
Dietary Interventions to Prevent Childhood Obesity: A Literature Review


Abstract
:1. Introduction
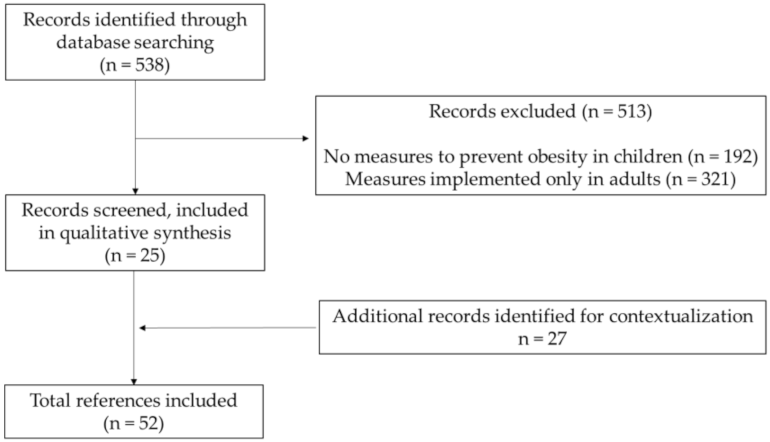
2. Materials and Methods
3. Results
3.1. School-Based Interventions
3.2. Community-Based Interventions
3.3. Interventions through Mass Media
3.4. Food Sector Interventions

{kind=link}
| Author (Study Title) (Reference) | Country, Year | Type of Intervention | Intervention Description | Target Audience | Results |
|---|---|---|---|---|---|
| School-Based Interventions | |||||
| Niederer I, et al. (Ballabeina study) [13] | Switzerland, 2009 | Cluster randomized controlled single-blinded trial | Lessons on nutrition (balanced nutrition and healthy nutritional behaviors in a didactic way), physical activity program, media use, and sleep, and adaptation of the built environment of the preschool. | Preschool children (mean 5.1 years) (n = 652), the parents, and the teachers | No differences in children’s BMI were found between groups. However, the intervention group had a reduction in body fat percentage, better motor agility, as well as benefits in reported physical activity, media use, and eating habits. |
| Singh AS, et al. [14,15] | Netherlands, 2006 | School-based trial | Educational component (classes in biology and physical education, and a computer-based information program); and an environmental component (e.g., serving smaller portion sizes in the canteen and healthier options, restricting access to vending machines, and food awareness by posters). | Students from the ages of 12–14 years (n = 1108) | With a twelve-month follow-up, a reduction in the skinfold thickness of the intervention groups was found, as well as lower consumption of sugar-containing beverages, and less screen time (but only in boys). |
| Kain J, et al. [16] | Chile, 2004 | School-based obesity-prevention trial | Weekly classes on physical activity and healthy nutrition for parents and students. Some environmental changes were also made (e.g., school kiosks were instructed to offer healthier choices and at the same time remain lucrative). | Parents and students from 1st to 8th grade; 2141 schools in the intervention group and 945 in the control group. | After 6 months, there was a reduction of body mass index (BMI) z-scores in boys and better physical fitness in both genders. On the other hand, the modifications in the kiosk’s food availability did not seem to change the students’ food choices. |
| Hollar D, et al. (Healthier Options for Public Schoolchildren (HOPS)) [17] | Florida, US, 2004–2006 | Randomized trial | Modifications in the school menu, school gardens, and physical activity; monthly newsletters with healthy nutrition and physical activity lessons for the students and parents. | 6 elementary schools (4588 children aged 6 to 13 years; 48% Hispanic) | After 2 years, a higher percentage of students who maintained a normal weight (<85th percentile of BMI-for-age) was found in the intervention group (52.1%) when comparing with the control group (40.7%). Students in the intervention group had improved academic performance. |
| Economos CD, et al. (Shape up Somerville) [18] | United States, (September 2003–June 2005) | Non-randomized controlled trial | Dietary intervention (e.g., promotion of fresh fruit and vegetables and taste tests, posters with nutritional and health information, training of food staff, modification of food offers in restaurants according to the study guidelines); increase of physical activity opportunities around the school (e.g., information on safe routes); modifications inside the school space (e.g., new equipment). | 1178 children (average 7.92 years) attending public school in three different communities from Somerville, Massachusetts | After 1 year, the BMI z-scores were 0.06 lower in the intervention group than in the control group. There was a decrease in overweight and obesity and an increase in remission in both sexes in the intervention group. The study design did not include randomization of the intervention. |
