Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Human Vaginal Microbiota
3.1.1. Human Vaginal Microbiota: Role as a Natural Barrier
3.1.2. Composition of Vaginal Microbiota Is Defined but Highly Dynamic
3.2. Vaginal Dysbiosis: An Imbalance in Vaginal Microbiota Composition
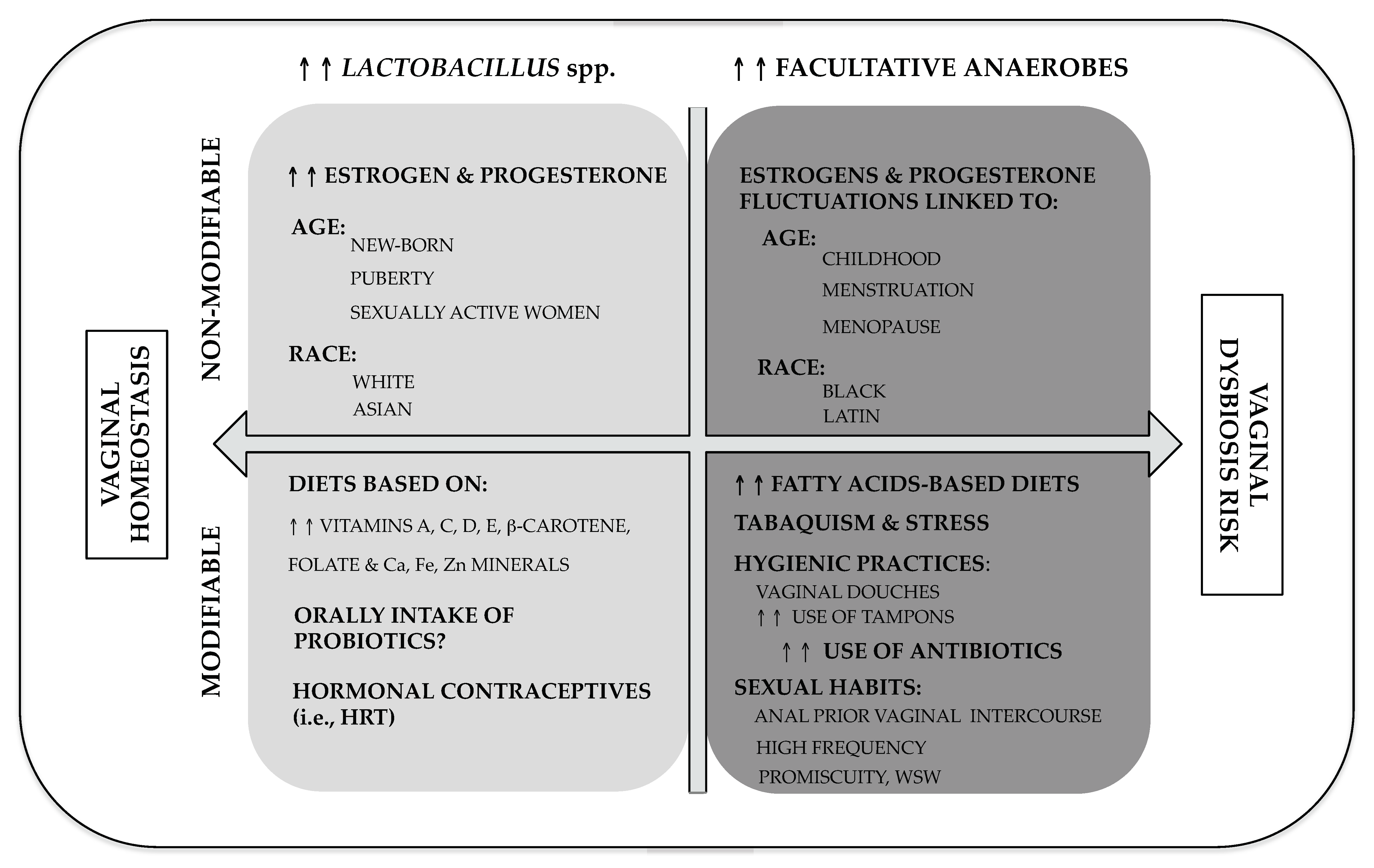
3.2.1. Risk Factors Associated with Vaginal Dysbiosis
Age and Hormone Physiology
Ethnicity
Tobacco
Stress
3.2.2. Other Factors That Influence Vaginal Dysbiosis
Sexual Activity
Lifestyle and Daily Practices
3.3. Pathogenesis Associated with Bacterial Vaginosis
3.3.1. Bacterial Vaginosis and Sexually Transmitted Diseases (STDs)
3.3.2. Bacterial Vaginosis and Pelvic Inflammatory Disease (PID)
3.3.3. Bacterial Vaginosis and Pregnancy
3.4. Impact of Nutrition in Maintaining Vaginal Homeostasis
3.4.1. Dietary Intake Consequences on Vaginal Homeostasis
3.4.2. Probiotics Influence on Vaginal Microbiota
Probiotics in Non-Pregnant Women
Probiotics in Pregnant Women
Other Results Obtained with Probiotics
3.5. Restoration of Vaginal Microbiota through Hormone Replacement Therapy (HRT)
3.6. Impact of Contraceptives on Vaginal Microbiota
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marchesi, J.R.; Ravel, J. The vocabulary of microbiome research: A proposal. Microbiome 2015, 3, 31. [Google Scholar] [CrossRef] [PubMed]
- Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Hamady, M.; Fraser-Liggett, C.M.; Knight, R.; Gordon, J.I. The human microbiome project. Nature 2007, 449, 804–810. [Google Scholar] [CrossRef] [PubMed]
- NIH Human Microbiome Project; National Institutes of Health: Bethesda, MD, USA. Available online: https://commonfund.nih.gov/hmp (accessed on 12 July 2019).
- Relman, D.A. The human microbiome and the future practice of medicine. JAMA 2015, 314, 1127–1128. [Google Scholar] [CrossRef]
- Fox, C.; Eichelberger, K. Maternal microbiome and pregnancy outcomes. Fertil. Steril. 2015, 104, 1358–1363. [Google Scholar] [CrossRef]
- Dethlefsen, L.; McFall-Ngai, M.; Relman, D.A. An ecological and evolutionary perspective on human-microbe mutualism and disease. Nature 2007, 449, 811–818. [Google Scholar] [CrossRef]
- Donders, G.G.; Bosmans, E.; Dekeersmaecker, A.; Vereecken, A.; Van Bulck, B.; Spitz, B. Pathogenesis of abnormal vaginal bacterial flora. Am. J. Obstet. Gynecol. 2000, 182, 872–878. [Google Scholar] [CrossRef]
- Gupta, K.; Stapleton, A.E.; Hooton, T.M.; Roberts, P.L.; Fennell, C.L.; Stamm, W.E. Inverse association of H2O2-producing lactobacilli and vaginal Escherichia coli colonization in women with recurrent urinary tract infections. J. Infect. Dis. 1998, 178, 446–450. [Google Scholar] [CrossRef]
- Pybus, V.; Onderdonk, A.B. Microbial interactions in the vaginal ecosystem, with emphasis on the pathogenesis of bacterial vaginosis. Microbes Infect. 1999, 1, 285–292. [Google Scholar] [CrossRef]
- Cherpes, T.L.; Meyn, L.A.; Krohn, M.A.; Lurie, J.G.; Hillier, S.L. Association between acquisition of herpes simplex virus type 2 in women and bacterial vaginosis. Clin. Infect. Dis. 2003, 37, 319–325. [Google Scholar] [CrossRef]
- Martin, H.L.; Richardson, B.A.; Nyange, P.M.; Lavreys, L.; Hillier, S.L.; Chohan, B.; Mandaliya, K.; Ndinya-Achola, J.O.; Bwayo, J.; Kreiss, J. Vaginal lactobacilli, microbial flora, and risk of human immunodeficiency virus type 1 and sexually transmitted disease acquisition. J. Infect. Dis. 1999, 180, 1863–1868. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D. Is there a protective role for vaginal flora? Curr. Infect. Dis. Rep. 1999, 1, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Watts, D.H.; Fazzari, M.; Minkoff, H.; Hillier, S.L.; Sha, B.; Glesby, M.; Levine, A.M.; Burk, R.; Palefsky, J.M.; Moxley, M.; et al. Effects of bacterial vaginosis and other genital infections on the natural history of human papillomavirus infection in HIV-1-infected and high-risk HIV-1-uninfected women. J. Infect. Dis. 2005, 191, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Wiesenfeld, H.C.; Hillier, S.L.; Krohn, M.A.; Landers, D.V.; Sweet, R.L. Bacterial vaginosis is a strong predictor of Neisseria gonorrhoeae and Chlamydia trachomatis infection. Clin. Infect. Dis. 2003, 36, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.K.; Hida, K.; Shukair, S.; Wang, Y.Y.; Figueiredo, A.; Cone, R.; Hope, T.J.; Hanes, J. Human immunodeficiency virus type 1 is trapped by acidic but not by neutralized human cervicovaginal mucus. J. Virol. 2009, 83, 11196–11200. [Google Scholar] [CrossRef]
- Taha, T.E.; Hoover, D.R.; Dallabetta, G.A.; Kumwenda, N.I.; Mtimavalye, L.A.; Yang, L.P.; Liomba, G.N.; Broadhead, R.L.; Chiphangwi, J.D.; Miotti, P.G. Bacterial vaginosis and disturbances of vaginal flora: Association with increased acquisition of HIV. AIDS 1998, 12, 1699–1706. [Google Scholar] [CrossRef]
- Ryckman, K.K.; Simhan, H.N.; Krohn, M.A.; Williams, S.M. Predicting risk of bacterial vaginosis: The role of race, smoking and corticotropin-releasing hormone-related genes. Mol. Hum. Reprod. 2009, 15, 131–137. [Google Scholar] [CrossRef]
- Sobel, J.D. Bacterial vaginosis. Annu. Rev. Med. 2000, 51, 349–356. [Google Scholar] [CrossRef]
- Brotman, R.M. Vaginal microbiome and sexually transmitted infections: An epidemiologic perspective. J. Clin. Investig. 2011, 121, 4610–4617. [Google Scholar] [CrossRef]
- Zhou, X.; Brown, C.J.; Abdo, Z.; Davis, C.C.; Hansmann, M.A.; Joyce, P.; Foster, J.A.; Forney, L.J. Differences in the composition of vaginal microbial communities found in healthy Caucasian and black women. ISME J. 2007, 1, 121–133. [Google Scholar] [CrossRef]
- van de Wijgert, J.H.; Borgdorff, H.; Verhelst, R.; Crucitti, T.; Francis, S.; Verstraelen, H.; Jespers, V. The vaginal microbiota: What have we learned after a decade of molecular characterization? PLoS ONE 2014, 9, e105998. [Google Scholar] [CrossRef] [PubMed]
- Fredricks, D.N.; Fiedler, T.L.; Marrazzo, J.M. Molecular identification of bacteria associated with bacterial vaginosis. N. Engl. J. Med. 2005, 353, 1899–1911. [Google Scholar] [CrossRef] [PubMed]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4680–4687. [Google Scholar] [CrossRef]
- Jespers, V.; Menten, J.; Smet, H.; Poradosu, S.; Abdellati, S.; Verhelst, R.; Hardy, L.; Buve, A.; Crucitti, T. Quantification of bacterial species of the vaginal microbiome in different groups of women, using nucleic acid amplification tests. BMC Microbiol. 2012, 12, 83. [Google Scholar] [CrossRef] [PubMed]
- Allsworth, J.E.; Peipert, J.F. Severity of bacterial vaginosis and the risk of sexually transmitted infection. Am. J. Obstet. Gynecol. 2011, 205, 113.e111–e116. [Google Scholar] [CrossRef] [PubMed]
- Spear, G.T.; St John, E.; Zariffard, M.R. Bacterial vaginosis and human immunodeficiency virus infection. AIDS Res. Ther. 2007, 4, 25. [Google Scholar] [CrossRef]
- Lamont, R.F.; Taylor-Robinson, D. The role of bacterial vaginosis, aerobic vaginitis, abnormal vaginal flora and the risk of preterm birth. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 119–120. [Google Scholar] [CrossRef]
- Larsson, P.G.; Platz-Christensen, J.J.; Dalaker, K.; Eriksson, K.; Fahraeus, L.; Irminger, K.; Jerve, F.; Stray-Pedersen, B.; Wolner-Hanssen, P. Treatment with 2% clindamycin vaginal cream prior to first trimester surgical abortion to reduce signs of postoperative infection: A prospective, double-blinded, placebo-controlled, multicenter study. Acta Obstet. Gynecol. Scand. 2000, 79, 390–396. [Google Scholar] [CrossRef]
