Effect of Ingestion of Medium-Chain Triglycerides on Substrate Oxidation during Aerobic Exercise Could Depend on Sex Difference in Middle-Aged Sedentary Persons

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
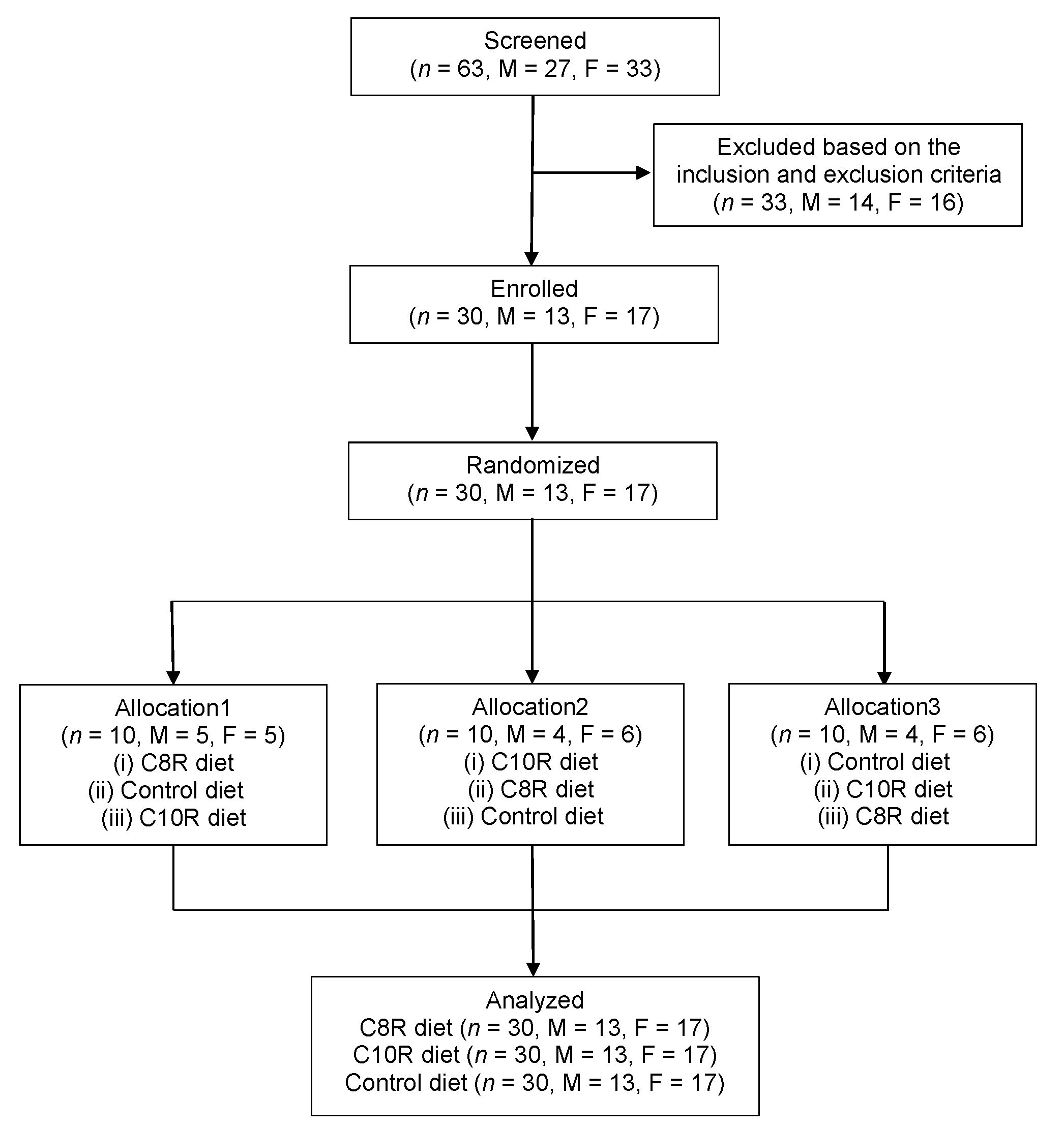
2.2. Participants
2.3. Randomized Allocation
2.4. Test Drink
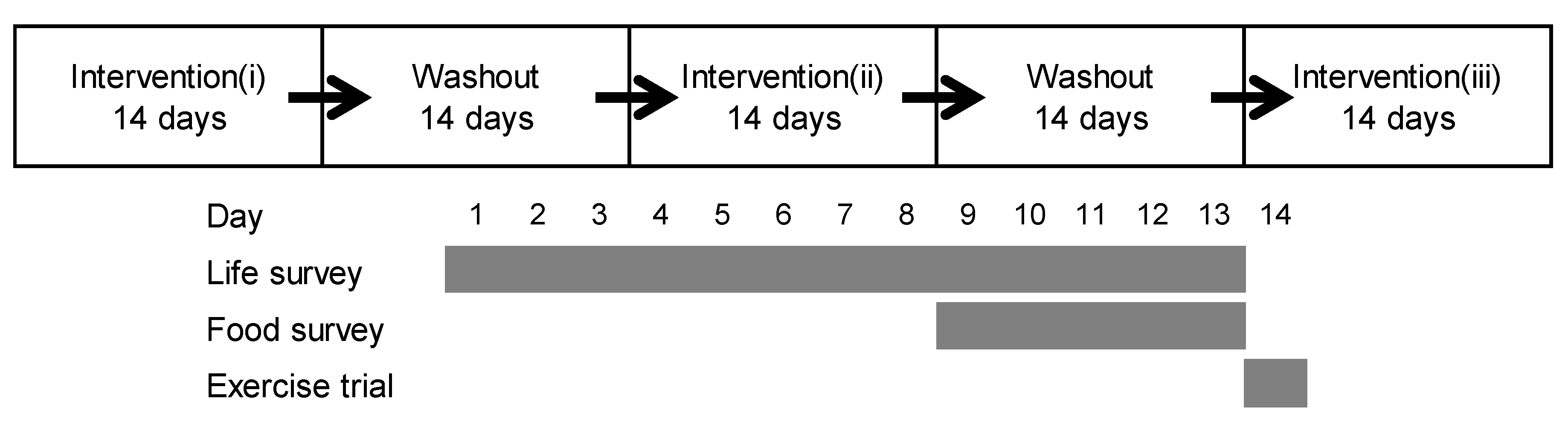
2.5. Intervention
2.6. Exercise Trial
2.7. Calculation
2.8. Statistical Analyses
3. Results
3.1. Participants
3.2. Dietary Intake
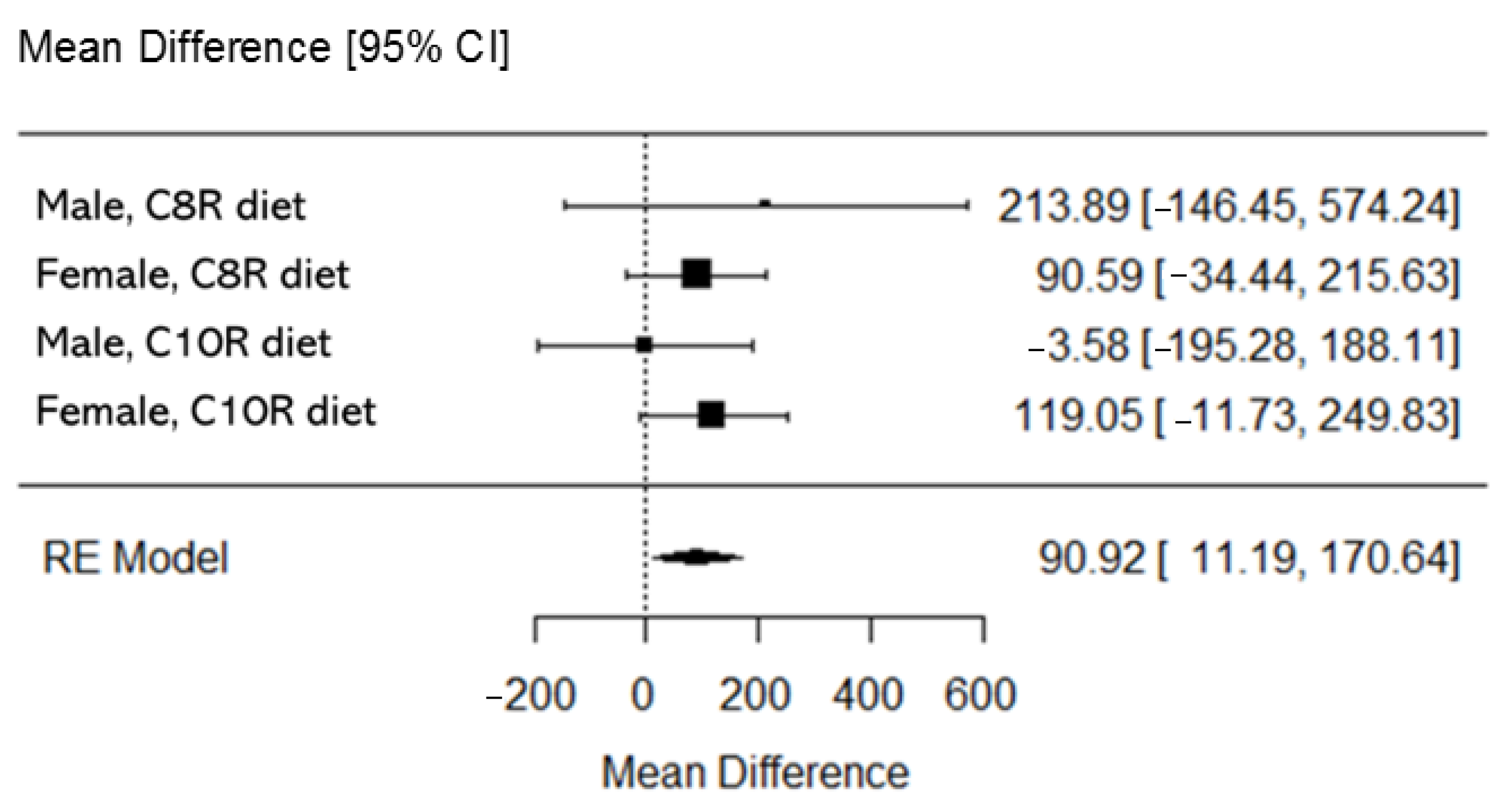
3.3. Exercise Trial
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FAO | Fat oxidation |
| CAO | Carbohydrate oxidation |
| RER | Respiratory exchange ratio |
| VT | Ventilation threshold |
| cFAO | Cumulative value of FAO |
| cCAO | Cumulative value of CAO |
| mFAO | Maximal FAO rate |
| PO | Power output |
| VE/VCO2 | Ventilation volume per VCO2 |
| @ | At time of |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Intervention Effect, ∆ | Diet | Female, n = 17W | p | Male, n = 13W | p |
|---|---|---|---|---|---|
| Cumulative fat oxidation, mg | |||||
| 20Ex | C8R | 0.98 | 0.95 | 0.95 | 0.55 |
| C10R | 0.97 | 0.74 | 0.93 | 0.37 | |
| InEx (~VT) | C8R | 0.96 | 0.57 | 0.94 | 0.46 |
| C10R | 0.95 | 0.39 | 0.83 | 0.02 | |
| # overall (20Ex and InEx, ~VT) | C8R | 0.95 | 0.53 | 0.96 | 0.73 |
| C10R | 0.92 | 0.14 | 0.93 | 0.31 | |
| Cumulative carbohydrate oxidation, mg | |||||
| 20Ex | C8R | 0.93 | 0.21 | 0.96 | 0.69 |
| C10R | 0.96 | 0.67 | 0.93 | 0.33 | |
| InEx (~VT) | C8R | 0.97 | 0.85 | 0.96 | 0.72 |
| C10R | 0.93 | 0.18 | 0.91 | 0.18 | |
| # overall (20Ex and InEx, ~VT) | C8R | 0.97 | 0.89 | 0.97 | 0.86 |
| C10R | 0.90 | 0.06 | 0.92 | 0.22 | |
| Maximal fat-oxidation rate, mg/min | |||||
