
Diet and Lifestyle Factors and Risk of Atherosclerotic Cardiovascular Disease—A Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
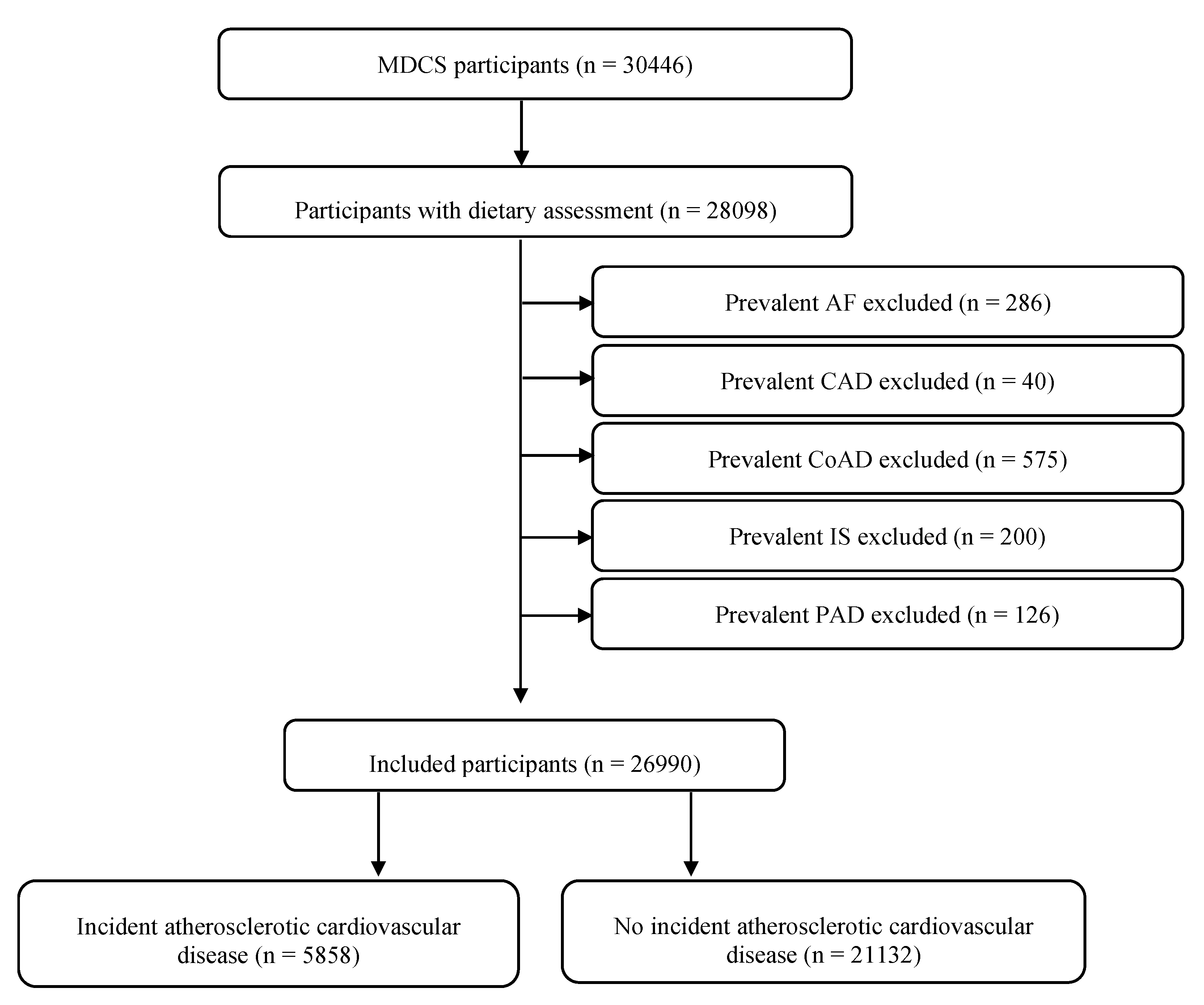
2.1. Study Population and Data Collection
2.2. Diet Assessment Method and Diet Quality Components
2.3. Lifestyle and Other Variables
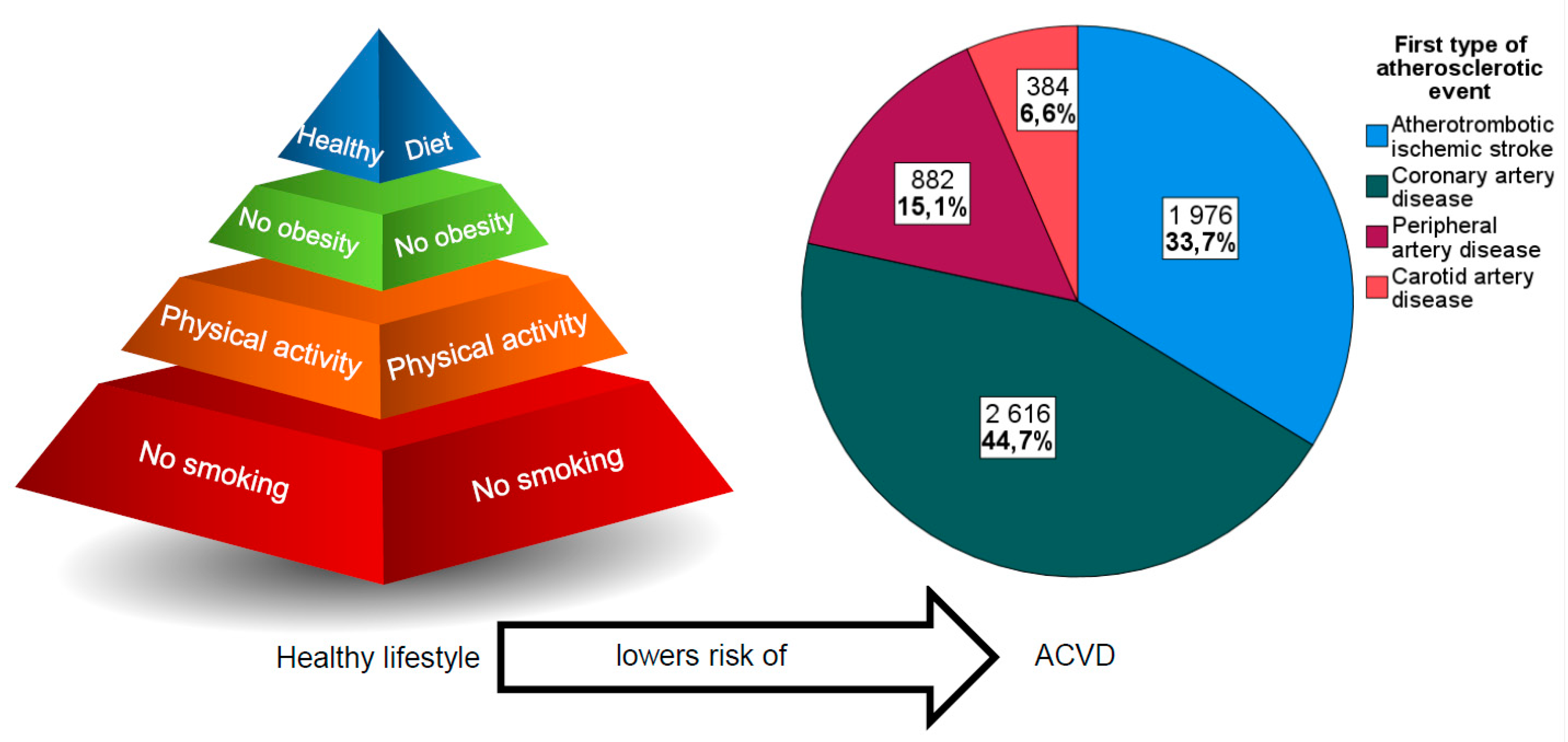
2.4. Endpoint Ascertainment
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Diet Quality Index Components and Atherosclerotic Disease Risk
3.3. Other Lifestyle Factors and Atherosclerotic Disease Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics-2021 update: A report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Mannsverk, J.; Wilsgaard, T.; Mathiesen, E.B.; Løchen, M.L.; Rasmussen, K.; Thelle, D.S.; Njølstad, I.; Hopstock, L.A.; Bønaa, K.H. Trends in Modifiable Risk Factors Are Associated with Declining Incidence of Hospitalized and Nonhospitalized Acute Coronary Heart Disease in a Population. Circulation 2016, 133, 74–81. [Google Scholar] [CrossRef]
- Khera, A.M.; Emdin, C.A.; Drake, I.; Natarajan, P.; Bick, A.G.; Cook, N.R.; Boerwinkle, E.; Mehran, R.; Baber, U.; Fuster, V.; et al. Genetic risk, adherence to a healthy life style, and coronary disease. N. Engl. J. Med. 2016, 375, 2349–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimovski, K.; Orho-Melander, M.; Drake, I. A favorable lifestyle lowers the risk of coronary artery disease consistently across strata of non-modifiable risk factors in a population-based cohort. BMC Public Health 2019, 19, 1575. [Google Scholar] [CrossRef] [PubMed]
- Hlebowicz, J.; Drake, I.; Gullberg, B.; Sonestedt, E.; Wallström, P.; Persson, M.; Nilsson, J.; Hedblad, B.; Wirfält, E. A high diet quality is associated with lower incidence of cardiovascular events in the Malmö diet and cancer cohort. PLoS ONE 2013, 8, e71095. [Google Scholar] [CrossRef]
- Kulezic, A.; Bergwall, S.; Fatemi, S.; Sonestedt, E.; Zarrouk, M.; Gottsäter, A.; Acosta, S. Healthy diet and fiber intake are associated with decreased risk of incident symptomatic peripheral artery disease–A prospective cohort study. Vasc. Med. 2019, 24, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Acosta, S. Diet and lifestyle as risk factors for carotid artery disease: A prospective cohort study. Cereb. Dis. 2020, 49, 563–569. [Google Scholar] [CrossRef]