- Llahi-Camp, J.M.; Rai, R.; Ison, C.; Regan, L.; Taylor-Robinson, D. Association of bacterial vaginosis with a history of second trimester miscarriage. Hum. Reprod. 1996, 11, 1575–1578. [Google Scholar] [CrossRef]
- Jacobsson, B.; Pernevi, P.; Chidekel, L.; Jorgen Platz-Christensen, J. Bacterial vaginosis in early pregnancy may predispose for preterm birth and postpartum endometritis. Acta Obstet. Gynecol. Scand. 2002, 81, 1006–1010. [Google Scholar] [CrossRef]
- Ma, B.; Forney, L.J.; Ravel, J. Vaginal microbiome: Rethinking health and disease. Annu. Rev. Microbiol. 2012, 66, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Aldunate, M.; Srbinovski, D.; Hearps, A.C.; Latham, C.F.; Ramsland, P.A.; Gugasyan, R.; Cone, R.A.; Tachedjian, G. Antimicrobial and immune modulatory effects of lactic acid and short chain fatty acids produced by vaginal microbiota associated with eubiosis and bacterial vaginosis. Front. Physiol. 2015, 6, 164. [Google Scholar] [CrossRef] [PubMed]
- Gajer, P.; Brotman, R.M.; Bai, G.; Sakamoto, J.; Schutte, U.M.; Zhong, X.; Koenig, S.S.; Fu, L.; Ma, Z.S.; Zhou, X.; et al. Temporal dynamics of the human vaginal microbiota. Sci. Transl. Med. 2012, 4, 132–152. [Google Scholar] [CrossRef] [PubMed]
- Boris, S.; Suarez, J.E.; Vazquez, F.; Barbes, C. Adherence of human vaginal lactobacilli to vaginal epithelial cells and interaction with uropathogens. Infect. Immun. 1998, 66, 1985–1989. [Google Scholar] [CrossRef]
- Martin, R.; Soberon, N.; Vazquez, F.; Suarez, J.E. Vaginal microbiota: Composition, protective role, associated pathologies, and therapeutic perspectives. Enferm. Infecc. Microbiol. Clin. 2008, 26, 160–167. [Google Scholar] [CrossRef]
- Strus, M.; Brzychczy-Wloch, M.; Gosiewski, T.; Kochan, P.; Heczko, P.B. The in vitro effect of hydrogen peroxide on vaginal microbial communities. FEMS Immunol. Med. Microbiol. 2006, 48, 56–63. [Google Scholar] [CrossRef]
- DiGiulio, D.B.; Callahan, B.J.; McMurdie, P.J.; Costello, E.K.; Lyell, D.J.; Robaczewska, A.; Sun, C.L.; Goltsman, D.S.; Wong, R.J.; Shaw, G.; et al. Temporal and spatial variation of the human microbiota during pregnancy. Proc. Natl. Acad. Sci. USA 2015, 112, 11060–11065. [Google Scholar] [CrossRef]
- Bradshaw, C.S.; Brotman, R.M. Making inroads into improving treatment of bacterial vaginosis—Striving for long-term cure. BMC Infect. Dis. 2015, 15, 292. [Google Scholar] [CrossRef]
- Srinivasan, S.; Liu, C.; Mitchell, C.M.; Fiedler, T.L.; Thomas, K.K.; Agnew, K.J.; Marrazzo, J.M.; Fredricks, D.N. Temporal variability of human vaginal bacteria and relationship with bacterial vaginosis. PLoS ONE 2010, 5, e10197. [Google Scholar] [CrossRef]
- Pyles, R.B.; Vincent, K.L.; Baum, M.M.; Elsom, B.; Miller, A.L.; Maxwell, C.; Eaves-Pyles, T.D.; Li, G.; Popov, V.L.; Nusbaum, R.J.; et al. Cultivated vaginal microbiomes alter HIV-1 infection and antiretroviral efficacy in colonized epithelial multilayer cultures. PLoS ONE 2014, 9, e93419. [Google Scholar] [CrossRef]
- Hanff, P.A.; Rosol-Donoghue, J.A.; Spiegel, C.A.; Wilson, K.H.; Moore, L.H. Leptotrichia sanguinegens sp. nov., a new agent of postpartum and neonatal bacteremia. Clin. Infect. Dis. 1995, 20 (Suppl. 2), S237–S239. [Google Scholar] [CrossRef] [PubMed]
- Geissdorfer, W.; Bohmer, C.; Pelz, K.; Schoerner, C.; Frobenius, W.; Bogdan, C. Tuboovarian abscess caused by Atopobium vaginae following transvaginal oocyte recovery. J. Clin. Microbiol. 2003, 41, 2788–2790. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, Y.; Mikamo, H.; Tanaka, K.; Watanabe, K. A case of uterine endometritis caused by Atopobium vaginae. J. Infect. Chemother. 2011, 17, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Knoester, M.; Lashley, L.E.; Wessels, E.; Oepkes, D.; Kuijper, E.J. First report of Atopobium vaginae bacteremia with fetal loss after chorionic villus sampling. J. Clin. Microbiol. 2011, 49, 1684–1686. [Google Scholar] [CrossRef]
- Adimora, A.A.; Schoenbach, V.J.; Doherty, I.A. Concurrent sexual partnerships among men in the United States. Am. J. Public Health 2007, 97, 2230–2237. [Google Scholar] [CrossRef]
- Nagy, E.; Froman, G.; Mardh, P.A. Fibronectin binding of Lactobacillus species isolated from women with and without bacterial vaginosis. J. Med. Microbiol. 1992, 37, 38–42. [Google Scholar] [CrossRef]
- Smith, S.B.; Ravel, J. The vaginal microbiota, host defence and reproductive physiology. J. Physiol. 2017, 595, 451–463. [Google Scholar] [CrossRef]
- Boskey, E.R.; Cone, R.A.; Whaley, K.J.; Moench, T.R. Origins of vaginal acidity: High D/L lactate ratio is consistent with bacteria being the primary source. Hum. Reprod. 2001, 16, 1809–1813. [Google Scholar] [CrossRef]
- Mossop, H.; Linhares, I.M.; Bongiovanni, A.M.; Ledger, W.J.; Witkin, S.S. Influence of lactic acid on endogenous and viral RNA-induced immune mediator production by vaginal epithelial cells. Obstet. Gynecol. 2011, 118, 840–846. [Google Scholar] [CrossRef]
- Gartner, L.; Hiatt, J. Atlas de Histología; McGraw-Hill: New York, NY, USA, 2008. [Google Scholar]
- Amabebe, E.; Anumba, D.O.C. The vaginal microenvironment: The physiologic role of lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef]
- Lewis, F.M.; Bernstein, K.T.; Aral, S.O. Vaginal microbiome and its relationship to behavior, sexual health, and sexually transmitted diseases. Obstet. Gynecol. 2017, 129, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Borgogna, J.-L.C.; Yeoman, C.J. The application of molecular methods towards an understanding of the role of the vaginal microbiome in health and disease. In Methods in Microbiology; Elsevier: Amsterdam, The Netherlands, 2017; Volume 44, pp. 37–91. [Google Scholar]
- Yamamoto, T.; Zhou, X.; Williams, C.J.; Hochwalt, A.; Forney, L.J. Bacterial populations in the vaginas of healthy adolescent women. J. Pediatric Adolesc. Gynecol. 2009, 22, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Hickey, R.J.; Zhou, X.; Pierson, J.D.; Ravel, J.; Forney, L.J. Understanding vaginal microbiome complexity from an ecological perspective. Transl. Res. J. Lab. Clin. Med. 2012, 160, 267–282. [Google Scholar] [CrossRef] [PubMed]
- Hyman, R.W.; Herndon, C.N.; Jiang, H.; Palm, C.; Fukushima, M.; Bernstein, D.; Vo, K.C.; Zelenko, Z.; Davis, R.W.; Giudice, L.C. The dynamics of the vaginal microbiome during infertility therapy with in vitro fertilization-embryo transfer. J. Assist. Reprod. Genet. 2012, 29, 105–115. [Google Scholar] [CrossRef]
- Brotman, R.M.; Ravel, J.; Bavoil, P.M.; Gravitt, P.E.; Ghanem, K.G. Microbiome, sex hormones, and immune responses in the reproductive tract: Challenges for vaccine development against sexually transmitted infections. Vaccine 2014, 32, 1543–1552. [Google Scholar] [CrossRef]
- Srinivasan, S.; Hoffman, N.G.; Morgan, M.T.; Matsen, F.A.; Fiedler, T.L.; Hall, R.W.; Ross, F.J.; McCoy, C.O.; Bumgarner, R.; Marrazzo, J.M.; et al. Bacterial communities in women with bacterial vaginosis: High resolution phylogenetic analyses reveal relationships of microbiota to clinical criteria. PLoS ONE 2012, 7, e37818. [Google Scholar] [CrossRef]