| 20Ex | C8R | 0.96 | 0.65 | 0.94 | 0.51 |
| C10R | 0.98 | 0.98 | 0.92 | 0.22 | |
| InEx | C8R | 0.95 | 0.53 | 0.94 | 0.51 |
| C10R | 0.88 | 0.03 | 0.93 | 0.36 | |
| Respiratory exchange ratio | |||||
| 20Ex (at mFAO) | C8R | 0.97 | 0.89 | 0.97 | 0.85 |
| C10R | 0.97 | 0.78 | 0.93 | 0.30 | |
| # InEx (at mFAO) | C8R | 0.99 | 0.99 | 0.97 | 0.93 |
| C10R | 0.96 | 0.67 | 0.97 | 0.92 | |
| Power output, W | |||||
| InEx (at VT) | C8R | 0.97 | 0.82 | 0.93 | 0.29 |
| C10R | 0.93 | 0.21 | 0.96 | 0.81 | |
| Elapsed time, sec | |||||
| overall (20Ex and InEx, ~VT) | C8R | 0.97 | 0.83 | 0.93 | 0.39 |
| C10R | 0.92 | 0.17 | 0.97 | 0.83 | |
| Oxygen uptake, ml/min | |||||
| InEx (at VT) | C8R | 0.96 | 0.57 | 0.87 | 0.05001 |
| C10R | 0.87 | 0.02 | 0.96 | 0.73 | |
| Ventilation volume per VCO2 volume, mL/mL | |||||
| InEx (at VT) | C8R | 0.94 | 0.36 | 0.96 | 0.79 |
| C10R | 0.92 | 0.16 | 0.99 | 1.00 | |
References
- Fletcher, G.; Eves, F.F.; Glover, E.I.; Robinson, S.L.; Vernooij, C.A.; Thompson, J.L.; Wallis, G.A. Dietary intake is independently associated with the maximal capacity for fat oxidation during exercise. Am. J. Clin. Nutr. 2017, 105, 864–872. [Google Scholar] [CrossRef]
- Sahlin, K.; Mogensen, M.; Bagger, M.; Fernström, M.; Pedersen, P.K. The potential for mitochondrial fat oxidation in human skeletal muscle influences whole body fat oxidation during low-intensity exercise. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E223–E230. [Google Scholar] [CrossRef] [Green Version]
- Leckey, J.J.; Hoffman, N.J.; Parr, E.B.; Devlin, B.L.; Trewin, A.J.; Stepto, N.K.; Morton, J.P.; Burke, L.M.; Hawley, J.A. High dietary fat intake increases fat oxidation and reduces skeletal muscle mitochondrial respiration in trained humans. FASEB J. 2018, 32, 2979–2991. [Google Scholar] [CrossRef] [Green Version]
