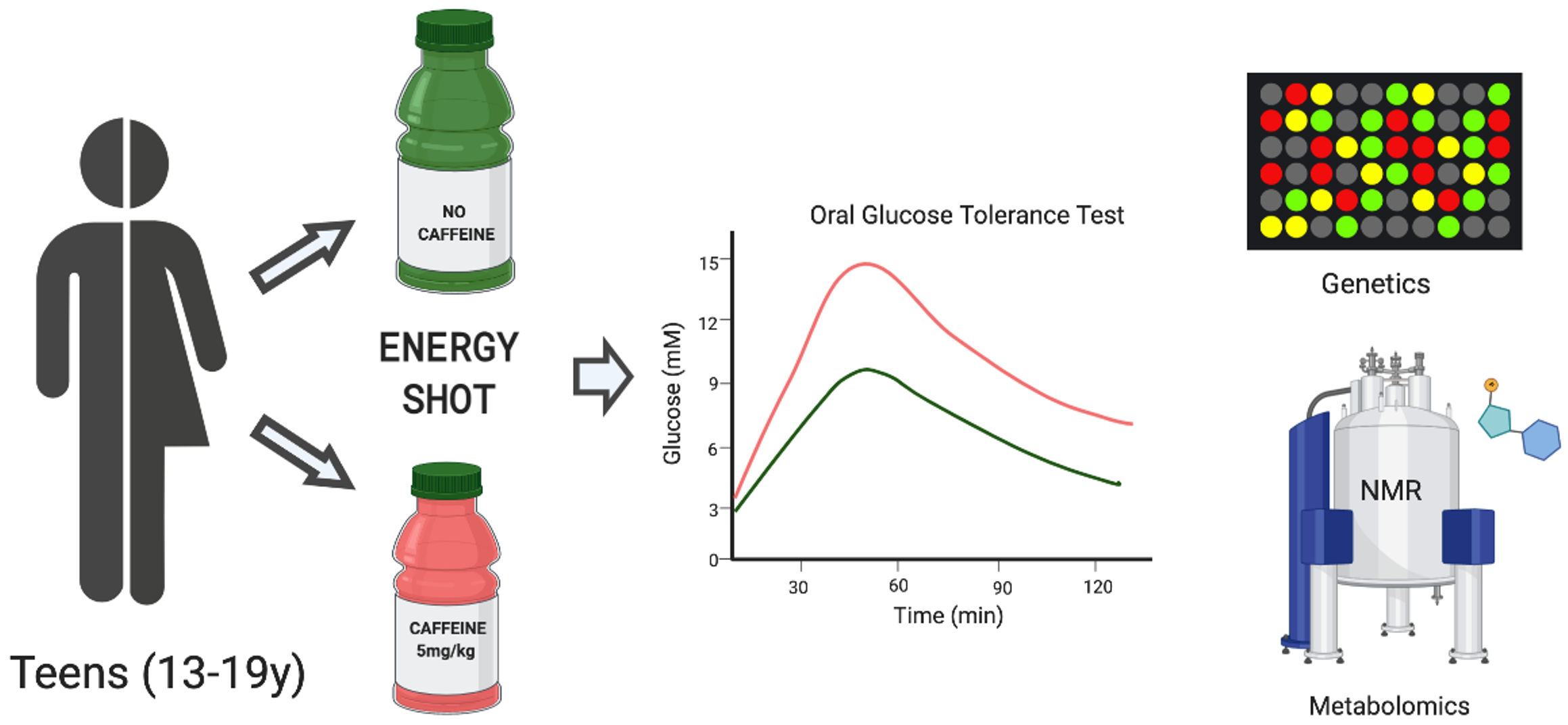
Caffeine-Containing Energy Shots Cause Acute Impaired Glucoregulation in Adolescents

 ,
,  ,
, 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Test Beverages
2.3. Experimental Design
2.4. Blood Analysis
2.5. Combined Caffeine Sensitivity Allele Score
2.6. Serum Metabolomics Analysis
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Impact of Caffeine-Containing Energy Shots on Glucose and Insulin Responses
3.3. Impacts of Caffeine-Containing Energy Shots on Gut and Metabolic Hormone Secretion
3.4. Combined Caffeine Sensitivity Allele Score
3.5. Serum Metabolomics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heckman, M.A.; Sherry, K.; de Mejia, E.G. Energy drinks: An assessment of their market size, consumer demographics, ingredient profile, functionality, and regulations in the United States. Compr. Rev. Food Sci. Food Saf. 2010, 9, 303–317. [Google Scholar] [CrossRef]
- Reid, J.L.; McCrory, C.; White, C.M.; Martineau, C.; Vanderkooy, P.; Fenton, N.; Hammond, D. Consumption of Caffeinated Energy Drinks Among Youth and Young Adults in Canada. Prev. Med. Rep. 2017, 5, 65–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on Nutrition and the Council on Sports Medicine and Fitness. Pediatrics Sports Drinks and Energy Drinks for Children and Adolescents: Are They Appropriate? Pediatrics 2011, 127, 1182–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigard, A.X. Risks of energy drinks in youths. Arch. Pediatr. 2010, 17, 1625–1631. [Google Scholar] [CrossRef]
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics 2011, 127, 511–528. [Google Scholar] [CrossRef] [Green Version]
- Shearer, J.; Graham, T.E. Performance effects and metabolic consequences of caffeine and caffeinated energy drink consumption on glucose disposal. Nutr. Rev. 2014, 72, 121–136. [Google Scholar] [CrossRef]
- Calamaro, C.J.; Mason, T.B.A.; Ratcliffe, S.J. Adolescents living the 24/7 lifestyle: Effects of caffeine and technology on sleep duration and daytime functioning. Pediatrics 2009, 123. [Google Scholar] [CrossRef] [Green Version]
- Owens, J.A.; Mindell, J.; Baylor, A. Effect of energy drink and caffeinated beverage consumption on sleep, mood, and performance in children and adolescents. Nutr. Rev. 2014, 72, 65–71. [Google Scholar] [CrossRef]
- Graham, T.E.; Sathasivam, P.; Rowland, M.; Marko, N.; Greer, F.; Battram, D. Caffeine ingestion elevates plasma insulin response in humans during an oral glucose tolerance test. Can. J. Physiol. Pharmacol. 2001, 79, 559–565. [Google Scholar] [CrossRef]
- Petrie, H.J.; Chown, S.E.; Belfie, L.M.; Duncan, A.M.; McLaren, D.H.; Conquer, J.A.; Graham, T.E. Caffeine ingestion increases the insulin response to an oral-glucose-tolerance test in obese men before and after weight loss. Am. J. Clin. Nutr. 2004, 80, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.E.; Spafford, C.; Graham, T.E.; Smith, G.N. Acute Caffeine Ingestion and Glucose Tolerance in Women with or without Gestational Diabetes Mellitus. J. Obstet. Gynaecol. Canada 2009, 31, 304–312. [Google Scholar] [CrossRef]