- Johansson, A.; Drake, I.; Engström, G.; Acosta, S. Modifiable and non-modifiable risk factors for atherothrombotic ischemic stroke among subjects in the Malmö Diet and Cancer Study. Nutrients 2021, 13, 1952. [Google Scholar] [CrossRef]
- Malmö Kost Cancer och Malmö Förebyggande Medicin. Lund: Lund University; updated 11 November 2019; cited 18 May 2020. Available online: https://www.malmo-kohorter.lu.se/malmo-kost-cancer-mkc (accessed on 1 October 2021).
- Tetens, I.; Pedersen, A.N.; Schwab, U.; Fogelholm, M.; Thorsdottir, I.; Gunnarsdottir, I.; Anderssen, S.; Möltzer, H.; Becker, W.; Hursti, U.-K.; et al. Nordic Nutrition Recommendations; Report; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Drake, I.; Gullberg, B.; Ericson, U.; Sonestedt, E.; Nilsson, J.; Wallstrom, P.; Hedblad, B.; Wirfält, E. Development of a diet quality index assessing adherence to the Swedish nutrition recommendations and dietary guidelines in the Malmo Diet and Cancer cohort. Public Health Nutr. 2011, 14, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.L.; Jacobs, D.R., Jr.; Schucher, B.; Knudsen, J.; Leon, A.S.; Debacher, G. A questionnaire for the assessment of leisure time physical activities. J. Chron. Dis. 1978, 31, 741–755. [Google Scholar] [CrossRef]
- Tran, H.; Anand, S.S. Oral antiplatelet therapy in cerebrovascular disease, coronary artery disease and peripheral arterial disease. JAMA 2004, 292, 1867–1874. [Google Scholar] [CrossRef] [Green Version]
- Lechner, K.; von Schacky, C.; McKenzie, A.L.; Worm, N.; Nixdorff, U.; Lechner, B.; Kränkel, N.; Halle, M.; Krauss, R.M.; Scherr, J. Lifestyle factors and high-risk atherosclerosis: Pathways and mechanisms beyond traditional risk factors. Eur. J. Prev. Cardiol. 2020, 27, 394–406. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.H.Y.; Micha, R.; Mozaffarian, D. Dietary fats and cardiometabolic disease: Mechanisms and effects on risk factors and outcomes. Nat. Rev. Cardiol. 2019, 16, 581–601. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Matttioli, A.V.; Palmiero, P.; Manfrini, O.; Puddu, P.E.; Nodari, S.; Dei Cas, A.; Ciccone, M.M.; Sucato, V.; Triggiani, M.; Cugusi, L.; et al. Mediterranean diet impact on cardiovascular diseases: A narrative review. J. Cardiovasc. Med. 2017, 18, 925–935. [Google Scholar] [CrossRef]