- Murphy, N.E.; Carrigan, C.T.; Margolis, L.M. High-fat ketogenic diets and physical performance: A systematic review. Adv. Nutr. 2020, nmaa101. [Google Scholar] [CrossRef]
- Evans, M.; Cogan, K.E.; Egan, B. Metabolism of ketone bodies during exercise and training: Physiological basis for exogenous supplementation. J. Physiol. 2017, 595, 2857–2871. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.M.; Whitfield, J.; Heikura, I.A.; Ross, M.L.R.; Tee, N.; Forbes, S.F.; Hall, R.; McKay, A.K.A.; Wallett, A.M.; Sharma, A.P. Adaptation to a low carbohydrate high fat diet is rapid but impairs endurance exercise metabolism and performance despite enhanced glycogen availability. J. Physiol. 2020. [Google Scholar] [CrossRef]
- Nosaka, N.; Suzuki, Y.; Suemitsu, H.; Kasai, M.; Kato, K.; Taguchi, M. Medium-chain triglycerides with maltodextrin increase fat oxidation during moderate-intensity exercise and extend the duration of subsequent high-intensity exercise. J. Oleo Sci. 2018, 67, 1455–1462. [Google Scholar] [CrossRef] [Green Version]
- Bach, A.C.; Babayan, V.K. Medium-chain triglycerides: An update. Am. J. Clin. Nutr. 1982, 36, 950–962. [Google Scholar] [CrossRef]
- Traul, K.A.; Driedger, A.; Ingle, D.L.; Nakhasi, D. Review of the toxicologic properties of medium-chain triglycerides. Food Chem. Toxicol. 2000, 38, 79–98. [Google Scholar] [CrossRef]
- Fushiki, T.; Matsumoto, K.; Inoue, K.; Kawada, T.; Sugimoto, E. Swimming endurance capacity of mice is increased by chronic consumption of medium-chain triglycerides. J. Nutr. 1995, 125, 531–539. [Google Scholar]
