
Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
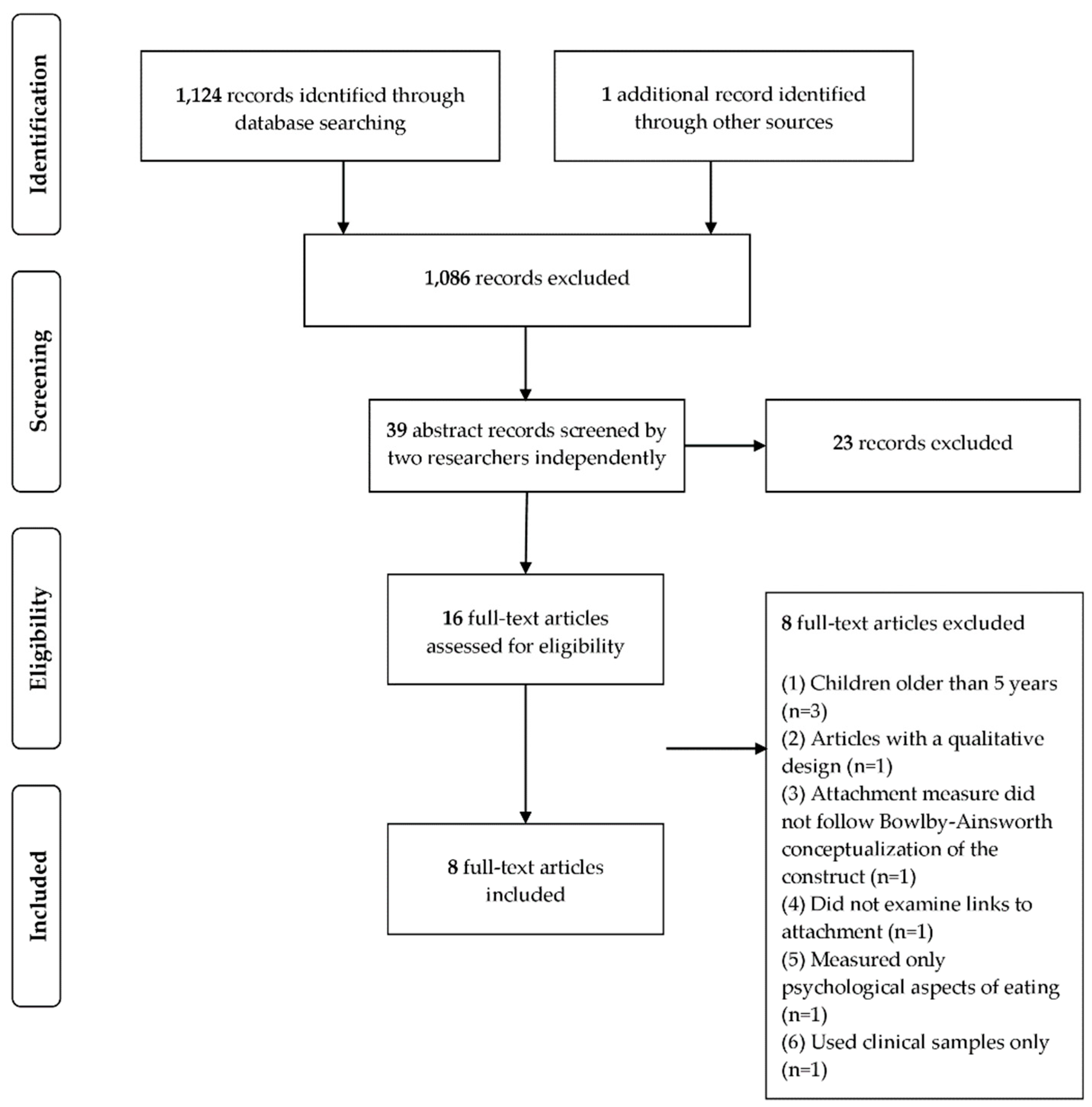
2.3. Study Selection
2.4. Data Extraction
3. Results
3.1. Studies Characteristics
3.2. Overview of Key Findings on the Relationship between Caregiver Attachment and Obesity
3.3. Overview of Key Findings on the Relationship between Caregiver–Child Attachment and Obesity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Regional Office for Europe. Mapping the Health System Response to Childhood Obesity in the WHO European Region: An Overview and Country Perspectives; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019; Available online: http://www.euro.who.int/__data/assets/pdf_file/0019/401176/Childhood-obesity-web.pdf?ua=1 (accessed on 1 July 2021).
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 July 2021).