| Bacardí-Gascon M, et al. [19] | Mexico, 2012 | Randomized cluster controlled trial | Sessions discussing healthy lifestyles to the school board and the teachers; interactive lessons to the children to increase fruit and vegetables intake and physical activity practice, and reduce soda and high fat and salt-containing snacks intake, while simultaneously decreasing TV watching time; healthy eating sessions to parents. | 532 school-aged children from 2nd and 3rd grade | By the sixth month, there was a greater decrease in BMI in the intervention group than in the control group (difference of −0.82 kg/m2 in children BMI), although it was not sustained after 18 and 24 months of intervention. |
| Foster GD, et al. [20] | USA, 2008 | Multicomponent School Nutrition Policy Initiative | School self-assessment (e.g., strategies like limiting the use of food as reward/punishment, promoting active recess, and serving breakfasts in classrooms); training of school staff and children in nutrition education; nutrition policies (e.g., changing sold foods); social marketing; school association meetings/workshops. | 1349 students in grades 4 through 6 from 10 schools | There were significantly fewer children in the intervention schools (7.5%) than in the control schools (14.9%) who became overweight after 2 years, but no differences after 2 years of follow-up. |
| Donnelly JE, et al. [21] | Nebraska, USA, 1996 | 2-year trial | Nutrition education (basic nutrition, diet, and general health, nutrition for growth and development, healthy food choices, snack alternatives, food safety), modified school lunches (meals planned according to the Lunchpower! Program aiming to reduce energy, fat, and sodium lunches), and increased physical activity. | Students from grades 3 to 5 in two school districts in rural Nebraska (n = 338) | After 2 years of the intervention, both schools showed no significant changes in the body fat percentage, but a significant increase in the BMI. The control school showed significantly higher total energy, total fat and sodium intake, and lower fiber intake. |
| Liu Z, et al. (The DECIDE-Children study) [23] | China, 2019 | Cluster-randomized controlled trial | Health education activities for parents and children; supervision and encouragement of children’s physical activity practice outside of school; school policies to prevent obesity. Development of an app called ‘Eat Wisely, Move Happily’ that aids in diffusing information, monitoring the children’s behavior, and managing their weight. | 4-grade primary schools (8–10 years old) (n = 1200) | No known results. |
| Xu H, et al. [24] | China, 2020 | Multicenter randomized controlled trial | Development of a nutrition handbook that was given to all students; nutrition and health courses to students, parents, teachers, and health workers (e.g., meals proportion, how to choose healthy foods, reduce eating out and unhealthy foods); informative posters around the school; course on physical activity for parents, and physical activity classes for students. | 4846 school children aged 7–13 years | The effects on children’s BMI were studied. There were some improvements in the diversity of the foods consumed at breakfast and a decrease in the consumption of some unhealthy foods. |
| Hannon BA, et al. (Abriendo Caminos Program) [25] | Illinois, California, Iowa, Texas, and Puerto Rico, 2019 | Randomized control trial | Workshop presentations and activities on nutrition education, family wellness, and physical activity. | Families of parents and 1 child aged 6–18 years (n = 500) | No known results. |
| Olsen NJ, et al. (Healthy Start) [26] | Denmark, 2020 | Randomized controlled trial | Guidance on how to improve the child’s diet and physical activity, quantity and quality of sleep, and reduce their stress. Cooking classes, games focused on exercise and motor skills development, access to a website with recipes. | Children aged 2 to 6 years (n = 3722) | The clinical effects of this intervention in the children’s growth and body composition were small. |
| Homs C, et al. (FIVALIN project) [27] | Barcelona, 2021 | Quasi-experimental design | Workshops on health education and sports educational sessions. | 810 children aged 8–12 years and 600 parents | No known results. |