- Nosaka, N.; Suzuki, Y.; Nagatoishi, A.; Kasai, M.; Wu, J.; Taguchi, M. Effect of ingestion of medium-chain triacylglycerols on moderate- and high-intensity exercise in recreational athletes. J. Nutr. Sci. Vitaminol. 2009, 55, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Ishizawa, R.; Masuda, K.; Sakata, S.; Nakatani, A. Effect of different fatty acid chain length on fatty acid oxidation-related protein expression levels in rat skeletal muscle. J. Oleo Sci. 2015, 64, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Venables, M.C.; Achten, J.; Jeukendrup, A.E. Determinants of fat oxidation during exercise in healthy men and women: A cross-sectional study. J. Appl. Physiol. 2005, 98, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Rynders, C.A.; Angadi, S.S.; Weltman, N.Y.; Gaesser, G.A.; Weltman, A. Oxygen uptake and ratings of perceived exertion at the lactate threshold and maximal fat oxidation rate in untrained adults. Eur. J. Appl. Physiol. 2011, 111, 2063–2068. [Google Scholar] [CrossRef] [Green Version]
- Ishizawa, R. The Mechanism of Mitochondrial Biogenesis by Fatty Acid in Skeletal Muscles. 2015. Available online: https://kanazawa-u.repo.nii.ac.jp/?action=repository_action_common_download&item_id=35940&item_no=1&attribute_id=31&file_no=1 (accessed on 21 April 2020). (In Japanese).
- Abe, T.; Hirasaka, K.; Kohno, S.; Tomida, C.; Haruna, M.; Uchida, T.; Ohno, A.; Oarada, M.; Teshima-Kondo, S.; Okumura, Y.; et al. Capric acid up-regulates UCP3 expression without PDK4 induction in mouse C2C12 myotubes. J. Nutr. Sci. Vitaminol. 2016, 62, 32–39. [Google Scholar] [CrossRef]
- St-Pierre, V.; Vandenberghe, C.; Lowry, C.-M.; Fortier, M.; Castellano, C.-A.; Wagner, R.; Cunnane, S.C. Plasma ketone and medium chain fatty acid response in humans consuming different medium chain triglycerides during a metabolic study day. Front Nutr. 2019, 6, 46. [Google Scholar] [CrossRef]
