Adherence to Mediterranean Diet, Physical Activity and Survival after Prostate Cancer Diagnosis

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
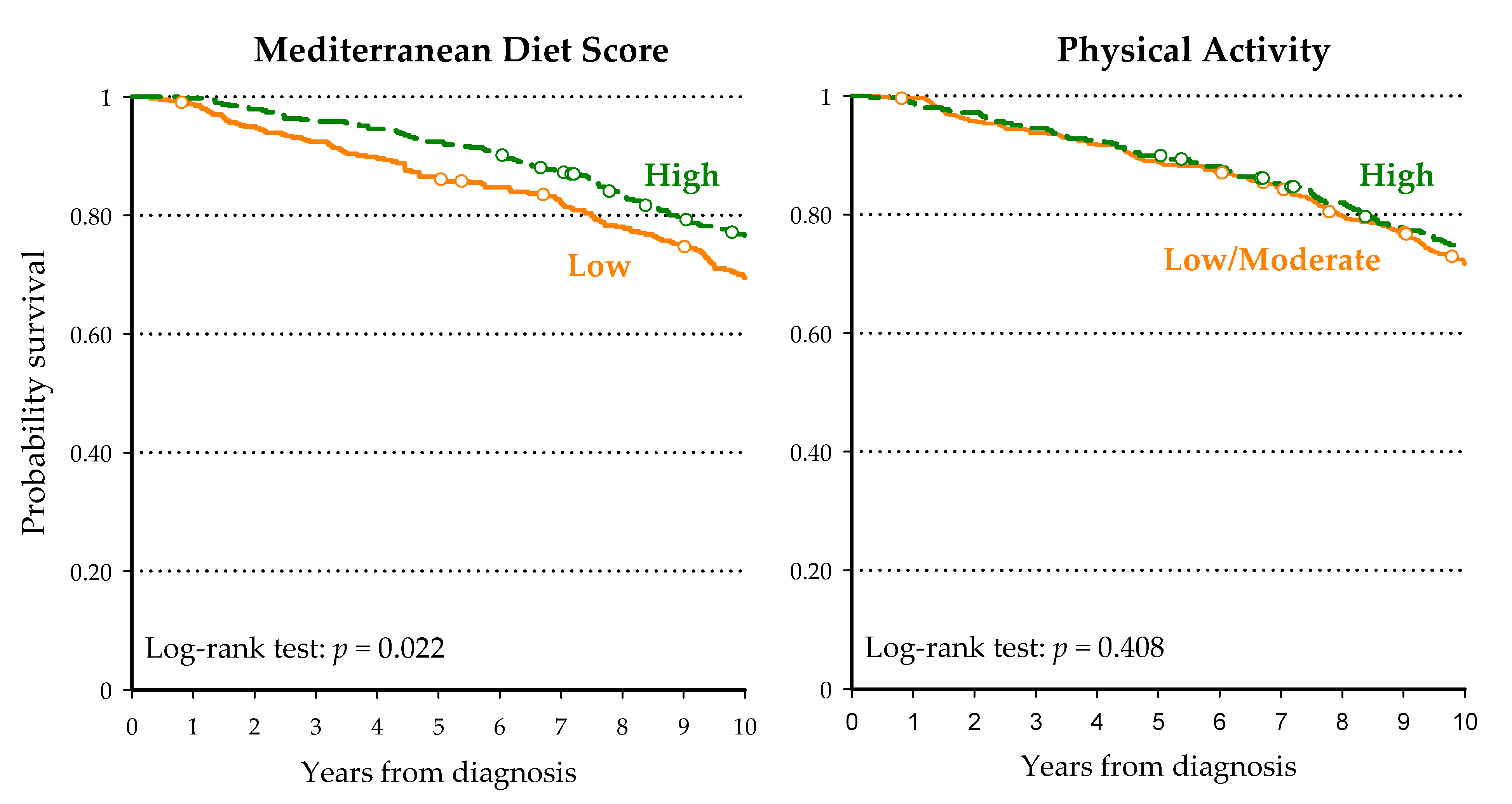
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2020. Available online: https://gco.iarc.fr/today (accessed on 11 January 2021).