- Petrova, M.I.; van den Broek, M.; Balzarini, J.; Vanderleyden, J.; Lebeer, S. Vaginal microbiota and its role in HIV transmission and infection. FEMS Microbiol. Rev. 2013, 37, 762–792. [Google Scholar] [CrossRef]
- Beghini, J.; Linhares, I.M.; Giraldo, P.C.; Ledger, W.J.; Witkin, S.S. Differential expression of lactic acid isomers, extracellular matrix metalloproteinase inducer, and matrix metalloproteinase-8 in vaginal fluid from women with vaginal disorders. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 1580–1585. [Google Scholar] [CrossRef]
- Verstraelen, H.; Verhelst, R.; Claeys, G.; De Backer, E.; Temmerman, M.; Vaneechoutte, M. Longitudinal analysis of the vaginal microflora in pregnancy suggests that L. crispatus promotes the stability of the normal vaginal microflora and that L. gasseri and/or L. iners are more conducive to the occurrence of abnormal vaginal microflora. BMC Microbiol. 2009, 9, 116. [Google Scholar] [CrossRef]
- Aagaard, K.; Riehle, K.; Ma, J.; Segata, N.; Mistretta, T.A.; Coarfa, C.; Raza, S.; Rosenbaum, S.; Van den Veyver, I.; Milosavljevic, A.; et al. A metagenomic approach to characterization of the vaginal microbiome signature in pregnancy. PLoS ONE 2012, 7, e36466. [Google Scholar] [CrossRef]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Bieda, J.; Chaemsaithong, P.; Miranda, J.; Chaiworapongsa, T.; Ravel, J. The vaginal microbiota of pregnant women who subsequently have spontaneous preterm labor and delivery and those with a normal delivery at term. Microbiome 2014, 2, 18. [Google Scholar] [CrossRef]
- DiGiulio, D.B. Diversity of microbes in amniotic fluid. Semin. Fetal Neonatal Med. 2012, 17, 2–11. [Google Scholar] [CrossRef]
- Bradley, F.; Birse, K.; Hasselrot, K.; Noel-Romas, L.; Introini, A.; Wefer, H.; Seifert, M.; Engstrand, L.; Tjernlund, A.; Broliden, K.; et al. The vaginal microbiome amplifies sex hormone-associated cyclic changes in cervicovaginal inflammation and epithelial barrier disruption. Am. J. Reprod. Immunol. 2018, 80, e12863. [Google Scholar] [CrossRef]
- Brotman, R.; Gajer, P.; Holm, J.; Robinson, C.; Ma, B.; Humphrys, M.; Tuddenham, S.; Ravel, J.; Ghanem, K. 4: Hormonal contraception is associated with stability and lactobacillus-dominance of the vaginal microbiota in a two-year observational study. Am. J. Obstet. Gynecol. 2016, 215, S828–S829. [Google Scholar] [CrossRef]
- Borgdorff, H.; Tsivtsivadze, E.; Verhelst, R.; Marzorati, M.; Jurriaans, S.; Ndayisaba, G.F.; Schuren, F.H.; van de Wijgert, J.H. Lactobacillus-dominated cervicovaginal microbiota associated with reduced HIV/STI prevalence and genital HIV viral load in African women. ISME J. 2014, 8, 1781–1793. [Google Scholar] [CrossRef]
- Miller, E.A.; Beasley, D.E.; Dunn, R.R.; Archie, E.A. Lactobacilli dominance and vaginal pH: Why is the human vaginal microbiome unique? Front. Microbiol. 2016, 7, 1936. [Google Scholar] [CrossRef]
- Brotman, R.M.; He, X.; Gajer, P.; Fadrosh, D.; Sharma, E.; Mongodin, E.F.; Ravel, J.; Glover, E.D.; Rath, J.M. Association between cigarette smoking and the vaginal microbiota: A pilot study. BMC Infect. Dis. 2014, 14, 471. [Google Scholar] [CrossRef]
- Shiraishi, T.; Fukuda, K.; Morotomi, N.; Imamura, Y.; Mishima, J.; Imai, S.; Miyazawa, K.; Taniguchi, H. Influence of menstruation on the microbiota of healthy women’s labia minora as analyzed using a 16S rRNA gene-based clone library method. Jpn. J. Infect. Dis. 2011, 64, 76–80. [Google Scholar]
- Mitchell, C.M.; Fredricks, D.N.; Winer, R.L.; Koutsky, L. Effect of sexual debut on vaginal microbiota in a cohort of young women. Obstet. Gynecol. 2012, 120, 1306–1313. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef]
- Kenyon, C.; Colebunders, R.; Crucitti, T. The global epidemiology of bacterial vaginosis: A systematic review. Am. J. Obstet. Gynecol. 2013, 209, 505–523. [Google Scholar] [CrossRef]
- Neggers, Y.H.; Nansel, T.R.; Andrews, W.W.; Schwebke, J.R.; Yu, K.F.; Goldenberg, R.L.; Klebanoff, M.A. Dietary intake of selected nutrients affects bacterial vaginosis in women. J. Nutr. 2007, 137, 2128–2133. [Google Scholar] [CrossRef]
- Hickey, R.J.; Abdo, Z.; Zhou, X.; Nemeth, K.; Hansmann, M.; Osborn, T.W., III; Wang, F.; Forney, L.J. Effects of tampons and menses on the composition and diversity of vaginal microbial communities over time. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 695–704, discussion 704–696. [Google Scholar] [CrossRef]
- Peipert, J.F.; Lapane, K.L.; Allsworth, J.E.; Redding, C.A.; Blume, J.D.; Stein, M.D. Bacterial vaginosis, race, and sexually transmitted infections: Does race modify the association? Sex. Transm. Dis. 2008, 35, 363–367. [Google Scholar] [CrossRef]
- Koumans, E.H.; Sternberg, M.; Bruce, C.; McQuillan, G.; Kendrick, J.; Sutton, M.; Markowitz, L.E. The prevalence of bacterial vaginosis in the United States, 2001-2004; associations with symptoms, sexual behaviors, and reproductive health. Sex. Transm. Dis. 2007, 34, 864–869. [Google Scholar] [CrossRef]
- Fettweis, J.M.; Brooks, J.P.; Serrano, M.G.; Sheth, N.U.; Girerd, P.H.; Edwards, D.J.; Strauss, J.F.; the Vaginal Microbiome, C.; Jefferson, K.K.; Buck, G.A. Differences in vaginal microbiome in African American women versus women of European ancestry. Microbiology 2014, 160, 2272–2282. [Google Scholar] [CrossRef]
- Gautam, R.; Borgdorff, H.; Jespers, V.; Francis, S.C.; Verhelst, R.; Mwaura, M.; Delany-Moretlwe, S.; Ndayisaba, G.; Kyongo, J.K.; Hardy, L.; et al. Correlates of the molecular vaginal microbiota composition of African women. BMC Infect. Dis. 2015, 15, 86. [Google Scholar] [CrossRef]
- Jespers, V.; van de Wijgert, J.; Cools, P.; Verhelst, R.; Verstraelen, H.; Delany-Moretlwe, S.; Mwaura, M.; Ndayisaba, G.F.; Mandaliya, K.; Menten, J.; et al. The significance of Lactobacillus crispatus and L. vaginalis for vaginal health and the negative effect of recent sex: A cross-sectional descriptive study across groups of African women. BMC Infect. Dis. 2015, 15, 115. [Google Scholar] [CrossRef]
- Borgdorff, H.; van der Veer, C.; van Houdt, R.; Alberts, C.J.; de Vries, H.J.; Bruisten, S.M.; Snijder, M.B.; Prins, M.; Geerlings, S.E.; Schim van der Loeff, M.F.; et al. The association between ethnicity and vaginal microbiota composition in Amsterdam, the Netherlands. PLoS ONE 2017, 12, e0181135. [Google Scholar] [CrossRef]
- Blekhman, R.; Goodrich, J.K.; Huang, K.; Sun, Q.; Bukowski, R.; Bell, J.T.; Spector, T.D.; Keinan, A.; Ley, R.E.; Gevers, D.; et al. Host genetic variation impacts microbiome composition across human body sites. Genome Biol. 2015, 16, 191. [Google Scholar] [CrossRef]
- Onywera, H.; Williamson, A.L.; Mbulawa, Z.Z.A.; Coetzee, D.; Meiring, T.L. Factors associated with the composition and diversity of the cervical microbiota of reproductive-age Black South African women: A retrospective cross-sectional study. PeerJ 2019, 7, e7488. [Google Scholar] [CrossRef] [PubMed]
- Cherpes, T.L.; Hillier, S.L.; Meyn, L.A.; Busch, J.L.; Krohn, M.A. A delicate balance: Risk factors for acquisition of bacterial vaginosis include sexual activity, absence of hydrogen peroxide-producing lactobacilli, black race, and positive herpes simplex virus type 2 serology. Sex. Transm. Dis. 2008, 35, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.M.; Borgogna, J.C.; Michalek, R.D.; Roberts, D.W.; Rath, J.M.; Glover, E.D.; Ravel, J.; Shardell, M.D.; Yeoman, C.J.; Brotman, R.M. Cigarette smoking is associated with an altered vaginal tract metabolomic profile. Sci. Rep. 2018, 8, 852. [Google Scholar] [CrossRef]
