The Effects of a Supermarket-Based Intervention on the Nutritional Quality of Private-Label Foods: A Prospective Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Intervention
2.2. Data Source for the Intervention—The Product Category Reports
2.3. Comparators
2.4. Outcomes
2.5. Data Source—Intervention Outcomes
2.6. Statistical Analysis
3. Results
3.1. Mean Nutrient Content in 2015 between the Intervention Supermarket and Comparators
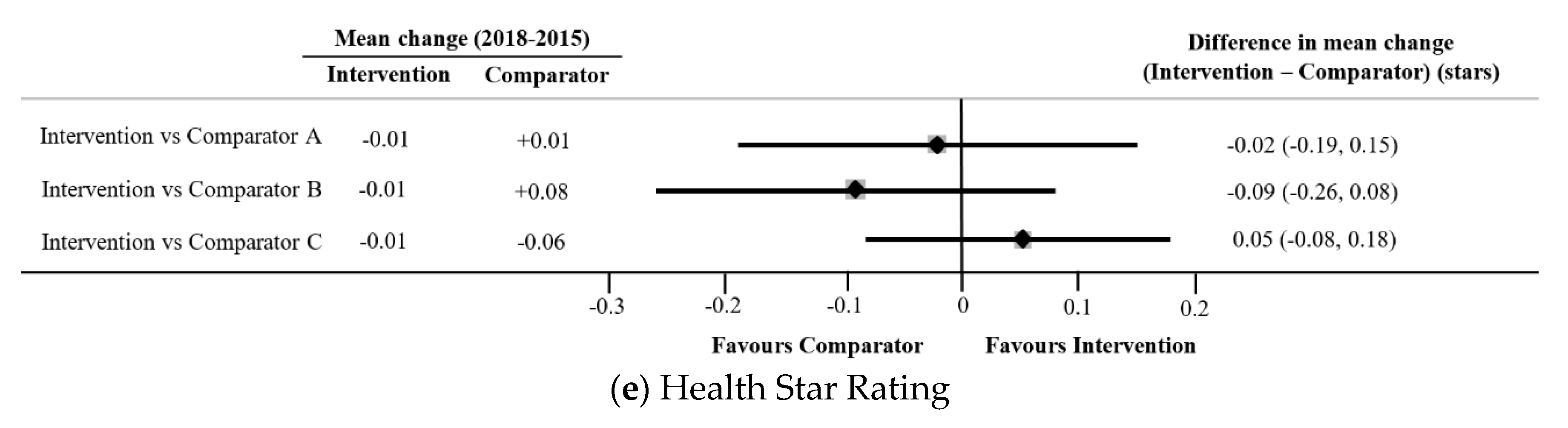
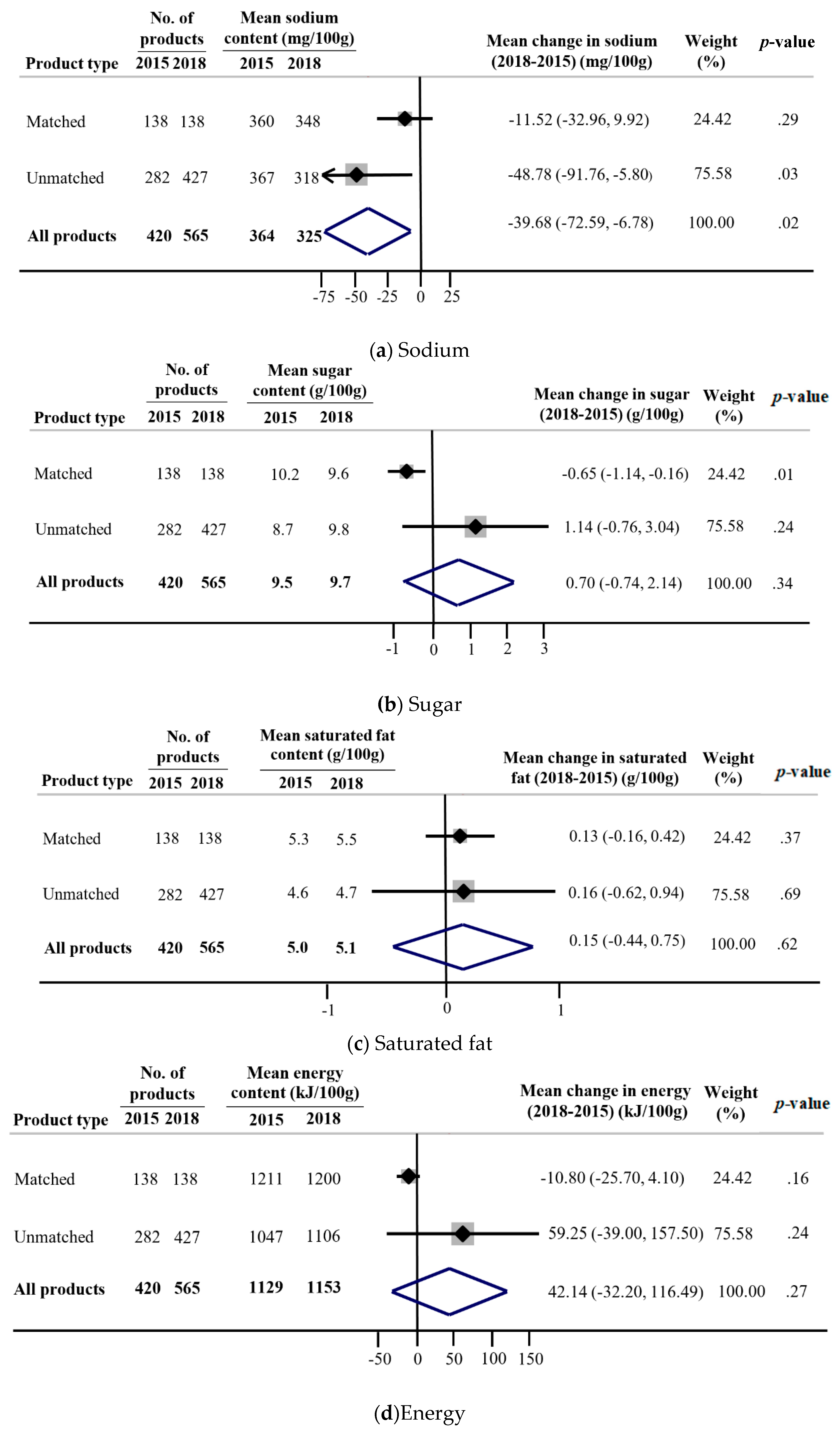
