Serum Vitamin D Concentration ≥75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults



Abstract
:1. Introduction
2. Subjects and Methods
2.1. Brief Survey Description and Setting
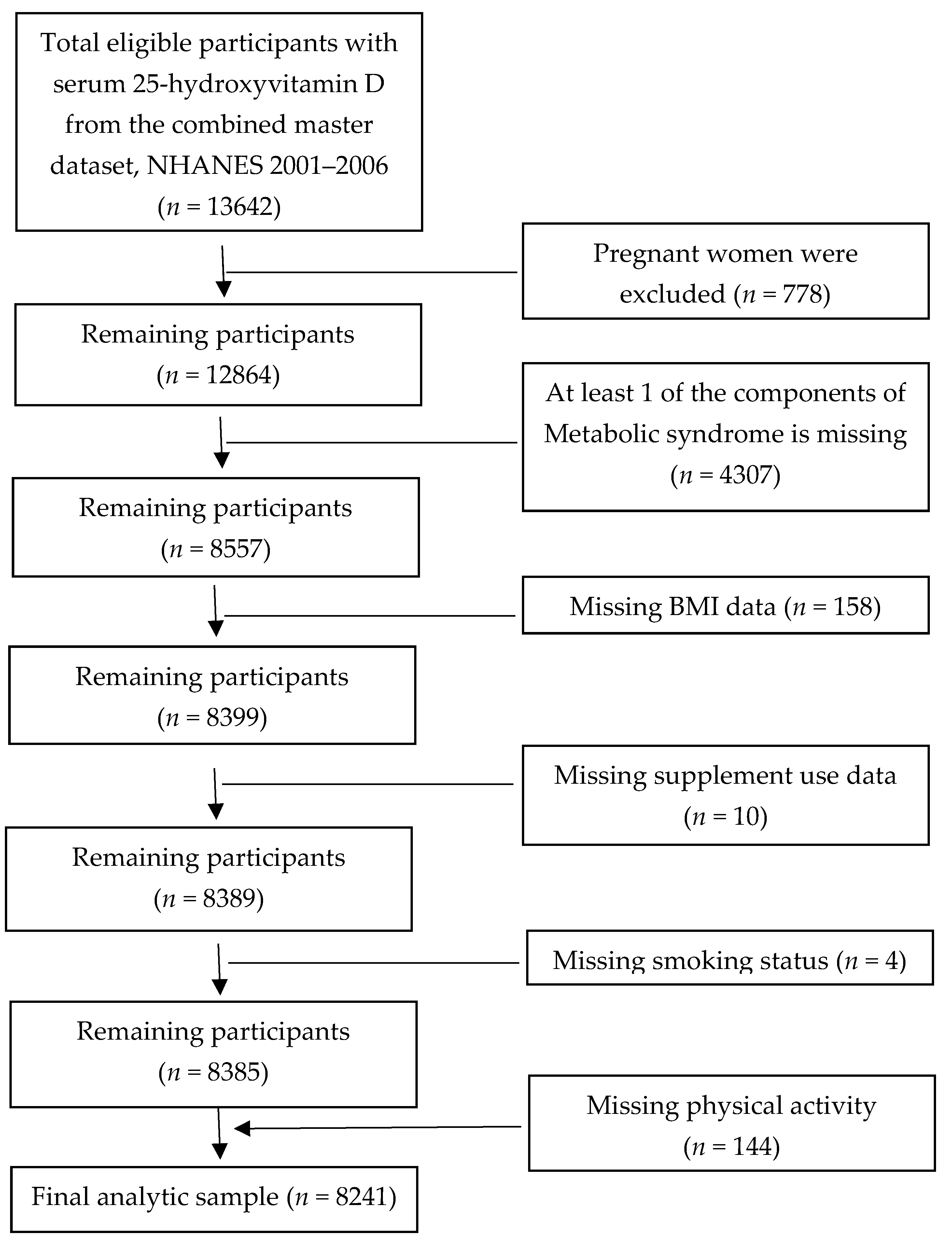
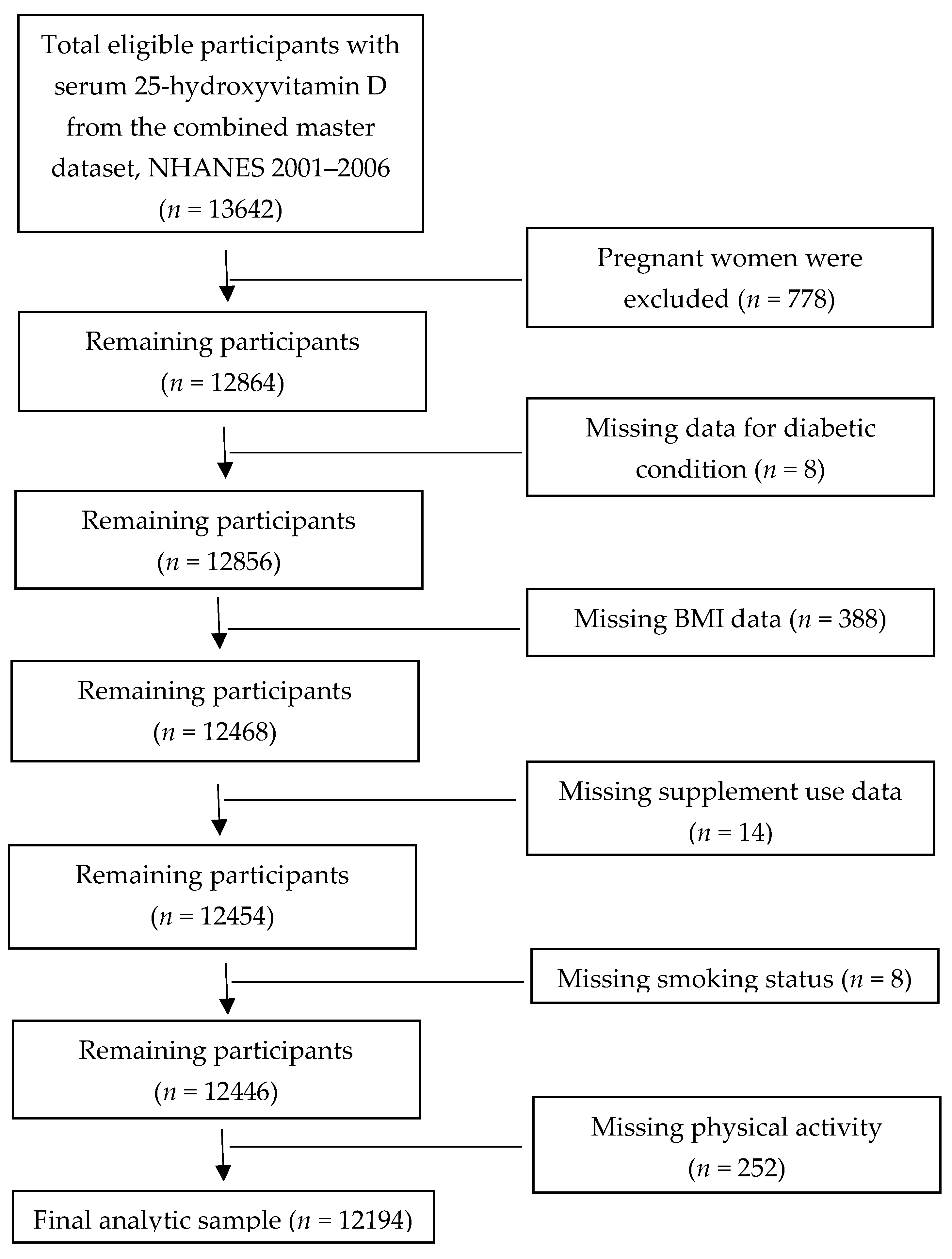
2.2. Sample Derivation and Eligibility Criteria
2.3. Criteria for MetS Diagnosis
2.4. Description of Study Variables
2.5. Description of Biochemical Assessments
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Serum 25(OH)D Concentrations, MetS and Diabetes
3.3. Serum 25(OH)D Concentrations, Cardiometabolic Markers, and CRF
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ganji, V.; Zhang, X.; Tangpricah, V. Serum 25-hydroxyvitamin D concentrations and prevalence estimates of hypovitaminosis D in the US population based on assay-adjusted data. J. Nutr. 2012, 142, 498–507. [Google Scholar] [CrossRef] [Green Version]
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Cabral, M.; Bos, A.; Amano, H.; Seino, S.; Shinkai, S. Relationship between skin color, sun exposure, UV protection, fish intake and serum levels of vitamin D in Japanese older adults. Nutr. Food Sci. 2017, 47, 409–422. [Google Scholar] [CrossRef]
- Yang, L.; Toriola, A.T. Leisure-time physical activity and circulating 25-hydroxyvitamin D levels in cancer survivors: A cross-sectional analysis using data from the US National Health and Nutrition Examination Survey. BMJ Open 2017, 7, e016064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranasinghe, S.; Jayalath, T.; Thennakoon, S.; Jayasekara, R.; Shiva, R.; Bandara, T. Variation of circulating 25-Hydroxyvitamin D levels with life style in a cohort group in Sri Lanka. Nutr. Food Sci. 2019, 49, 506–516. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: The underappreciated D-lightful hormone that is important for skeletal and cellular health. Curr. Opin. Endocrinol. Diabetes 2002, 9, 87–98. [Google Scholar] [CrossRef]
