwendu, C.; Kelly, P.M.; Petersen, S.; et al. School-Based systems change for obesity prevention in adolescents: Outcomes of the Australian capital territory “It’s Your Move!”. Aust. N. Z. J. Public Health 2017, 41, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Lubans, D.R.; Smith, J.J.; Plotnikoff, R.C.; Dally, K.A.; Okely, A.D.; Salmon, J.; Morgan, P.J. Assessing the sustained impact of a school-based obesity prevention program for adolescent boys: The ATLAS cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 92. [Google Scholar] [CrossRef] [Green Version]
- Dewar, D.L.; Morgan, P.J.; Plotnikoff, R.C.; Okely, A.D.; Collins, C.E.; Batterham, M.; Callister, R.; Lubans, D.R. The nutrition and enjoyable activity for teen girls study: A cluster randomized controlled trial. Am. J. Prev. Med. 2013, 45, 313–317. [Google Scholar] [CrossRef]
- Lubans, D.R.; Morgan, P.J.; Aguiar, E.J.; Callister, R. Randomized controlled trial of the physical activity leaders (PALs) program for adolescent boys from disadvantaged secondary schools. Prev. Med. Int. J. Devoted Pract. Theory 2011, 52, 239–246. [Google Scholar] [CrossRef]
- Wilksch, S.M.; Paxton, S.J.; Byrne, S.M.; Austin, S.B.; McLean, S.A.; Thompson, K.M.; Dorairaj, K.; Wade, T.D. Prevention across the spectrum: A randomized controlled trial of three programs to reduce risk factors for both eating disorders and obesity. Psychol. Med. 2015, 45, 1811–1823. [Google Scholar] [CrossRef] [Green Version]
- Lenz Dunker, K.L.; Claudino, A.M. Preventing weight-related problems among adolescent girls: A cluster randomized trial comparing the Brazilian ‘New Moves’ program versus observation. Obes. Res. Clin. Pract. 2018, 12, 102–115. [Google Scholar] [CrossRef]
- Sgambato, M.R.; Cunha, D.B.; da Silva Nalin Souza, B.; Henriques, V.T.; da Rocha Muniz Rodrigues, R.; Viegas Rego, A.L.; Pereira, R.A.; Yokoo, E.M.; Sichieri, R. Effectiveness of school-home intervention for adolescent obesity prevention: Parallel school-randomized study. Br. J. Nutr. 2019, 1–20. [Google Scholar] [CrossRef]
- Sánchez-Carracedo, D.; Fauquet, J.; López-Guimerà, G.; Leiva, D.; Puntí, J.; Trepat, E.; Pàmias, M.; Palao, D. The MABIC project: An effectiveness trial for reducing risk factors for eating disorders. Behav. Res. Ther. 2016, 77, 23–33. [Google Scholar] [CrossRef] [Green Version]
- González-Jiménez, E.; Cañadas, G.R.; Lastra-Caro, A.; Cañadas-De la Fuente, G.A. Efectividad de una intervención educativa sobre nutrición y actividad física en una población de adolescentes: Prevención de factores de riesgos endocrino-metabólicos y cardiovasculares. Aquichan 2014, 14, 549–559. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.; Penelo, E.; Gutierrez, T.; Raich, R.M. Disordered eating prevention programme in schools: A 30-month follow-up. Eur. Eat. Disord. Rev. 2011, 19, 349–356. [Google Scholar] [CrossRef]
- Ardic, A.; Erdogan, S. The effectiveness of the COPE healthy lifestyles TEEN program: A school-based intervention in middle school adolescents with 12-month follow-up. J. Adv. Nurs. 2017, 73, 1377–1389. [Google Scholar] [CrossRef]
- Bonsergent, E.; Agrinier, N.; Thilly, N.; Tessier, S.; Legrand, K.; Lecomte, E.; Aptel, E.; Hercberg, S.; Collin, J.-F.; Briançon, S.; et al. Overweight and obesity prevention for adolescents: A cluster randomized controlled trial in a school setting. Am. J. Prev. Med. 2013, 44, 30–39. [Google Scholar] [CrossRef]
- Jansen, W.; Borsboom, G.; Meima, A.; Joosten-Van Zwanenburg, E.; Mackenbach, J.P.; Raat, H.; Brug, J. Effectiveness of a primary school-based intervention to reduce overweight. Int. J. Pediatr. Obes. 2011, 6, e70–e77. [Google Scholar] [CrossRef]
- Simon, C.; Schweitzer, B.; Oujaa, M.; Wagner, A.; Arveiler, D.; Triby, E.; Copin, N.; Blanc, S.; Platat, C. Successful overweight prevention in adolescents by increasing physical activity: A 4-year randomized controlled intervention. Int. J. Obes. 2008, 32, 1489–1498. [Google Scholar] [CrossRef] [Green Version]
- Grydeland, M.; Bjelland, M.; Anderssen, S.A.; Klepp, K.-I.; Bergh, I.H.; Andersen, L.F.; Ommundsen, Y.; Lien, N. Effects of a 20-month cluster randomised controlled school-based intervention trial on BMI of school-aged boys and girls: The HEIA study. Br. J. Sport. Med. 2014, 48, 768. [Google Scholar] [CrossRef]
- Yang, Y.; Kang, B.; Lee, E.Y.; Yang, H.K.; Kim, H.S.; Lim, S.Y.; Lee, J.H.; Lee, S.S.; Suh, B.K.; Yoon, K.H. Effect of an obesity prevention program focused on motivating environments in childhood: A school-based prospective study. Int. J. Obes. 2017, 41, 1027–1034. [Google Scholar] [CrossRef]
- Rerksuppaphol, L.; Rerksuppaphol, S. Internet based obesity prevention program for Thai school children—A randomized control trial. J. Clin. Diagn. Res. 2017, 11, SC07–SC11. [Google Scholar] [CrossRef]
- Fotu, K.F.; Millar, L.; Mavoa, H.; Kremer, P.; Moodie, M.; Snowdon, W.; Utter, J.; Vivili, P.; Schultz, J.T.; Malakellis, M.; et al. Outcome results for the Ma’alahi Youth Project, a Tongan community-based obesity prevention programme for adolescents. Obes. Rev. 2011, 12, 41–50. [Google Scholar] [CrossRef]
- Stock, S.; Miranda, C.; Evans, S.; Plessis, S.; Ridley, J.; Yeh, S.; Chanoine, J.-P. Healthy buddies: A novel, peer-led health promotion program for the prevention of obesity and eating disorders in children in elementary school. Pediatrics 2007, 120, e1059–e1068. [Google Scholar] [CrossRef] [Green Version]