- Lee, S.; Hudson, R.; Kilpatrick, K.; Graham, T.E.; Ross, R. Caffeine ingestion is associated with reductions in glucose uptake independent of obesity and type 2 diabetes before and after exercise training. Diabetes Care 2005, 28, 566–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaudoin, M.-S.; Allen, B.; Mazzetti, G.; Sullivan, P.J.; Graham, T.E. Caffeine ingestion impairs insulin sensitivity in a dose-dependent manner in both men and women. Appl. Physiol. Nutr. Metab. 2013, 38, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Dekker, M.J.; Gusba, J.E.; Robinson, L.E.; Graham, T.E. Glucose homeostasis remains altered by acute caffeine ingestion following 2 weeks of daily caffeine consumption in previously non-caffeine-consuming males. Br. J. Nutr. 2007, 98, 556. [Google Scholar] [CrossRef] [Green Version]
- Nehlig, A. Interindividual differences in caffeine metabolism and factors driving caffeine consumption. Pharmacol. Rev. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, C.; Graham, T.E. Effects of exercise and thermal stress on caffeine pharmacokinetics in men and eumenorrheic women. J. Appl. Physiol. 2002, 93, 1471–1478. [Google Scholar] [CrossRef] [Green Version]
- Mayengbam, S.; Virtanen, H.; Hittel, D.S.; Elliott, C.; Reimer, R.A.R.A.; Vogel, H.J.H.J.; Shearer, J. Metabolic consequences of discretionary fortified beverage consumption containing excessive vitamin B levels in adolescents. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Carere, D.A.; Couper, M.P.; Crawford, S.D.; Kalia, S.S.; Duggan, J.R.; Moreno, T.A.; Mountain, J.L.; Roberts, J.S.; Green, R.C.; Krier, J.B.; et al. Design, methods, and participant characteristics of the Impact of Personal Genomics (PGen) Study, a prospective cohort study of direct-to-consumer personal genomic testing customers. Genome Med. 2014, 6, 96. [Google Scholar] [CrossRef] [Green Version]
- Nordestgaard, A.T.; Thomsen, M.; Nordestgaard, B.G. Coffee intake and risk of obesity, metabolic syndrome and type 2 diabetes: A Mendelian randomization study. Int. J. Epidemiol. 2015, 44, 551–565. [Google Scholar] [CrossRef]
- Gronwald, W.; Klein, M.S.; Kaspar, H.; Fagerer, S.R.; Nürnberger, N.; Dettmer, K.; Bertsch, T.; Oefner, P.J. Urinary Metabolite Quantification Employing 2D NMR Spectroscopy. Anal. Chem. 2008, 80, 9288–9297. [Google Scholar] [CrossRef]
- Yeh, K.C.; Kwan, K.C. A comparison of numerical integrating algorithms by trapezoidal, Lagrange, and spline approximation. J. Pharmacokinet. Biopharm. 1978. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, H.J.; Brown, R.E. Detecting outliers when fitting data with nonlinear regression—A new method based on robust nonlinear regression and the false discovery rate. BMC Bioinform. 2006, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorkin, B.C.; Coates, P.M. Caffeine-containing energy drinks: Beginning to address the gaps in what we know. Adv. Nutr. 2014, 5, 541–543. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.B.; Park, S.; Jin, G.-R.; Jung, J.H.; Park, H.J.; Lee, S.H.; Shin, S.; Lee, B.-H. Trends in Beverage Consumption and Related Demographic Factors and Obesity among Korean Children and Adolescents. Nutrients 2020, 12, 2651. [Google Scholar] [CrossRef]