- Maki, K.C.; Rubin, M.R. Serum 23-hydroxyvitamin D is independently associated with high-density lipoprotein cholesterol and the metabolic syndrome in men and women. J. Clin. Lipidol. 2009, 3, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Baz-Hecht, M.; Goldfine, A.B. The impact of vitamin D deficiency on diabetes and cardiovascular risk. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Judd, S.E.; Nanes, M.S. Optimal vitamin D status attenuates the age-associated increase in systolic blood pressure in white Americans: Results from the third National Health and Nutrition Examination Survey. Am. J. Clin. Nutr. 2008, 87, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Ganji, V.; Milone, C.; Cody, M.M.; McCarty, F.; Wang, Y.T. Serum vitamin D concentrations are related to depression in young adult US population: The Third National Health and Nutrition Examination Survey. Int. Arch. Med. 2010, 3, 29–30. [Google Scholar] [CrossRef] [Green Version]
- Spina, C.S.; Tangpricha, V.; Uskokovic Adorinic, L.; Maehr, H.; Holick, M.F. Vitamin D and cancer. Anticancer Res. 2006, 26, 2515–2524. [Google Scholar] [PubMed]
- Potenza, M.V.; Mechanick, J.I. The metabolic syndrome: Definition, global impact, and pathophysiology. Nutr. Clin. Pr. 2009, 24, 560–577. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.D.; Kroon, J.J.; Greenway, F.L.; Bouchard, C.; Ryan, D.; Katzmarzyk, P.T. Prevalence of risk factors for metabolic syndrome in adolescents: National Health and Nutrition Examination Survey (NHANES), 2001–2006. Arch. Pediatr. Adolesc. Med. 2009, 163, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsiki, N.; Anagnostis, P.; Kotsa, K.; Goulis, D.G.; Mikhailidis, D.P. Obesity, Metabolic Syndrome and the Risk of Microvascular Complications in Patients with Diabetes mellitus. Curr. Pharm. Des. 2019, 25, 2051–2059. [Google Scholar] [CrossRef]
- Polly, P.; Tan, T.C. The role of vitamin D in skeletal and cardiac muscle function. Front. Physiol. 2014, 5, 145. [Google Scholar] [CrossRef] [Green Version]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef]