- Chrousos, G.P. Regulation and dysregulation of the hypothalamic-pituitary-adrenal axis. The corticotropin-releasing hormone perspective. Endocrinol. Metab. Clin. N. Am. 1992, 21, 833–858. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Culhane, J.F.; Rauh, V.; Barve, S.S. Stress and preterm birth: Neuroendocrine, immune/inflammatory, and vascular mechanisms. Matern. Child Health J. 2001, 5, 119–125. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Culhane, J.F.; Rauh, V.; Barve, S.S.; Hogan, V.; Sandman, C.A.; Hobel, C.J.; Chicz-DeMet, A.; Dunkel-Schetter, C.; Garite, T.J.; et al. Stress, infection and preterm birth: A biobehavioural perspective. Paediatr. Perinat. Epidemiol. 2001, 15 (Suppl. 2), 17–29. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. Psychosocial stress, cortisol levels, and maintenance of vaginal health. Front. Endocrinol. 2018, 9, 568. [Google Scholar] [CrossRef]
- Fethers, K.A.; Fairley, C.K.; Hocking, J.S.; Gurrin, L.C.; Bradshaw, C.S. Sexual risk factors and bacterial vaginosis: A systematic review and meta-analysis. Clin. Infect. Dis. 2008, 47, 1426–1435. [Google Scholar] [CrossRef]
- Jespers, V.; Crucitti, T.; Menten, J.; Verhelst, R.; Mwaura, M.; Mandaliya, K.; Ndayisaba, G.F.; Delany-Moretlwe, S.; Verstraelen, H.; Hardy, L.; et al. Prevalence and correlates of bacterial vaginosis in different sub-populations of women in sub-Saharan Africa: A cross-sectional study. PLoS ONE 2014, 9, e109670. [Google Scholar] [CrossRef]
- Forcey, D.S.; Vodstrcil, L.A.; Hocking, J.S.; Fairley, C.K.; Law, M.; McNair, R.P.; Bradshaw, C.S. Factors associated with bacterial vaginosis among women who have sex with women: A systematic review. PLoS ONE 2015, 10, e0141905. [Google Scholar] [CrossRef]
- Marrazzo, J.M.; Fiedler, T.L.; Srinivasan, S.; Thomas, K.K.; Liu, C.; Ko, D.; Xie, H.; Saracino, M.; Fredricks, D.N. Extravaginal reservoirs of vaginal bacteria as risk factors for incident bacterial vaginosis. J. Infect. Dis. 2012, 205, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Simon, C. Introduction: Do microbes in the female reproductive function matter? Fertil. Steril. 2018, 110, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Brotman, R.M.; Klebanoff, M.A.; Nansel, T.R.; Andrews, W.W.; Schwebke, J.R.; Zhang, J.; Yu, K.F.; Zenilman, J.M.; Scharfstein, D.O. A longitudinal study of vaginal douching and bacterial vaginosis—A marginal structural modeling analysis. Am. J. Epidemiol. 2008, 168, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Low, N.; Chersich, M.F.; Schmidlin, K.; Egger, M.; Francis, S.C.; van de Wijgert, J.H.; Hayes, R.J.; Baeten, J.M.; Brown, J.; Delany-Moretlwe, S.; et al. Intravaginal practices, bacterial vaginosis, and HIV infection in women: Individual participant data meta-analysis. PLoS Med. 2011, 8, e1000416. [Google Scholar] [CrossRef]
- Fashemi, B.; Delaney, M.L.; Onderdonk, A.B.; Fichorova, R.N. Effects of feminine hygiene products on the vaginal mucosal biome. Microb. Ecol. Health Dis. 2013, 24. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.M.J.; Holmes, K.K. Bacterial vaginosis. In Sexually Transmitted Diseases, 4th ed.; Holmes, K.K., Sparling, P.F., Mardh, P.A., Eds.; McGraw-Hill: New York, NY, USA, 2008; pp. 737–768. [Google Scholar]
- Schwebke, J.R. Abnormal vaginal flora as a biological risk factor for acquisition of HIV infection and sexually transmitted diseases. J. Infect. Dis. 2005, 192, 1315–1317. [Google Scholar] [CrossRef] [PubMed]
- St Amant, D.C.; Valentin-Bon, I.E.; Jerse, A.E. Inhibition of Neisseria gonorrhoeae by Lactobacillus species that are commonly isolated from the female genital tract. Infect. Immun. 2002, 70, 7169–7171. [Google Scholar] [CrossRef]
- Kalyoussef, S.; Nieves, E.; Dinerman, E.; Carpenter, C.; Shankar, V.; Oh, J.; Burd, B.; Angeletti, R.H.; Buckheit, K.W.; Fredricks, D.N.; et al. Lactobacillus proteins are associated with the bactericidal activity against E. coli of female genital tract secretions. PLoS ONE 2012, 7, e49506. [Google Scholar] [CrossRef]
- Brotman, R.M.; Klebanoff, M.A.; Nansel, T.R.; Yu, K.F.; Andrews, W.W.; Zhang, J.; Schwebke, J.R. Bacterial vaginosis assessed by gram stain and diminished colonization resistance to incident gonococcal, chlamydial, and trichomonal genital infection. J. Infect. Dis. 2010, 202, 1907–1915. [Google Scholar] [CrossRef]
- Schwebke, J.R.; Desmond, R. A randomized trial of metronidazole in asymptomatic bacterial vaginosis to prevent the acquisition of sexually transmitted diseases. Am. J. Obstet. Gynecol. 2007, 196, 517.e511–e516. [Google Scholar] [CrossRef]
- Schwebke, J.R.; Lee, J.Y.; Lensing, S.; Philip, S.S.; Wiesenfeld, H.C.; Sena, A.C.; Trainor, N.; Acevado, N.; Saylor, L.; Rompalo, A.M.; et al. Home screening for bacterial vaginosis to prevent sexually transmitted diseases. Clin. Infect. Dis. 2016, 62, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Sutton, M.; Sternberg, M.; Koumans, E.H.; McQuillan, G.; Berman, S.; Markowitz, L. The prevalence of Trichomonas vaginalis infection among reproductive-age women in the United States, 2001–2004. Clin. Infect. Dis. 2007, 45, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Mirmonsef, P.; Krass, L.; Landay, A.; Spear, G.T. The role of bacterial vaginosis and trichomonas in HIV transmission across the female genital tract. Curr. HIV Res. 2012, 10, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Fichorova, R.N.; Buck, O.R.; Yamamoto, H.S.; Fashemi, T.; Dawood, H.Y.; Fashemi, B.; Hayes, G.R.; Beach, D.H.; Takagi, Y.; Delaney, M.L.; et al. The villain team-up or how Trichomonas vaginalis and bacterial vaginosis alter innate immunity in concert. Sex. Transm. Infect. 2013, 89, 460–466. [Google Scholar] [CrossRef]
- Balkus, J.E.; Richardson, B.A.; Rabe, L.K.; Taha, T.E.; Mgodi, N.; Kasaro, M.P.; Ramjee, G.; Hoffman, I.F.; Abdool Karim, S.S. Bacterial vaginosis and the risk of trichomonas vaginalis acquisition among HIV-1-negative women. Sex. Transm. Dis. 2014, 41, 123–128. [Google Scholar] [CrossRef]
- Brotman, R.M.; Bradford, L.L.; Conrad, M.; Gajer, P.; Ault, K.; Peralta, L.; Forney, L.J.; Carlton, J.M.; Abdo, Z.; Ravel, J. Association between Trichomonas vaginalis and vaginal bacterial community composition among reproductive-age women. Sex. Transm. Dis. 2012, 39, 807–812. [Google Scholar] [CrossRef]
- Fastring, D.R.; Amedee, A.; Gatski, M.; Clark, R.A.; Mena, L.A.; Levison, J.; Schmidt, N.; Rice, J.; Gustat, J.; Kissinger, P. Co-occurrence of Trichomonas vaginalis and bacterial vaginosis and vaginal shedding of HIV-1 RNA. Sex. Transm. Dis. 2014, 41, 173–179. [Google Scholar] [CrossRef]
- Nagot, N.; Ouedraogo, A.; Defer, M.C.; Vallo, R.; Mayaud, P.; Van de Perre, P. Association between bacterial vaginosis and Herpes simplex virus type-2 infection: Implications for HIV acquisition studies. Sex. Transm. Infect. 2007, 83, 365–368. [Google Scholar] [CrossRef]
- Allsworth, J.E.; Lewis, V.A.; Peipert, J.F. Viral sexually transmitted infections and bacterial vaginosis: 2001–2004 National health and nutrition examination survey data. Sex. Transm. Dis. 2008, 35, 791–796. [Google Scholar] [CrossRef]