- Castillo, I.; Solano, S.; Sepulveda, A.R. A controlled study of an integrated prevention program for improving disordered eating and body image among Mexican university students: A 3-month follow-up. Eur. Eat. Disord. Rev. 2019, 27, 541–556. [Google Scholar] [CrossRef]
- Aperman-Itzhak, T.; Yom-Tov, A.; Vered, Z.; Waysberg, R.; Livne, I.; Eilat-Adar, S. School-Based intervention to promote a healthy lifestyle and obesity prevention among fifth- and sixth-grade children. Am. J. Health Educ. 2018, 49, 289–295. [Google Scholar] [CrossRef]
- Lazorick, S.; Fang, X.; Hardison, G.T.; Crawford, Y. Improved body mass index measures following a middle school-based obesity intervention-the MATCH program. J. Sch. Health 2015, 85, 680–687. [Google Scholar] [CrossRef]
- Nollen, N.L.; Mayo, M.S.; Carlson, S.E.; Rapoff, M.A.; Goggin, K.J.; Ellerbeck, E.F. Mobile technology for obesity prevention: A randomized pilot study in racial- and ethnic-minority girls. Am. J. Prev. Med. 2014, 46, 404–408. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Friend, S.; Flattum, C.; Horning, M.; Draxten, M.; Neumark-Sztainer, D.; Gurvich, O.; Story, M.; Garwick, A.; Kubik, M.Y. Promoting healthful family meals to prevent obesity: HOME Plus, a randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 154. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.J.B.; Morgan, P.J.P.; Plotnikoff, R.C.P.; Dally, K.A.P.; Salmon, J.P.; Okely, A.D.P.; Finn, T.L.; Lubans, D.R.P. Smart-Phone obesity prevention trial for adolescent boys in low-income communities: The ATLAS RCT. Pediatrics 2014, 134. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.-L.; Weiss, S.; Heyman, M.B.; Cooper, B.; Lustig, R.H. The efficacy of the web-based childhood obesity prevention program in Chinese American adolescents (Web ABC study). J. Adolesc. Health 2011, 49, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Shaw-Perry, M.; Horner, C.; Treviño, R.P.; Sosa, E.T.; Hernandez, I.; Bhardwaj, A. NEEMA: A school-based diabetes risk prevention program designed for African-American children. J. Natl. Med. Assoc. 2007, 99, 368–375. [Google Scholar]
- Neumark-Sztainer, D.R.; Friend, S.E.; Flattum, C.F.; Hannan, P.J.; Story, M.T.; Bauer, K.W.; Feldman, S.B.; Petrich, C.A. New moves-preventing weight-related problems in adolescent girls a group-randomized study. Am. J. Prev. Med. 2010, 39, 421–432. [Google Scholar] [CrossRef] [Green Version]
- Simpson, C.C.; Burnette, C.B.; Mazzeo, S.E. Integrating eating disorder and weight gain prevention: A pilot and feasibility trial of INSPIRE. Eat. Weight Disord. EWD 2019, 761–775. [Google Scholar] [CrossRef]
- Tanofsky-Kraff, M.; Shomaker, L.B.; Wilfley, D.E.; Young, J.F.; Sbrocco, T.; Stephens, M.; Brady, S.M.; Galescu, O.; Demidowich, A.; Olsen, C.H.; et al. Excess weight gain prevention in adolescents: Three-year outcome following a randomized controlled trial. J. Consult. Clin. Psychol. 2017, 85, 218–227. [Google Scholar] [CrossRef]
- Stice, E.; Rohde, P.; Shaw, H.; Marti, C.N. Efficacy trial of a selective prevention program targeting both eating disorders and obesity among female college students: 1- and 2-year follow-up effects. J. Consult. Clin. Psychol. 2013, 81, 183–189. [Google Scholar] [CrossRef] [Green Version]
- Franko, D.L.; Cousineau, T.M.; Rodgers, R.F.; Roehrig, J.P. BodiMojo: Effective Internet-based promotion of positive body image in adolescent girls. Body Image 2013, 10, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Austin, S.B.; Kim, J.; Wiecha, J.; Troped, P.J.; Feldman, H.A.; Peterson, K.E. School-Based overweight preventive intervention lowers incidence of disordered weight-control behaviors in early adolescent girls. Arch. Pediatr. Adolesc. Med. 2007, 161, 865. [Google Scholar] [CrossRef] [Green Version]
- Austin, S.B.; Field, A.E.; Wiecha, J.; Peterson, K.E.; Gortmaker, S.L. The impact of a school-based obesity prevention trial on disordered weight-control behaviors in early adolescent girls. Arch. Pediatr. Adolesc. Med. 2005, 159, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Shomaker, L.B.; Tanofsky-Kraff, M.; Matherne, C.E.; Mehari, R.D.; Olsen, C.H.; Marwitz, S.E.; Bakalar, J.L.; Ranzenhofer, L.M.; Kelly, N.R.; Schvey, N.A.; et al. A randomized, comparative pilot trial of family-based interpersonal psychotherapy for reducing psychosocial symptoms, disordered-eating, and excess weight gain in at-risk preadolescents with loss-of-control-eating. Int. J. Eat. Disord. 2017, 50, 1084–1094. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Simpson, K.; Parker, B.; Capizzi, J.; Thompson, P.; Clarkson, P.; Freedson, P.; Pescatello, L.S. Validity and reliability question 8 of the Paffenbarger Physical Activity Questionnaire among healthy adults. J. Phys. Act. Health 2015, 12, 116–123. [Google Scholar] [CrossRef]
- Trott, M.; Jackson, S.E.; Firth, J.; Jacob, L.; Grabovac, I.; Mistry, A.; Stubbs, B.; Smith, L. A comparative meta-analysis of the prevalence of exercise addiction in adults with and without indicated eating disorders. Eat. Weight Disord. 2020, 1–10. [Google Scholar] [CrossRef]
- Stice, E.; Fisher, M.; Martinez, E. Eating disorder diagnostic scale: Additional evidence of reliability and validity. Psychol. Assess. 2004, 16, 60–71. [Google Scholar] [CrossRef] [Green Version]