3.2. Differences in the Mean Change in Nutrient Content between 2015 and 2018 between the Intervention Supermarket and Comparators
3.3. Mean Change in Nutrient Content between 2015 and 2018 for Products in the Intervention Supermarket
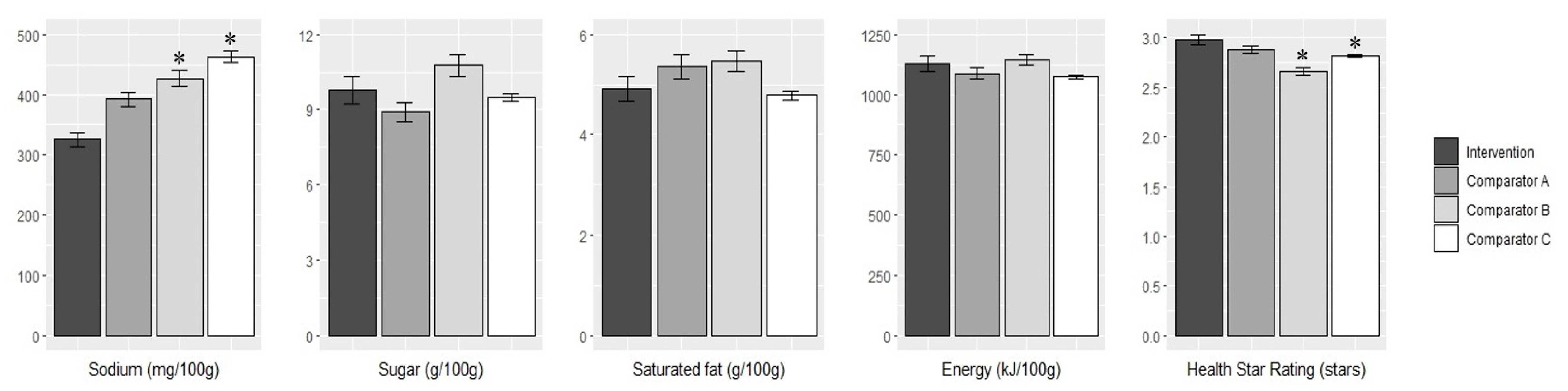
3.4. Comparison of the Mean Nutrient Content in 2018 between the Intervention Supermarket and Comparators
3.5. Adjustment for Multiple Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Noncommunicable Diseases (NCD) Country Profiles, Australia. Available online: https://www.who.int/nmh/countries/aus_en.pdf?ua=1 (accessed on 4 October 2019).
