Effects of Cocoa Polyphenols and Dark Chocolate on Obese Adults: A Scoping Review

 ,
, 
Abstract
1. Introduction
2. Method
2.1. Identifying Research Question
2.2. Identifying Relevant Literature
2.3. Selecting Literature
2.4. Charting Data
2.5. Collating, Summarizing, and Reporting Results
3. Results
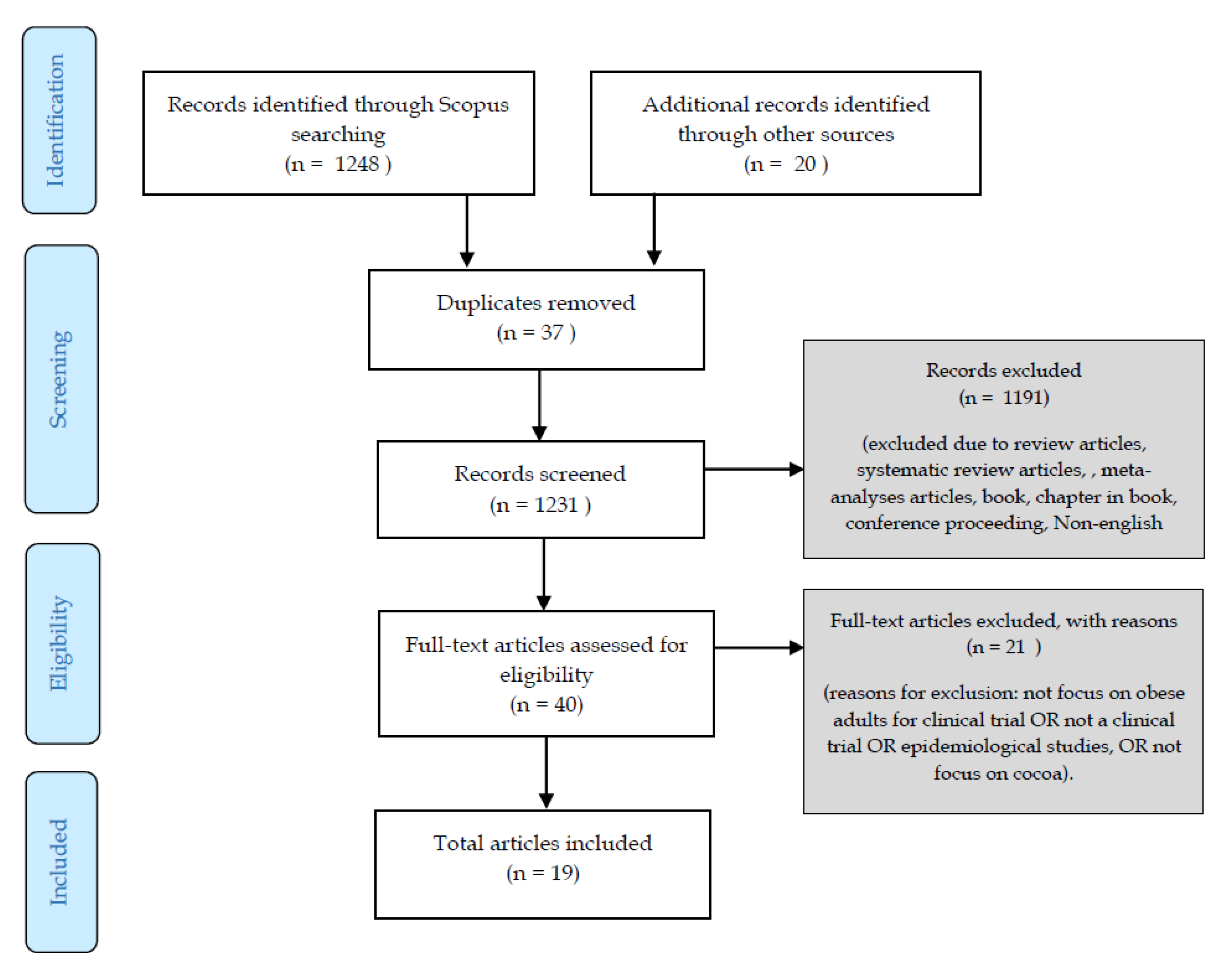
3.1. Articles Identified
3.2. Study Populations
3.3. Epidemiological Studies
3.4. Intervention Studies
3.4.1. Intervention Design and Dosage
3.4.2. Changes in Body Weight, BMI, Waist Circumference, and Blood Pressure
3.4.3. Changes in Glucose and Lipid Profiles
3.4.4. Changes in Oxidative and Inflammatory Markers
3.5. Other Measurements
4. Discussion
5. Conclusions

{kind=link}
| Study (Country) | Study Design | Participants | Dose/Form of Cocoa | Duration | Outcome Measures |
|---|---|---|---|---|---|
| Davison et al. [26] (Australia) | Randomized double-blind parallel placebo-controlled trial | N = 49; (age 18–65) (17 males, 32 females) | G1: High flavanol (902 mg) + 45 min exercise 3 times a week G2: Low flavanol (36 mg) + 45 min exercise 3 times a week G3: High flavanol (902 mg) G4: Low flavanol (36 mg) Form of cocoa: dairy-based powder mix | 12 weeks |
|
| Monagas et al. [20] (Spain) | Randomized cross-over controlled trial | N = 42 at high risk for CVD (age > 55) (19 men, 23 women) | G1: 40 g cocoa powder (495 mg polyphenols) + 500 mL skim milk/day G2: 500 mL skim milk/day | 4 weeks |
|
| Almoosawi et al. [25] (UK) | Randomized cross-over controlled trial | N = 14 (age 21–50) (8 males, 6 females) | G1:20 g dark chocolate (500 mg polyphenols) G2: 20 g dark chocolate (1000 mg polyphenols) | 2 weeks 1 week run-in phase, 1 week washout |
|
| Njike et al. [38] (USA) | Randomized controlled double-blind cross-over trial | N = 44 | G1: sugar-free cocoa beverage (22 g cocoa, 805 mg flavanol) G2: sweetened cocoa beverage (22 g cocoa, 805 mg flavanol) G3: placebo beverage | 6 weeks 4 weeks washout |
|
| Khan et al. [19] (Spain) | Randomized controlled cross-over trial | N = 42 at high risk of CVD (age > 55) (19 men, 23 women) | G1: 40 g cocoa powder (495 polyphenols) + 500 mL skim milk G2: 500 mL skim milk | 4 weeks |
|
| Stote et al. [22] (USA) | Randomized placebo-controlled cross-over trial | N = 20 obese at risk of insulin resistance (age 25–55) (10 women, 10 men) | G1: control, 56 g cocoa powder beverage (30 mg flavanol) G2: low, 56 g cocoa powder beverage (180 mg flavanol) G3: medium, 56 g cocoa powder beverage (400 mg flavanol) G4: high, 56 g cocoa powder beverage (900 mg flavanol) G5: tea (900 mg) | 5 days intervention 10 days washout |