- Ardestani, A.; Parker, B.; Mathur, S.; Clarkson, P.; Pescatello, L.S.; Hoffman, H.J.; Polk, D.M.; Thompson, P.D. Relation of vitmain D level to maximal oxygen uptake in adults. Am. J. Cardiol. 2011, 107, 1246–1249. [Google Scholar] [CrossRef] [Green Version]
- Mowry, D.A.; Costello, M.M.; Heelan, K.A. Association among cardiorespiratory fitness, body fat, and bone marker measurements in healthy young females. J. Am. Osteopat. Assoc. 2009, 10, 534–539. [Google Scholar]
- Carson, E.L.; Pourshahidi, L.K.; Hill, T.R.; Cashman, K.D.; Strain, J.J.; Boreham, C.A.; Mulhern, M.S. Vitamin D, Muscle Function, and Cardiorespiratory Fitness in Adolescents From the Young Hearts Study. J. Clin. Endocrinol. Metab. 2015, 100, 4621–4628. [Google Scholar] [CrossRef] [Green Version]
- Chai, W.; Fan, J.X.; Wen, M. Association of individual and community factors with C-reactive protein and 25-hydroxyvitamin D: Evidence from the National Health and Nutrition Examination Survey (NHANES). SSM-Popul. Health 2016, 2, 889–896. [Google Scholar] [CrossRef] [Green Version]
- de Souza, W.N.; Norde, M.M.; Oki, É.; Rogero, M.M.; Marchioni, D.M.; Fisberg, R.M.; Martini, L.A. Association between 25-hydroxyvitamin D and inflammatory biomarker levels in a cross-sectional population-based study, São Paulo, Brazil. Nutr. Res. 2016, 36, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al-Khalidi, B.; Kimball, S.M.; Rotondi, M.A.; Ardern, C.I. Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: A cross-sectional analysis of NHANES, 2001–2010. Nutr. J. 2017, 16, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parva, N.R.; Tadepalli, S.; Singh, P.; Qian, A.; Joshi, R.; Kandala, H.; Nookala, V.K.; Cheriyath, P. Prevalence of Vitamin D Deficiency and Associated Risk Factors in the US Population (2011–2012). Cureus 2018, 10, e2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L.; Carroll, M.D.; Kruszon-Moran, D.; Dohrmann, S.M.; Curtin, L.R. National health and nutrition examination survey: Analytic guidelines, 1999–2010. Vital Health Stat. 2 2013, 161, 1–24. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497.