- Willcox, S. Chronic diseases in Australia: The case for changing course; Australian Health Policy Collaboration Issues paper No. 2014-02; Australian Health Policy Collaboration: Melbourne, Australia, 2014. [Google Scholar]
- Australian Institute of Health and Welfare. Australia’s Health 2016; Australia’s health series no. 15. Cat. no. AUS 199; Australian Institute of Health and Welfare: Canberra, ACT, Australia, 2016.
- World Health Organization. Noncommunicable Diseases Progress Monitor 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Hawkes, C. Dietary implications of supermarket development: A global perspective. Dev. Policy Rev. 2008, 26, 657–692. [Google Scholar] [CrossRef]
- Melaku, Y.; Renzaho, A.; Gill, T.; Taylor, A.; Dal Grande, E.; de Courten, B.; Baye, E.; Gonzalez-Chica, D.; Hyppönen, E.; Shi, Z.; et al. Burden and trend of diet-related non-communicable diseases in Australia and comparison with 34 OECD countries, 1990-2015: findings from the Global Burden of Disease Study 2015. Eur. J. Nutr. 2019, 58, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Euromonitor International. Packaged Food in Australia; Euromonitor International: London, UK, 2018. [Google Scholar]
- Rauber, F.; da Costa Louzada, M.; Steele, E.; Millett, C.; Monteiro, C.; Levy, R. Ultra-processed food consumption and chronic non-communicable diseases-related dietary nutrient profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [Green Version]
- Pulker, C.; Trapp, G.; Foulkes-Taylor, F.; Scott, J.; Pollard, C. The extent and nature of supermarket own brand foods in Australia: Study protocol for describing the contribution of selected products to the healthfulness of food environments. Nutr. J. 2018, 17, 95. [Google Scholar] [CrossRef] [Green Version]
- Pulker, C.; Trapp, G.; Scott, J.; Pollard, C. The nature and quality of Australian supermarkets’ policies that can impact public health nutrition, and evidence of their practical application: A cross-sectional study. Nutrients 2019, 11, 853. [Google Scholar] [CrossRef] [Green Version]
- Department of Agriculture. Australian Food Statistics 2012–13; Department of Agriculture, Ed.; Australian Government: Canberra, Australia, 2014.
- Cloutman, N. IBISWorld Industry Report G4111: Supermarkets and Grocery Stores in Australia; IBISWorld: Los Angeles, CA, USA, 2018. [Google Scholar]
- Nenycz-Thiel, M. Private labels in Australia: A case where retailer concentration does not predicate private labels share. J. Brand Manag. 2010, 18, 624–633. [Google Scholar] [CrossRef]
- The Nielsen Company. The State of Private Label Around The World. Available online: https://www.nielsen.com/wp-content/uploads/sites/3/2019/04/Nielsen20Global20Private20Label20Report20November202014.pdf (accessed on 1 September 2019).
- The Nielsen Company. Our Penchant For Private Label. Available online: https://www.nielsen.com/au/en/insights/article/2014/our-penchant-for-private-label/ (accessed on 1 September 2019).
- The Nielsen Company. Find Your Growth. Available online: http://www.nielsen.com/au/en/insights/reports/2016/find-your-growth.html (accessed on 4 October 2019).
- Euromonitor International. Company Shares. Available online: http://www.portal.euromonitor.com (accessed on 24 August 2019).