- Lamantia, V.; Sniderman, A.; Faraj, M. Nutritional management of hyperapoB. Nutr. Res. Rev. 2016, 29, 202–233. [Google Scholar] [CrossRef]
- Lilja, E.; Bergwall, S.; Sonestedt, E.; Gottsäter, A.; Acosta, S. The association between dietary intake, lifestyle and incident symptomatic peripheral arterial disease among individuals with diabetes mellitus: Insights from the Malmö Diet and Cancer Study. Ther. Adv. Endocrinol. Metabol. 2019, 10, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Look AHEAD Research Group; Wing, R.R.; Bolin, P.; Brancati, F.L.; Bray, G.A.; Clark, J.M.; Coday, M. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N. Engl. J. Med. 2013, 369, 145–154. [Google Scholar] [PubMed] [Green Version]
- Soliman, G.A. Dietary fiber, atherosclerosis, and cardiovascular disease. Nutrients 2019, 11, 1155. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Je, Y. Dietary fibre intake and mortality from cardiovascular disease and all cancers: A meta-analysis of prospective cohort studies. Arch. Cardiovasc. Dis. 2016, 109, 39–54. [Google Scholar] [CrossRef] [Green Version]
- Hartley, L.; May, M.D.; Loveman, E.; Colquitt, J.L.; Rees, K. Dietary fibre for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2016, 1, CD011472. [Google Scholar] [CrossRef]
- Wallström, P.; Sonestedt, E.; Hlebowicz, J.; Ericson, U.; Drake, I.; Persson, M.; Gullberg, B.; Hedblad, B.; Wirfält, E. Dietary fiber and saturated fat intake associations with cardiovascular disease differ by sex in the Malmö Diet and Cancer cohort: A prospective study. PLoS ONE 2012, 7, e31637. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Otto, M.C.; Mozaffarian, D.; Kromhout, D.; Bertoni, A.G.; Sibley, C.T.; Jacobs, D.R., Jr.; Nettleton, J.A. Dietary intake of saturated fat by food source and incident cardiovascular disease: The multi-ethnic study of atherosclerosis. Am. J. Clin. Nutr. 2012, 96, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattisson, I.; Wirfält, E.; Andrén, C.; Gullberg, B.; Berglund, G. Dietary fat intake—Food sources and dietary correlates in the Malmö Diet and Cancer cohort. Public Heal. Nutr. 2003, 6, 559–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abete, I.; Romaguera, D.; Vieira, A.R.; Lopez de Munain, A.; Norat, T. Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality: A meta-analysis of cohort studies. Br. J. Nutr. 2014, 112, 762–775. [Google Scholar] [CrossRef]