| Li B, et al. (The CHIRPY DRAGON intervention) [28] | China, 2019 | Cluster-randomized controlled trial | Workshops and family activities to promote physical activity and healthy eating behaviors; school support to improve physical activity and healthy food provision. | School children with a mean age of 6.15 years (n = 1641) | There was a decrease in the BMI z-scores of the children in the intervention group, along with an increase in the consumption of fruit and vegetables, and a decrease in the consumption of sugar-sweetened beverages and unhealthy snacks. There was also a decrease in screen time and an increase in physical activity in this group. |
| Anselma M, et al. (Kids in Action) [29] | Amsterdam, 2019 | Controlled trial | Meetings with children to develop interventions that targeted their physical activity and healthy eating habits. These interventions consist of environmental changes, organizational changes, or educational approaches. | Children aged 9–12 years from four primary schools | No known results. |
| Hamulka J, et al. (The ABC of Healthy Eating Project) [30] | Poland, 2018 | Education-based intervention study | Diet and lifestyle-related programs for the intervention group and school activities with the theme of nutrition and healthy lifestyles for both the intervention and the control group. | School children aged 11–13 years. (464 students) | No known results. |
| Community-based interventions | |||||
| Elder JP, et al. (MOVE/me Muevo) [31] | San Diego County, USA, 2014 | Randomized community trial | Activities and phone calls from health coaches on how to increase the consumption of fruit and vegetables; decrease the consumption of sugar-sweetened beverages; increase healthy food portions; reduce eating out and do healthier options when eating out; increase the availability and accessibility of healthy foods and beverages at home; reduce the screen time and avoid eating in front of the TV, and increase the number of family meals. | 541 families with children between the ages of 5 and 8 years old | After 2 years, there were no significant differences between the control and the intervention group concerning BMI or waist circumference. Some changes were observed in dietary intake, namely a reduction in fat and sugary beverages in the intervention group. |
| De Silva-Sanigorski A, et al. (Romp & Chomp) [32] | Australia, 2020 | Community-based trial | Changes in the provision of water in childcare centers, childcare policies regarding healthy eating and physical activity; teaching of skills in physical activity and nutrition to the childcare professionals; production and distribution of promotional materials (balloons, stickers, posters, postcards). | Children aged 1–5 y (n = 12,000) and their families | After 3 years of intervention, the 3.5 years old subsample showed considerably lower mean weight, BMI, and z-score BMI, and the 2 and 3.5 years old children showed a considerably lower prevalence of overweight and obesity when compared with the baseline values. The intervention group also showed a considerably lower intake of packaged snacks and fruit juice. |
| Crespo NC, et al. (The Aventuras Para Niños Study) [33] | Southern California, 2003 | Randomized Community-based trial | Three arms: family-only, community-only, or family+community intervention. In the family-only intervention, professionals call/make home visits to discuss how to maintain a healthy diet, prepare meals, and be physically active. The community-only intervention included improving the school’s playgrounds, implementing salad bars, as well as community parks, displaying water bottles in the classrooms for the students, better physical education equipment and healthy menus for the children, all of this combined with spreading media messages through posters, news and point-of-choice messages in grocery stores, with health messages. The family+community included all described. | 811 predominantly Mexican immigrant/Mexican-American mothers with children in kindergarten through second grade | No noteworthy main effects nor interactions for the family or community interventions were found, including on BMI z-scores. Despite the lack of significant effects on the children’s BMI z-score, there were multiple obesity-related behaviors in these children that were changed by the family intervention, like increased consumption of fruit and vegetables. |