- Nosaka, N.; Tsujino, S.; Honda, K.; Suemitsu, H.; Kato, K. Enhancement of fat oxidation during submaximal exercise in sedentary persons: Variations by medium-chain fatty acid composition and age group. Lipids 2020, 55, 173–183. [Google Scholar] [CrossRef]
- The University Hospital Medical Information Network Center, Clinical Trials Registry. Available online: https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000038644 (accessed on 1 December 2020).
- Ministry of Education, Culture, Sports, Science and Technology, Japan. Standard Tables of Food Composition in Japan -2015- (Seventh revised Edition). 2015. Available online: http://www.mext.go.jp/en/policy/science_technology/policy/title01/detail01/1374030.htm (accessed on 22 April 2020).
- Schneider, D.A.; Phillips, S.E.; Stoffolano, S. The simplified V-slope method of detecting the gas exchange threshold. Med. Sci. Sports Exerc. 1993, 25, 1180–1184. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Saris, W.H.; Schrauwen, P.; Brouns, F.; Wagenmakers, A.J. Metabolic availability of medium-chain triglycerides coingested with carbohydrates during prolonged exercise. J. Appl. Physiol. 1995, 79, 756–762. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Thielen, J.J.; Wagenmakers, A.J.; Brouns, F.; Saris, W.H. Effect of medium-chain triacylglycerol and carbohydrate ingestion during exercise on substrate utilization and subsequent cycling performance. Am. J. Clin. Nutr. 1998, 67, 397–404. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria, 2017. Available online: https://www.R-project.org/ (accessed on 1 December 2020).