- Micha, R.; Wallace, S.K.; Mozaffarian, D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: A systematic review and meta-analysis. Circulation 2010, 121, 2271–2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and processed meat consumption and mortality: Dose–response meta-analysis of prospective cohort studies. Public Health Nutr. 2015, 19, 893–905. [Google Scholar] [CrossRef] [Green Version]
- Micha, R.; Michas, G.; Mozzaffarian, D. Unprocessed red and processed meats and risk of coronary artery disease and type 2 diabetes–an updated review of the evidence. Curr. Atheroscler. Rep. 2012, 14, 515–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensink, R.P. Effects of Saturated Fatty Acids on Serum Lipids and Lipoporoteins: A Systematic Review and Regression Analysis; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Moholdt, T.; Lavie, C.J.; Nauman, J. Sustained physical activity, not weight loss, associated with improved survival in coronary heart disease. J. Am. Coll. Cardiol. 2018, 71, 1094–1101. [Google Scholar] [CrossRef]
- Steell, L.; Ho, F.; Sillars, A.; Rocha, F.P.; Li, H.; Lyall, D.M.; Iliodromiti, S.; Welsh, P.; Anderson, J.; Mackay, D.F.; et al. Dose-response associations of cardiorespiratory fitness with all-cause mortality and incidence and mortality of cancer and cardiovascular and respiratory diseases: The UK Biobank cohort study. Br. J. Sports Med. 2019, 53, 1371–1378. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Manjer, J.; Carlsson, S.; Elmståhl, S.; Gullberg, B.; Janzon, L.; Lindström, M.; Berglund, G.; Mattisson, I. The Malmö Diet and cancer Study: Representativity, cancer incidence and mortality in participants and non-participants. Eur. J. Cancer Prev. 2001, 10, 489–499. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.G.; Platonov, P.G.; Hedblad, B.; Engström, G.; Melander, O. Atrial fibrillation in the Malmö Diet and Cancer study: A study of occurrence, risk factors and diagnostic validity. Eur. J. Epidemiol. 2010, 25, 95–102. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Incident Atherosclerotic Cardiovascular Disease (n = 5858) | No Incident Atherosclerotic Cardiovascular Disease (n = 21,132) | Age-and Sex Adjusted HR (95% CI) | Multivariable * Adjusted HR (95% CI) | |