- Esber, A.; Vicetti Miguel, R.D.; Cherpes, T.L.; Klebanoff, M.A.; Gallo, M.F.; Turner, A.N. Risk of bacterial vaginosis among women with herpes simplex virus type 2 infection: A systematic review and meta-analysis. J. Infect. Dis. 2015, 212, 8–17. [Google Scholar] [CrossRef]
- Oh, J.E.; Kim, B.C.; Chang, D.H.; Kwon, M.; Lee, S.Y.; Kang, D.; Kim, J.Y.; Hwang, I.; Yu, J.W.; Nakae, S.; et al. Dysbiosis-induced IL-33 contributes to impaired antiviral immunity in the genital mucosa. Proc. Natl. Acad. Sci. USA 2016, 113, E762–E771. [Google Scholar] [CrossRef] [PubMed]
- Abbai, N.S.; Nyirenda, M.; Naidoo, S.; Ramjee, G. Prevalent herpes simplex virus-2 increases the risk of incident bacterial vaginosis in women from South Africa. AIDS Behav. 2018, 22, 2172–2180. [Google Scholar] [CrossRef] [PubMed]
- King, C.C.; Jamieson, D.J.; Wiener, J.; Cu-Uvin, S.; Klein, R.S.; Rompalo, A.M.; Shah, K.V.; Sobel, J.D. Bacterial vaginosis and the natural history of human papillomavirus. Infect. Dis. Obstet. Gynecol. 2011, 2011, 319460. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Lee, S.; Lee, H.; Song, Y.M.; Lee, K.; Han, M.J.; Sung, J.; Ko, G. Association of the vaginal microbiota with human papillomavirus infection in a Korean twin cohort. PLoS ONE 2013, 8, e63514. [Google Scholar] [CrossRef] [PubMed]
- Brotman, R.M.; Shardell, M.D.; Gajer, P.; Tracy, J.K.; Zenilman, J.M.; Ravel, J.; Gravitt, P.E. Interplay between the temporal dynamics of the vaginal microbiota and human papillomavirus detection. J. Infect. Dis. 2014, 210, 1723–1733. [Google Scholar] [CrossRef]
- Mitra, A.; MacIntyre, D.A.; Lee, Y.S.; Smith, A.; Marchesi, J.R.; Lehne, B.; Bhatia, R.; Lyons, D.; Paraskevaidis, E.; Li, J.V.; et al. Cervical intraepithelial neoplasia disease progression is associated with increased vaginal microbiome diversity. Sci. Rep. 2015, 5, 16865. [Google Scholar] [CrossRef]
- Dahoud, W.; Michael, C.W.; Gokozan, H.; Nakanishi, A.K.; Harbhajanka, A. Association of bacterial vaginosis and human papilloma virus infection with cervical squamous intraepithelial lesions. Am. J. Clin. Pathol. 2019, 152, 185–189. [Google Scholar] [CrossRef]
- Sanchez-Garcia, E.K.; Contreras-Paredes, A.; Martinez-Abundis, E.; Garcia-Chan, D.; Lizano, M.; de la Cruz-Hernandez, E. Molecular epidemiology of bacterial vaginosis and its association with genital micro-organisms in asymptomatic women. J. Med. Microbiol. 2019, 68, 1373–1382. [Google Scholar] [CrossRef]
- Atashili, J.; Poole, C.; Ndumbe, P.M.; Adimora, A.A.; Smith, J.S. Bacterial vaginosis and HIV acquisition: A meta-analysis of published studies. AIDS 2008, 22, 1493–1501. [Google Scholar] [CrossRef]
- Nunn, K.L.; Wang, Y.Y.; Harit, D.; Humphrys, M.S.; Ma, B.; Cone, R.; Ravel, J.; Lai, S.K. Enhanced trapping of HIV-1 by human cervicovaginal mucus is associated with lactobacillus crispatus-dominant microbiota. mBio 2015, 6. [Google Scholar] [CrossRef]
- Cone, R.A. Vaginal microbiota and sexually transmitted infections that may influence transmission of cell-associated HIV. J. Infect. Dis. 2014, 210 (Suppl. 3), S616–S621. [Google Scholar] [CrossRef]
- Sabo, M.C.; Lehman, D.A.; Wang, B.; Richardson, B.A.; Srinivasan, S.; Osborn, L.; Matemo, D.; Kinuthia, J.; Fiedler, T.L.; Munch, M.M.; et al. Associations between vaginal bacteria implicated in HIV acquisition risk and proinflammatory cytokines and chemokines. Sex. Transm. Infect. 2019. [Google Scholar] [CrossRef] [PubMed]
- Westrom, L.; Joesoef, R.; Reynolds, G.; Hagdu, A.; Thompson, S.E. Pelvic inflammatory disease and fertility. A cohort study of 1844 women with laparoscopically verified disease and 657 control women with normal laparoscopic results. Sex. Transm. Dis. 1992, 19, 185–192. [Google Scholar] [CrossRef]
- Ness, R.B.; Soper, D.E.; Holley, R.L.; Peipert, J.; Randall, H.; Sweet, R.L.; Sondheimer, S.J.; Hendrix, S.L.; Amortegui, A.; Trucco, G.; et al. Effectiveness of inpatient and outpatient treatment strategies for women with pelvic inflammatory disease: Results from the Pelvic Inflammatory Disease Evaluation and Clinical Health (PEACH) randomized trial. Am. J. Obstet. Gynecol. 2002, 186, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Kiviat, N.B.; Wolner-Hanssen, P.; Eschenbach, D.A.; Wasserheit, J.N.; Paavonen, J.A.; Bell, T.A.; Critchlow, C.W.; Stamm, W.E.; Moore, D.E.; Holmes, K.K. Endometrial histopathology in patients with culture-proved upper genital tract infection and laparoscopically diagnosed acute salpingitis. Am. J. Surg. Pathol. 1990, 14, 167–175. [Google Scholar] [CrossRef]
- Haggerty, C.L.; Totten, P.A.; Astete, S.G.; Lee, S.; Hoferka, S.L.; Kelsey, S.F.; Ness, R.B. Failure of cefoxitin and doxycycline to eradicate endometrial Mycoplasma genitalium and the consequence for clinical cure of pelvic inflammatory disease. Sex. Transm. Infect. 2008, 84, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.R.; Manhart, L.E.; Bukusi, E.A.; Astete, S.; Brunham, R.C.; Holmes, K.K.; Sinei, S.K.; Bwayo, J.J.; Totten, P.A. Association between Mycoplasma genitalium and acute endometritis. Lancet 2002, 359, 765–766. [Google Scholar] [CrossRef]
- Soper, D.E.; Brockwell, N.J.; Dalton, H.P.; Johnson, D. Observations concerning the microbial etiology of acute salpingitis. Am. J. Obstet. Gynecol. 1994, 170, 1008–1014. [Google Scholar] [CrossRef]
- Jossens, M.O.; Schachter, J.; Sweet, R.L. Risk factors associated with pelvic inflammatory disease of differing microbial etiologies. Obstet. Gynecol. 1994, 83, 989–997. [Google Scholar] [CrossRef]
- Haggerty, C.L.; Hillier, S.L.; Bass, D.C.; Ness, R.B.; PID Evaluation and Clinical Health Study Investigators. Bacterial vaginosis and anaerobic bacteria are associated with endometritis. Clin. Infect. Dis. 2004, 39, 990–995. [Google Scholar] [CrossRef]
- Ness, R.B.; Kip, K.E.; Hillier, S.L.; Soper, D.E.; Stamm, C.A.; Sweet, R.L.; Rice, P.; Richter, H.E. A cluster analysis of bacterial vaginosis-associated microflora and pelvic inflammatory disease. Am. J. Epidemiol. 2005, 162, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Gundi, V.A.; Desbriere, R.; La Scola, B. Leptotrichia amnionii and the female reproductive tract. Emerg. Infect. Dis. 2004, 10, 2056–2057. [Google Scholar] [CrossRef] [PubMed]
- Gardella, C.; Riley, D.E.; Hitti, J.; Agnew, K.; Krieger, J.N.; Eschenbach, D. Identification and sequencing of bacterial rDNAs in culture-negative amniotic fluid from women in premature labor. Am. J. Perinatol. 2004, 21, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Hebb, J.K.; Cohen, C.R.; Astete, S.G.; Bukusi, E.A.; Totten, P.A. Detection of novel organisms associated with salpingitis, by use of 16S rDNA polymerase chain reaction. J. Infect. Dis. 2004, 190, 2109–2120. [Google Scholar] [CrossRef]
- Haggerty, C.L.; Totten, P.A.; Tang, G.; Astete, S.G.; Ferris, M.J.; Norori, J.; Bass, D.C.; Martin, D.H.; Taylor, B.D.; Ness, R.B. Identification of novel microbes associated with pelvic inflammatory disease and infertility. Sex. Transm. Infect. 2016, 92, 441–446. [Google Scholar] [CrossRef]
- Taylor, B.D.; Totten, P.A.; Astete, S.G.; Ferris, M.J.; Martin, D.H.; Ness, R.B.; Haggerty, C.L. Toll-like receptor variants and cervical Atopobium vaginae infection in women with pelvic inflammatory disease. Am. J. Reprod. Immunol. 2018, 79. [Google Scholar] [CrossRef]