- Nagao, K.; Yanagita, T. Medium-chain fatty acids: Functional lipids for the prevention and treatment of the metabolic syndrome. Pharmacol. Res. 2010, 61, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Ivy, J.L.; Costill, D.L.; Fink, W.J.; Maglischo, E. Contribution of medium and long chain triglyceride intake to energy metabolism during prolonged exercise. Int. J. Sports Med. 1980, 1, 15–20. [Google Scholar] [CrossRef]
- Décombaz, J.; Arnaud, M.J.; Milon, H.; Moesch, H.; Philippossian, G.; Thélin, A.L.; Howald, H. Energy metabolism of medium-chain triglycerides versus carbohydrates during exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 52, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Massicotte, D.; Peronnet, F.; Brisson, G.R.; Hillaire-Marcel, C. Oxidation of exogenous medium-chain fatty acids during prolonged exercise: Comparison with glucose. J. Appl. Physiol. 1992, 73, 1334–1339. [Google Scholar] [CrossRef]
- Van Zyl, C.G.; Lambert, E.V.; Hawley, J.A.; Noakes, T.D.; Dennis, S.C. Effects of medium-chain triglyceride ingestion on fuel metabolism and cycling performance. J. Appl. Physiol. 1996, 80, 2217–2225. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Saris, W.H.M.; Van Diesen, R.; Brouns, F.; Wagenmakers, A.J.M. Effect of endogenous carbohydrate availability on oral medium-chain triglyceride oxidation during prolonged exercise. J. Appl. Physiol. 1996, 80, 949–954. [Google Scholar] [CrossRef] [Green Version]
- Sidossis, L.S.; Gastaldelli, A.; Klein, S.; Wolfe, R.R. Regulation of plasma fatty acid oxidation during low- and high-intensity exercise. Am. J. Physiol. Endocrinol. Metab. 1997, 272, E1065–E1070. [Google Scholar] [CrossRef]
- Melanson, E.L.; MacLean, P.S.; Hill, J.O. Exercise improves fat metabolism in muscle but does not increase 24-h fat oxidation. Exerc. Sport Sci. Rev. 2009, 37, 93–101. [Google Scholar] [CrossRef]
- Ööpik, V.; Timpmann, S.; Medijainen, L.; Lemberg, H. Effects of daily medium-chain triglyceride ingestion on energy metabolism and endurance performance capacity in well-trained runners. Nutr. Res. 2001, 21, 1125–1135. [Google Scholar] [CrossRef]
- Misell, L.M.; Lagomarcino, N.D.; Schuster, V.; Kern, M. Chronic medium-chain triacylglycerol consumption and endurance performance in trained runners. J. Sports Med. Phys. Fit. 2001, 41, 210–215. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 21 April 2020).
- Fukazawa, A.; Koike, A.; Karasawa, T.; Tsutsui, M.; Kondo, S.; Terada, S. Effects of a ketogenic diet containing medium-chain triglycerides and endurance training on metabolic enzyme adaptations in rat skeletal muscle. Nutrients 2020, 12, 1269. [Google Scholar] [CrossRef]