- Puhl, R.M.; Latner, J.D. Stigma, obesity, and the health of the nation’s children. Psychol. Bull. 2007, 133, 557–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.C.; Lawlor, D.A.; Kimm, S.Y.S. Childhood obesity. Lancet 2010, 375, 1737–1748. [Google Scholar] [CrossRef]
- Kumar, S.; Kelly, S.A. Review of Childhood Obesity. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [Green Version]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Bennett, P.H.; Looker, H.C. Childhood obesity, other cardiovascular risk factors, and premature death. N. Engl. J. Med. 2010, 362, 485–493. [Google Scholar] [CrossRef]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2010, 35, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Sonntag, D. Why early prevention of childhood obesity is more than a medical concern: A health economic approach. Ann. Nutr. Metab. 2017, 70, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, D.; Dee, A.; Perry, I.J. The lifetime costs of overweight and obesity in childhood and adolescence: A systematic review. Obes. Rev. 2018, 19, 452–463. [Google Scholar] [CrossRef]
- McCarthy, A.; Hughes, R.; Tilling, K.; Davies, D.; Smith, G.D.; Ben-Shlomo, Y. Birth weight; postnatal, infant, and childhood growth; and obesity in young adulthood: Evidence from the Barry Caerphilly Growth Study. Am. J. Clin. Nutr. 2007, 86, 907–913. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Taking Action on Childhood Obesity; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/274792/WHO-NMH-PND-ECHO-18.1-eng.pdf (accessed on 1 July 2021).
- Peirson, L.; Fitzpatrick-Lewis, D.; Morrison, K.; Warren, R.; Usman Ali, M.; Raina, P. Treatment of overweight and obesity in children and youth: A systematic review and meta-analysis. CMAJ Open 2015, 3, E35–E46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and management of childhood obesity and its psychological and health comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, H.H.; Neale, M.C.; Eaves, L.J. Genetic and environmental factors in relative body weight and human adiposity. Behav. Genet. 1997, 27, 325–351. [Google Scholar] [CrossRef]
- Farooqi, I.S.; O’Reilly, S. Genetic factors in human obesity. Obes. Rev. 2007, 8, 37–40. [Google Scholar] [CrossRef]
- da Silveira, J.A.C.; Taddei, J.A.A.C.; Guerra, P.H.; Nobre, M.R.C. The effect of participation in school-based nutrition education interventions on body mass index: A meta-analysis of randomized controlled community trials. Prev. Med. 2013, 56, 237–243. [Google Scholar] [CrossRef]
- Brown, E.C.; Buchan, D.S.; Cavana, J.; Baker, J.S.; Wyatt, F.B.; Kilgore, J.L. Fit for school: Results of a 10-week school-based child healthy weight pilot intervention for primary school students. Int. J. Health Promot. Educ. 2016, 54, 229–244. [Google Scholar] [CrossRef]
- Liu, J.; Hay, J.; Faught, B.E.; Wade, T.; Cairney, J.; Merchant, A.T.; Trevisan, M. Family eating and activity habits, diet quality and pre-adolescent overweight and obesity. Public Health 2012, 126, 532–534. [Google Scholar] [CrossRef]
- Lee, H. The role of local food availability in explaining obesity risk among young school-aged children. Soc. Sci. Med. 2012, 74, 1193–1203. [Google Scholar] [CrossRef]
- Demerath, E.W.; Choh, A.C.; Czerwinski, S.A.; Lee, M.; Sun, S.S.; Chumlea, W.C.; Duren, D.; Richard, J.S.; Blangero, J.; Towne, B.; et al. Genetic and environmental influences on infant weight & weight change: The Fels longitudinal study. Am. J. Hum. Biol. 2007, 19, 692–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruijt-Metz, D. Etiology, treatment, and prevention of obesity in childhood and adolescence: A decade in review. J. Res. Adolesc. 2011, 21, 129–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: Implications for prevention. Int. J. Obes. 2010, 34, 1116–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midei, A.J.; Matthews, K.A. Social relationships and negative emotional traits are associated with central adiposity and arterial stiffness in healthy adolescents. Health Psychol. 2009, 28, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Anderson, S.E.; Whitaker, R.C. Attachment security and obesity in US preschool-aged children. Arch. Pediatr. Adolesc. Med. Proc. 2011, 165, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Anderson, S.E.; Gooze, R.A.; Lemeshow, S.; Whitaker, R.C. Quality of early maternal–child relationship and risk of adolescent obesity. Pediatrics 2012, 129, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, L.; Braet, C.; van Durme, K.; Decaluwé, V.; Bosmans, G. The parent-child relationship as predictor of eating pathology and weight gain in preadolescents. J. Clin. Child. Adolesc. Psychol. 2012, 41, 445–457. [Google Scholar] [CrossRef]