- Behrman, R.E.; Butler, A.S. (Eds.) Preterm Birth: Causes, Consequences, and Prevention; National Academies Press: Washington, DC, USA, 2007. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Romero, R.; Mazor, M.; Munoz, H.; Gomez, R.; Galasso, M.; Sherer, D.M. The preterm labor syndrome. Ann. N. Y. Acad. Sci. 1994, 734, 414–429. [Google Scholar] [CrossRef]
- Goncalves, L.F.; Chaiworapongsa, T.; Romero, R. Intrauterine infection and prematurity. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 3–13. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F. Infection as a cause of preterm birth. Clin. Perinatol. 2003, 30, 677–700. [Google Scholar] [CrossRef]
- Wen, S.W.; Smith, G.; Yang, Q.; Walker, M. Epidemiology of preterm birth and neonatal outcome. Semin. Fetal Neonatal Med. 2004, 9, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Donati, L.; Di Vico, A.; Nucci, M.; Quagliozzi, L.; Spagnuolo, T.; Labianca, A.; Bracaglia, M.; Ianniello, F.; Caruso, A.; Paradisi, G. Vaginal microbial flora and outcome of pregnancy. Arch. Gynecol. Obstet. 2010, 281, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.B.; Hanlon, A.L.; Wu, G.; Liu, C.; Fredricks, D.N. First trimester levels of BV-associated bacteria and risk of miscarriage among women early in pregnancy. Matern. Child Health J. 2015, 19, 2682–2687. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.E.; Lamont, R.F.; Taylor-Robinson, D.; Morgan, D.J.; Ison, C.; Pearson, J. Abnormal bacterial colonisation of the genital tract and subsequent preterm delivery and late miscarriage. BMJ 1994, 308, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Kurki, T.; Sivonen, A.; Renkonen, O.V.; Savia, E.; Ylikorkala, O. Bacterial vaginosis in early pregnancy and pregnancy outcome. Obstet. Gynecol. 1992, 80, 173–177. [Google Scholar] [CrossRef]
- Lamont, R.F.; Nhan-Chang, C.L.; Sobel, J.D.; Workowski, K.; Conde-Agudelo, A.; Romero, R. Treatment of abnormal vaginal flora in early pregnancy with clindamycin for the prevention of spontaneous preterm birth: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2011, 205, 177–190. [Google Scholar] [CrossRef]
- Lamont, R.F. Advances in the prevention of infection-related preterm birth. Front. Immunol. 2015, 6, 566. [Google Scholar] [CrossRef]
- Lamont, R.F.; Sobel, J.D.; Akins, R.A.; Hassan, S.S.; Chaiworapongsa, T.; Kusanovic, J.P.; Romero, R. The vaginal microbiome: New information about genital tract flora using molecular based techniques. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 533–549. [Google Scholar] [CrossRef]
- Callahan, B.J.; DiGiulio, D.B.; Goltsman, D.S.A.; Sun, C.L.; Costello, E.K.; Jeganathan, P.; Biggio, J.R.; Wong, R.J.; Druzin, M.L.; Shaw, G.M.; et al. Replication and refinement of a vaginal microbial signature of preterm birth in two racially distinct cohorts of US women. Proc. Natl. Acad. Sci. USA 2017, 114, 9966–9971. [Google Scholar] [CrossRef]
- Hyman, R.W.; Fukushima, M.; Jiang, H.; Fung, E.; Rand, L.; Johnson, B.; Vo, K.C.; Caughey, A.B.; Hilton, J.F.; Davis, R.W.; et al. Diversity of the vaginal microbiome correlates with preterm birth. Reprod. Sci. 2014, 21, 32–40. [Google Scholar] [CrossRef]
- Nelson, D.B.; Shin, H.; Wu, J.; Dominguez-Bello, M.G. The gestational vaginal microbiome and spontaneous preterm birth among nulliparous African American women. Am. J. Perinatol. 2016, 33, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Stafford, G.P.; Parker, J.L.; Amabebe, E.; Kistler, J.; Reynolds, S.; Stern, V.; Paley, M.; Anumba, D.O.C. Spontaneous preterm birth is associated with differential expression of vaginal metabolites by lactobacilli-dominated microflora. Front. Physiol. 2017, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Stout, M.J.; Zhou, Y.; Wylie, K.M.; Tarr, P.I.; Macones, G.A.; Tuuli, M.G. Early pregnancy vaginal microbiome trends and preterm birth. Am. J. Obstet. Gynecol. 2017, 217, 356.e351–e355. [Google Scholar] [CrossRef] [PubMed]
- Farr, A.; Kiss, H.; Hagmann, M.; Machal, S.; Holzer, I.; Kueronya, V.; Husslein, P.W.; Petricevic, L. Role of lactobacillus species in the intermediate vaginal flora in early pregnancy: A retrospective cohort study. PLoS ONE 2015, 10, e0144181. [Google Scholar] [CrossRef] [PubMed]
- Kindinger, L.M.; Bennett, P.R.; Lee, Y.S.; Marchesi, J.R.; Smith, A.; Cacciatore, S.; Holmes, E.; Nicholson, J.K.; Teoh, T.G.; MacIntyre, D.A. The interaction between vaginal microbiota, cervical length, and vaginal progesterone treatment for preterm birth risk. Microbiome 2017, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef]
- Lamont, R.F.; Taylor-Robinson, D.; Wigglesworth, J.S.; Furr, P.M.; Evans, R.T.; Elder, M.G. The role of mycoplasmas, ureaplasmas and chlamydiae in the genital tract of women presenting in spontaneous early preterm labour. J. Med. Microbiol. 1987, 24, 253–257. [Google Scholar] [CrossRef]
- Taylor-Robinson, D.; Lamont, R.F. Mycoplasmas in pregnancy. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 164–174. [Google Scholar] [CrossRef]
- Marchesi, J.R.; Adams, D.H.; Fava, F.; Hermes, G.D.; Hirschfield, G.M.; Hold, G.; Quraishi, M.N.; Kinross, J.; Smidt, H.; Tuohy, K.M.; et al. The gut microbiota and host health: A new clinical frontier. Gut 2016, 65, 330–339. [Google Scholar] [CrossRef]
- Verstraelen, H.; Delanghe, J.; Roelens, K.; Blot, S.; Claeys, G.; Temmerman, M. Subclinical iron deficiency is a strong predictor of bacterial vaginosis in early pregnancy. BMC Infect. Dis. 2005, 5, 55. [Google Scholar] [CrossRef]
- Tohill, B.C.; Heilig, C.M.; Klein, R.S.; Rompalo, A.; Cu-Uvin, S.; Piwoz, E.G.; Jamieson, D.J.; Duerr, A. Nutritional biomarkers associated with gynecological conditions among US women with or at risk of HIV infection. Am. J. Clin. Nutr. 2007, 85, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Krohn, M.A.; Simhan, H.N. Maternal vitamin D deficiency is associated with bacterial vaginosis in the first trimester of pregnancy. J. Nutr. 2009, 139, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Klebanoff, M.A.; Turner, A.N. Bacterial vaginosis and season, a proxy for vitamin D status. Sex. Transm. Dis. 2014, 41, 295–299. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Akoh, C.C.; Pressman, E.K.; Cooper, E.; Queenan, R.A.; Pillittere, J.; O’Brien, K.O. Low vitamin D is associated with infections and proinflammatory cytokines during pregnancy. Reprod. Sci. 2018, 25, 414–423. [Google Scholar] [CrossRef]
- Thoma, M.E.; Klebanoff, M.A.; Rovner, A.J.; Nansel, T.R.; Neggers, Y.; Andrews, W.W.; Schwebke, J.R. Bacterial vaginosis is associated with variation in dietary indices. J. Nutr. 2011, 141, 1698–1704. [Google Scholar] [CrossRef]
- Reid, G. Probiotic lactobacilli for urogenital health in women. J. Clin. Gastroenterol. 2008, 42 (Suppl. 3), S234–S236. [Google Scholar] [CrossRef]
- Chenoll, E.; Moreno, I.; Sanchez, M.; Garcia-Grau, I.; Silva, A.; Gonzalez-Monfort, M.; Genoves, S.; Vilella, F.; Seco-Durban, C.; Simon, C.; et al. Selection of new probiotics for endometrial health. Front. Cell. Infect. Microbiol. 2019, 9, 114. [Google Scholar] [CrossRef]
- Machado, D.; Castro, J.; Palmeira-de-Oliveira, A.; Martinez-de-Oliveira, J.; Cerca, N. Bacterial vaginosis biofilms: Challenges to current therapies and emerging solutions. Front. Microbiol. 2015, 6, 1528. [Google Scholar] [CrossRef]