|---|---|---|---|---|
| Male sex (%) | 2991 (51.1) | 7290 (34.5) | 1.85 (1.75–1.95) | 1.79 (1.68–1.90) |
| Age (years) | 61.8 (55.5–66.2) | 56.1 (50.3–63.0) | 1.81 a (1.76–1.86) | 1.78 a (1.72–1.84) |
| Total energy intake (kcal/day) | 2223.1 (1840.4–2703.9) | 2174.6 (1815.0–2611.8) | 0.95 a (0.92–0.98) | 0.99 a (0.96–1.02) |
| BMI (kg/m2) | 25.9 (23.5–28.4) | 25.1 (22.8–27.7) | 1.10 a (1.07–1.13) | 1.06 a (1.03–1.10) |
| Hypertension (%) | 4318/5842 (73.9) | 11,983/21,092 (56.8) | 1.52 (1.43–1.62) | 1.50 (1.41–1.60) |
| Diabetes mellitus (%) | 480 (8.2) | 607 (2.9) | 2.36 (2.15–2.60) | 2.26 (2.05–2.49) |
| Alcohol Consumption (%) | ||||
| Zero-consumers | 455 (7.8) | 1261 (6.0) | 1.15 (1.04–1.29) | 1.10 (0.98–1.23) |
| Quintile 1 (<0.9 g/day for women/<3.4 g/day for men) | 1234 (21.1) | 3766 (17.8) | 1 (Ref) | 1 (Ref) |
| Quintile 2 (0.9–4.3 g/day for women/3.4–9.1 g/day for men) | 1181 (20.2) | 3852 (18.2) | 0.91 (0.84–0.98) | 0.95 (0.87–1.03) |
| Quintile 3 (4.4–8.1 g/day for women/9.2–15.7 g/day for men) | 1056 (18.0) | 4023 (19.0) | 0.80 (0.74–0.87) | 0.87 (0.79–0.94) |
| Quintile 4 (8.2–14.0 g/day for women/15.7–25.7 g/day for men) | 973 (16.6) | 4095 (19.4) | 0.78 (0.72–0.85) | 0.84 (0.77–0.92) |
| Quintile 5 (>14.0 g/day for women/>25.7 g/day for men) | 959 (16.4) | 4135 (19.6) | 0.86 (0.79–0.94) | 0.88 (0.80–0.96) |
| Smoking (%) | ||||
| Never | 1886/5853 (32.2) | 8519/21,125 (40.3) | 1 (Ref) | 1 (Ref) |
| Former | 1882/5853 (32.2) | 7057/21,125 (33.4) | 1.17 (1.09–1.25) | 1.18 (1.10–1.26) |
| Current | 2085/5853 (35.6) | 5549/21,125 (26.3) | 2.16 (2.02–2.31) | 2.24 (2.10–2.40) |
| Leisure-Time Physical Activity (%) | ||||
| <7.5 MET-h/week | 667/5803 (11.5) | 1917/20,998 (9.1) | 1 (Ref) | 1 (Ref) |
| 7.5–15.0 MET-h/week | 935/5803 (16.1) | 3068/20,998 (14.6) | 0.84 (0.76–0.93) | 0.92 (0.83–1.02) |
| 15.1–25.0 MET-h/week | 1222/5803 (21.3) | 4941/20,998 (23.5) | 0.68 (0.62–0.75) | 0.77 (0.70–0.85) |
| 25.1–50.0 MET-h/week | 1992/5803 (21.1) | 7758/20,998 (36.9) | 0.69 (0.63–0.75) | 0.81 (0.73–0.88) |
| >50.0 MET-h/week | 987/5803 (17.0) | 3314/20,998 (15.8) | 0.71 (0.64–0.79) | 0.82 (0.74–0.91) |
| Educational Level (%) | ||||
| Less than 9 years | 3020/5840 (51.7) | 8143/21,088 (38.6) | 1 (Ref) | 1 (Ref) |