- Bahrami, F.; Kelishadi, R.; Jafari, N.; Kaveh, Z.; Isanejad, O. Association of children’s obesity with the quality of parental-child attachment and psychological variables. Acta Paediatr. 2013, 102, e321–e324. [Google Scholar] [CrossRef]
- Bost, K.K.; Wiley, A.R.; Fiese, B.; Hammons, A.; McBride, B.; SRONG KIDS Team. Associations between adult attachment style, emotion regulation, and preschool children’s food consumption. J. Dev. Behav. Pediatr. 2014, 35, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Keitel-Korndörfer, A.; Sierau, S.; Klein, A.M.; Bergmann, S.; Grube, M.; von Klitzing, K. Insatiable insecurity: Maternal obesity as a risk factor for mother–child attachment and child weight. Attach. Hum. Dev. 2015, 17, 399–413. [Google Scholar] [CrossRef] [PubMed]
- Diener, M.J.; Geenen, R.; Koelen, J.A.; Aarts, F.; Gerdes, V.E.A.; Brandjes, D.P.M.; Hinnen, C. The significance of attachment quality for obesity: A meta-analytic review. Can. J. Behav. Sci. 2016, 48, 255–265. [Google Scholar] [CrossRef]
- Roemmich, J.N.; Smith, J.R.; Epstein, L.H.; Lambiase, M. Stress reactivity and adiposity of youth. Obesity 2007, 15, 2303–2310. [Google Scholar] [CrossRef]
- De Vriendt, T.; Moreno, L.A.; De Henauw, S. Chronic stress and obesity in adolescents: Scientific evidence and methodological issues for epidemiological research. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 511–519. [Google Scholar] [CrossRef]
- Dallman, M.F. Stress-induced obesity and the emotional nervous system. Trends Endocrinol. Metab. 2010, 21, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Ganley, R.M. Emotion and eating in obesity: A review of the literature. Int. J. Eat. Disord. 1989, 8, 343–361. [Google Scholar] [CrossRef]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef]
- Braet, C.; Van Strien, T. Assessment of emotional, externally induced and restrained eating behaviour in nine to twelve-year-old obese and non-obese children. Behav. Res. Ther. 1997, 35, 863–873. [Google Scholar] [CrossRef]
- Nguyen-Michel, S.T.; Unger, J.B.; Spruijt-Metz, D. Dietary correlates of emotional eating in adolescence. Appetite 2007, 49, 494–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowlby, J. Attachment and Loss: Attachment, 2nd ed.; Original Work Published 1969; Basic Books: New York, NY, USA, 1982; Volume 1. [Google Scholar]
- Warren, S.L.; Bost, K.K.; Roisman, G.I.; Silton, R.L.; Spielberg, J.M.; Engels, A.S.; Choi, E.; Sutton, B.P.; Miller, G.A.; Heller, W. Effects of adult attachment and emotional distractors on brain mechanisms of cognitive control. Psychol. Sci. 2010, 21, 1818–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, M.D.S. Attachments beyond infancy. Am. Psychol. 1989, 44, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; Cummings, E.M. A secure base from which to explore close relationships. Child Dev. 2000, 71, 164–172. [Google Scholar] [CrossRef]
- Bretherton, I. Fathers in attachment theory and research: A review. Early Child Dev. Care 2010, 180, 9–23. [Google Scholar] [CrossRef]
- Kerns, K.A.; Mathews, B.L.; Koehn, A.J.; Williams, C.T.; Siener-Ciesla, S. Assessing both safe haven and secure base support in parent–child relationships. Attach. Hum. Dev. 2015, 17, 337–353. [Google Scholar] [CrossRef]
- Main, M.; Kaplan, N.; Cassidy, J. Security in infancy, childhood, and adulthood: A move to the level of representation. Monogr. Soc. Res. Child Dev. 1985, 50, 66. [Google Scholar] [CrossRef]
- Waters, H.S.; Waters, E. The attachment working models concept: Among other things, we build script-like representations of secure base experiences. Attach. Hum. Dev. 2006, 8, 185–197. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and Loss: Separation, Anxiety, and Anger; Basic Books: New York, NY, USA, 1973; Volume 2. [Google Scholar]
- Bowlby, J. The Making and Breaking of Affectional Bonds; Tavistock: London, UK, 1979. [Google Scholar]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S. Patterns of Attachment: A Psychological Study of the Strange Situation; Erlbaum: Hillsdale, NJ, USA, 1978. [Google Scholar]