|
| Almoosawi et al. [24] (UK) | Randomized controlled single-blind cross-over trial | N = 42 (21 normal BMI, 21 owt/obese) | G1: 20 g dark choc (500 mg polyphenols) G2: 20 g placebo dark choc | 4 weeks 2 weeks washout period |
|
| West et al. [23] (USA) | Randomized placebo-controlled cross-over trial | N = 30 postmenopausal women (age 40–64) | G1: 37 g dark choc + sugar-free cocoa beverage, total flavanol 814 mg G2: low-flavanol chocolate bar + cocoa-free beverage, total flavanol 3 mg | 4 weeks 2 weeks washout period |
|
| Nickols Richardson et al. [28] (USA) | Randomized controlled parallel trial | N = 60 overweight/obese women (age 25–45) | Daily energy-restricted diet with: G1: 236 mL sugar-free natural cocoa beverage per day (272 kJ/day), one 1.45 oz dark chocolate (270 mg flavanol) G2: 236 mL sugar-free cocoa-free vanilla beverage per day (272 kJ/day), two non-chocolate sweet snacks (fruit-flavored licorice stick) (0 mg flavanol) | 18 weeks |
|
| Basu et al. [21] (USA) | Randomized controlled double-blind cross-over trial | N = 18 obese adults with elevated waist circumference, type 2 diabetes (14 females, 4 males, age > 21) | G1: 20 g cocoa beverage (960 mg polyphenols, 480 mg flavanols) + high-fat fast-food breakfast (766 kcal) G2: 12 g flavanol-free placebo (110 mg polyphenols, <0.1 mg flavanols) + high-fat fast-food breakfast (766 kcal) | 6 h 1 week washout |
|
| Munguia et al. [35] (Mexico) | Randomized controlled double-blind trial | N = 15 overweight with borderline criteria of metabolic syndrome (age 20–60) (11 females, 4 males) | G1: cocoa bean extract powder (80 mg flavonoids) G2: placebo powder (sugar-free, no flavonoids) | 4 weeks |
|
| Ibeiro-Baraibar et al. [27] (Spain) | Randomized controlled parallel double-blind trial | N = 24 (12 males, 12 females) (age 50–80) | G1: –15% energy-restricted diet + ready-to-eat meals + 1.4 g cocoa extract (645 mg polyphenols) G2: –15% energy-restricted diet + ready-to-eat meals | 4 weeks |
|
| Lee et al. [50] (USA) | Randomized controlled four-period cross-over trial | N = 31 overweight/obese with elevated LDL-c (13 males, 18 females) (age 30–70) | G1: No treatment food (average American diet) G2: 42.5 g almonds (ALD)G3: 18 g cocoa powder + 43 g dark chocolate (CHOC) (422 mg polyphenols) G4: ALD + CHOC (422 mg polyphenols) | 4 weeks 2 weeks washout period |
|