- Quaglia, A.; Vercelli, M.; Puppo, A.; Casella, C.; Artioli, E.; Crocetti, E.; Falcini, F.; Ramazzotti, V.; Tagliabue, G.; Prostate Cancer Working Group. Prostate cancer in Italy before and during the ‘PSA era’: Serviva trend and prognostic determinants. Eur. J. Cancer Prev. 2003, 12, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Guzzinati, S.; Virdone, S.; De Angelis, R.; Panato, C.; Buzzoni, C.; Capocaccia, R.; Francisci, S.; Gigli, A.; Zorzi, M.; Tagliabue, G.; et al. Characteristics of people living in Italy after a cancer diagnosis in 2010 and projections to 2020. BMC Cancer 2018, 18, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hemelrijck, M.; Folkvaljon, Y.; Adolfsson, J.; Akre, O.; Holmberg, L.; Garmo, H.; Stattin, P. Causes of death in men with localized prostate cancer: A nationwide, population-based study. BJU Int. 2016, 117, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eleftheriou, D.; Benetou, V.; Trichopoulou, A.; La Vecchia, C.; Bamia, C. Mediterranean diet and its components in relation to all-cause mortality: Meta-analysis. Br. J. Nutr. 2018, 120, 1081–1097. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; DuPre, N.; Richman, E.L.; Stampfer, M.J.; Chan, J.M.; Giovannucci, E.L. Mediterranean diet and prostate cancer risk and mortality in the Health Professionals Follow-up Study. Eur. Urol. 2014, 65, 887–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.; Chan, J.M. Physical activity and survival after prostate cancer diagnosis in the Health Professionals Follow-Up Study. J. Clin. Oncol. 2011, 29, 726–732. [Google Scholar] [CrossRef]
- Bonn, S.E.; Sjölander, A.; Lagerros, Y.T.; Wiklund, F.; Stattin, P.; Holmberg, E.; Grönberg, H.; Bälter, K. Physical activity and survival among men diagnosed with prostate cancer. Cancer Epidemiol. Biomaker Prev. 2014, 24, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Friedenreich, C.M.; Wang, Q.; Neilson, H.K.; Kopciuk, K.A.; McGregor, S.E.; Courneya, K.S. Physical activity and survival after prostate cancer. Eur. Urol. 2016, 70, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Jacobs, E.J.; Gapstur, S.M.; Maliniak, M.L.; Gansler, T.; McCullough, M.L.; Stevens, V.L.; Patel, A.V. Recreational physical activity in relation to prostate cancer-specific mortality among men with nonmetastatic prostate cancer. Eur. Urol. 2017, 72, 931–939. [Google Scholar] [CrossRef]
- Karavasiloglou, N.; Pestoni, G.; Wanner, M.; Faeh, D.; Rohrmann, S. Healthy lifestyle is inversely associated with mortality in cancer survivors: Results from the Third National Health and Nutrition Examination Survey (NHANES III). PLoS ONE 2019, 14, e0218048. [Google Scholar] [CrossRef] [Green Version]
- Polesel, J.; Gini, A.; Dal Maso, L.; Stocco, C.; Birri, S.; Taborelli, M.; Serraino, D.; Zucchetto, A. The negative impact of tobacco smoking on survival after prostate cancer diagnosis. Cancer Causes Control. 2015, 26, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Taborelli, M.; Polesel, J.; Parpinel, M.; Stocco, C.; Birri, S.; Serraino, D.; Zucchetto, A. Fruit and vegetables consumption is directly associated to survival after prostate cancer. Mol. Nutr. Food Res. 2017, 61, 1600816. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report on a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Zucchetto, A.; Gini, A.; Shivappa, N.; Hébert, J.R.; Stocco, C.; Dal Maso, L.; Birri, S.; Serraino, D.; Polesel, J. Dietary inflammatory index and prostate cancer survival. Int. J. Cancer 2016, 139, 2398–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnagnarella, P.; Parpinel, M.; Salvini, S.; Franceschi, S.; Palli, D.; Boyle, P. The update of the Italian Food Composition Database. J. Food Comp. Anal. 2004, 17, 509–522. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalbfleisch, J.D.; Prentice, R.L. The Statistical Analysis of Failure Time Data; Wiley: New York, NY, USA, 2002. [Google Scholar]