- Goran, M.I.; Gower, B.A. Longitudinal Study on Pubertal Insulin Resistance. Diabetes 2001, 50, 2444–2450. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.E.; Savani, S.; Battram, D.S.; McLaren, D.H.; Sathasivam, P.; Graham, T.E. Caffeine ingestion before an oral glucose tolerance test impairs blood glucose management in men with type 2 diabetes. J. Nutr. 2004, 134, 2528–2533. [Google Scholar] [CrossRef]
- Shi, X.; Xue, W.; Liang, S.; Zhao, J.; Zhang, X. Acute caffeine ingestion reduces insulin sensitivity in healthy subjects: A systematic review and meta-analysis. Nutr. J. 2016, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Johnston, K.L.; Clifford, M.N.; Morgan, L.M. Coffee acutely modifies gastrointestinal hormone secretion and glucose tolerance in humans: Glycemic effects of chlorogenic acid and caffeine. Am. J. Clin. Nutr. 2003, 78, 728–733. [Google Scholar] [CrossRef]
- Beaudoin, M.S.; Robinson, L.E.; Graham, T.E. An oral lipid challenge and acute intake of caffeinated coffee additively decrease glucose tolerance in healthy men. J. Nutr. 2011, 141, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Moisey, L.L.; Robinson, L.E.; Graham, T.E. Consumption of caffeinated coffee and a high carbohydrate meal affects postprandial metabolism of a subsequent oral glucose tolerance test in young, healthy males. Br. J. Nutr. 2010, 103, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Moisey, L.L.; Kacker, S.; Bickerton, A.C.; Robinson, L.E.; Graham, T.E. Caffeinated coffee consumption impairs blood glucose homeostasis in response to high and low glycemic index meals in healthy men. Am. J. Clin. Nutr. 2008, 87, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Battram, D.S.; Arthur, R.; Weekes, A.; Graham, T.E. The glucose intolerance induced by caffeinated coffee ingestion is less pronounced than that due to alkaloid caffeine in men. J. Nutr. 2006, 136, 1276–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shearer, J.; Farah, A.; De Paulis, T.; Bracy, D.P.; Pencek, R.R.; Graham, T.E.; Wasserman, D.H. Quinides of Roasted Coffee Enhance Insulin Action in Conscious Rats. J. Nutr. 2003, 133. [Google Scholar] [CrossRef] [PubMed]
- Vergauwen, L.; Hespel, P.; Richter, E.A. Adenosine receptors mediate synergistic stimulation of glucose uptake and transport by insulin and by contractions in rat skeletal muscle. J. Clin. Investig. 1994, 93, 974–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thong, F.S.L.; Graham, T.E. The putative roles of adenosine in insulin- and exercise-mediated regulation of glucose transport and glycogen metabolism in skeletal muscle. Can. J. Appl. Physiol. 2002, 27, 152–178. [Google Scholar] [CrossRef]
- Fredholm, B.B. On the Mechanism of Action of Theophylline and Caffeine. Acta Med. Scand. 1985, 217, 149–153. [Google Scholar] [CrossRef]