| Leyva Soto et al. [34] (USA) | Randomized placebo-controlled double-blind trial | N = 84 young volunteers (47 men, 37 women) | G1: 2 g dark chocolate (70% cocoa) G2: 2 g milk chocolate | 6 months |
|
| Study | Population | Investigation | Outcomes |
|---|---|---|---|
| Vernarelli and Lambert [31] | 9551 adults | Association of flavonoid consumption and multiple markers for obesity including body mass index, waist circumference, and C-reactive protein | An inverse association between total flavonoid intake and BMI (body mass index) was observed (p-trend, 0.013) after adjusting for age, sex, race, education, physical activity, smoking status, poverty/income ratio, total alcohol intake, total fat intake, and dietary energy density |
| Cuenca-Garcia M et al. [29] | 1458 adolescents | To determine whether chocolate consumption is associated with higher BMI and other markers of total and central body fat | Higher consumption of chocolate was associated with lower BMI, body fat estimated from skinfold and BIA (bioelectrical impedance analysis), waist circumference |
| O’Neil et al. [62] | 15,023 adults | To determine candy and chocolate consumption with nutrient intake, diet quality, weight status, and CVD (cardiovascular disease) risk factors | Chocolate consumers had lower weight, TG (triglycerides) and CRP (C-reactive protein) levels, and higher HDL-c (high-density lipoprotein) levels |
| Golomb et al. [32] | 1018 adults | To examine the cross-sectional relationship of chocolate consumption frequency and BMI | Frequent chocolate intake linked to lower BMI |
| Greenberg and Buijsse [33] | 15,732 and 12,830 participants at the first and second visit | To assess prospective and cross-sectional associations between chocolate intake and body weight | Prospective analysis shows more frequent consumption of chocolate was significantly associated with long-term greater weight gain in a dose-response manner; cross-sectional analysis yielded the opposite: an inverse association between chocolate intake and current BMI |
Author Contributions
Funding
Conflicts of Interest
References
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef]
- World Health Organization Website. Available online: https://www.who.int/health-topics/obesity#tab=tab_1 (accessed on 11 October 2020).
- World Health Organization Website. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 11 October 2020).
- Centers for Disease Control and Prevention Adult Obesity Facts. Overweight & Obesity. CDC 2015, 31, 239–242.