- Bretherton, I. The origins of attachment theory: John Bowlby and Mary Ainsworth. Dev. Psychol. 1992, 28, 759–775. [Google Scholar] [CrossRef]
- van IJzendoorn, M.H. Adult attachment representations, parental responsiveness, and infant attachment: A meta-analysis on the predictive validity of the Adult Attachment Interview. Psychol. Bull. 1995, 117, 387–403. [Google Scholar] [CrossRef] [PubMed]
- Roque, L.; Veríssimo, M.; Fernandes, M.; Rebelo, A. Emotion regulation and attachment: Relationships with children’s secure base, during different situational and social contexts in naturalistic settings. Infant Behav. Dev. 2013, 36, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Brumariu, L.E. Parent-child attachment and emotion regulation. New Dir. Child Adolesc. Dev. 2015, 2015, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Faber, A.; Dubé, L.; Knäuper, B. Attachment and eating: A meta-analytic review of the relevance of attachment for unhealthy and healthy eating behaviors in the general population. Appetite 2018, 123, 410–438. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J. Emotion regulation: Influences of attachment relationships. Monogr. Soc. Res. Child Dev. 1994, 59, 228–249. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Sapir-Lavid, Y.; Avihou-Kanza, N. What’s inside the minds of securely and insecurely attached people? The secure-base script and its associations with attachment-style dimensions. J. Pers. Soc. Psychol. 2009, 97, 615–633. [Google Scholar] [CrossRef] [Green Version]
- Bowlby, J. Developmental psychiatry comes of age. Am. J. Psychiatry 1988, 145, 1–10. [Google Scholar] [CrossRef]
- Bretherton, I. Open communication and internal working models: Their role in the development of attachment relationships. In Nebraska Symposium on Motivation, 1988: Socioemotional Development; Thompson, R.A., Ed.; University of Nebraska Press: Lincoln, NE, USA, 1990; pp. 57–113. [Google Scholar]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef]
- Blumenthal, D.M.; Gold, M.S. Neurobiology of food addiction. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 359–365. [Google Scholar] [CrossRef]
- Pecoraro, N.; Reyes, F.; Gomez, F.; Bhargava, A.; Dallman, M.F. Chronic stress promotes palatable feeding, which reduces signs of stress: Feedforward and feedback effects of chronic stress. Endocrinology 2004, 145, 3754–3762. [Google Scholar] [CrossRef]
- Onaka, T.; Takayanagi, Y.; Yoshida, M. Roles of oxytocin neurones in the control of stress, energy metabolism, and social behaviour. J. Neuroendocrinol. 2012, 24, 587–598. [Google Scholar] [CrossRef]
- Haedt-Matt, A.A.; Keel, P.K. Revisiting the affect regulation model of binge eating: A meta-analysis of studies using ecological momentary assessment. Psychol. Bull. 2011, 137, 660–681. [Google Scholar] [CrossRef] [Green Version]
- Sroufe, L.A.; Waters, E. Attachment as an organizational construct. Child Dev. 1977, 48, 1184–1199. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion regulation: A theme in search of definition. Monogr. Soc. Res. Child Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef] [PubMed]
- Frankel, L.A.; Hughes, S.O.; O’Connor, T.M.; Power, T.G.; Fisher, J.O.; Hazen, N.L. Parental influences on children’s self-regulation of energy intake: Insights from developmental literature on emotion regulation. J. Obes. 2012, 2012, 327259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, N.; Fabes, R.A.; Murphy, B.C. Parents’ reactions to children’s negative emotions: Relations to children’s social competence and comforting behavior. Child Dev. 1996, 67, 2227–2247. [Google Scholar] [CrossRef]
- Mikulincer, M.; Orbach, I. Attachment styles and repressive defensiveness: The accessibility and architecture of affective memories. J. Pers. Soc. Psychol. 1995, 68, 917–925. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Pereg, D. Attachment theory and affect regulation: The dynamics, development, and cognitive consequences of attachment-related strategies. Motiv. Emot. 2003, 27, 77–102. [Google Scholar] [CrossRef]