- Goldfein, J.A.; Devlin, M.J.; Kamenetz, C. Eating Disorder Examination-Questionnaire with and without instruction to assess binge eating in patients with binge eating disorder. Int. J. Eat. Disord. 2005, 37, 107–111. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Thompson, J.K.; van den Berg, P.; Roehrig, M.; Guarda, A.S.; Heinberg, L.J. The sociocultural attitudes towards appearance scale-3 (SATAQ-3): Development and validation. Int. J. Eat. Disord. 2004, 35, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.K.; Cattarin, J.; Fowler, B.; Fisher, E. The Perception of Teasing Scale (POTS): A revision and extension of the Physical Appearance Related Teasing Scale (PARTS). J. Personal. Assess. 1995, 65, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Frijters, J.E.R.; van Staveren, W.A.; Defares, P.B.; Deurenberg, P. The predictive validity of the Dutch Restrained Eating Scale. Int. J. Eat. Disord. 1986, 5, 747–755. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A. Affects Separable and Inseparable: On the Hierarchical Arrangement of the Negative Affects. J. Personal. Soc. Psychol. 1996, 62, 489–505. [Google Scholar] [CrossRef]
- Lacey, J.; Lomax, A.J.; McNeil, C.; Marthick, M.; Levy, D.; Kao, S.; Nielsen, T.; Dhillon, H.M. A supportive care intervention for people with metastatic melanoma being treated with immunotherapy: A pilot study assessing feasibility, perceived benefit, and acceptability. Support. Care Cancer 2019, 27, 1497–1507. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Tzanninis, S.; Ntanasis-Stathopoulos, I.; Panotopoulos, G.; Kostopoulou, M.; Tzanninis, I.G.; Tsagianni, A.; Sergentanis, T.N. Prevention and treatment of childhood and adolescent obesity: A systematic review of meta-analyses. World J. Pediatr. 2019, 15, 350–381. [Google Scholar] [CrossRef]
- Morillo Sarto, H.; Barcelo-Soler, A.; Herrera-Mercadal, P.; Pantilie, B.; Navarro-Gil, M.; Garcia-Campayo, J.; Montero-Marin, J. Efficacy of a mindful-eating programme to reduce emotional eating in patients suffering from overweight or obesity in primary care settings: A cluster-randomised trial protocol. BMJ Open 2019, 9, e031327. [Google Scholar] [CrossRef]
- Bullivant, B.; Rhydderch, S.; Griffiths, S.; Mitchison, D.; Mond, J.M. Eating disorders “mental health literacy”: A scoping review. J. Ment. Health 2020, 29, 336–349. [Google Scholar] [CrossRef]
- Philippi, S.T.; Leme, A.C.B. Weight-Teasing: Does body dissatisfaction mediate weight-control behaviors of Brazilian adolescent girls from low-income communities? Cad. Saude Publica 2018, 34, e00029817. [Google Scholar] [CrossRef]
- Rzepa, S.; Weissman, M. Social Adjustment Scale Self-Report (SAS-SR). Encycl. Qual. Life Well-Being Res. 2014, 6017–6021. [Google Scholar] [CrossRef]
- Gunlicks-Stoessel, M.; Mufson, L.; Jekal, A.; Turner, J.B. The impact of perceived interpersonal functioning on treatment for adolescent depression: IPT-A versus treatment as usual in school-based health clinics. J. Consult. Clin. Psychol. 2010, 78, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Goldschmidt, A.B.; Aspen, V.P.; Sinton, M.M.; Tanofsky-Kraff, M.; Wilfley, D.E. Disordered eating attitudes and behaviors in overweight youth. Obesity 2008, 16, 257–264. [Google Scholar] [CrossRef]
- Pena-Romero, A.C.; Navas-Carrillo, D.; Marin, F.; Orenes-Pinero, E. The future of nutrition: Nutrigenomics and nutrigenetics in obesity and cardiovascular diseases. Crit. Rev. Food Sci. Nutr. 2018, 58, 3030–3041. [Google Scholar] [CrossRef]
- Hauck, C.; Cook, B.; Ellrott, T. Food addiction, eating addiction and eating disorders. Proc. Nutr. Soc. 2020, 79, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.Y.; Yin, W.Q.; Sun, H.W.; Yang, S.X.; Li, X.Y.; Liu, H.Q. The association between disordered eating and health-related quality of life among children and adolescents: A systematic review of population-based studies. PLoS ONE 2019, 14, e0222777. [Google Scholar] [CrossRef]
- Andersson, M.A.; Harkness, S.K. When do biological attributions of mental illness reduce stigma? Using qualitative comparative analysis to contextualize attributions. Soc. Ment. Health 2017, 8, 175–194. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Sittig, S.; McGowan, A.; Iyengar, S. Extensive review of persuasive system design categories and principles: Behavioral obesity interventions. J. Med. Syst. 2020, 44, 128. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Story, M.; Hannan, P.J.; Rex, J. New Moves: A school-based obesity prevention program for adolescent girls. Prev. Med. 2003, 37, 41–51. [Google Scholar] [CrossRef]
- Leme, A.C.; Philippi, S.T. Cultural adaptation and psychometric properties of social cognitive scales related to adolescent dietary behaviors. Cad. Saúde Coletiva 2014, 22, 252–259. [Google Scholar] [CrossRef]
- McCabe, B.E.; Plotnikoff, R.C.; Dewar, D.L.; Collins, C.E.; Lubans, D.R. Social cognitive mediators of dietary behavior change in adolescent girls. Am. J. Health Behav. 2015, 39, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Dewar, D.L.; Plotnikoff, R.C.; Morgan, P.J.; Okely, A.D.; Costigan, S.A.; Lubans, D.R. Testing social-cognitive theory to explain physical activity change in adolescent girls from low-income communities. Res. Q. Exerc. Sport 2013, 84, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Barnett, A.; Baranowski, T. Testing theories of dietary behavior change in youth using the mediating variable model with intervention programs. J. Nutr. Educ. Behav. 2009, 41, 309–318. [Google Scholar] [CrossRef]