- Ostchega, Y.; Seu, R.; Sarafrazi Isfahani, N.; Zhang, G.; Hughes, J.P.; Miller, I. Waist Circumference Measurement Methodology Study: National Health and Nutrition Examination Survey, 2016. Vital Health Stat. 2 2019, 182, 1–20. [Google Scholar]
- National Health and Nutrition Examination Survey 2015–2016 Data Documentation, Codebook, and Frequencies. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2015–2016/BPX_I.htm (accessed on 3 July 2019).
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Mutt, S.J.; Jokelainen, J.; Sebert, S.; Auvinen, J.; Järvelin, M.R.; Keinänen-Kiukaanniemi, S.; Herzig, K.H. Vitamin D Status and Components of Metabolic Syndrome in Older Subjects from Northern Finland (Latitude 65° North). Nutrients 2019, 11, 1229. [Google Scholar] [CrossRef] [Green Version]
- Yin, X.; Sun, Q.; Zhang, X.; Lu, Y.; Sun, C.; Cui, Y.; Wang, S. Serum 25(OH)D is inversely associated with metabolic syndrome risk profile among urban middle-aged Chinese population. Nutr. J. 2012, 11, 68. [Google Scholar] [CrossRef] [Green Version]
- Lu, L.; Yu, Z.; Pan, A.; Hu, F.B.; Franco, O.H.; Li, H.; Li, X.; Yang, X.; Chen, Y.; Lin, X. Plasma 25-hydroxyvitamin D concentration and metabolic syndrome among middle-aged and elderly Chinese individuals. Diabetes Care 2009, 32, 1278–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chon, S.J.; Yun, B.H.; Jung, Y.S.; Cho, S.H.; Choi, Y.S.; Kim, S.Y.; Lee, B.S.; Seo, S.K. Association between vitamin D status and risk of metabolic syndrome among Korean postmenopausal women. PLoS ONE 2014, 9, e89721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupton, J.R.; Faridi, K.F.; Martin, S.S.; Sharma, S.; Kulkarni, K.; Jones, S.R.; Michos, E.D. Deficient serum 25-hydroxyvitamin D is associated with an atherogenic lipid profile: The Very Large Database of Lipids (VLDL-3) study. J. Clin. Lipidol. 2016, 10, 72–81.e1. [Google Scholar] [CrossRef]
- Huang, C.Y.; Chang, H.H.; Lu, C.W.; Tseng, F.Y.; Lee, L.T.; Huang, K.C. Vitamin D status and risk of metabolic syndrome among non-diabetic young adults. Clin. Nutr. 2015, 34, 484–489. [Google Scholar] [CrossRef]
- Lucato, P.; Solmi, M.; Maggi, S.; Bertocco, A.; Bano, G.; Trevisian, C.; Manzato, E.; Sergi, G.; Schofield, P.; Kouidrat, Y.; et al. Low vitamin D levels increase the risk of type-2 diabetes in older adultsA a systematic review and meta analysis. Maturitas 2017, 100, 8–15. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, J.; DeLuca, H.F. Where is the vitamin D receptor? Arch. Biochem. Biophys. 2012, 523, 123–133. [Google Scholar] [CrossRef]
- Zeitz, U.; Weber, K.; Soegiarto, D.W.; Wolf, E.; Balling, R.; Erben, R.G. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB J. 2003, 17, 509–511. [Google Scholar] [CrossRef]
- Sisley, S.R.; Arble, D.M.; Chambers, A.P.; Gutierrez-Aguilar, R.; He, Y.; Xu, Y.; Gardner, D.; Moore, D.D.; Seeley, R.J.; Sandoval, D.A. Hypothalamic Vitamin D Improves Glucose Homeostasis and Reduces Weight. Diabetes 2016, 65, 2732–2741. [Google Scholar] [CrossRef] [Green Version]
- Jamka, M.; Woźniewicz, M.; Jeszka, J.; Mardas, M.; Bogdański, P.; Stelmach-Mardas, M. The effect of vitamin D supplementation on insulin and glucose metabolism in overweight and obese individuals: Systematic review with meta-analysis. Sci. Rep. 2015, 5, 16142. [Google Scholar] [CrossRef] [Green Version]
- Poolsup, N.; Suksomboon, N.; Plordplong, N. Effect of vitamin D supplementation on insulin resistance and glycaemic control in prediabetes: A systematic review and meta-analysis. Diabet. Med. 2016, 33, 290–299. [Google Scholar] [CrossRef]