| Borys JM, et al. (EPODE (Ensemble Prevenons l’Obesité Des Enfants/Together Let’s Prevent Childhood Obesity) [34] | France, 2004 | Community-based intervention | Changes in local environments, childhood settings, and family norms to make them more supportive and aid the adoption of healthy lifestyles in children. | Children aged 1–12 years, and their families, as well as a wide variety of local stakeholders in 10 French pilot communities | No known results. |
| Swinburn BA, et al. and Schultz JT, et al. (Pacific Obesity Prevention in Communities (OPIC) project) [35,36] | Australia, Fiji, New Zealand, and Tonga, over 30 months, between 2004 and 2009 | Community-based intervention | Interventions aiming to reduce the consumption of high sugar content drinks and energy-dense snacks and increase physical activity. | 18 000 children 12–18 years, 300 stakeholders, 60 multi-professional research staff, 27 research students. | The authors state that the project can produce positive effects in diet and physical activity, but effects on childhood obesity are not clearly described. |
| Interventions through mass media | |||||
| World Health Organization and Assembly of the Republic (TV ban/restrictions of food commercials to kids in several countries [38] and Portugal) [39] | Sweden, Norway, Denmark, Austria, Ireland, Australia, Greece, and Portugal, 2019 | Mass-media based- intervention | Sweden has banned TV food commercials for children under the age of 12 and TV food advertising for children. Norway, Denmark, Austria, Ireland, Australia, and Greece have also made some restrictions on commercials for children. Portugal approved a law to restrict advertising to children for foodstuffs and beverages of high energy value, salt, sugar, and saturated fatty acids content. | Children | No efficacy results. However, energy-dense foods and drinks and fast-food companies often target children in their advertisements, since they are very easily influenced at this age, namely through TV commercials. |
| Interventions through the Food Sector | |||||
| Goiana-da-Silva F, et al. (Taxation of sugar-sweetened beverages) [41] | Portugal, 2017 | Food sector intervention | Taxation of sugar-sweetened beverages as an intervention to reduce its high consumption in the country. | Community | Decrease of 6.58 million liters per year, which translates into a decrease in consumption of 21% compared to the baseline consumption data of IAN-AF 2015–2016. The number of cases of obesity prevented had a higher impact in adolescents (0.012%), preventing 0.76 cases of obesity yearly, followed by an impact of 0.062% in adults aged 18 to <65 years, and the children showed an impact of 0.049%. These data show that Portugal achieved its goal, decreasing sales of sugar-sweetened beverages. |
| Young L, et al. (“Pick the Trick” program) [45] | Australia and New Zealand | Food sector intervention | Providing foods with symbols for the consumers making it easier to identify the healthier choices. | Community | No known results |
| Kelly B, et al. and Nielsen S, et al. (WHO front-of-pack labeling system) [47] | WHO-E Food and Nutrition Action Plan 2015–2020 | Food sector intervention | Among other future policies, there is the intention of application of a single front-of-pack labeling system in all countries. | Community | No known results |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Popkin, B.M. Impact on Body Composition. Proc. Nutr. Soc. 2011, 70, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Null, N. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- Wabitsch, M.; Moss, A.; Kromeyer-Hauschild, K. Unexpected plateauing of childhood obesity rates in developed countries. BMC Med. 2014, 12, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wardle, J.; Carnell, S.; Haworth, C.M.A.; Plomin, R. Evidence for a strong genetic influence on childhood adiposity despite the force of the obesogenic environment. Am. J. Clin. Nutr. 2008, 87, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llewellyn, C.; Wardle, J. Behavioral susceptibility to obesity: Gene-environment interplay in the development of weight. Physiol. Behav. 2015, 152, 494–501. [Google Scholar] [CrossRef]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef]