- Irving, L.M.; Neumark-Sztainer, D. Integrating the prevention of eating disorders and obesity: Feasible or futile? Prev. Med. 2002, 34, 299–309. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |



{kind=link}
{kind=link}
| Studies | Intervention Name (Country) | Study Design | Sample Characteristics | Strategy and Techniques |
|---|---|---|---|---|
| Shared Risk Factors for Obesity and Eating Disorders Programs | ||||
| Simpson et al. 2019 [52] | INSPIRE (USA) | One-group pre-post-design | 27 female adolescents (M = 18.6 ± SD 1.01 years old) | Dissonance-based intervention + healthy weight + dialectical behavioral therapy. |
| Leme et al., 2019 [5] | Healthy Habits, Healthy Girls—Brazil (Brazil) | Randomized controlled trial with post- and 6-month | 253 adolescent girls (M = 16.1 ± SE 0.1 years old); 142 in intervention group | Social Cognitive Theory. |
| Achieve sustainable diet and physical activity behaviors, and decrease risk factors for eating disorders. | ||||
| Castillo et al. 2019 [43] | No intervention name (Mexico) | Three-arm quasi experimental study with post and 3-month follow-up | 361 adolescent girls (M = 19.78 ± 2.06 years old); 133 in experimental group; 105 in control skills group and 123 non-intervention group | Cognitive Dissonance and Constructivist Approach. |
| Raise awareness to beauty standards and perpetuated by the mass media. | ||||
| Increase physical activity and healthy eating. | ||||
| Improve self-esteem, build positive self-concept, and reduce extreme perfectionism, and resolve conflicts. | ||||
| Lenz and Claudino et al. 2018 [29] | Adaption of the US New Moves (Brazil) | Randomized Controlled trial with post- and 6-month follow-up. | 270 adolescent girls (M = 13.4 ± 0.64 years old) with 139 in intervention group. | Social Cognitive Theory. |
| Address issues related to female adolescents to promote health. | ||||
| Shomaker et al. 2017 [58] | No intervention name (USA) | Randomized Controlled trial with post-intervention, 6 month and 1-year follow-up | 29 pre-adolescents (M = 11.7 ± 1.6 years old) with 15 in intervention group. | Family-Based Interpersonal Therapy. |
| Psycho-education on interpersonal model of loss of control-eating and general skill-building applied to improve communication, increase support, and resolve conflict between parent and child. | ||||
| Sánchez-Carracedo et al. 2016 [31] | The MABIC Project (Spain) | Non-randomized controlled trial with post- and 1-year follow-up. | 565 adolescent girls (M= 13.8 ± 0.5 years old) with 152 in intervention group. | Social Cognitive Theory, Media Literacy Education Approach, and Cognitive Dissonance Theory. |
| Increase knowledge through sessions of the practical and relevant aspects of foods. | ||||
| Wilksch et al. 2015 [28] | No intervention name (Australia) | Four-arm randomized controlled trial with post, intervention, 6-month and 12-month follow-up. | 1316 adolescents (M = 13.21 ± 0.68 years old) with 269 in media smart, 347 in life smart and 225 HELPP group. | Principles of media internalization (Media Smart group). |
| Principles that health is more than weight (Life Smart group). | ||||
| Principles of eating disorder risk factors of internalization of social appearance ideals and comparisons. | ||||
| Evidence principles of being interactive, avoiding psychoeducation on weight-related concerns and with multiple sessions. | ||||
| Stice et al. 2013 [54] | Healthy Weight 2 (USA) | Randomized controlled trial post-, 6 month, 1-year and 2-year follow-up. | 398 young adults (M = 18.4, 17–20 years old) with 192 in intervention group. | Healthy weight approach to reduce eating disorders and obesity. |
| Nutrition science principles for health behavior changes. | ||||
| Franko et al. 2013 [55] | BodyMojo (USA) | Randomized controlled trial with 4–6 weeks and 3-month follow-up. | 65 boys (M = 15.4 ± 1.4 years old) and 113 girls (M = 15.2 ± 0.3 years old), randomized in classes. | Socio-Cognitive Theory, Health Belief Model, Theory of Planned Behavior, Transtheoretical Model. |
| Internet-based program for health behavior change through technology and social engagement, offering a personalized experience, goal setting, and interactive games and videos. | ||||
| Gonzalez et al. 2011 [33] | No intervention name (Spain) | Three arms quasi-experimental design with post-intervention, 6 and 30-month follow-up. | 443 adolescents (M = 13.5 ± 0.4 years old) with 143 media literacy and 99 media literacy and nutrition. | Social Cognitive Theory. |
| Focus on media literacy to increase nutrition awareness. | ||||
| Interactive format, sessions, and new activism and media literacy components. | ||||
| Critical thinking and promotion of health and well-being to develop resilience for sociocultural messages. | ||||
| Neumark-Sztainer et al. 2010 [51] | New Moves (USA) | Randomized controlled trial with post and 9-month follow-up. | 356 adolescent girls (M = 15.8 ± 1.2 years old) with 182 in intervention group. | Social Cognitive Theory and Transtheoretical Model. |
| Socio-environmental, personal, and behavioral factors for changes in diet, physical activity, and weight-control behaviors. | ||||
| Stock et al. 2007 [42] | Healthy Bodies (Canada) | Prospective pilot study with post-intervention. | 199 adolescents (4th to 7th grade) with 128 in intervention group. | Prescribed learning outcomes from the British Columbia Minister of Health. |