- Chandler, P.D.; Wang, L.; Zhang, X.; Sesso, H.D.; Moorthy, M.V.; Obi, O.; Lewis, J.; Prince, R.L.; Danik, J.S.; Manson, J.E.; et al. Effect of vitamin D supplementation alone or with calcium on adiposity measures: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2015, 73, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Sollid, S.T.; Svartberg, J.; Schirmer, H.; Joakimsen, R.M.; Njølstad, I.; Fuskevåg, O.M.; Figenschau, Y.; Hutchinson, M.Y. Vitamin D 20 000 IU per week for five years does not prevent progression from prediabetes to diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 1647–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulseth, H.L.; Wium, C.; Angel, K.; Eriksen, E.F.; Birkeland, K.I. Effects of Vitamin D Supplementation on Insulin Sensitivity and Insulin Secretion in Subjects with Type 2 Diabetes and Vitamin D Deficiency: A Randomized Controlled Trial. Diabetes Care 2017, 40, 872–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemieux, P.; Weisnagel, J.S.; Caron, A.Z.; Julien, A.S.; Morisset, A.S.; Carreau, A.M.; Poirier, J.; Tchernof, A.; Robitaille, J.; Bergeron, J.; et al. Effects of 6-month vitamin D supplementation on insulin sensitivity and secretion: A randomized, placebo-controlled trial. Eur. J. Endocrinol. 2019, 181, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Lucas, T.S.; Duncan, A.M.; Rabasa-Lhoret, R.; Vieth, R.; Gibbs, A.L.; Badawi, A.; Wolever, T.M. Effect of vitamin D supplementation on oral glucose tolerance in individuals with low vitamin D status and increased risk for developing type 2 diabetes (EVIDENCE): A double-blind, randomized, placebo-controlled clinical trial. Diabetes Diabetes Obes. Metab. 2016, 19, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Koundourakis, N.E.; Androulakis, N.E.; Malliaraki, N.; Margioris, A.N. Vitamin D and exercise performance in professional soccer players. PLoS ONE 2014, 9, e101659. [Google Scholar] [CrossRef]
- Lämmle, L.; Bergmann, K.; Bös, K.; Koletzko, B. Predictors of differences in vitamin D levels in children and adolescents and their relation to endurance performance. Ann. Nutr. Metab. 2013, 62, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Varkaneh, K.H.; Fatahi, S.; Tajik, S.; Rahmani, J.; Zarezadeh, M.; Shab-Bidar, S. Dietary inflammatory index in relation to obesity and body mass index: A meta-analysis. Nutr. Food Sci. 2018, 48, 702–721. [Google Scholar] [CrossRef]
- Avan, A.; Tavakoly Sany, S.B.; Ghayour-Mobarhan, M.; Rahimi, H.R.; Tajfard, M.; Ferns, G. Serum C-reactive protein in the prediction of cardiovascular diseases: Overview of the latest clinical studies and public health practice. J. Cell. Physiol. 2018, 233, 8508–8525. [Google Scholar] [CrossRef]
- Reddy, P.; Lent-Schochet, D.; Ramakrishnan, N.; McLaughlin, M.; Jialal, I. Metabolic syndrome is an inflammatory disorder: A conspiracy between adipose tissue and phagocytes. Clin. Chim. Acta 2019, 496, 35–44. [Google Scholar] [CrossRef]