| Elementary school (9–10 year) | 1379/5840 (23.6) | 5728/21,088 (27.2) | 0.83 (0.78–0.89) | 0.89 (0.84–0.96) |
| Elementary + upper secondary school (9–13 year) | 469/5840 (8.0) | 1937/21,088 (9.2) | 0.77 (0.70–0.86) | 0.86 (0.78–0.96) |
| University studies, no degree | 418/5840 (7.2) | 1940/21,088 (9.2) | 0.73 (0.65–0.81) | 0.82 (0.74–0.92) |
| University studies, with degree | 554/5840 (9.5) | 3340/21,088 (15.8) | 0.63 (0.57–0.69) | 0.74 (0.67–0.82) |
| Diet Quality | ||||
| Low (%) | 962 (16.4) | 3202 (15.2) | 1 (Ref) | 1 (Ref) |
| Medium (%) | 4134 (70.6) | 15,114 (71.5) | 0.85 (0.80–0.92) | 0.91 (0.84–0.98) |
| High (%) | 762 (13.0) | 2816 (13.3) | 0.82 (0.75–0.91) | 0.92 (0.83–1.01) |
| Diet score (0–6) | 3 (2–4) | 3 (2–4) | 0.95 (0.92–0.98)/ point increase | 0.94 (0.91–0.97)/ point increase |
| Dietary Components | ||||
| Saturated fat (E%) | 15.7 (13.6–18.5) | 15.8 (13.7) | 0.93 a (0.89–0.96) | 0.96 a (0.92–0.99) |
| Polyunsaturated fat (E%) | 5.8 (4.9–6.9) | 5.7 (4.8–6.8) | 1.02 a (0.99–1.05) | 1.02 a (0.99–1.05) |
| Sucrose (E%) | 8.0 (5.9–10.4) | 8.0 (6.1–10.3) | 0.96 a (0.93–0.99) | 1.01 a (0.98–1.04) |
| Fiber (g/MJ) | 2.1 (1.7–2.5) | 2.1 (1.8–2.6) | 0.88 a (0.84–0.93) | 0.93 a (0.89–0.98) |
| Vegetables and fruit (g/day) | 333.6 (229.5–455.6) | 351.5 (250.5–479.8) | 0.96 a (0.92–0.99) | 0.99 a (0.95–1.03) |
| Fish (g/week) | 284.4 (151.8–451.6) | 274.6 (148.4–434.3) | 0.93 a (0.91–0.96) | 0.95 a (0.93–0.98) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acosta, S.; Johansson, A.; Drake, I. Diet and Lifestyle Factors and Risk of Atherosclerotic Cardiovascular Disease—A Prospective Cohort Study. Nutrients 2021, 13, 3822. https://doi.org/10.3390/nu13113822
Acosta S, Johansson A, Drake I. Diet and Lifestyle Factors and Risk of Atherosclerotic Cardiovascular Disease—A Prospective Cohort Study. Nutrients. 2021; 13(11):3822. https://doi.org/10.3390/nu13113822
Chicago/Turabian StyleAcosta, Stefan, Anna Johansson, and Isabel Drake. 2021. "Diet and Lifestyle Factors and Risk of Atherosclerotic Cardiovascular Disease—A Prospective Cohort Study" Nutrients 13, no. 11: 3822. https://doi.org/10.3390/nu13113822
APA StyleAcosta, S., Johansson, A., & Drake, I. (2021). Diet and Lifestyle Factors and Risk of Atherosclerotic Cardiovascular Disease—A Prospective Cohort Study. Nutrients, 13(11), 3822. https://doi.org/10.3390/nu13113822