| 3 main components of healthy living: be physical activity, eat healthy, and positive body image. | ||||
| 21 lessons over the study school year. | ||||
| Austin et al. 2007 [56] | The 5-2-1 go! (USA) | Randomized controlled trial with post intervention. | 1451 adolescents (6th and 7th grade) with 614 in intervention group. | Learning outcomes from previous trial (Planet Girls). |
| Multiple modules in schools to address nutrition and physical activity in various domains: nutrition services, physical education, and policies and environment. | ||||
| Austin et al. 2005 [57] | Planet Health (USA) | Randomized controlled trial with post-and 21-month follow-up. | 480 adolescent girls (M = 11.5 ± 0.7 years old) with 254 in intervention group | Social Cognitive Theory. |
| Interdisciplinary curriculum with materials integrated in major subject areas and physical education classes via grade- and subject appropriate skills and competencies. | ||||
| Energy-Balance Programs | ||||
| Sgambato et al. 2019 [30] | PAAPPAS—“Parents, Students, Community Health Agents and teachers for Healthy Eating” (Brazil) | Randomized controlled trial with post-interventions | 2447 adolescents (M = 11.5 ± 1.4 years old) with 1290 in intervention group. | Family Health System. |
| Reduce weight gain at school and home environments. | ||||
| Aperman-Itzhak et al. 2018 [44] | No intervention name (Israel) | Controlled, non-randomized and non-blinded trial with post-intervention | 373 adolescents (10–12 years old) with 187 in intervention group. | Program developed by a registered dietitian and cardiologist. |
| Promote healthy eating and physical activity, integrating the head of the local council stakeholders and school teachers | ||||
| Yang et al. 2017 [39] | No intervention name (South Korea) | Quasi-experimental trial with 1-year follow-up | 768 adolescents (M = 11.0 ± 1.5 years old) with 418 in intervention group. | Based on pre-intervention results + personalized suggestions for improving physical strength and dietary intake. |
| School-based interventions with continuation in the community. | ||||
| Rerksuppaphol and Rerksuppaphol 2017 [40] | No intervention name (Thailand) | Randomized controlled trial with post-intervention. | 217 adolescents (M = 10.7 ± 3.1 years old) with 111 in intervention group. | Internet-based obesity program. |
| Information on health nutrition, food habits, and physical activity included in text and graphics. | ||||
| Participants collect their weight and height and interpreted their weight status. | ||||
| Malakellis et al. 2017 [24] | It’s Your Move—ACT IYM (Australia) | Quasi-experimental trial with 2-year follow-up. | 880 adolescents (12–16 years old) with 628 in intervention group. | ANGELO framework—identify and prioritize key determinants, considering gaps in knowledge community capacity, culturally specific needs, and current health promotion. |
| Changes in school and community-based environment. | ||||
| Ardic and Erdogan 2017 [34] | COPE Healthy lifestyles teen program (Turkey) | Quasi-experimental trial with post and 12-month follow-up. | 100 adolescents (M = 12.8 ± 0.8 years old) with 50 in intervention group. | Adaptation of US study (COPE). |
| Cognitive behavioral skill building. | ||||
| Educational information for healthy lifestyle. | ||||
| Lubans et al. 2016 [25] | ATLAS Boys (Australia) | Randomized controlled trial with post, 8- and 18-month follow-up. | 361 adolescent boys (M = 12.7 ± 0.5 years old) with 181 in intervention group. | Self-Determination and Social Cognitive Theory. |
| Increase autonomy, competence, and relatedness to improve autonomous motivation for leisure time physical activity and school sports. | ||||
| Fulkerson et al. 2015 [47] | Home Plus (USA) | Randomized controlled trial with 12- and 21-month follow-up. | 149 families (children M = 10.3 ± 1.4 and; parents M = 41.6 ± 7.6 years old) with 74 families in intervention group. | Social Cognitive Theory and Social Ecological Model. |
| Family changes on planning, frequency, and healthiness of family meals and snacks (limiting meals related to screen-time). | ||||
| Lazorick et al. 2015 [45] | MATCH (USA) | Randomized controlled trial with post-intervention follow-up. | 362 adolescents (M = 13.1 ± 0.5 years old) with 189 in intervention group. | Social Cognitive Theory and Self-Determination Theory. |
| Education and behavioral curriculum (school). | ||||
| Lessons delivered in sequence of a planned manner, repeated key concepts, and applied enhance skills for healthy choices. | ||||
| González-Jiménez et al. 2014 [32] | No intervention name (Spain) | One group, pre post-test design | 91 adolescents (15–17 years old) | Knowledge education program to reduce weight gain. |
| Three workshops on healthy eating. | ||||
| Activities during physical education classes | ||||
| Grydeland et al. 2014 [38] | HEIA Study (Norway) | Randomized controlled trial with 2-month follow-up | 1485 adolescents (M = 11.2 ± 0.3 years old) with 465 in intervention group. | Social Ecological Framework. |
| Multiple components for health promotion to increase awareness and physical activity, and reduce screen-time. | ||||
| Nollen et al. 2014 [46] | No intervention name (USA) | Randomized controlled trial with post, 8-week and 12-week follow-up. | 51 adolescent girls (M = 11.3 ± 1.6 years old) with 26 in intervention group. | Mobile technology with four-week 3 modules: to improve fruit and vegetable and sugar-sweetened beverages intake and screen-time. |