- Monteiro, L.; Veríssimo, M.; Vaughn, B.E.; Santos, A.J.; Bost, K.K. Secure base representations for both fathers and mothers predict children’s secure base behavior in a sample of Portuguese families. Attach. Hum. Dev. 2008, 10, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Mazzeschi, C.; Pazzagli, C.; Laghezza, L.; Radi, G.; Battistini, D.; De Feo, P. The role of both parents’ attachment pattern in understanding childhood obesity. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenhammar, C.; Olsson, G.; Bahmanyar, S.; Hulting, A.-L.; Wettergren, B.; Edlund, B.; Montgomery, S. Family stress and BMI in young children. Acta Paediatr. 2010, 99, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Cole, P.M.; Hall, S.E. Emotion dysregulation as a risk factor for psychopathology. In Child and Adolescent Psychopathology; Beauchaine, T.P., Hinshaw, S.P., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2008; pp. 265–298. [Google Scholar]
- Sala, M.N.; Pons, F.; Molina, P. Emotion regulation strategies in preschool children. Br. J. Dev. Psychol. 2014, 32, 440–453. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- de Campora, G.; Giromini, L.; Guerriero, V.; Chiodo, C.; Zavattini, G.C.; Larciprete, G. Influence of maternal reflective functioning on mothers’ and children’s weight: A follow-up study. Infant Ment. Health J. 2019, 40, 862–873. [Google Scholar] [CrossRef]
- Hepworth, A.D.; Berlin, L.J.; Martoccio, T.L.; Harden, B.J. Maternal attachment style, sensitivity, and infant obesity risk in low-income, Latino families. Attach. Hum. Dev. 2021, 23, 75–89. [Google Scholar] [CrossRef]
- Keitel-Korndörfer, A.; Bergmann, S.; Nolte, T.; Wendt, V.; von Klitzing, K.; Klein, A.M. Maternal mentalization affects—but not children’s—weight via emotional eating. Attach. Hum. Dev. 2016, 18, 487–507. [Google Scholar] [CrossRef]
- Fonagy, P.; Target, M.; Steele, H.; Steele, M. Reflective-Functioning Manual: Version 5.0 for Application to Adult Attachment Interviews; University College London: London, UK, 1998. [Google Scholar]
- George, C.; Kaplan, N.; Main, M. Adult Attachment Interview (AAI); Unpublished Manuscript; University of California: Berkeley, CA, USA, 1985. [Google Scholar]
- Hazan, C.; Shaver, P. Romantic love conceptualized as an attachment process. J. Pers. Soc. Psychol. 1987, 52, 511–524. [Google Scholar] [CrossRef]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Self-report measures of adult attachment: An integrative overview. In Attachment Theory and Close Relationships; Simpson, J.A., Rholes, W.S., Eds.; Guilford Press: New York, NY, USA, 1998; pp. 46–76. [Google Scholar]
- Waters, E. Appendix A: Attachment Q-set (version 3.0). Monogr. Soc. Res. Child Dev. 1995, 60, 234–246. [Google Scholar] [CrossRef]
- Andreassen, C.; West, J. Measuring socioemotional functioning in a national birth cohort study. Infant Ment. Health J. 2007, 28, 627–646. [Google Scholar] [CrossRef] [PubMed]
- Najarian, M.; Snow, K.; Lennon, J.; Kinsey, S. Early Childhood Longitudinal Study, Birth Cohort (ECLS-B), Preschool–Kindergarten 2007 Psychometric Report (NCES 2010-009); National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education: Washington, DC, USA, 2010. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Jonhson, C.L. CDC growth charts: United States. Adv. Data 2000, 8, 1–27. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Brophy, S.; Cooksey, R.; Gravenor, M.B.; Mistry, R.; Thomas, N.; Lyons, R.A.; Williams, R. Risk factors for childhood obesity at age 5: Analysis of the Millennium Cohort Study. BMC Public Health 2009, 9, 467. [Google Scholar] [CrossRef] [Green Version]
- Janjua, N.Z.; Mahmood, B.; Islam, M.A.; Goldenberg, R.L. Maternal and early childhood risk factors for overweight and obesity among low-income predominantly black children at age five years: A prospective cohort study. J. Obes. 2012, 2012, 457173. [Google Scholar] [CrossRef]
- Williams, A.S.; Ge, B.; Petroski, G.; Kruse, R.L.; McElroy, J.A.; Koopman, R.J. Socioeconomic status and other factors associated with childhood obesity. J. Am. Board Fam. Med. 2018, 31, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cartwright, M.; Wardle, J.; Steggles, N.; Simon, A.E.; Croker, H.; Jarvis, M.J. Stress and dietary practices in adolescents. Health Psychol. 2003, 22, 362–369. [Google Scholar] [CrossRef]
- Faber, A.; Dubé, L. Parental attachment insecurity predicts child and adult high-caloric food consumption. J. Health Psychol. 2015, 20, 511–524. [Google Scholar] [CrossRef]