- Djalalinia, S.; Qorbani, M.; Peykari, N.; Kelishadi, R. Health impacts of obesity. Pak. J. Med. Sci 2015, 31, 239–242. [Google Scholar] [PubMed]
- Kearns, K.; Dee, A.; Fitzgerald, A.P.; Doherty, E.; Perry, I.J. Chronic disease burden associated with overweight and obesity in Ireland: The effects of a small BMI reduction at population level. BMC Public Health 2014, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Dludla, P.V.; Nkambule, B.B.; Jack, B.; Mkandla, Z.; Mutize, T.; Silvestri, S.; Orlando, P.; Tiano, L.; Louw, J.; Mazibuko-Mbeje, S.E. Inflammation and oxidative stress in an obese state and the protective effects of gallic acid. Nutrients 2019, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, C.N.; Saltiel, A.R. Inflammatory links between obesity and metabolic disease. J. Clin. Investig. 2011, 121, 2111–2117. [Google Scholar] [CrossRef] [PubMed]
- Soeliman, F.A.; Azadbakht, L. Weight loss maintenance: A review on dietary related strategies. J. Res. Med. Sci. 2014, 19, 268–275. [Google Scholar] [PubMed]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed]
- D’Archivio, M.; Filesi, C.; Di Benedetto, R.; Gargiulo, R.; Giovannini, C.; Masella, R. Polyphenols, dietary sources and bioavailability. Ann. Ist. Super. Sanita 2007, 43, 348–361. [Google Scholar]
- Pandey, K.B.; Rizvi, S.I. Plant polyphenols as dietary antioxidants in human health and disease. Oxidative Med. Cell. Longev. 2009, 2, 270–278. [Google Scholar] [CrossRef]
- Crozier, A.; Lean, M.E.J.; McDonald, M.S.; Black, C. Quantitative Analysis of the Flavonoid Content of Commercial Tomatoes, Onions, Lettuce, and Celery. J. Agric. Food Chem. 1997, 45, 590–595. [Google Scholar] [CrossRef]
- Lee, K.W.; Kim, Y.J.; Lee, H.J.; Lee, C.Y. Cocoa Has More Phenolic Phytochemicals and a Higher Antioxidant Capacity than Teas and Red Wine. J. Agric. Food Chem. 2003, 51, 7292–7295. [Google Scholar] [CrossRef]
- Aprotosoaie, A.; Miron, A.; Trifan, A.; Luca, V.; Costache, I.-I. The Cardiovascular Effects of Cocoa Polyphenols—An Overview. Diseases 2016, 4, 39. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.B.; Hurst, W.J.; Payne, M.J.; Stuart, D.A.; Apgar, J.; Sweigart, D.S.; Ou, B. Impact of alkalization on the antioxidant and flavanol content of commercial cocoa powders. J. Agric. Food Chem. 2008, 56, 8527–8533. [Google Scholar] [CrossRef] [PubMed]
- Meydani, M.; Hasan, S.T. Dietary polyphenols and obesity. Nutrients 2010, 2, 737–751. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 5, 69. [Google Scholar] [CrossRef]
- Khan, N.; Monagas, M.; Andres-Lacueva, C.; Casas, R.; Urpí-Sardà, M.; Lamuela-Raventós, R.M.; Estruch, R. Regular consumption of cocoa powder with milk increases HDL cholesterol and reduces oxidized LDL levels in subjects at high-risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 1046–1053. [Google Scholar] [CrossRef]
- Monagas, M.; Khan, N.; Andres-Lacueva, C.; Casas, R.; Urpí-Sardà, M.; Llorach, R.; Lamuela-Raventós, R.M.; Estruch, R. Effect of cocoa powder on the modulation of inflammatory biomarkers in patients at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2009, 90, 1144–1150. [Google Scholar] [CrossRef]
- Basu, A.; Betts, N.M.; Leyva, M.J.; Fu, D.; Aston, C.E.; Lyons, T.J. Acute Cocoa Supplementation Increases Postprandial HDL Cholesterol and Insulin in Obese Adults with Type 2 Diabetes after Consumption of a High-Fat Breakfast. J. Nutr. 2015, 145, 2325–2332. [Google Scholar] [CrossRef]
- Stote, K.S.; Clevidence, B.A.; Novotny, J.A.; Henderson, T.; Radecki, S.V.; Baer, D.J. Effect of cocoa and green tea on biomarkers of glucose regulation, oxidative stress, inflammation and hemostasis in obese adults at risk for insulin resistance. Eur. J. Clin. Nutr. 2012, 66, 1153–1159. [Google Scholar] [CrossRef]