- Fine, J.P.; Gray, R.J. A proportional hazard model for the subdistribution of a competing risk. J. Am. Stat. Ass. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Li, R.; Chambless, L. Test for additive interaction in proportional hazard models. Ann. Epidemiol. 2007, 17, 117–236. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomized trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Ratjen, I.; Schafmayer, C.; di Giuseppe, R.; Waniek, S.; Plachta-Danielzik, S.; Koch, M.; Nöthlings, U.; Hampe, J.; Schlesinger, S.; Lieb, W. Postdiagnostic Mediterranean and Healthy Nordic dietary pattern are inversely associated with all-cause mortality in long-term colorectal cancer survivors. J. Nutr. 2017, 147, 636–644. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.H.; Willett, W.C.; Fung, T.; Rosner, B.; Holmes, M.D. Diet quality indices and postmenopausal breast cancer survival. Nutr. Cancer 2011, 63, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Hackshaw-McGeagh, L.E.; Perry, R.E.; Leach, V.A.; Qandil, S.; Jeffreys, M.; Martin, R.M.; Lane, J.A. A systemic review of dietary, nutritional, and physical activity interventions for the prevention of prostate cancer progression and mortality. Cancer Cause Control. 2015, 26, 1521–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey Lopez, J.P.; Gebel, K.; Chia, D.; Stamatakis, E. Association of vigorous physical activity with all-cause, cardiovascular and cancer mortality among 64913 adults. BMJ Open Sport Exerc. Med. 2019, 5, e000596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibler, E.A.; Zhu, X.; Shrubsole, M.; Hou, L.; Dai, Q. Physical activity, dietary calcium to magnesium intake and mortality in the National Health and Examination Survey 1999-2006 cohort. Int. J. Cancer 2020, 146, 2979–2986. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Neilson, H.K.; Farris, M.S.; Courneya, K.S. Physical activity and cancer outcomes: A precision medicine approach. Clin. Cancer Res. 2016, 22, 4766–4775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, R.J.; Ngo, T.H.; Leung, P.S.; Aronson, W.J.; Golding, L.A. A low-fat diet and/or strenuous exercise alters the IGF axis in vivo and reduces prostate tumor cell growth in vitro. Prostate 2003, 56, 50150–50156. [Google Scholar] [CrossRef]
- Barnard, R.J.; Kobayashi, N.; Aronson, W.J. Effect of diet and exercise intervention on the growth of prostate epithelial cells. Prostate Cancer Prostatic Dis. 2008, 11, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Avery, K.N.; Donovan, J.L.; Gilbert, R.; Davis, M.; Emmett, P.; Down, L.; Oliver, S.; Neal, D.E.; Hamdy, F.C.; Lane, J.A. Men with prostate cancer make positive dietary changes following diagnosis and treatment. Cancer Causes Control. 2013, 24, 1119–1128. [Google Scholar] [CrossRef]
- Rubin, M.A.; Girelli, G.; Demichelis, F. Genomic correlates to the newly proposed grading prognostic groups for prostate cancer. Eur. Urol. 2016, 69, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Registro Tumori del Friuli Venezia Giulia. Dati di incidenza, 1999–2003. Available online: http://www.cro.sanita.fvg.it/opencms/export/sites/cro/it/_organigramma/_docs/Registro-Tumori-FVG-1999_2003.pdf (accessed on 18 December 2020).



{kind=link}
{kind=link}
| MDS | Physical Activity | |||||||
|---|---|---|---|---|---|---|---|---|
| Low (0–4) | High (5–9) | Low/Moderate | High | |||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| Age (years) | ||||||||
| <65 | 158 | (40.1) | 156 | (40.7) | 178 | (41.3) | 136 | (39.3) |
| ≥65 | 236 | (59.9) | 227 | (59.3) | 253 | (58.7) | 210 | (60.7) |
| p = 0.858 | p = 0.574 | |||||||
| Education (years) | ||||||||
| <7 | 230 | (58.4) | 166 | (43.3) | 162 | (37.5) | 234 | (67.6) |
| 7 to 11 | 94 | (23.9) | 133 | (34.7) | 157 | (36.3) | 71 | (20.5) |
| ≥12 | 70 | (17.8) | 84 | (21.9) | 113 | (26.2) | 41 | (11.9) |
| p < 0.001 | p < 0.001 | |||||||
| Gleason score | ||||||||