- Thompson, S.R.; Watson, M.C.; Tilford, S. The Ottawa Charter 30 years on: Still an important standard for health promotion. Int. J. Health Promot. Educ. 2018, 56, 73–84. [Google Scholar] [CrossRef]
- Issanchou, S. Determining Factors and Critical Periods in the Formation of Eating Habits: Results from the Habeat Project. Ann. Nutr. Metab. 2017, 70, 251–256. [Google Scholar] [CrossRef]
- Plachta-Danielzik, S.; Kehden, B.; Landsberg, B.; Rosario, A.S.; Kurth, B.-M.; Arnold, C.; Graf, C.; Hense, S.; Ahrens, W.; Müller, M.J. Attributable Risks for Childhood Overweight: Evidence for Limited Effectiveness of Prevention. Pediatrics 2012, 130, e865–e871. [Google Scholar] [CrossRef] [Green Version]
- Kopelman, P.; Jebb, S.A.; Butland, B. Executive summary: Foresight ‘tackling obesities: Future choices’ project. Obes. Rev. 2007, 8. [Google Scholar] [CrossRef]
- Bleich, S.N.; Segal, J.; Wu, Y.; Wilson, R.; Wang, Y. Systematic review of community-based childhood obesity prevention studies. Pediatrics 2013, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niederer, I.; Kriemler, S.; Zahner, L.; Bürgi, F.; Ebenegger, V.; Hartmann, T.; Meyer, U.; Schindler, C.; Nydegger, A.; Marques-Vidal, P.; et al. Influence of a lifestyle intervention in preschool children on physiological and psychological parameters (Ballabeina): Study design of a cluster randomized controlled trial. BMC Public Health 2009, 9, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.S.; Chin, A.; Paw, M.J.M.; Kremers, S.P.J.; Visscher, T.L.S.; Brug, J.; Van Mechelen, W. Design of the Dutch Obesity Intervention in Teenagers (NRG-DOiT): Systematic development, implementation and evaluation of a school-based intervention aimed at the prevention of excessive weight gain in adolescents. BMC Public Health 2006, 6, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.S.; Chin, A.; Paw, M.J.M.; Brug, J.; van Mechelen, W. Dutch obesity intervention in teenagers: Effectiveness of a school-based program on body composition and behavior. Arch. Pediatr. Adolesc. Med. 2009, 163, 309. [Google Scholar] [CrossRef] [PubMed]
- Kain, J.; Uauy, R.; Vio, A.F.; Cerda, R.; Leyton, B. School-based obesity prevention in Chilean primary school children: Methodology and evaluation of a controlled study. Int. J. Obes. 2004, 28, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Hollar, D.; Messiah, S.E.; Lopez-Mitnik, G.; Hollar, T.L.; Almon, M.; Agatston, A.S. Effect of a two-year obesity prevention intervention on percentile changes in body mass index and academic performance in low-income elementary school children. Am. J. Public Health 2010, 100, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Economos, C.D.; Hyatt, R.R.; Must, A.; Goldberg, J.P.; Kuder, J.; Naumova, E.; Collins, J.J.; Nelson, M.E. Shape Up Somerville two-year results: A community-based environmental change intervention sustains weight reduction in children. Prev. Med. 2013, 57, 322–327. [Google Scholar] [CrossRef]
- Bacardí-Gascon, M.; Pérez-Morales, M.E.; Jiménez-Cruz, A. A six month randomized school intervention and an 18-month follow-up intervention to prevent childhood obesity in Mexican elementary schools. Nutr. Hosp. 2012, 27, 755–762. [Google Scholar] [PubMed]
- Foster, G.D.; Sherman, S.; Borradaile, K.E.; Grundy, K.M.; Vander Veur, S.S.; Nachmani, J.; Karpyn, A.; Kumanyika, S.; Shults, J.; Healy, C.M.; et al. A Policy-Based School Intervention to Prevent Overweight and Obesity. Pediatrics 2008, 121, e794–e802. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.E.; Jacobsen, D.J.; Whatley, J.E.; Hill, J.O.; Swift, L.L.; Cherrington, A.; Polk, B.; Tran, Z.V.; Reed, G. Nutrition and Physical Activity Program to Attenuate Obesity and Promote Physical and Metabolic Fitness in Elementary School Children. Obes. Res. 1996, 4, 229–243. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Healthy People 2000: National Health Promotion and Disease Prevention Objectives; DHHS Publication No. (PHS) 91-50212; U.S. Government Printing Office, Public Health Service: Washington, DC, USA, 1990; pp. 93–134.