| Dewar et al. 2013 [26] | NEAT Girls (Australia) | Randomized controlled trial with 12- and 24-month follow-up. | 357 adolescent girls (M = 13.2 ± 0.5 years old) with 178 in intervention group. | Social Cognitive Theory. |
| Range of strategies to promote lifestyle and lifetime physical activity, improve diet intake, and reduce time on screens. | ||||
| Bonsergent et al. 2013 [35] | PRALIMAP trial (France) | Randomized Controlled trial with mid- and post-intervention follow-up. | 3538 adolescents (M = 15.6 ± 0.7 years old) with 1949 in education strategy and 1589 in non-education strategy. Education was divided in environmental with 1029 and non-environmental with 920 individuals. Non-education divided in environmental with 699 and non-environmental with 890 individuals. | Personal skills were used for educational strategy, detection of weight-related problems, and proposing a care model for a screening strategy and favorable and supportive environment for environmental strategy. |
| * Screening = non-education | ||||
| Lubans et al. 2011 [27] | Physical Activity Leaders—PAL (Australia) | Randomized controlled trial with 3- and 6-month follow-up. | 100 adolescents (M = 14.3 ± 0.6 years old) with 50 in intervention group. | Social Cognitive Theory. |
| Promotion of lifestyle and lifetime activities. | ||||
| Jansen et al. 2011 [36] | Lekker Fit (Enjoy being fit) (The Netherlands) | Randomized controlled trial with post-intervention. | 1236 adolescents (M = 10.8 ± 1.0 years old) with 583 in intervention group. | Theory of Planned Behavior. |
| ANGELO framework (identify and prioritize environmental determinants). | ||||
| Intervention targeted individual behaviors, school policies, and curriculum. | ||||
| Fotu et al. 2011 [41] | Ma’alahi Youth Project (Tonga) | Quasi-experimental design with 3-year follow-up | 1712 adolescents (M = 14.8 ± 1.9 years old) with 897 in intervention group. | Develop on communities the capacity to build on their own promotion for a healthy lifestyle. |
| Social marketing approaches, community capacity building, and grass-roots activities. | ||||
| Chen et al. 2011 [49] | WEB ABC study (USA) | Randomized controlled trial with 2-, 6- and 8-month follow-up | 63 adolescents (M = 12.5 ± 3.2 years old) with 27 in intervention group | Transtheoretical Model and Social Cognitive Theory. |
| Web-based program to enhance diet and physical activity self-efficacy, ease comprehension, and use problem solving skills. | ||||
| Simon et al. 2008 [37] | No intervention name (France) | Randomized controlled trial with post and 4-year follow-up. | 954 adolescents (M = 11.6 ± 0.6 years old) with 475 in intervention group | Multilevel theory-based. |
| Provide environment institutional conditions to promote health use knowledge and skills acquired. | ||||
| Changes attitudes towards health and social support from parents and educators. | ||||
| Shaw-Peri et al. 2007 [50] | NEEMA (USA) | One-group with pre-post design. | 269 adolescents (M = 10.5 ± 0.7 years old) | Based on the learning outcomes of a previous study reporting increased risk for diabetes type 2. |
| Changes in social structures to promote physical activity, fiber intake, and reduce saturated fat, sugar, and sedentary time. | ||||
| Author, Publication Year | Assessment at Follow-Up | Summary of Main Results |
|---|---|---|
| Shared Risk Factors for Obesity and Eating Disorders Studies | ||
| Simpson et al. 2019 [52] | Eating disorders symptoms/Body shape satisfaction. Emotion regulation. Positive/negative affect. Weight status. Diet intake. Physical activity. | ↓eating pathology, eating satisfaction, thin-ideal internalization, restrained eating, negative affect, emotion dysregulation. ↓ fat intake. No significant increase in BMI. Acceptable and feasible. |
| Leme et al. 2019 [5] | Body and shape satisfaction. Weight-control behaviors. Weight stigma. Social cognitive aspects of diet and PA. Diet intake. Physical activity. Weight status. | No significant decrease in BMI. Increase in waist circumference. Week and weekends decrease time on screens. Weekends increase vegetables intake. Social support and strategies were improved. Unhealthy weight was increased (favoring intervention group). |
| Castillo et al. 2019 [43] | Body and weight image. Risk factors for eating disorders. Emotion regulation. Sex-specific image concerns. Physical Activity. Weight status. | Male students did not present any significant effect. Girls improved significant for thin-ideal internalization and disordered eating attitudes. |
| Dunker and Claudino 2018 [29] | Body image. Emotional regulations. Weight status. | No significant results for any eating disorders risk factors. Participants’ low adherence in the program. |
| Shomaker et al. 2017 [58] | Weight status and body fat. Risk factors for eating disorders. Emotional regulation. Positive/negative affect. | Intervention was feasible and acceptable. Benefits to social interactions and eating. Family-based interpersonal therapy improved depression and anxiety, and loss of control compared to health education (control). Family-based interpersonal therapy reduced disordered eating attitudes. No significant differences in BMI |