| 2–6 | 195 | (49.5) | 200 | (52.2) | 232 | (53.8) | 163 | (47.1) |
| 7 | 83 | (21.1) | 81 | (21.2) | 92 | (21.3) | 72 | (20.8) |
| 8–10 | 73 | (18.5) | 47 | (12.3) | 59 | (13.6) | 61 | (17.6) |
| Unknown | 43 | (10.9) | 55 | (14.4) | 48 | (11.1) | 50 | (14.5) |
| p = 0.071 | p = 0.149 | |||||||
| Tobacco smoking | ||||||||
| Never | 121 | (30.7) | 104 | (27.2) | 125 | (29.0) | 100 | (28.9) |
| Former | 185 | (47.0) | 214 | (55.9) | 219 | (50.8) | 180 | (52.0) |
| Current | 88 | (22.3) | 65 | (17.0) | 87 | (20.2) | 66 | (19.1) |
| p = 0.035 | p = 0.916 | |||||||
| Central obesity a | ||||||||
| No | 256 | (65.0) | 254 | (66.3) | 281 | (65.2) | 229 | (66.2) |
| Yes | 138 | (35.0) | 129 | (33.7) | 150 | (34.8) | 117 | (33.8) |
| p = 0.693 | p = 0.773 | |||||||
| Total energy intake (kJ) | ||||||||
| <9811 | 133 | (33.8) | 125 | (32.6) | 178 | (41.3) | 80 | (23.1) |
| 9811 to <12,502 | 130 | (33.0) | 129 | (33.7) | 151 | (35.0) | 108 | (31.2) |
| ≥12,502 | 131 | (33.3) | 129 | (33.7) | 102 | (23.7) | 158 | (45.7) |
| p = 0.946 | p < 0.001 | |||||||
| Score | Patients | Deaths | Survival Probabilities | HR (95% CI) a | |||
|---|---|---|---|---|---|---|---|
| n | (%) | 5 Years | 10 Years | 15 Years | |||
| Mediterranean Diet Score | |||||||
| Low (0–4) | 394 | 180 | (45.7) | 86.3% | 69.5% | 50.7% | Reference |
| High (5–9) | 383 | 151 | (39.4) | 92.4% | 76.5% | 57.3% | 0.80 (0.60–1.00) |
| Physical activity | |||||||
| Low/Moderate | 389 | 183 | (47.0) | 87.6% | 69.3% | 49.5% | Reference |
| High | 388 | 148 | (38.1) | 91.0% | 76.6% | 58.5% | 0.79 (0.63–0.98) |
| Mediterranean Diet Score and Physical activity | |||||||
| Low and Low/Moderate | 197 | 66 | (33.5) | 89.8% | 84.2% | 66.2% | Reference |
| Low and High | 197 | 53 | (26.9) | 94.9% | 88.3% | 72.8% | 0.70 (0.48 to 1.02) |
| High and Low/Moderate | 234 | 55 | (23.5) | 97.0% | 92.7% | 76.3% | 0.66 (0.46 to 0.95) |
| High and High | 149 | 34 | (22.8) | 94.0% | 91.3% | 76.9% | 0.58 (0.38 to 0.90) |
| Score | Patients | PCa Mortality | Non-PCa Mortality | ||||
|---|---|---|---|---|---|---|---|
| Events | HR (95% CI) | Events | HR (95% CI) | ||||
| n | (%) | n | (%) | ||||
| Mediterranean Diet Score | |||||||
| Low (0–4) | 394 | 41 | (10.4) | Reference | 78 | (19.8) | Reference |
| High (5–9) | 383 | 34 | (8.9) | 0.83 (0.53 to 1.31) | 55 | (14.4) | 0.73 (0.51 to 1.05) |
| Physical activity | |||||||
| Low/Moderate | 427 | 40 | (9.4) | Reference | 81 | (19.0) | Reference |
| High | 346 | 35 | (10.1) | 0.95 (0.57 to 1.59) | 52 | (15.0) | 0.72 (0.49 to 1.08) |
| Mediterranean Diet Score and Physical activity | |||||||
| Low and Low/Moderate | 197 | 21 | (10.7) | Reference | 45 | (22.8) | Reference |
| Low and High | 197 | 19 | (8.1) | 0.85 (0.44 to 1.65) | 36 | (15.4) | 0.67 (0.41 to 1.10) |
| High and Low/Moderate | 234 | 20 | (10.2) | 0.75 (0.41 to 1.38) | 33 | (16.8) | 0.68 (0.43 to 1.07) |
| High and High | 149 | 15 | (10.0) | 0.79 (0.40 to 1.59) | 19 | (12.8) | 0.51 (0.29 to 0.91) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Maso, M.; Augustin, L.S.A.; Toffolutti, F.; Stocco, C.; Dal Maso, L.; Jenkins, D.J.A.; Fleshner, N.E.; Serraino, D.; Polesel, J. Adherence to Mediterranean Diet, Physical Activity and Survival after Prostate Cancer Diagnosis. Nutrients 2021, 13, 243. https://doi.org/10.3390/nu13010243
Di Maso M, Augustin LSA, Toffolutti F, Stocco C, Dal Maso L, Jenkins DJA, Fleshner NE, Serraino D, Polesel J. Adherence to Mediterranean Diet, Physical Activity and Survival after Prostate Cancer Diagnosis. Nutrients. 2021; 13(1):243. https://doi.org/10.3390/nu13010243
Chicago/Turabian StyleDi Maso, Matteo, Livia S. A. Augustin, Federica Toffolutti, Carmen Stocco, Luigino Dal Maso, David J. A. Jenkins, Neil E. Fleshner, Diego Serraino, and Jerry Polesel. 2021. "Adherence to Mediterranean Diet, Physical Activity and Survival after Prostate Cancer Diagnosis" Nutrients 13, no. 1: 243. https://doi.org/10.3390/nu13010243