- Turner, N.; Hariharan, K.; TidAng, J.; Frangioudakis, G.; Beale, S.M.; Wright, L.E.; Zeng, X.Y.; Leslie, S.J.; Li, J.-Y.; Kraegen, E.W.; et al. Enhancement of muscle mitochondrial oxidative capacity and alterations in insulin action are lipid species dependent. Diabetes 2009, 58, 2547–2554. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare, Japan. Physical Activity Reference for Health Promotion. 2013. Available online: http://www.nibiohn.go.jp/eiken/info/pdf/sintai2013.pdf (accessed on 20 April 2020). (In Japanese)
- Aihara, Y.; Takahashi, Y.; Kotoyori, T.; Mitsuda, T.; Ito, R.; Aihara, M.; Ikezawa, Z.; Yokota, S. Frequency of food-dependent, exercise-induced anaphylaxis in Japanese junior-high-school students. J. Allergy Clin. Immunol. 2001, 108, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Urisu, A.; Ebisawa, M.; Ito, K.; Aihara, Y.; Ito, S.; Mayumi, M.; Kohno, Y.; Kondo, N.; Committee for Japanese Pediatric Guideline for Food Allergy, Japanese Society of Pediatric Allergy and Clinical Immunology; Japanese Society of Allergology. Japanese guideline for food allergy 2014. Allergol. Int. 2014, 63, 399–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Nutrition | Control | C8R | C10R |
|---|---|---|---|
| Energy, kcal | 200 | 200 | 200 |
| Protein, g | 1.4 | 1.4 | 1.4 |
| Fat, g | 0 | 6.0 | 6.0 |
| (C8R MCTs, g) | (-) | (6.0) | (-) |
| (C10R MCTs, g) | (-) | (-) | (6.0) |
| Carbohydrate, g | 48.0 | 34.6 | 34.6 |
| Characteristics | Sex | Value |
|---|---|---|
| Number, n | Female | 17 |
| Male | 13 | |
| Age, year | Female | 48.2 ± 3.7 |
| Male | 48.8 ± 3.6 | |
| Height, cm | Female | 157.8 ± 5.0 |
| Male | 169.1 ± 8.8 | |
| Body weight, kg | Female | 55.4 ± 5.6 |
| Male | 67.8 ± 9.0 | |
| Body mass index, kg/m2 | Female | 22.2 ± 1.7 |
| Male | 23.6 ± 1.1 |
| Nutritional Indices | Control Diet | C8R Diet | C10R Diet |
|---|---|---|---|
| Female, n = 17 | |||
| Energy, kcal | 1758 ± 337 | 1755 ± 252 | 1775 ± 349 |
| Protein, g | 56.6 ± 13.0 | 57.9 ± 9.7 | 58.3 ± 10.6 |
| Fat, g | 58.9 ± 17.3 | 63.6 ± 12.6 | 67.9 ± 14.8 |
| Octanoic acid, mg | 124.8 ± 118.5 | 3790.8 ± 78.8 * | 1623.4 ± 67.1 * |
| Decanoic acid, mg | 211.5 ± 147.6 | 1506.2 ± 142.4 * | 3724.0 ± 133.2 * |
| Carbohydrate, g | 240.5 ± 47.6 | 225.5 ± 35.9 | 223.5 ± 52.9 |
| Male, n = 13 | |||
| Energy, kcal | 1978 ± 342 | 2034 ± 412 | 1936 ± 430 |
| Protein, g | 69.6 ± 19.2 | 70.9 ± 17.2 | 64.8 ± 12.4 |
| Fat, g | 63.2 ± 16.5 | 69.8 ± 20.5 | 67.0 ± 22.0 |
| Octanoic acid, mg | 88.5 ± 116.4 | 3748.8 ± 101.7 * | 1585.4 ± 84.0 * |
| Decanoic acid, mg | 167.3 ± 227.8 | 1402.6 ± 121.2 * | 3657.9 ± 150.5 * |
| Carbohydrate, g | 268.5 ± 49.9 | 259.7 ± 51.8 | 253.2 ± 55.8 |
| Intervention Effect, ∆ | Diet | Female, n = 17 | p | Male, n = 13 | p |
|---|---|---|---|---|---|
| Cumulative fat oxidation, mg | |||||
| # 20Ex | C8R | 12.1 ± 16.2 | 0.46 | 84.0 ± 28.2 | 0.007 |
| C10R | 6.5 ± 16.2 | 0.69 | 37.1 ± 28.2 | 0.20 | |
| # InEx (~VT) | C8R | 82.6 ± 55.0 | 0.14 | 118 ± 139 | 0.41 |
| C10R | 108 ± 55.0 | 0.06 | −28.6 ± 139 | 0.84 | |
| # overall (20Ex and InEx, ~VT) | C8R | 94.7 ± 65.8 | 0.16 | 202 ± 151 | 0.20 |