- Glanz, K.; Bader, M.; Iyer, S. Retail grocery store marketing strategies and obesity: An integrative review. Am. J. Prev. Med. 2012, 42, 503–512. [Google Scholar] [CrossRef]
- Pulker, C.; Trapp, G.; Scott, J.; Pollard, C. What are the position and power of supermarkets in the Australian food system, and the implications for public health? A systematic scoping review. Obes. Rev. 2018, 19, 198–218. [Google Scholar] [CrossRef]
- Trevena, H.; Reeve, B.; Bero, L.; Thow, A. Private food safety standards in the global food supply chain: A scoping review protocol. JBI Evid. Synth. 2020, 18, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Dunford, E.; Jones, A.; Mhurchu, C.N.; Crino, M.; Taylor, F.; Woodward, M.; Neal, B. Incorporating added sugar improves the performance of the health star rating front-of-pack labelling system in Australia. Nutrients 2017, 9, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, N.; Rowe, S.; Brackett, R.; Burton-Freeman, B.; Hentges, E.; Kretser, A.; Klurfeld, D.; Meyers, L.; Mukherjea, R.; Ohlhorst, S. Achieving a transparent, actionable framework for public-private partnerships for food and nutrition research. Am. J. Clin. Nutr. 2015, 101, 1359–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraak, V.; Harrigan, P.; Lawrence, M.; Harrison, P.; Jackson, M.; Swinburn, B. Balancing the benefits and risks of public-private partnerships to address the global double burden of malnutrition. Public Health Nutr. 2012, 15, 503–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, T.; Trevena, T.; Sacks, G.; Dunford, E.; Martin, J.; Webster, J.; Swinburn, B.; Moodie, A.; Neal, B. A systematic interim assessment of the Australian Government’s Food and Health Dialogue. Med. J. Aust. 2014, 200, 92–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunford, E.; Webster, J.; Metzler, A.; Czernichow, S.; Mhurchu, C.N.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef]
- Dunford, E.; Trevena, H.; Goodsell, C.; Ng, K.; Webster, J.; Millis, A.; Goldstein, S.; Hugueniot, O.; Neal, B. FoodSwitch: A mobile phone app to enable consumers to make healthier food choices and crowdsourcing of national food composition data. JMIR mHealth uHealth 2014, 2, e37. [Google Scholar] [CrossRef]
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. The importance of the normality assumption in large public health data sets. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Van Gunst, A.; Roodenburg, A.; Steenhuis, I. Reformulation as an integrated approach of four disciplines: A qualitative study with food companies. Foods 2018, 7, 64. [Google Scholar] [CrossRef] [Green Version]
- OECD. The Heavy Burden of Obesity: The Economics of Prevention; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Yeung, C.; Gohil, P.; Rangan, A.; Flood, V.; Arcot, J.; Gill, T.; Louie, J. Modelling of the impact of universal added sugar reduction through food reformulation. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.; Magnusson, R.; Swinburn, B.; Webster, J.; Wood, A.; Sacks, G.; Neal, B. Designing a healthy food partnership: Lessons from the Australian Food and Health Dialogue. BMC Public Health 2016, 16, 651. [Google Scholar] [CrossRef] [Green Version]
- Healthy Food Partnership. Healthy Food Partnership Reformulation Program: Evidence Informing the Approach, Draft Targets and Modelling Outcomes. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/reformulation (accessed on 18 September 2019).
- Healthy Food Partnership. Reformulation Working Group. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/reformulation (accessed on 30 September 2019).
- WHO. Shake The Salt Habit. Available online: https://apps.who.int/iris/bitstream/handle/10665/250134/WHO-NMH-PND-16.4-eng.pdf?sequence=1 (accessed on 3 June 2019).