- Liu, Z.; Wu, Y.; Niu, W.-Y.; Feng, X.; Lin, Y.; Gao, A.; Zhang, F.; Fang, H.; Gao, P.; Li, H.-J.; et al. A school-based, multi-faceted health promotion programme to prevent obesity among children: Protocol of a cluster-randomised controlled trial (the DECIDE-Children study). BMJ Open 2019, 9, e027902. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Ecker, O.; Zhang, Q.; Du, S.; Liu, A.; Li, Y.; Hu, X.; Li, T.; Guo, H.; Li, Y.; et al. The effect of comprehensive intervention for childhood obesity on dietary diversity among younger children: Evidence from a school-based randomized controlled trial in China. PLoS ONE 2020, 15, e0235951. [Google Scholar] [CrossRef] [PubMed]
- Hannon, B.; Teran-Garcia, M.; Nickols-Richardson, S.M.; Musaad, S.M.; Villegas, E.M.; Hammons, A.; Wiley, A.; Fiese, B.H. Implementation and Evaluation of the Abriendo Caminos Program: A Randomized Control Trial Intervention for Hispanic Children and Families. J. Nutr. Educ. Behav. 2019, 51, 1211–1219. [Google Scholar] [CrossRef]
- Olsen, N.J.; Ängquist, L.; Frederiksen, P.; Lykke Mortensen, E.; Lilienthal Heitmann, B. Primary prevention of fat and weight gain among obesity susceptible healthy weight preschool children. Main results from the “Healthy Start” randomized controlled intervention. Pediatr. Obes. 2021, 16, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Homs, C.; Berruezo, P.; Según, G.; Estrada, L.; de Bont, J.; Riera-Romaní, J.; Carrillo-Álvarez, E.; Schröder, H.; Milà, R.; Gómez, S.F. Family-based intervention to prevent childhood obesity among school-age children of low socioeconomic status: Study protocol of the FIVALIN project. BMC Pediatr. 2021, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Pallan, M.; Liu, W.J.; Hemming, K.; Frew, E.; Lin, R.; Martin, J.; Zanganeh, M.; Hurley, K.; Cheng, K.K.; et al. The CHIRPY DRAGON intervention in preventing obesity in Chinese primary-school--aged children: A cluster-randomised controlled trial. PLoS Med. 2019, 16, e1002971. [Google Scholar] [CrossRef]
- Anselma, M.; Altenburg, T.; Chinapaw, M. Kids in Action: The protocol of a Youth Participatory Action Research project to promote physical activity and dietary behaviour. BMJ Open 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hamulka, J.; Wadolowska, L.; Hoffmann, M.; Kowalkowska, J.; Gutkowska, K. Effect of an education program on nutrition knowledge, attitudes toward nutrition, diet quality, lifestyle, and body composition in polish teenagers. The ABC of healthy eating project: Design, protocol, and methodology. Nutrients 2018, 10, 1439. [Google Scholar] [CrossRef] [Green Version]
- Elder, J.P.; Crespo, N.C.; Corder, K.; Ayala, G.X.; Slymen, D.J.; Lopez, N.V.; Moody, J.S.; McKenzie, T.L. Childhood obesity prevention and control in city recreation centres and family homes: The MOVE/me Muevo Project. Pediatr. Obes. 2014, 9, 218–231. [Google Scholar] [CrossRef] [Green Version]
- De Silva-Sanigorski, A.; Elea, D.; Bell, C.; Kremer, P.; Carpenter, L.; Nichols, M.; Smith, M.; Sharp, S.; Boak, R.; Swinburn, B. Obesity prevention in the family day care setting: Impact of the Romp & Chomp intervention on opportunities for children’s physical activity and healthy eating. Child Care Health Dev. 2011, 37, 385–393. [Google Scholar]
- Crespo, N.C.; Elder, J.P.; Ayala, G.X.; Slymen, D.J.; Campbell, N.R.; Sallis, J.F.; McKenzie, T.L.; Baquero, B.; Arredondo, E.M. Results of a Multi-level Intervention to Prevent and Control Childhood Obesity among Latino Children: The Aventuras Para Niños Study. Ann. Behav. Med. 2012, 43, 84–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borys, J.-M.; Le Bodo, Y.; Jebb, S.A.; Seidell, J.; Summerbell, C.; Richard, D.; De Henauw, S.; Moreno, L.A.; Romon, M.; Visscher, T.L.S.; et al. EPODE approach for childhood obesity prevention: Methods, progress and international development. Obes. Rev. 2011, 13, 299–315. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Millar, L.; Utter, J.; Kremer, P.; Moodie, M.; Mavoa, H.; Snowdon, W.; McCabe, M.; Malakellis, M.; De Courten, M.; et al. The Pacific Obesity Prevention in Communities project: Project overview and methods. Obes. Rev. 2011, 12 (Suppl. 2), 3–11. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.T.; Moodie, M.; Mavoa, H.; Utter, J.; Snowdon, W.; McCabe, M.P.; Millar, L.; Kremer, P.; Swinburn, B.A. Experiences and challenges in implementing complex community-based research project: The Pacific Obesity Prevention in Communities project. Obes. Rev. 2011, 12 (Suppl. 2), 12–19. [Google Scholar] [CrossRef]
- Robinson, T.N. Reducing children’s television viewing to prevent obesity: A randomized controlled trial. JAMA 1999, 282, 1561–1567. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Marketing of Foods High in Fat, Salt and Sugar to Children: Update 2012–2013. 2013. Available online: https://www.euro.who.int/__data/assets/pdf_file/0019/191125/e96859.pdf (accessed on 2 September 2021).