- Ostadmohammadi, V.; Milajerdi, A.; Ghayour-Mobarhan, M.; Ferns, G.; Taghizadeh, M.; Badehnoosh, B.; Mirzaei, H.; Asemi, Z. The Effects of Vitamin D Supplementation on Glycemic Control, Lipid Profiles and C-Reactive Protein Among Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2019, 25, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yuan, W.; Sun, L.; Szeto, F.L.; Wong, K.E.; Li, X.; Kong, J.; Li, Y.C. 1,25-Dihydroxyvitamin D3 targeting of NF-kappaB suppresses high glucose-induced MCP-1 expression in mesangial cells. Kidney Int. 2007, 72, 193–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganji, V.; Zhang, X.; Shaikh, N.; Tangpricha, V. Serum 25-hydroxyvitamin D concentrations are associated with prevalence of metabolic syndrome and various cardiometabolic risk factors in US children and adolescents based on assay-adjusted serum 25-hydroxyvitamin D data from NHANES 2001–2006. Am. J. Clin. Nutr. 2011, 94, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Dan, Q.; Nie, X.-I.; Wu, S.; Cai, J. Vitamin D and hypertension: Prospective study and meta-analysis. PLoS ONE 2017, 12, e0174298. [Google Scholar]
- Sakamoto, R.; Jaceldo-Siegl, K.; Haddad, E.; Oda, K.; Fraser, G.E.; Tonstad, S. Relationship of vitamin D levels to blood pressure in a biethnic population. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 776–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forman, J.P.; Giovannucci, E.; Holmes, M.D.; Bischoff-Ferrari, H.A.; Tworoger, S.S.; Willett, W.C.; Curhan, G.C. Plasma 25-hydroxyvitamin d levels and risk of incident hypertension. Hypertension 2007, 49, 1063–1069. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Zhang, L.; Li, C.; Gai, Z.; Li, Y. Vitamin D and Vitamin D Receptor: New Insights in the Treatment of Hypertension. Curr. Protein Pept. Sci. 2019, 20, 984–995. [Google Scholar] [CrossRef]
- Ni, W.; Watts, S.W.; Ng, M.; Chen, S.; Glenn, D.J.; Gardner, D.G. Elimination of vitamin D receptor in vascular endothelial cells alters vascular function. Hypertension 2014, 64, 1290–1298. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.C.; Qiao, G.; Uskokovic, M.; Xiang, W.; Zheng, W.; Kong, J. Vitamin D: A negative endocrine regulator of the renin-angiotensin system and blood pressure. J. Steroid Biochem. Mol. Boil. 2004, 89, 387–392. [Google Scholar] [CrossRef]
- Kheiri, B.; Abdalla, A.; Osman, M.; Ahmed, S.; Hassan, M.; Bachuwa, M. Vitamin D deficiency and risk of cardiovascular diseases: A narrative review. Clin. Hypertens. 2018, 24, 9. [Google Scholar] [CrossRef]
- Goel, R.; Lal, H. Role of vitamin D supplementation in hypertension. Indian J. Clin. Biochem. 2011, 26, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Mirhosseini, N.; Rainsbury, J.; Kimball, S.M. Vitamin D Supplementation, Serum 25(OH)D Concentrations and Cardiovascular Disease Risk Factors: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2018, 5, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, S.; Hao, X. The effect of vitamin D3 on blood pressure in people with vitamin D deficiency. A system review and meta-analysis. Medicine 2019, 98, e15284. [Google Scholar] [CrossRef] [PubMed]
- Golzarand, M.; Shab-Bidar, S.; Koochakpoor, G.; Djafarian, K.; Speakman, J.R. Effect of vitamin D3 supplementation on blood pressure in adults: An updated meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 663–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corica, D.; Zusi, C.; Olivieri, F.; Marigliano, M.; Piona, C.; Fornari, E.; Morandi, A.; Corradi, M.; Del Giuduce, E.M.; Gatti, D.; et al. Vitamin D affects insulin sensitivity and β-cell function in obese non-diabetic youths. Eur. J. Endocrinol. 2019, 181, 439–450. [Google Scholar] [CrossRef]
- Trummer, C.; Theiler-Schwetz, V.; Kollmann, M.; Wölfler, M.; Münzker, J.; Pilz, S.; Pieber, T.R.; Heijboer, A.C.; Obermayer-Pietsch, B.; Lerchbaum, E. Effects of vitamin D supplementation on metabolic and endocrine parameters in healthy premenopausal women: A randomized controlled trial. Clin. Nutr. 2020, 39, 718–726. [Google Scholar] [CrossRef]