| Sanchez-Carracedo et al. 2016 [31] | Risk for eating disorders. Body image concern. Emotional regulations. Weight status and body fat. Diet intake. Physical activity. | Media Smart and HELPP were less concerned about their shape and weight compared to control girls. Media Smart and control had less eating concerns and pressure than HELPP girls. Media Smart and HELPP benefitted from media internalization compared to control boys. Media Smart had more physical activity than HELPP and control participants. Media Smart had less time spent on screens than control participants. |
| Wilksch et al. 2015 [28] | Weight status Risk for eating disorders. Body image concern. Emotional regulations. Weight status and body fat. Diet intake. Physical activity. | Intervention group reduced body dissatisfaction and eating disorders symptoms. No effects for BMI, depressive symptoms, dieting, energy intake, and physical activity. |
| Stice et al. 2013 [54] | Risk factors for eating disorders. Body image concern. Emotion regulation. | Intervention decreased body image concerns compared to control girls (but not sustained over a 3-month follow-up). Among boys there were no significant differences between intervention and control groups. |
| Franko et al. 2013 [55] | Weight status. Risk factors for eating disorders. Body image concern. | Prevention presented lower risk factors for eating disorders and body image concern than the control group. |
| Gonzalez et al. 2011 [33] | Weight status and body fat %. Physical activity. Diet intake. Body image concern. Weight control behaviors. Social cognitive aspects of health. | No significant differences in BMI. Improvement in screen-time, diet intake, weight-control behaviors, and body image. Friends, teachers and family support for diet and physical activity behaviors. |
| Neumark-Sztainer et al. 2010 [51] | Weight status. Cardiovascular markers. Physical fitness. Knowledge on behavior and attitudes towards health behaviors. Emotional regulation. Body image concern. Risk for eating disorders. | BMI and weight decreased. Improvement in health knowledge: body image, eating disorders risk factors, physical activity and diet. Increase in systolic blood pressure. |
| Stock et al. 2007 [42] | Weight control behaviors. Diet intake. Physical activity. Weight status and body fat %. | Girls reported less weight-control behaviors after intervention. No significant differences for boys. |
| Austin et al. 2007 [56] | Weight control behaviors. Diet intake. Physical activity. Weight status and body fat %. | Girls reported less purging and using diet pills to control weight from both intervention and control groups. |
| Austin et al. 2005 [57] | Eating disorders symptoms/Body shape satisfaction. Emotion regulation. Positive/negative affect. Weight status. Diet intake. Physical activity. | ↓eating pathology, eating satisfaction, thin-ideal internalization, restrained eating, negative affect, emotion dysregulation. ↓ fat intake. No significant increase in BMI. Acceptable and feasible. |
| Energy-Balance Programs | ||
| Sgambato et al. 2019 [30] | Diet intake. Physical Activity. Health knowledge, attitudes and behaviors. Weight status and body fat %. | Weight status increased in the intervention group. Small decrease in body fat %. No significant differences on daily frequency intake of foods. Physical activity increased in the intervention group. 30% of the sample was analyzed using a 24 h Recall and significantly decrease fruit juice in the intervention group. |
| Aperman-Itzhak et al. 2018 [44] | Weight status, waist circumference, and body fat %. Blood pressure. Physical fitness. Health behaviors: physical activity, sleep, and diet intake. Nutrition knowledge. Body image. Emotion regulations. Parents’ obesity social-determinants aspects. | Overweight and obesity decreased only in the intervention group. Religious children have increased risk for being overweight. Knowledge improved in the intervention and control groups. |
| Yang et al. 2017 [39] | Weight status, body fat %. Blood pressure. Physical fitness. | No significant difference in overweight incidence between the intervention and control groups. Intervention decreased BMI, height, body fat %, and increased muscular fitness compared to the control group. Blood pressure was significantly reduced, mainly in those with higher BMI, boys, and older children. Physical fitness was improved. Normal weight boys and younger individuals showed better weight-related outcomes. |
| Rerksuppaphol and Rerksuppaphol 2017 [40] | Weight status. | Control showed an increased in overweight and BMI compared to the intervention group. |
| Malakellis et al. 2017 [24] | Weight status. Health knowledge, attitudes and behaviors. Environment perceptions (home, school, and neighborhood). Emotional regulations. | Two of three intervention schools decreased the prevalence of overweight. |
| Ardic and Erdocan 2017 [34] | Weight status. Physical activity (daily steps). Diet and water intake. Nutrition and physical activity knowledge. Emotional regulations. | Intervention group improve diet, physical activity, and stress management. Increased number of daily steps/weeks, fruit and vegetables, and water intake. Knowledge about nutrition and physical activity was improved. Anxiety levels and BMI were reduced, but effects were not significant. |