| C10R | 115 ± 65.8 | 0.09 | 8.5 ± 151 | 0.96 | |
| Cumulative carbohydrate oxidation, mg | |||||
| # 20Ex | C8R | 9.1 ± 38.8 | 0.82 | −286 ± 81.6 | 0.002 |
| C10R | −9.8 ± 38.8 | 0.80 | −46 ± 81.6 | 0.58 | |
| # InEx (~VT) | C8R | 775 ± 373 | 0.046 | −188 ± 770 | 0.81 |
| C10R | 825 ± 373 | 0.03 | 366 ± 770 | 0.64 | |
| # overall (20Ex and InEx, ~VT) | C8R | 784 ± 381 | 0.048 | −474 ± 803 | 0.56 |
| C10R | 815 ± 381 | 0.04 | 320 ± 803 | 0.69 | |
| Maximal fat-oxidation rate, mg/min | |||||
| # 20Ex | C8R | 11.6 ± 8.7 | 0.19 | 38.2 ± 17.4 | 0.04 |
| C10R | 1.8 ± 8.7 | 0.84 | 22.0 ± 17.4 | 0.22 | |
| # InEx | C8R | 16.6 ± 9.3 | 0.08 | 22.4 ± 21.2 | 0.30 |
| C10R | 12.3 ± 8.1 | 0.20 | 9.2 ± 21.2 | 0.67 | |
| Respiratory exchange ratio | |||||
| # 20Ex (at mFAO) | C8R | −0.009 ± 0.008 | 0.28 | −0.05 ± 0.02 | 0.007 |
| C10R | −0.004 ± 0.008 | 0.63 | −0.02 ± 0.02 | 0.30 | |
| # InEx (at mFAO) | C8R | −0.007 ± 0.008 | 0.38 | −0.03 ± 0.01 | 0.02 |
| C10R | −0.006 ± 0.008 | 0.48 | −0.01 ± 0.01 | 0.27 | |
| Power output, W | |||||
| # InEx (at VT) | C8R | 2.5 ± 2.0 | 0.23 | 4.5 ± 4.1 | 0.28 |
| C10R | 5.8 ± 2.0 | 0.008 | 4.3 ± 4.1 | 0.30 | |
| Elapsed time, sec | |||||
| overall (20Ex and InEx, ~VT) | C8R | 15.2 ± 12.3 | 0.22 | 22.0 ± 19.1 | 0.26 |
| C10R | 34.8 ± 12.3 | 0.008 | 21.1 ± 19.1 | 0.28 | |
| Oxygen uptake, ml/min | |||||
| # InEx (at VT) | C8R | 28.8 ± 31.2 | 0.36 | −31.2 ± 78.6 | 0.70 |
| C10R | 60.5 ± 27.2 | 0.009 | 67.9 ± 78.6 | 0.40 | |
| Ventilation volume per VCO2 volume, mL/mL | |||||
| # InEx (at VT) | C8R | 0.01 ± 0.43 | 0.99 | 0.56 ± 0.42 | 0.20 |
| C10R | −0.39 ± 0.43 | 0.37 | 0.77 ± 0.42 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nosaka, N.; Tsujino, S.; Honda, K.; Suemitsu, H.; Kato, K.; Kondo, K. Effect of Ingestion of Medium-Chain Triglycerides on Substrate Oxidation during Aerobic Exercise Could Depend on Sex Difference in Middle-Aged Sedentary Persons. Nutrients 2021, 13, 36. https://doi.org/10.3390/nu13010036
Nosaka N, Tsujino S, Honda K, Suemitsu H, Kato K, Kondo K. Effect of Ingestion of Medium-Chain Triglycerides on Substrate Oxidation during Aerobic Exercise Could Depend on Sex Difference in Middle-Aged Sedentary Persons. Nutrients. 2021; 13(1):36. https://doi.org/10.3390/nu13010036
Chicago/Turabian StyleNosaka, Naohisa, Shougo Tsujino, Kazumitsu Honda, Hiromi Suemitsu, Kazuhiko Kato, and Kazuo Kondo. 2021. "Effect of Ingestion of Medium-Chain Triglycerides on Substrate Oxidation during Aerobic Exercise Could Depend on Sex Difference in Middle-Aged Sedentary Persons" Nutrients 13, no. 1: 36. https://doi.org/10.3390/nu13010036
APA StyleNosaka, N., Tsujino, S., Honda, K., Suemitsu, H., Kato, K., & Kondo, K. (2021). Effect of Ingestion of Medium-Chain Triglycerides on Substrate Oxidation during Aerobic Exercise Could Depend on Sex Difference in Middle-Aged Sedentary Persons. Nutrients, 13(1), 36. https://doi.org/10.3390/nu13010036