- Basrai, M.; Schweinlin, A.; Menzel, J.; Mielke, H.; Weikert, C.; Dusemund, B.; Putze, K.; Watzl, B.; Lampen, A.; Bischoff, S.C. Energy drinks induce acute cardiovascular and metabolic changes pointing to potential risks for young adults: A randomized controlled trial. J. Nutr. 2019, 149, 441–450. [Google Scholar] [CrossRef]
- Higgins, J.P.; Yang, B.; Herrin, N.E.; Yarlagadda, S.; Le, G.T.; Ortiz, B.L.; Ali, A.; Infanger, S.C. Consumption of energy beverage is associated with attenuation of arterial endothelial flow-mediated dilatation. World J. Cardiol. 2017, 9, 162. [Google Scholar] [CrossRef]
- Cotter, B.V.; Jackson, D.A.E.; Merchant, R.C.; Babu, K.M.; Baird, J.R.; Nirenberg, T.; Linakis, J.G. Energy drink and other substance use among adolescent and young adult emergency department patients. Pediatr. Emerg. Care 2013, 29, 1091–1097. [Google Scholar] [CrossRef]
- Jackson, D.A.E.; Cotter, B.V.; Merchant, R.C.; Babu, K.M.; Baird, J.R.; Nirenberg, T.; Linakis, J.G. Behavioral and physiologic adverse effects in adolescent and young adult emergency department patients reporting use of energy drinks and caffeine. Clin. Toxicol. 2013, 51, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Laitala, V.S.; Kaprio, J.; Silventoinen, K. Genetics of coffee consumption and its stability. Addiction 2008, 103, 2054–2061. [Google Scholar] [CrossRef] [PubMed]
- Keijzers, G.; De Galan, B.E.; Tack, C.J.; Smits, P. Caffeine can decrease insulin sensitivity in humans. Diabetes Care 2002, 25, 364–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, L.; Gonzalez, F.J.; Kalow, W.; Tang, B.K. Biotransformation of caffeine, paraxanthine, theobromine and theophylline by cDNA-expressed human CYP1A2 and CYP2E1. Pharmacogenetics 1992, 2, 73–77. [Google Scholar] [CrossRef] [PubMed]
- De Galan, B.E.; Tack, C.J.; Lenders, J.W.; Pasman, J.W.; Elving, L.D.; Russel, F.G.; Lutterman, J.A.; Smits, P. Theophylline improves hypoglycemia unawareness in type 1 diabetes. Diabetes 2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landolt, H.P. Genotype-Dependent Differences in Sleep, Vigilance, and Response to Stimulants. Curr. Pharm. Des. 2008, 14, 3396–3407. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Tuttle, T.D.; Higgins, C.L. Energy beverages: Content and safety. Mayo Clin. Proc. 2010, 85, 1033–1041. [Google Scholar] [CrossRef] [Green Version]
- Steinke, L.; Lanfear, D.E.; Dhanapal, V.; Kalus, J.S. Effect of “energy drink” consumption on hemodynamic and electrocardiographic parameters in healthy young adults. Ann. Pharmacother. 2009. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 5-h Energy Original (CAF, Regular Strength) | 5-h Energy Decaf (DECAF) | ||||
|---|---|---|---|---|---|
| Ingredient | Amount | %Daily Value | Ingredient | Amount | %Daily Value |
| Vitamin B6 | 40 mg | 2000% | Vitamin B6 | 40 mg | 2000% |
| Folic Acid | 400 mcg | 100% | Folic Acid | 400 mcg | 100% |
| Vitamin B12 | 500 mcg | 8333% | Vitamin B12 | 500 mcg | 8333% |
| Sodium | 18 mg | <1% | Sodium | 18 mg | <1% |
| Niacin | 30 mg | 150% | Niacin | 0 mg | 0% |