| Lubans et al. 2016 [25] | Weight status and waist circumference. Physical activity and sedentary behaviors. Sugar-sweetened beverages intake. Muscular fitness and resistance training skills. School sports motivation regulation. | No significant effect for BMI, waist circumference, and body fat %. No significant effect for physical activity. Screen-time, sugar-sweetened beverages, muscular fitness, and resistance training were improved. |
| Lazorick et al. 2015 [45] | Weight status. Physical fitness. Diet intake. Physical activity and sedentary behaviors. Sleep behaviors. | MATCH significant decreased BMI compared to the control group. Subgroup analysis showed decreased among overweight and obese participants. Lifestyle behaviors were not significant. |
| Fulkerson et al. 2015 [47] | Weight status. Pubertal development scale. Family dinner frequency. | No significant difference in BMI; but promising reduction in excess weight gain. Subgroup analysis showed that pre-pubescent children showed lower BMI in the intervention group. |
| Gonzalez-Jimenez et al. 2014 [32] | Weight status, waist circumference, and waist-to-hip ratio. Pubertal category scores | Weight status was improved. Significant results for diet intake. No significant results for physical activity. |
| Nollen et al. 2014 [46] | Home availability of fruit and vegetables, sugar-sweetened beverages, and screen devices. Diet intake. Screen-time behaviors. | Mobile technology used the program about 63% of days compared to the control girls. Non-significant increase in fruit and vegetables and decrease in sugar-sweetened beverage intake. No significant differences for BMI and screen-time use. |
| Dewar et al. 2013 [26] | Weight status and body fat %. Physical activity and sedentary behaviors. Diet intake. | Non-significant effect on the decrease for BMI and body fat % between the intervention and control groups. Screen-time was significantly reduced. No significant effect for physical activity, diet intake, and self-esteem. |
| Bonsergent et al. 2013 [35] | Weight status. Emotional regulations. Risk factors for eating disorders. | Screening improved the BMI and decreased the overweight incidence compared to the non-screening strategy. Education and environment strategies were less effective. |
| Lubans et al. 2011 [27] | Weight status, body fat %, and waist circumference. Physical fitness. Physical activity. Fruit and vegetables, sugar-sweetened beverages, and water intake. | Significant effect in BMI and body fat %. No significant effect for waist circumference, muscular fitness, and physical activity. Adolescents reported less intake on sugar-sweetened beverages after intervention. |
| Jansen et al. 2011 [36] | Weight status and waist circumference. Physical fitness. | Overweight increased at both the intervention and control groups. No significant effects for BMI. |
| Fotu et al. 2011 [41] | Weight status and body fat %. Diet intake. Physical activity. | Increased in overweight prevalence. Intervention group decrease body fat %. Diet and physical activity were not improved. |
| Chen et al. 2011 [49] | Weight status and waist-to-hip ratio. Blood pressure. Diet and physical activity knowledge and self-efficacy. Diet intake. Physical activity. | Waist-to-hip ratio and diastolic blood pressure were decreased. Fruit and vegetables intake, and physical activity were improved. Nutrition and physical activity knowledge improved. |
| Grydeland et al. 2014 [38] | Weight status, waist circumference, and waist-to-hip circumference. | Effects on BMI only for girls. Beneficial effect for BMI in participants with high educated parents. Negative effects for waist-to-hip ratio in participants with low educated parents. No significant for waist circumference and weight status. |
| Simon et al. 2008 [37] | Weight status. Physical activity. Plasma lipids. | Intervention lower increased in BMI than control groups. Intervention better effect on non-overweight students. Non-significant differences in overweight students. Intervention improved supervised PA, screen-time, and HDL-c. |
| Shaw-Peri et al. 2007 [51] | Weight status and % body fat. Plasma glucose. | Fitness laps, fasting glucose, and % body fat improved by the end of the study. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leme, A.C.B.; Haines, J.; Tang, L.; Dunker, K.L.L.; Philippi, S.T.; Fisberg, M.; Ferrari, G.L.; Fisberg, R.M. Impact of Strategies for Preventing Obesity and Risk Factors for Eating Disorders among Adolescents: A Systematic Review. Nutrients 2020, 12, 3134. https://doi.org/10.3390/nu12103134
Leme ACB, Haines J, Tang L, Dunker KLL, Philippi ST, Fisberg M, Ferrari GL, Fisberg RM. Impact of Strategies for Preventing Obesity and Risk Factors for Eating Disorders among Adolescents: A Systematic Review. Nutrients. 2020; 12(10):3134. https://doi.org/10.3390/nu12103134
Chicago/Turabian StyleLeme, Ana Carolina B., Jess Haines, Lisa Tang, Karin L. L. Dunker, Sonia T. Philippi, Mauro Fisberg, Gerson L. Ferrari, and Regina M. Fisberg. 2020. "Impact of Strategies for Preventing Obesity and Risk Factors for Eating Disorders among Adolescents: A Systematic Review" Nutrients 12, no. 10: 3134. https://doi.org/10.3390/nu12103134
APA StyleLeme, A. C. B., Haines, J., Tang, L., Dunker, K. L. L., Philippi, S. T., Fisberg, M., Ferrari, G. L., & Fisberg, R. M. (2020). Impact of Strategies for Preventing Obesity and Risk Factors for Eating Disorders among Adolescents: A Systematic Review. Nutrients, 12(10), 3134. https://doi.org/10.3390/nu12103134