- Assembley of the Republic. Law no 30/2019. Diário da República n.o 79/2019, Série I de 2019-04-23. Available online: https://dre.pt/application/conteudo/122151046 (accessed on 2 September 2021).
- Jacobson, M.F.; Brownell, K.D. Small Taxes on Soft Drinks and Snack Foods to Promote Health | Center for Science in the Public Interest. Am. J. Public Health 2000, 90, 854–857. [Google Scholar]
- Goiana-Da-Silva, F.; Severo, M.; Silva, D.C.E.; Gregório, M.J.; Allen, L.N.; Muc, M.; Nunes, A.M.; Torres, D.; Miraldo, M.; Ashrafian, H.; et al. Projected impact of the Portuguese sugar-sweetened beverage tax on obesity incidence across different age groups: A modelling study. PLoS Med. 2020, 17, e1003036. [Google Scholar] [CrossRef]
- Teng, A.M.; Jones, A.C.; Mizdrak, A.; Signal, L.; Genç, M.; Wilson, N. Impact of sugar-sweetened beverage taxes on purchases and dietary intake: Systematic review and meta-analysis. Obes. Rev. 2019, 20, 1187–1204. [Google Scholar] [CrossRef]
- Roberts, K.E.; Ells, L.J.; McGowan, V.J.; Machaira, T.; Targett, V.C.; Allen, R.E.; Tedstone, A.E. A rapid review examining purchasing changes resulting from fiscal measures targeted at high sugar foods and sugar-sweetened drinks. Nutr. Diabetes 2017, 7, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastasiou, K.; Miller, M.; Dickinson, K. The relationship between food label use and dietary intake in adults: A systematic review. Appetite 2019, 138, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Young, L.; Swinburn, B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Promot. Int. 2002, 17, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. European Food and Nutrition Action Plan 2015–2020 (2014). Denmark: WHO Regional Office for Europe. 2014. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/294474/European-Food-Nutrition-Action-Plan-20152020-en.pdf (accessed on 2 September 2021).
- Kelly, B.; Jewell, J. What Is the Evidence on the Policy Specifications, Development Processes and Effectiveness of Existing Front-of-Pack Food Labelling Policies in the WHO European Region. 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/384460/Web-WHO-HEN-Report-61-on-FOPL.pdf (accessed on 2 September 2021).
- Nielsen, S.; Popkin, B. Patterns and trends in food portion sizes, 1977–1998. JAMA 2003, 289, 450–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, L.R.; Nestle, M. Reducing portion sizes to prevent obesity. Am. J. Prev. Med. 2012, 43, 565–568. [Google Scholar] [CrossRef]
- World Health Organisation. Global Nutrition Policy Review 2016–2017: Country Progress in Creating Enabling Policy Environments for Promoting Healthy Diets and Nutrition. 2018. Available online: https://www.who.int/publications/i/item/9789241514873 (accessed on 2 September 2021).
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention. 2012. Available online: https://apps.who.int/iris/bitstream/handle/10665/80149/9789241504782_eng.pdf;jsessionid=C20C82A9D40706BE6D43BDAB600599FF?sequence=1 (accessed on 2 September 2021).
- Oliveira, A.; Durão, C.; Lopes, C. Social and health behaviour determinants of obesity. In Recent Advances in Obesity: Understanding Obesity—From Its Origins to Impact on Life; Monteiro, R., Martins, M., Eds.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2020. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, A.R.; Oliveira, A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients 2021, 13, 3447. https://doi.org/10.3390/nu13103447
Pereira AR, Oliveira A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients. 2021; 13(10):3447. https://doi.org/10.3390/nu13103447
Chicago/Turabian StylePereira, Ana Rita, and Andreia Oliveira. 2021. "Dietary Interventions to Prevent Childhood Obesity: A Literature Review" Nutrients 13, no. 10: 3447. https://doi.org/10.3390/nu13103447
APA StylePereira, A. R., & Oliveira, A. (2021). Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients, 13(10), 3447. https://doi.org/10.3390/nu13103447