- Saltzman, J.A.; Liechty, J.M.; Bost, K.K.; Fiese, B.H.; SRONG KIDS Team. Parent binge eating and restrictive feeding practices: Indirect effects of parent’s responses to child’s negative emotion. Eat. Behav. 2016, 21, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saltzman, J.A.; Pineros-Leano, M.; Liechty, J.M.; Bost, K.K.; Fiese, B.H.; SRONG KIDS Team. Eating, feeding, and feeling: Emotional responsiveness mediates longitudinal associations between maternal binge eating, feeding practices, and child weight. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, C.; Santos, A.F.; Fernandes, M.; Santos, A.J.; Bost, K.; Veríssimo, M. Caregivers’ perceived emotional and feeding responsiveness toward preschool children: Associations and paths of influence. Nutrients 2021, 13, 1334. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Stifter, C.A.; Birch, L.L. Temperament and childhood obesity risk: A review of the literature. J. Dev. Behav. Pediatr. 2012, 33, 732–745. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.E.; Keim, S.A. Parent–child interaction, self-regulation, and obesity prevention in early childhood. Curr. Obes. Rep. 2016, 5, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Fiese, B.H.; Bost, K.K. Family ecologies and child risk for obesity: Focus on regulatory processes. Fam. Relat. 2016, 65, 94–107. [Google Scholar] [CrossRef]
- Saltzman, J.A.; Fiese, B.H.; Bost, K.K.; McBride, B.A. Development of appetite self-regulation: Integrating perspectives from attachment and family systems theory. Child Dev. Perspect. 2018, 12, 51–57. [Google Scholar] [CrossRef]
- Bergmeier, H.; Paxton, S.J.; Milgrom, J.; Anderson, S.E.; Baur, L.; Hill, B.; Lim, S.; Green, R.; Skouteris, H. Early mother-child dyadic pathways to childhood obesity risk: A conceptual model. Appetite 2020, 144, 104459. [Google Scholar] [CrossRef]
- McMeekin, S.; Jansen, E.; Mallan, K.; Nicholson, J.; Magarey, A.; Daniels, L. Associations between infant temperament and early feeding practices. A cross-sectional study of Australian mother-infant dyads from the NOURISH randomised controlled trial. Appetite 2013, 60, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, L.; Veríssimo, M.; Vaughn, B.E.; Santos, A.J.; Torres, N.; Fernandes, M. The organization of children’s secure base behaviour in two-parent Portuguese families and father’s participation in child-related activities. Eur. J. Dev. Psychol. 2010, 7, 545–560. [Google Scholar] [CrossRef]
- Veríssimo, M.; Santos, A.J.; Vaughn, B.E.; Torres, N.; Monteiro, L.; Santos, O. Quality of attachment to father and mother and number of reciprocal friends. Early Child Dev. Care 2011, 181, 27–38. [Google Scholar] [CrossRef]
- Fernandes, C.; Fernandes, M.; Santos, A.J.; Antunes, M.; Monteiro, L.; Vaughn, B.E.; Veríssimo, M. Early attachment to mothers and fathers: Contributions to preschoolers’ emotional regulation. Front. Psychol. 2021, 12, 660866. [Google Scholar] [CrossRef]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stang, A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A.E.; Cook, N.R.; Gillman, M.W. Weight status in childhood as a predictor of becoming overweight or hypertensive in early adulthood. Obes. Res. 2005, 13, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors (Year) Country | Sample Characteristics | Study Design | Attachment Measures | Weight Status or Food Consumption Measures |
|---|---|---|---|---|
| Anderson and Whitaker (2011) (US) [24] | 6650 children (female = 48.7%; male = 51.3%) and mothers | Longitudinal cohort | Toddler Attachment Sort-45 (assessed at 24 months) | BMI percentiles (assessed at 41⁄2 years) |
| Children’s age range = 24.3 to 54.3 months | ||||
| Mothers’ age = ≥35 (17.5%), >30–35 (25.6%), >25–30 (25.7%), >20–25 (23.8%), 15–20 (7.3%) | ||||
| Children’s race/ethnicity: White (55.9%), Black (15.4%), Hispanic (22.6%), other race (6.1%) | ||||
| Maternal educational level: college graduate (26.4%), some college (26.7%), high school degree (28.9%), less than high school degree (18%) | ||||
| Families’ income (income to poverty ratio): >3.00 (25.7%), 1.86–3.00 (28.1%), 1.00–1.85 (23.5%), 0.50–0.99 (12.7%), <0.50 (10%) | ||||
| Caregivers’ marital status/living arrangements: living together (79.1%), separated (20.9%) | ||||
| Anderson et al. (2012) (US) [25] | 977 children (female = 50.4%; male = 49.6%) and mothers | Longitudinal cohort | Strange Situation (assessed at 15 and 36 months) Attachment Q-set (assessed at 24 months) | BMI percentiles (assessed at 15 or 12 years) |