- Chetwin, E.; Manhanzva, M.T.; Abrahams, A.G.; Froissart, R.; Gamieldien, H.; Jaspan, H.; Jaumdally, S.Z.; Barnabas, S.L.; Dabee, S.; Happel, A.U.; et al. Antimicrobial and inflammatory properties of South African clinical Lactobacillus isolates and vaginal probiotics. Sci. Rep. 2019, 9, 1917. [Google Scholar] [CrossRef]
- Al-Ghazzewi, F.H.; Tester, R.F. Biotherapeutic agents and vaginal health. J. Appl. Microbiol. 2016, 121, 18–27. [Google Scholar] [CrossRef]
- Buggio, L.; Somigliana, E.; Borghi, A.; Vercellini, P. Probiotics and vaginal microecology: Fact or fancy? BMC Women’s Health 2019, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Fu, Y.; Yang, C.; Ma, J. Effects of metronidazole combined probiotics over metronidazole alone for the treatment of bacterial vaginosis: A meta-analysis of randomized clinical trials. Arch. Gynecol. Obstet. 2017, 295, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Oduyebo, O.O.; Anorlu, R.I.; Ogunsola, F.T. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Song, L.; Zhao, W. Effects of probiotics for the treatment of bacterial vaginosis in adult women: A meta-analysis of randomized clinical trials. Arch. Gynecol. Obstet. 2014, 289, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.Y.; Feng, D.; Wei, D.M.; Mei, L.; Chen, H.; Wang, X.; Fang, F. Probiotics for vulvovaginal candidiasis in non-pregnant women. Cochrane Database Syst. Rev. 2017, 11, CD010496. [Google Scholar] [CrossRef]
- Sobel, J.D. Vulvovaginal candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Sobel, J.D. Recurrent vulvovaginal candidiasis. Am. J. Obstet. Gynecol. 2016, 214, 15–21. [Google Scholar] [CrossRef]
- Blostein, F.; Levin-Sparenberg, E.; Wagner, J.; Foxman, B. Recurrent vulvovaginal candidiasis. Ann. Epidemiol. 2017, 27, 575–582. [Google Scholar] [CrossRef]
- De Seta, F.; Parazzini, F.; De Leo, R.; Banco, R.; Maso, G.P.; De Santo, D.; Sartore, A.; Stabile, G.; Inglese, S.; Tonon, M.; et al. Lactobacillus plantarum P17630 for preventing Candida vaginitis recurrence: A retrospective comparative study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 182, 136–139. [Google Scholar] [CrossRef]
- Jarde, A.; Lewis-Mikhael, A.M.; Moayyedi, P.; Stearns, J.C.; Collins, S.M.; Beyene, J.; McDonald, S.D. Pregnancy outcomes in women taking probiotics or prebiotics: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 14. [Google Scholar] [CrossRef]
- Reid, G.; Bocking, A. The potential for probiotics to prevent bacterial vaginosis and preterm labor. Am. J. Obstet. Gynecol. 2003, 189, 1202–1208. [Google Scholar] [CrossRef]
- Kirihara, N.; Kamitomo, M.; Tabira, T.; Hashimoto, T.; Taniguchi, H.; Maeda, T. Effect of probiotics on perinatal outcome in patients at high risk of preterm birth. J. Obstet. Gynaecol. Res. 2018, 44, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Younes, J.A.; Van der Mei, H.C.; Gloor, G.B.; Knight, R.; Busscher, H.J. Microbiota restoration: Natural and supplemented recovery of human microbial communities. Nat. Rev. Microbiol. 2011, 9, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Brennan, L.; Kennelly, M.A.; Maguire, O.C.; Smith, T.; Curran, S.; Coffey, M.; Foley, M.E.; Hatunic, M.; Shanahan, F.; et al. Impact of probiotics in women with gestational diabetes mellitus on metabolic health: A randomized controlled trial. Am. J. Obstet. Gynecol. 2015, 212, 496. [Google Scholar] [CrossRef] [PubMed]
- Gille, C.; Boer, B.; Marschal, M.; Urschitz, M.S.; Heinecke, V.; Hund, V.; Speidel, S.; Tarnow, I.; Mylonas, I.; Franz, A.; et al. Effect of probiotics on vaginal health in pregnancy. EFFPRO, a randomized controlled trial. Am. J. Obstet. Gynecol. 2016, 215, e601–e608. [Google Scholar] [CrossRef]
- Daskalakis, G.J.; Karambelas, A.K. Vaginal probiotic administration in the management of preterm premature rupture of membranes. Fetal Diagn. Ther. 2017, 42, 92–98. [Google Scholar] [CrossRef]
- Nordqvist, M.; Jacobsson, B.; Brantsaeter, A.L.; Myhre, R.; Nilsson, S.; Sengpiel, V. Timing of probiotic milk consumption during pregnancy and effects on the incidence of preeclampsia and preterm delivery: A prospective observational cohort study in Norway. BMJ Open 2018, 8, e018021. [Google Scholar] [CrossRef]
- Yeganegi, M.; Watson, C.S.; Martins, A.; Kim, S.O.; Reid, G.; Challis, J.R.; Bocking, A.D. Effect of Lactobacillus rhamnosus GR-1 supernatant and fetal sex on lipopolysaccharide-induced cytokine and prostaglandin-regulating enzymes in human placental trophoblast cells: Implications for treatment of bacterial vaginosis and prevention of preterm labor. Am. J. Obstet. Gynecol. 2009, 200, 532. [Google Scholar] [CrossRef]
- Bloise, E.; Torricelli, M.; Novembri, R.; Borges, L.E.; Carrarelli, P.; Reis, F.M.; Petraglia, F. Heat-killed lactobacillus rhamnosus GG modulates urocortin and cytokine release in primary trophoblast cells. Placenta 2010, 31, 867–872. [Google Scholar] [CrossRef]
- Haahr, T.; Ersboll, A.S.; Karlsen, M.A.; Svare, J.; Sneider, K.; Hee, L.; Weile, L.K.; Ziobrowska-Bech, A.; Ostergaard, C.; Jensen, J.S.; et al. Treatment of bacterial vaginosis in pregnancy in order to reduce the risk of spontaneous preterm delivery—A clinical recommendation. Acta Obstet. Gynecol. Scand. 2016, 95, 850–860. [Google Scholar] [CrossRef]
- Olsen, P.; Williamson, M.; Traynor, V.; Georgiou, C. The impact of oral probiotics on vaginal Group B streptococcal colonisation rates in pregnant women: A pilot randomised control study. Women Birth. J. Aust. Coll. Midwives 2018, 31, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Mirmonsef, P.; Hotton, A.L.; Gilbert, D.; Burgad, D.; Landay, A.; Weber, K.M.; Cohen, M.; Ravel, J.; Spear, G.T. Free glycogen in vaginal fluids is associated with Lactobacillus colonization and low vaginal pH. PLoS ONE 2014, 9, e102467. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Nikita, L.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Muhleisen, A.L.; Herbst-Kralovetz, M.M. Menopause and the vaginal microbiome. Maturitas 2016, 91, 42–50. [Google Scholar] [CrossRef]
- Nelson, H.D. Commonly used types of postmenopausal estrogen for treatment of hot flashes: Scientific review. JAMA 2004, 291, 1610–1620. [Google Scholar] [CrossRef]
- Devillard, E.; Burton, J.P.; Hammond, J.-A.; Lam, D.; Reid, G. Novel insight into the vaginal microflora in postmenopausal women under hormone replacement therapy as analyzed by PCR-denaturing gradient gel electrophoresis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 117, 76–81. [Google Scholar] [CrossRef]
- Ginkel, P.D.; Soper, D.E.; Bump, R.C.; Dalton, H.P. Vaginal flora in postmenopausal women: The effect of estrogen replacement. Infect. Dis. Obstet. Gynecol. 1993, 1, 94–97. [Google Scholar] [CrossRef]
- Heinemann, C.; Reid, G. Vaginal microbial diversity among postmenopausal women with and without hormone replacement therapy. Can. J. Microbiol. 2005, 51, 777–781. [Google Scholar] [CrossRef]
- Galhardo, C.; Soares, J.J.; Simões, R.; Haidar, M.; de Lima Rodrigues, G.; Baracat, E. Estrogen effects on the vaginal pH, flora and cytology in late postmenopause after a long period without hormone therapy. Clin. Exp. Obstet. Gynecol. 2006, 33, 85–89. [Google Scholar]
- Setty, P.; Redekal, L.; Warren, M.P. Vaginal estrogen use and effects on quality of life and urogenital morbidity in postmenopausal women after publication of the Women’s Health Initiative in New York City. Menopause 2016, 23, 7–10. [Google Scholar] [CrossRef]