- West, S.G.; McIntyre, M.D.; Piotrowski, M.J.; Poupin, N.; Miller, D.L.; Preston, A.G.; Wagner, P.; Groves, L.F.; Skulas-Ray, A.C. Effects of dark chocolate and cocoa consumption on endothelial function and arterial stiffness in overweight adults. Br. J. Nutr. 2014, 111, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Almoosawi, S.; Tsang, C.; Ostertag, L.M.; Fyfe, L.; Al-Dujaili, E.A.S. Differential effect of polyphenol-rich dark chocolate on biomarkers of glucose metabolism and cardiovascular risk factors in healthy, overweight and obese subjects: A randomized clinical trial. Food Funct. 2012, 3, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Almoosawi, S.; Fyfe, L.; Ho, C.; Al-dujaili, E. The effect of polyphenol-rich dark chocolate on fasting capillary whole blood glucose, total cholesterol, blood pressure and glucocorticoids in healthy overweight and obese subjects. Br. J. Nutr. 2010, 103, 842–850. [Google Scholar] [CrossRef]
- Davison, K.; Coates, A.M.; Buckley, J.D.; Howe, P.R.C. Effect of cocoa flavanols and exercise on cardiometabolic risk factors in overweight and obese subjects. Int. J. Obes. 2008, 32, 1289–1296. [Google Scholar] [CrossRef]
- Ibero-Baraibar, I.; Suárez, M.; Arola-Arnal, A.; Zulet, M.A.; Martinez, J.A. Cocoa extract intake for 4 weeks reduces postprandial systolic blood pressure response of obese subjects, even after following an energy-restricted diet. Food Nutr. Res. 2016, 60, 30449. [Google Scholar] [CrossRef]
- Nickols-Richardson, S.M.; Piehowski, K.E.; Metzgar, C.J.; Miller, D.L.; Preston, A.G. Changes in body weight, blood pressure and selected metabolic biomarkers with an energy-restricted diet including twice daily sweet snacks and once daily sugar-free beverage. Nutr. Res. Pract. 2014, 8, 695–704. [Google Scholar] [CrossRef]
- Cuenca-García, M.; Ruiz, J.R.; Ortega, F.B.; Castillo, M.J. Association between chocolate consumption and fatness in European adolescents. Nutrition 2014, 30, 236–239. [Google Scholar] [CrossRef]
- Hughes, L.A.E.; Arts, I.C.W.; Ambergen, T.; Brants, H.A.M.; Dagnelie, P.C.; Goldbohm, R.A.; Van Den Brandt, P.A.; Weijenberg, M.P. Higher dietary flavone, flavonol, and catechin intakes are associated with less of an increase in BMI over time in women: A longitudinal analysis from the Netherlands Cohort Study. Am. J. Clin. Nutr. 2008, 88, 1341–1352. [Google Scholar]
- Vernarelli, J.A.; Lambert, J.D. Flavonoid intake is inversely associated with obesity and C-reactive protein, a marker for inflammation, in US adults. Nutr. Diabetes 2017, 7, e276. [Google Scholar] [CrossRef]
- Golomb, B.A.; Koperski, S.; White, H.L. Association between more frequent chocolate consumption and lower body mass index. Arch. Intern. Med. 2012, 172, 519–521. [Google Scholar] [CrossRef]
- Greenberg, J.A.; Buijsse, B. Habitual Chocolate Consumption May Increase Body Weight in a Dose-Response Manner. PLoS ONE 2013, 8, e70271. [Google Scholar] [CrossRef]
- Leyva-Soto, A.; Chavez-Santoscoy, R.A.; Lara-Jacobo, L.R.; Chavez-Santoscoy, A.V.; Gonzalez-Cobian, L.N. Daily consumption of chocolate rich in flavonoids decreases cellular genotoxicity and improves biochemical parameters of lipid and glucose metabolism. Molecules 2018, 23, 2220. [Google Scholar]
- Munguía, L.; Gutiérrez-Salmeán, G.; Hernández, M.; Ortiz, A.; Sánchez, M.E.; Nájera, N.; Meaney, E.; Rubio-Gayosso, I.; Ceballos, G. Beneficial effects of a flavanol-enriched cacao beverage on anthropometric and cardiometabolic risk profile in overweight subjects. Rev. Mex. Cardiol. 2015, 26, 78–86. [Google Scholar]
- Pasquali, R.; Vicennati, V.; Cacciari, M.; Pagotto, U. The hypothalamic-pituitary-adrenal axis activity in obesity and the metabolic syndrome. Ann N Y Acad Sci. 2006, 1083, 111–128. [Google Scholar] [CrossRef]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef]