| Children’s age range = 15 to 36 months | ||||
| Mothers’s race/ethnicity: White (80.7%), nonwhite (19.3%) | ||||
| Maternal educational level: graduate degree (15.7%), bachelor degree (22.4%), some college or associate degree (33.2%), high school degree (20.6%), less than high school degree (8.2%) | ||||
| Families’ income (income to poverty ratio): ≥5.00 (23.2%), 3.00–4.99 (28.1%), 1.86–2.99 (22%), 1.00–1.85 (14.9%), <1.00 (11.9%) | ||||
| Bost et al. (2014) (US) [28] | 497 caregivers (female = 90%; male = 10%) of children | Cross- sectional | Relationship Questionnaire | Early Childhood Longitudinal Study-B parent interview child health section |
| Children’s age range = 2.5 to 3.5 years | ||||
| Caregivers’ age mean = 32.5 years | ||||
| Caregivers’ race/ethnicity: White (78%), African-American (18.2%), Asian (8%), Latino (3.8%) | ||||
| Caregivers’ educational level: postgraduate degree (27.9%), college degree (26.3%), some college or technical training (32.1%), high school degree or less (11%) | ||||
| Families’ income (annual household income): <40,000 (47.8%), <24,000 (29%) | ||||
| de Campora et al. (2019) (IT) [76] | 51 mothers of children (female = 43.4%; male = 56.6%) | Longitudinal birth cohort | Reflective Functioning Scale of the Adult Attachment Interview (assessed during pregnancy) | BMI (assessed at 3 years) |
| Children’s age range = birth to 3 years | ||||
| Mothers’ age mean = 34.8 years | ||||
| Maternal educational level: bachelor degree or more (43.1%), high school degree or less (56.9%) | ||||
| Hepworth et al. (2021) (US) [77] | 55 mothers of children (female = 46%; male = 54%) | Cross- sectional | Adult Attachment Scale Experiences in Close Relationships Scale | Weight-for-length Z-scores |
| Children’s age mean = 12.7 months | ||||
| Mothers’ age mean = 30.9 years | ||||
| Mothers’ race/ethnicity: Latino (95%) | ||||
| Maternal educational level: high school degree (51%), less than high school degree (49%) | ||||
| Maternal professional situation: employed (53%), unemployed (47%) | ||||
| Families’ income (status): low | ||||
| Maternal marital status/living arrangements: married or cohabitating (82%) | ||||
| Keitel-Korndörfer et al. (2015) (DE) [29] | 62 children (female = 56%; male = 44%) and mothers (normal-weight = 50%; obese = 50%) | Cross- sectional | Attachment Q-Set | BMI percentiles |
| Children’s age range = 19 to 58 months | ||||
| Mothers’ age range = 22.8 to 44.0 years | ||||
| Maternal educational level: high school degree (normal-weight = 57%; obese = 48%), less than high school degree (normal-weight = 43%; obese = 52%) | ||||
| Maternal marital status/living arrangements: in a relationship with the father (normal-weight = 81%; obese = 71%), not in relationship (normal-weight = 19%; obese = 29%) | ||||
| Keitel-Korndörfer et al. (2016) (DE) [78] | 60 children (female = 55%; male = 45%) and mothers (normal-weight = 50%; obese = 50%) | Cross- sectional | Reflective Functioning Scale of the Adult Attachment Interview Attachment Q-Set | BMI percentiles |
| Children’s age range = 18 to 55 months | ||||
| Mothers’ age mean = 31.7 years | ||||
| Maternal educational level: high school degree (normal-weight = 55%; obese = 50%), less than high school degree (normal-weight = 45%; obese = 50%) | ||||
| Maternal marital status/living arrangements: in a relationship with the father (normal-weight = 80%; obese = 70%), not in relationship (normal-weight = 20%; obese = 30%) | ||||
| Stenhammar et al. (2010) (SE) [72] | 873 children and caregivers (mothers = 865; fathers = 746) | Cross- sectional | Relationship Questionnaire | BMI percentiles |
| Children’s age = 3 years | ||||
| Caregivers’ educational level: college degree (48.2%), some college (2.8%), high school degree (42.8%), less than high school degree (6.2%) | ||||
| Caregivers’ professional situation: employed (77%), parental leave (11%), student (7%), unemployed (5%) | ||||
| Caregivers’ marital status/living arrangements: living together (92.9%), separated (7.1%) |
| Authors (Year) Country | Key Findings | Covariates |
|---|---|---|
| Bost et al. (2014) (US) [28] | Caregivers’ insecure attachment was associated with children’s unhealthy food consumption indirectly through unsupportive responses (punishing or dismissing responses) to children’s distress. These unsupportive responses predicted the increased use of emotion-related and pressuring feeding styles. | Controlled for children’s and caregivers’ age, children’s gender, caregivers’ BMI, race/ethnicity, education level, depression, and anxiety. |