| Caffeine | 215 mg | n/a | Caffeine | 6 mg | n/a |
| Energy Blend | 1870 mg | n/a | Energy Blend | 2009 mg | n/a |
| (Taurine, glucuronic acid, malic acid, N-Acetyl L-tyrosine, L-phenylalanine, caffeine, citicoline) | (Taurine, choline, glucuronic acid, N-Acetyl L-tyrosine, L-Phenylalanine, malic acid, caffeine) | ||||
| Other Ingredients: Purified water, natural and artificial flavors, sucralose, potassium sorbate, sodium benzoate, EDTA. | Other Ingredients: Purified water, natural and artificial flavors, sucralose, potassium sorbate, sodium benzoate, EDTA. | ||||
| Males | Females | |
|---|---|---|
| n | 10 | 10 |
| Age (years) | 16.4 ± 2.2 | 17.5 ± 2.2 |
| Height (m) | 1.75 ± 0.1 | 1.64 ± 0.1 |
| Weight (kg) | 72.3 ± 24.6 | 59.3 ± 4.3 |
| BMI | 23.1 ± 6.0 | 22.2 ± 2.2 |
| BP (Systolic) | 133 ± 15 | 111 ± 8 |
| BP (Diastolic) | 71 ± 9 | 62 ± 9 |
| % Fat | 17.3 ± 4.7 | 24.2 ± 4.5 |
| % Lean | 79.4 ± 4.3 | 72.4 ± 4.4 |
| Measure | Treatment | AUC Mean (SE) | p-Value |
|---|---|---|---|
| Ghrelin (pg/mL/120 min) | DECAF | 5208.2 (519.2) | p = 0.945 |
| CAF | 5173.6 (615.3) | ||
| PYY (pg/mL/120 min) | DECAF | 7530.1 (868.4) | p = 0.412 |
| CAF | 7771.1 (864.2) | ||
| Leptin (pg/mL/120 min) | DECAF | 536,471.8 (72,667.4) | p = 0.246 |
| CAF | 489,282.6 (67,250.3) | ||
| GIP (pg/mL/120 min) | DECAF | 2960.6 (565.8) | p = 0.915 |
| CAF | 3003.4 (517.0) | ||
| GLP-1(pmol/L/120 min | DECAF | 407.0 (47.8) | p = 0.438 |
| CAF | 383.2 (40.4) | ||
| Glucagon (ng/L/120 min) | DECAF | 3085.8 (508.1) | p = 0.998 |
| CAF | 2963.2 (347.7) | ||
| C-peptide (nmol/L/120 min) | DECAF | 115.0 (7.2) | p = 0.241 |
| CAF | 120.1 (6.7) |
| SNP | GENE | CHR | POSITION | GMAF | ALLELE | SCORE | COUNT |
|---|---|---|---|---|---|---|---|
| TT | 0 | 2 | |||||
| rs4410790 | AHR | 13 | 17284577 | C > T, 0.387 | CT | 1 | 11 |
| CC | 2 | 7 | |||||
| CC | 0 | 9 | |||||
| rs2470893 | CYP1A1-4011 | 15 | 75019449 | C > T, 0.278 | TC | 1 | 10 |
| TT | 2 | 1 | |||||
| CC | 0 | 12 | |||||
| rs2472297 | CYP1A1-12441 | 15 | 75027880 | C > T, 0.225 | TC | 1 | 8 |
| TT | 2 | 0 | |||||
| AA | 0 | 3 | |||||
| rs2472299 | CYP1A1 | 15 | 74741059 | G > A, 0.350 | GA | 1 | 5 |
| GG | 2 | 12 | |||||
| CC | 0 | 3 | |||||
| rs762551 | CYP1A2-163 | 15 | 75041917 | A > C, 0.674 | AC | 1 | 5 |
| AA | 2 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shearer, J.; Reimer, R.A.; Hittel, D.S.; Gault, M.A.; Vogel, H.J.; Klein, M.S. Caffeine-Containing Energy Shots Cause Acute Impaired Glucoregulation in Adolescents. Nutrients 2020, 12, 3850. https://doi.org/10.3390/nu12123850
Shearer J, Reimer RA, Hittel DS, Gault MA, Vogel HJ, Klein MS. Caffeine-Containing Energy Shots Cause Acute Impaired Glucoregulation in Adolescents. Nutrients. 2020; 12(12):3850. https://doi.org/10.3390/nu12123850
Chicago/Turabian StyleShearer, Jane, Raylene A. Reimer, Dustin S. Hittel, Mackenzie A. Gault, Hans J. Vogel, and Matthias S. Klein. 2020. "Caffeine-Containing Energy Shots Cause Acute Impaired Glucoregulation in Adolescents" Nutrients 12, no. 12: 3850. https://doi.org/10.3390/nu12123850