- Esteghamati, A.; Ashraf, H.; Khalilzadeh, O.; Zandieh, A.; Nakhjavani, M.; Rashidi, A.; Haghazali, M.; Asgari, F. Optimal cut-off of homeostasis model assessment of insulin resistance (HOMA-IR) for the diagnosis of metabolic syndrome: Third national surveillance of risk factors of non-communicable diseases in Iran (SuRFNCD-2007). Nutr. Metab. 2010, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Ziaee, A.; Esmailzadehha, N.; Oveisi, S.; Ghorbani, A.; Ghanei, L. The threshold value of homeostasis model assessment for insulin resistance in Qazvin Metabolic Diseases Study (QMDS): Assessment of metabolic syndrome. J. Res. Heal. Sci. 2015, 15, 94–100. [Google Scholar]
- Arellano-Ruiz, P.; García-Hermoso, A.; Cavero-Redondo, I.; Pozuelo-Carrascosa, D.; Martínez-Vizcaíno, V.; Solera-Martinez, M. Homeostasis Model Assessment cut-off points related to metabolic syndrome in children and adolescents: A systematic review and meta-analysis. Eur. J. Pediatr. 2019, 178, 1813–1822. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J. Steroid Biochem. Mol. Boil. 2018, 175, 177–189. [Google Scholar] [CrossRef]
- Khan, H.; Kunutsor, S.; Franco, O.H.; Chowdhury, R. Vitamin D, type 2 diabetes and other metabolic outcomes: A systematic review and meta-analysis of prospective studies. Proc. Nutr. Soc. 2013, 72, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Belenchia, A.M.; Tosh, A.K.; Hillman, L.S.; Peterson, C.A. Correcting vitamin D insufficiency improves insulin sensitivity in obese adolescents: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 774–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Men | Women | p-Value 2 |
|---|---|---|---|
| Serum 25(OH)D (nmol/L) (n = 8241) Body mass index (kg/m2) (n = 8241) Waist circumference (cm) (n = 8155) | 55.5 ± 0.8 27.9 ± 0.1 99.4 ± 0.3 | 53.5 ± 0.9 27.8 ± 0.2 92.5 ± 0.4 | 0.0003 0.43 <0.0001 |
| Systolic blood pressure (mm Hg) (n = 8020) Diastolic blood pressure (mm Hg) (n = 8020) | 122 ± 0.4 72 ± 0.3 | 120 ± 0.4 69 ± 0.3 | 0.0003 <0.0001 |
| Serum HDL-cholesterol (mg/dL) (n = 8231) Serum LDL-cholesterol (mg/dL) (n = 5243) | 48 ± 0.3 114 ± 1 | 59 ± 0.4 111 ± 1 | <0.0001 <0.02 |
| Serum triglycerides (mg/dL) (n = 5404) | 130 ± 2 | 110 ± 2 | <0.0001 |
| Plasma glucose (mg/dL) (n = 5415) Blood glycohemoglobin (%) (n = 8225) | 101 ± 0.4 5.5 ± 0.01 | 97 ± 0.5 5.5 ± 0.02 | <0.0001 0.33 |
| Serum insulin (µU/mL) (n = 5391) Serum C-peptide (nmol/L) (n = 3668) | 9.0 ± 0.2 0.75 ± 0.01 | 8.0 ± 0.2 0.70 ± 0.01 | <0.0001 0.0001 |
| HOMA-IR 3 (n = 5389) Serum C-reactive protein (µg/dL) (n = 8237) Serum total homocysteine (µmol/L) (n = 8227) Serum fibrinogen (mg/dL) (n = 1253) VO2 max (mL/kg/min) (n = 2625) | 2.3 ± 0.04 149 ± 4 8.8 ± 0.1 347 ± 7 40 ± 0.2 | 1.9 ± 0.05 204 ± 6 7.5 ± 0.1 375 ± 5 28 ± 0.3 | <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 |
| Variable | Serum 25(OH)D Concentration | p-Value | |||
|---|---|---|---|---|---|
| <30 nmol/L | 30-<50 nmol/L | 50-<75 nmol/L | ≥75 nmol/L | ||
| Sample size, n | 1311 | 2570 | 3068 | 1292 | |
| MetS Cases, n | 621 | 1138 | 1144 | 323 | |
| Prevalence of MetS (%) | 45.5 | 41.7 | 34.5 | 21.6 | <0.0001 2 |
| Unadjusted OR (95% CI) | 3.03 (2.39, 3.84) 3 | 2.59 (2.05, 3.27) 3 | 1.91 (1.51, 2.43) 3 | 1.0 4 | <0.0001 5 |
| Multivariable adjusted OR (95% CI) | 2.98 (2.14, 4.16) 3 | 2.84 (2.22, 3.64) 3 | 1.78 (1.38, 2.31) 3 | 1.0 4 | <0.0001 6 |