- Trevena, H.; Neal, B.; Dunford, E.; Haskelberg, H.; Wu, J. A comparison of the sodium content of supermarket private-label and branded foods in Australia. Nutrients 2015, 7, 7027–7041. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, M.; Soler, L. Food reformulation and nutritional quality of food consumption: An analysis based on households panel data in France. Eur. J. Clin. Nutr. 2018, 72, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiteri, S.; Olstad, D.-L.; Woods, J. Nutritional quality of new food products released into the Australian retail food market in 2015—Is the food industry part of the solution? BMC Public Health 2018, 18, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, G.; Mialon, M.; Vandevijvere, S.; Trevena, H.; Snowdon, W.; Crino, M.; Swinburn, B. Comparison of food industry policies and commitments on marketing to children and product (re)formulation in Australia, New Zealand and Fiji. Crit. Public Health 2014, 25, 299–319. [Google Scholar] [CrossRef]
- Crino, M.; Sacks, G.; Dunford, E.; Trieu, K.; Webster, J.; Vandevijvere, S.; Swinburn, B.; Wu, J.; Neal, B. Measuring the healthiness of the packaged food supply in Australia. Nutrients 2018, 10, 702. [Google Scholar] [CrossRef] [Green Version]
- Sustainable Development Goals. Sustainable Development Goal 17. Available online: https://sustainabledevelopment.un.org/sdg17 (accessed on 1 October 2019).
- Buse, K.; Walt, G. Global public-private partnerships: Part I—A new development in health? Bull. World Health Organ. 2000, 78, 549–561. [Google Scholar]
- Deakin University. World-First Trial Puts Healthy Supermarkets to the Taste Test. Available online: https://www.deakin.edu.au/about-deakin/media-releases/articles/world-first-trial-puts-healthy-supermarkets-to-the-taste-test (accessed on 1 October 2019).
- Pulker, C.; Trapp, G.; Scott, J.; Pollard, C.M. Global supermarkets’ corporate social responsibility commitments to public health: A content analysis. Global Health 2018, 14, 121. [Google Scholar] [CrossRef] [Green Version]
- Sacks, G.; Robinson, E.; Cameron, A. Inside Our Supermarkets: Assessment of Company Policies and Commitments Related to Obesity Prevention and Nutrition, Australia 2018; Deakin University: Melbourne, Australia, 2018. [Google Scholar]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Brownell, K. Thinking forward: The quicksand of appeasing the food industry. PLoS Med. 2012, 9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Categories | All groups | ||
|---|---|---|---|
| n (%) | Change over Time (%) | ||
| 2015 | 2018 | ||
| All products | 6703 (100) | 8428 (100) | +25.7 |
| Bread and bakery products | 1344 (20.1) | 1663 (19.7) | +23.7 |
| Cereal and grain products | 699 (10.4) | 837 (9.9) | +19.7 |
| Convenience foods | 624 (9.3) | 1058 (12.6) | +69.6 |
| Dairy | 1069 (15.9) | 1383 (16.4) | +29.4 |
| Edible oils and oil emulsions | 79 (1.2) | 100 (1.2) | +26.6 |
| Fish and fish products | 289 (4.3) | 309 (3.7) | +6.9 |
| Fruit and vegetables | 521 (7.8) | 545 (6.5) | +4.6 |
| Meat and meat products | 577 (8.6) | 853 (10.1) | +47.8 |
| Non-alcoholic beverages | 256 (3.8) | 235 (2.8) | −8.2 |
| Sauces, dressings, spreads and dips | 944 (14.1) | 1111 (13.2) | +17.7 |
| Snack foods | 266 (4.0) | 298 (3.5) | +12.0 |
| Special foods | 35 (0.5) | 36 (0.4) | +2.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coyle, D.H.; Wu, J.H.; Di Tanna, G.L.; Shahid, M.; Taylor, F.; Neal, B.; Trevena, H. The Effects of a Supermarket-Based Intervention on the Nutritional Quality of Private-Label Foods: A Prospective Study. Nutrients 2020, 12, 1692. https://doi.org/10.3390/nu12061692
Coyle DH, Wu JH, Di Tanna GL, Shahid M, Taylor F, Neal B, Trevena H. The Effects of a Supermarket-Based Intervention on the Nutritional Quality of Private-Label Foods: A Prospective Study. Nutrients. 2020; 12(6):1692. https://doi.org/10.3390/nu12061692
Chicago/Turabian StyleCoyle, Daisy H., Jason HY Wu, Gian Luca Di Tanna, Maria Shahid, Fraser Taylor, Bruce Neal, and Helen Trevena. 2020. "The Effects of a Supermarket-Based Intervention on the Nutritional Quality of Private-Label Foods: A Prospective Study" Nutrients 12, no. 6: 1692. https://doi.org/10.3390/nu12061692