| de Campora et al. (2019) (IT) [76] | Maternal mentalization was only marginally significantly associated with children’s BMI. Multiple regression models suggest that maternal mentalization might explain the variance of children’s BMI beyond the effects of maternal emotional dysregulation. | No information available. |
| Hepworth et al. (2021) (US) [77] | Mother’s insecure attachment style, according to the AAS, was associated with children’s higher weight-for-length Z-scores. This association was not mediated by maternal sensitivity. Mother’s attachment avoidance and attachment anxiety, according to the ECR, did not predicted children’s weight-for-length Z-scores. | Controlled for children’s age at baseline, children’s gender, maternal BMI, family cumulative risk, and randomized controlled trial (RCT) group. |
| Keitel-Korndörfer et al. (2016) (DE) [78] | Lower maternal mentalization was associated with children’s higher BMI percentiles indirectly through a lower quality of mother–child attachment. | Controlled for maternal intelligence quotient (IQ) and maternal depression. |
| Stenhammar et al. (2010) (SE) [72] | Caregivers’ insecure attachment was associated with overweight in children. This association was not independent of maternal stress. Maternal stress was associated with overweight and underweight in children. | Controlled for children’s and caregivers’ gender, children’s number of older and younger siblings, mothers’ self-perceived weight, caregivers’ age, education level, professional situation, and living arrangements. |
| Authors (Year) Country | Key Findings | Covariates |
|---|---|---|
| Anderson and Whitaker (2011) (US) [24] | The odds for obesity at 41⁄2 years of age were 1.30 times higher for children with an insecure mother–child attachment than for children with a secure mother–child attachment measured at 24 months. | Controlled for children’s and mothers’ age, children’s gender, children’s birth weight, maternal BMI, race/ethnicity, education level, income to poverty ratio, the quality of mother–child interaction during play (maternal responsiveness, child engagement, and child negativity), and parenting practices related to obesity (television/video/DVD viewing and the frequency of eating family dinners). |
| Anderson et al. (2012) (US) [25] | Insecure mother–child attachment at 24 months of age (according to the AQS) was associated with increased odds for adolescent obesity, but not at 15 and 36 months (according to the SSP). The odds for adolescent obesity were 2.45 times higher for children with an insecure mother–child attachment than for children with a secure mother–child attachment. | Controlled for children’s age, children’s birth weight, maternal BMI, race/ethnicity, education level, and income to poverty ratio. |
| Keitel-Korndörfer et al. (2015) (DE) [29] | Insecure mother–child attachment was associated with children’s higher BMI percentiles. | Controlled for children’s BMI birth percentile, caregivers’ BMI, and maternal marital status. |
| Keitel-Korndörfer et al. (2016) (DE) [78] | Lower maternal mentalization was associated with children’s higher BMI percentile indirectly through a lower quality of mother–child attachment. | Controlled for maternal intelligence quotient (IQ) and maternal depression. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, A.F.; Martins, M.C.; Fernandes, C.; Bost, K.K.; Veríssimo, M. Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature. Nutrients 2021, 13, 3572. https://doi.org/10.3390/nu13103572
Santos AF, Martins MC, Fernandes C, Bost KK, Veríssimo M. Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature. Nutrients. 2021; 13(10):3572. https://doi.org/10.3390/nu13103572
Chicago/Turabian StyleSantos, Ana F., Mariana C. Martins, Carla Fernandes, Kelly K. Bost, and Manuela Veríssimo. 2021. "Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature" Nutrients 13, no. 10: 3572. https://doi.org/10.3390/nu13103572
APA StyleSantos, A. F., Martins, M. C., Fernandes, C., Bost, K. K., & Veríssimo, M. (2021). Relation between Attachment and Obesity in Preschool Years: A Systematic Review of the Literature. Nutrients, 13(10), 3572. https://doi.org/10.3390/nu13103572