- Njike, V.Y.; Faridi, Z.; Shuval, K.; Dutta, S.; Kay, C.D.; West, S.G.; Kris-Etherton, P.M.; Katz, D.L. Effects of sugar-sweetened and sugar-free cocoa on endothelial function in overweight adults. Int. J. Cardiol. 2011, 149, 83–88. [Google Scholar] [CrossRef]
- Ibero-Baraibar, I.; Abete, I.; Navas-Carretero, S.; Massis-Zaid, A.; Martinez, J.A.; Zulet, M.A. Oxidised LDL levels decreases after the consumption of ready-to-eat meals supplemented with cocoa extract within a hypocaloric diet. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 416–422. [Google Scholar] [CrossRef]
- González-Sarrías, A.; Combet, E.; Pinto, P.; Mena, P.; Dall’Asta, M.; Garcia-Aloy, M.; Rodríguez-Mateos, A.; Gibney, E.R.; Dumont, J.; Massaro, M.; et al. A systematic review and meta-analysis of the effects of flavanol-containing tea, cocoa and apple products on body composition and blood lipids: Exploring the factors responsible for variability in their efficacy. Nutrients 2017, 9, 746. [Google Scholar] [CrossRef]
- Miller, K.B.; Stuart, D.A.; Smith, N.L.; Lee, C.Y.; Mchale, N.L.; Flanagan, J.A.; Boxin, O.U.; Hurst, W.J. Antioxidant activity and polyphenol and procyanidin contents of selected commercially available cocoa-containing and chocolate products in the United States. J. Agric. Food Chem. 2006, 54, 4062–4068. [Google Scholar] [CrossRef]
- Jalil, A.M.M.; Ismail, A. Polyphenols in cocoa and cocoa products: Is there a link between antioxidant properties and health? Molecules 2008, 13, 2190–2219. [Google Scholar] [CrossRef]
- Rimbach, G.; Egert, S.; De Pascual-Teresa, S. Chocolate: (Un)healthy source of polyphenols? Genes Nutr. 2011, 6, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Doughty, K.; Ali, A. Cocoa and Chocolate in Human Health and Disease. Antioxid. Redox Signal 2011, 15, 2779–2811. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A.; Magkos, F.; Bier, D.M.; Brenna, J.T.; de Oliveira Otto, M.C.; Hill, J.O.; King, J.C.; Mente, A.; Ordovas, J.M.; Volek, J.S.; et al. Saturated Fats and Health: A Reassessment and Proposal for Food-Based Recommendations: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, H.; Tanaka, J.; Kikuchi, M.; Fukuda, T.; Ito, H.; Hatano, T.; Yoshida, T. Effect of Polyphenol-αich Extract from Walnut on Diet-Induced Hypertriglyceridemia in Mice via Enhancement of Fatty Acid Oxidation in the Liver. J. Agric. Food Chem. 2009, 57, 1786–1792. [Google Scholar] [CrossRef] [PubMed]
- Matsui, N.; Ito, R.; Nishimura, E.; Yoshikawa, M.; Kato, M.; Kamei, M.; Shibata, H.; Matsumoto, I.; Abe, K.; Hashizume, S. Ingested cocoa can prevent high-fat diet-induced obesity by regulating the expression of genes for fatty acid metabolism. Nutrition 2005, 21, 594–601. [Google Scholar] [CrossRef]
- Greenberg, J.A.; O’donnell, R.; Shurpin, M.; Kordunova, D. Epicatechin, procyanidins, cocoa, and appetite: A randomized controlled trial. Am. J. Clin. Nutr. 2016, 104, 613–619. [Google Scholar] [CrossRef]
- Massolt, E.T.; van Haard, P.M.; Rehfeld, J.F.; Posthuma, E.F.; van der Veer, E.; Schweitzer, D.H. Appetite suppression through smelling of dark chocolate correlates with changes in ghrelin in young women. Regul. Pept. 2010, 161, 81–86. [Google Scholar] [CrossRef]
- Lee, Y.; Berryman, C.E.; West, S.G.; Chen, C.Y.O.; Blumberg, J.B.; Lapsley, K.G.; Preston, A.G.; Fleming, J.A.; Kris-Etherton, P.M. Effects of dark chocolate and almonds on cardiovascular risk factors in overweight and obese individuals: A randomized controlled-feeding trial. J. Am. Heart Assoc. 2017, 6, e005162. [Google Scholar] [CrossRef]
- Jia, L.; Liu, X.; Bai, Y.Y.; Li, S.H.; Sun, K.; He, C.; Hui, R. Short-term effect of cocoa product consumption on lipid profile: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2010, 92, 218–225. [Google Scholar] [CrossRef]
- Tokede, O.A.; Gaziano, J.M.; Djoussé, L. Effects of cocoa products/dark chocolate on serum lipids: A meta-analysis. Eur. J. Clin. Nutr. 2011, 65, 879–886. [Google Scholar] [CrossRef]