| Variable | Serum 25(OH)D Concentration | p-Value | |||
|---|---|---|---|---|---|
| <30 nmol/L | 30-<50 nmol/L | 50-<75 nmol/L | ≥75 nmol/L | ||
| Sample size, n | 1970 | 3816 | 4591 | 1817 | |
| Diabetes Cases, n 2 | 283 | 465 | 372 | 100 | |
| Prevalence, % | 11.6 | 9.3 | 5.9 | 4.1 | <0.0001 3 |
| Unadjusted OR (95% CI) | 2.88 (2.14, 3.86) 4 | 2.28 (1.75, 2.98) 4 | 1.47 (1.16, 1.87) 4 | 1.0 5 | <0.0001 6 |
| Multivariable adjusted OR (95% CI) | 1.70 (1.19, 2.43) 4 | 1.63 (1.20, 2.21) 4 | 1.33 (1.00, 1.78) 4 | 1.0 5 | 0.008 7 |
| Variable | Serum 25(OH)D Concentration 2 | p Value 3 | |||
|---|---|---|---|---|---|
| <30 nmol/L | 30-<50 nmol/L | 50->75 nmol/L | ≥75 nmol/L | ||
| Waist circumference, cm (n = 12047) 4 | 100 (98, 102) a | 100 (99, 101) a | 96 (95, 97) b | 93 (91, 94) c | <0.0001 |
| Systolic blood pressure, mm Hg (n = 11694) 5 Diastolic blood pressure, mm Hg (n = 11697) 6 | 124 (122, 125) 72.4 (71.1, 73.7) a | 123 (122, 123) 71.3 (70.6, 72.1) a | 122 (121, 123) 71.5 (70.8, 72.1) a | 121 (120, 122) 69.8 (68.9, 70.7) b | 0.12 <0.008 |
| Serum HDL-cholesterol, mg/dL (n = 12172) 7 Serum LDL cholesterol, mg/dL (n = 5292) 8 | 53.7 (52.3, 55.2) a, b 116 (113, 119) | 51.5 (50.7, 52.2) c 117 (114, 119) | 53.2 (52.6, 53.9) a 118 (116, 119) | 55.7 (54.8, 56.7) b 119 (116, 122) | <0.0001 0.45 |
| Serum fasting triglycerides, mg/dL (n = 5451) 9 | 134 (117, 153) a | 130 (120, 140) a | 115 (110, 120) a,b | 107 (101, 112) b | 0.0001 |
| Fasting plasma glucose, mg/dL (n = 5475) 10 Blood glycohemoglobin, % (n = 12179) 11 Serum insulin, µU/mL (n = 5434) 12 Serum C-peptide, nmol/L (n = 3707) 13 Serum total homocysteine, µmol/L (n = 12170)14 | 100 (98, 103) 5.49 (5.45, 5.54) a 11.4 (10.8, 12.1) a 0.78 (0.74, 0.82) a 8.78 (8.43, 9.15) a | 100 (99, 102) 5.48 (5.44, 5.51) a 10.9 (10.4, 11.5) a 0.76 (0.72, 0.80) a 8.22 (8.06, 8.38) b | 99 (98, 100) 5.44 (5.41, 5.47) a 9.5 (9.2, 9.9) b 0.71 (0.68, 0.74) b 7.87 (7.78, 7.96)c | 97 (96, 99) 5.35 (5.31, 5.39) b 8.9 (8.6, 9.2) b 0.67 (0.66, 0.69) b 7.89 (7.74, 8.04) c | <0.04 0.0002 <0.0001 <0.0001 <0.0001 |
| Serum C-reactive protein, µg/dL (n = 11924) 15 | 222 (205, 241) a | 207 (197, 218) a,b | 191 (184, 198) b | 190 (179, 201) b | <0.003 |
| HOMA-IR (n = 5445) 16 Serum fibrinogen (mg/dL) (n = 1265) 17 VO2 max (mL/kg/min) (n = 2625) 18 | 2.50 (2.25, 2.78) a 368 (348, 388) 33.9 (33.2, 34.7) a | 2.22 (2.05, 2.41) a 2 375 (362, 387) 33.6 (33.0, 34.2) a | 2.08 (1.98, 2.19) b 364 (355, 374) 34.4 (33.9, 34.9) a | 1.76 (1.67, 1.86) c 372 (358, 387) 35.8 (35.1, 36.6) b | <0.0001 0.06 0.0009 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganji, V.; Tangpricha, V.; Zhang, X. Serum Vitamin D Concentration ≥75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults. Nutrients 2020, 12, 730. https://doi.org/10.3390/nu12030730
Ganji V, Tangpricha V, Zhang X. Serum Vitamin D Concentration ≥75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults. Nutrients. 2020; 12(3):730. https://doi.org/10.3390/nu12030730
Chicago/Turabian StyleGanji, Vijay, Vin Tangpricha, and Xu Zhang. 2020. "Serum Vitamin D Concentration ≥75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults" Nutrients 12, no. 3: 730. https://doi.org/10.3390/nu12030730
APA StyleGanji, V., Tangpricha, V., & Zhang, X. (2020). Serum Vitamin D Concentration ≥75 nmol/L Is Related to Decreased Cardiometabolic and Inflammatory Biomarkers, Metabolic Syndrome, and Diabetes; and Increased Cardiorespiratory Fitness in US Adults. Nutrients, 12(3), 730. https://doi.org/10.3390/nu12030730