- Achilles, S.L.; Hillier, S.L. The complexity of contraceptives: Understanding their impact on genital immune cells and vaginal microbiota. AIDS 2013, 27 (Suppl. 1), S5–S15. [Google Scholar] [CrossRef]
- Riggs, M.; Klebanoff, M.; Nansel, T.; Zhang, J.; Schwebke, J.; Andrews, W. Longitudinal association between hormonal contraceptives and bacterial vaginosis in women of reproductive age. Sex. Transm. Dis. 2007, 34, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Vodstrcil, L.A.; Hocking, J.S.; Law, M.; Walker, S.; Tabrizi, S.N.; Fairley, C.K.; Bradshaw, C.S. Hormonal contraception is associated with a reduced risk of bacterial vaginosis: A systematic review and meta-analysis. PLoS ONE 2013, 8, e73055. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.M.; McLemore, L.; Westerberg, K.; Astronomo, R.; Smythe, K.; Gardella, C.; Mack, M.; Magaret, A.; Patton, D.; Agnew, K.; et al. Long-term effect of depot medroxyprogesterone acetate on vaginal microbiota, epithelial thickness and HIV target cells. J. Infect. Dis. 2014, 210, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Fichorova, R.N.; Chen, P.L.; Morrison, C.S.; Doncel, G.F.; Mendonca, K.; Kwok, C.; Chipato, T.; Salata, R.; Mauck, C. The contribution of cervicovaginal infections to the immunomodulatory effects of hormonal contraception. mBio 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.P.; Edwards, D.J.; Blithe, D.L.; Fettweis, J.M.; Serrano, M.G.; Sheth, N.U.; Strauss, J.F., III; Buck, G.A.; Jefferson, K.K. Effects of combined oral contraceptives, depot medroxyprogesterone acetate and the levonorgestrel-releasing intrauterine system on the vaginal microbiome. Contraception 2017, 95, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Bassis, C.M.; Allsworth, J.E.; Wahl, H.N.; Sack, D.E.; Young, V.B.; Bell, J.D. Effects of intrauterine contraception on the vaginal microbiota. Contraception 2017, 96, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Achilles, S.L.; Austin, M.N.; Meyn, L.A.; Mhlanga, F.; Chirenje, Z.M.; Hillier, S.L. Impact of contraceptive initiation on vaginal microbiota. Am. J. Obstet. Gynecol. 2018, 218, e1–e10. [Google Scholar] [CrossRef]
- Srinivasan, S.; Morgan, M.T.; Fiedler, T.L.; Djukovic, D.; Hoffman, N.G.; Raftery, D.; Marrazzo, J.M.; Fredricks, D.N. Metabolic signatures of bacterial vaginosis. mBio 2015, 6. [Google Scholar] [CrossRef]
- Eschenbach, D.A. Bacterial vaginosis: Resistance, recurrence, and/or reinfection? Clin. Infect. Dis. 2007, 44, 220–221. [Google Scholar] [CrossRef][Green Version]
- Hardy, L.; Jespers, V.; Dahchour, N.; Mwambarangwe, L.; Musengamana, V.; Vaneechoutte, M.; Crucitti, T. Unravelling the bacterial vaginosis-associated biofilm: A multiplex gardnerella vaginalis and atopobium vaginae fluorescence in situ hybridization assay using peptide nucleic acid probes. PLoS ONE 2015, 10, e0136658. [Google Scholar] [CrossRef] [PubMed]
- Mastromarino, P.; Vitali, B.; Mosca, L. Bacterial vaginosis: A review on clinical trials with probiotics. New Microbiol. 2013, 36, 229–238. [Google Scholar] [PubMed]
- Workowski, K.A. Centers for disease control and prevention sexually transmitted diseases treatment guidelines. Clin. Infect. Dis. 2015, 61, S759–S762. [Google Scholar] [CrossRef] [PubMed]
- de Simone, C. The unregulated probiotic market. Clin. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef]
- Kolacek, S.; Hojsak, I.; Canani, R.B.; Guarino, A.; Indrio, F.; Pot, B.; Shamir, R.; Szajewska, H.; Vandenplas, Y.; Van Goudoever, J. Commercial probiotic products: A call for improved quality control. A Position Paper by the ESPGHAN Working Group for Probiotics and Prebiotics. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 117–124. [Google Scholar] [CrossRef]
- Hamilton, D.T.; Morris, M. The racial disparities in STI in the U.S.: Concurrency, STI prevalence, and heterogeneity in partner selection. Epidemics 2015, 11, 56–61. [Google Scholar] [CrossRef]
- Dominguez-Bello, M.G.; De Jesus-Laboy, K.M.; Shen, N.; Cox, L.M.; Amir, A.; Gonzalez, A.; Bokulich, N.A.; Song, S.J.; Hoashi, M.; Rivera-Vinas, J.I.; et al. Partial restoration of the microbiota of cesarean-born infants via vaginal microbial transfer. Nat. Med. 2016, 22, 250–253. [Google Scholar] [CrossRef]
- Onderdonk, A.B.; Delaney, M.L.; Fichorova, R.N. The human microbiome during bacterial vaginosis. Am. Soc. Microbiol. 2016, 29, 2. [Google Scholar] [CrossRef]
- Goldstein, I.; Alexander, J.L. Practical aspects in the management of vaginal atrophy and sexual dysfunction in perimenopausal and postmenopausal women. J. Sex. Med. 2005, 2, 154–165. [Google Scholar] [CrossRef]


{kind=link}
| CST | Vaginal pH | Ethnic Group | Type of Bacteria | Microorganism’s Contribution to Homeostasis or Dysbiosis | References |
|---|---|---|---|---|---|
| I | 4.0 ± 0.3 | White | L. crispatus | 1Lactobacillus spp. beneficial impact reside on: Preventing urogenital diseases. Adhesion to epithelial cells. Production compounds with antimicrobial properties (i.e., H2O2) Stimulated Lactic Dehydrogenase→Decrease pH→Protective Environment. Production of Bacteriocins. 2Common properties linked to dysbiotic statement: | [8,9,10,11,12,13,14,15,16,17,18,19,20,22,25,35,36,37,38,39,40,41] |
| II | 5.0 | L. gasseri | |||
| III | 4.4 | Asian | L. iners | ||
| IV A | G. vaginalis A. vaginae Prevotella spp. | Production of Biofilms → Adhesion to Epithelial Cells→ Antibiotic Tolerance, Resistance to Host Immune Defence. Production of Cytolysins. Production of Amines → pH Alkalinisation. Activates NF-κB cascade. Secretion of Collagenase and Fibrinolysins→Enhance Mucosal Surface Degradation →Detachment of Epithelial Cells. | [42,43,44,45,46] | ||
| 5.3 ± 0.6 | Black Hispanic | 3 Common properties linked to dysbiotic statement: | |||
| IV B | A. vaginae Leptotrichia spp. Mobiluncus spp. | Secretion of Collagenase and Fibrinolysins→Enhance Mucosal Surface Degradation →Detachment of Epithelial Cells. Adhesins that contribute to Epithelial Colonization. Hemolysin→Cytotoxic Activity. 3 plus: Malic Acid and Trimethylamine Production→vaginal irritation. | [42,43,44,45,46] [46] | ||
| V | 4.4 | L. jensenii | 1 | [8,9,10,11,12,13,14,15,16,17,18,19,20,22,25,35,36,37,38,39,40,41] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrientos-Durán, A.; Fuentes-López, A.; de Salazar, A.; Plaza-Díaz, J.; García, F. Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis. Nutrients 2020, 12, 419. https://doi.org/10.3390/nu12020419
Barrientos-Durán A, Fuentes-López A, de Salazar A, Plaza-Díaz J, García F. Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis. Nutrients. 2020; 12(2):419. https://doi.org/10.3390/nu12020419
Chicago/Turabian StyleBarrientos-Durán, Antonio, Ana Fuentes-López, Adolfo de Salazar, Julio Plaza-Díaz, and Federico García. 2020. "Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis" Nutrients 12, no. 2: 419. https://doi.org/10.3390/nu12020419
APA StyleBarrientos-Durán, A., Fuentes-López, A., de Salazar, A., Plaza-Díaz, J., & García, F. (2020). Reviewing the Composition of Vaginal Microbiota: Inclusion of Nutrition and Probiotic Factors in the Maintenance of Eubiosis. Nutrients, 12(2), 419. https://doi.org/10.3390/nu12020419