- Ruzaidi, A.; Amin, I.; Nawalyah, A.G.; Hamid, M.; Faizul, H.A. The effect of Malaysian cocoa extract on glucose levels and lipid profiles in diabetic rats. J. Ethnopharmacol. 2005, 98, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Khalili, M.; Haghighat, N.; Eghtesadi, S.; Shidfar, F.; Heidari, I.; Ebrahimpour-Koujan, S.; Eghtesadi, M. High-cocoa polyphenol-rich chocolate improves blood pressure in patients with diabetes and hypertension. ARYA Atheroscler. 2015, 11, 21–29. [Google Scholar] [PubMed]
- Dorenkott, M.R.; Griffin, L.E.; Goodrich, K.M.; Thompson-Witrick, K.A.; Fundaro, G.; Ye, L.; Stevens, J.R.; Ali, M.; O’Keefe, S.F.; Hulver, M.W.; et al. Oligomeric cocoa procyanidins possess enhanced bioactivity compared to monomeric and polymeric cocoa procyanidins for preventing the development of obesity, insulin resistance, and impaired glucose tolerance during high-fat feeding. J. Agric. Food Chem. 2014, 62, 2216–2227. [Google Scholar] [CrossRef] [PubMed]
- Styskal, J.; Van Remmen, H.; Richardson, A.; Salmon, A.B. Oxidative stress and diabetes: What can we learn about insulin resistance from antioxidant mutant mouse models? Free Radic. Biol. Med 2012, 52, 46–58. [Google Scholar] [CrossRef]
- Berlett, B.S.; Stadtman, E.R. Protein oxidation in aging, disease, and oxidative stress. J. Biol. Chem. 1997, 272, 20313–20316. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity & inflammation: The linking mechanism & the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar]
- Kalupahana, N.S.; Moustaid-Moussa, N.; Claycombe, K.J. Immunity as a link between obesity and insulin resistance. Mol. Aspects Med. 2012, 33, 26–34. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Cekanova, M.; LeMieux, M.; Greer, B.; Moustaid-Moussa, N. Modulation of adipose tissue inflammation by bioactive food compounds. J. Nutr. Biochem. 2013, 24, 613–623. [Google Scholar] [CrossRef]
- Sorrenti, V.; Ali, S.; Mancin, L.; Davinelli, S.; Paoli, A.; Scapagnini, G. Cocoa Polyphenols and Gut Microbiota Interplay: Bioavailability, Prebiotic Effect, and Impact on Human Health. Nutrients 2020, 12, 1908. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Fulgoni, V.L.; Nicklas, T.A. Candy consumption was not associated with body weight measures, risk factors for cardiovascular disease, or metabolic syndrome in US adults: NHANES 1999–2004. Nutr. Res. 2011, 31, 122–130. [Google Scholar] [CrossRef]

| Criteria | Inclusion | Exclusion |
|---|---|---|
| Literature type | Journal (research articles) | Systematic review, book and book series, book chapter, conference proceedings |
| Language | English | Non-English |
| Timeline Study type | Between 2008 and 2019 Human clinical trials and observational studies | Published before 2008 Animal and in vitro studies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halib, H.; Ismail, A.; Mohd Yusof, B.-N.; Osakabe, N.; Mat Daud, Z.A. Effects of Cocoa Polyphenols and Dark Chocolate on Obese Adults: A Scoping Review. Nutrients 2020, 12, 3695. https://doi.org/10.3390/nu12123695
Halib H, Ismail A, Mohd Yusof B-N, Osakabe N, Mat Daud ZA. Effects of Cocoa Polyphenols and Dark Chocolate on Obese Adults: A Scoping Review. Nutrients. 2020; 12(12):3695. https://doi.org/10.3390/nu12123695
Chicago/Turabian StyleHalib, Hasmiza, Amin Ismail, Barakatun-Nisak Mohd Yusof, Naomi Osakabe, and Zulfitri Azuan Mat Daud. 2020. "Effects of Cocoa Polyphenols and Dark Chocolate on Obese Adults: A Scoping Review" Nutrients 12, no. 12: 3695. https://doi.org/10.3390/nu12123695
APA StyleHalib, H., Ismail, A., Mohd Yusof, B.-N., Osakabe, N., & Mat Daud, Z. A. (2020). Effects of Cocoa Polyphenols and Dark Chocolate on Obese Adults: A Scoping Review. Nutrients, 12(12), 3695. https://doi.org/10.3390/nu12123695