
Role of Citrus Fruit Juices in Prevention of Kidney Stone Disease (KSD): A Narrative Review


Abstract
:1. Introduction
2. Methods
2.1. Evidence Acquisition
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
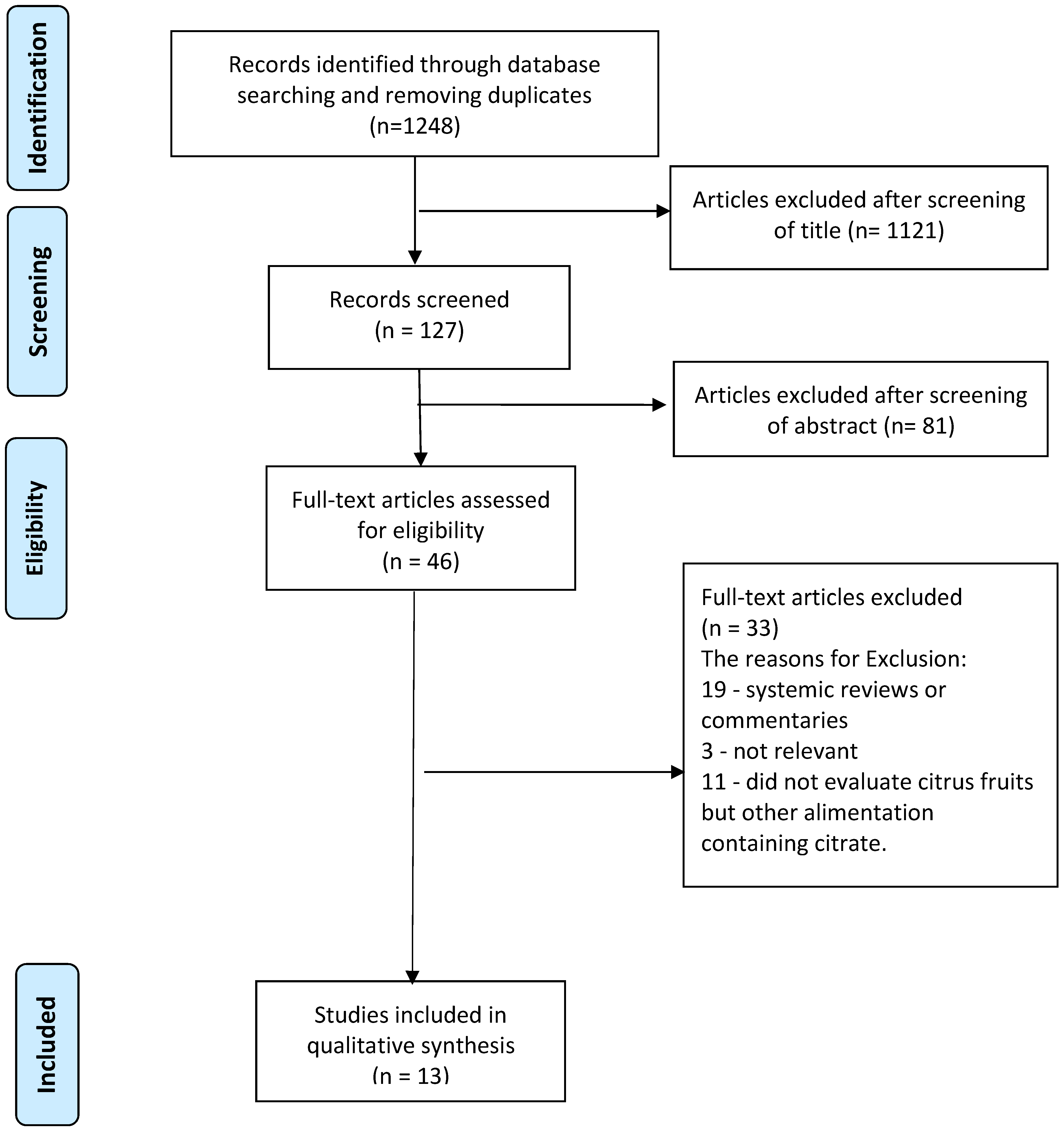
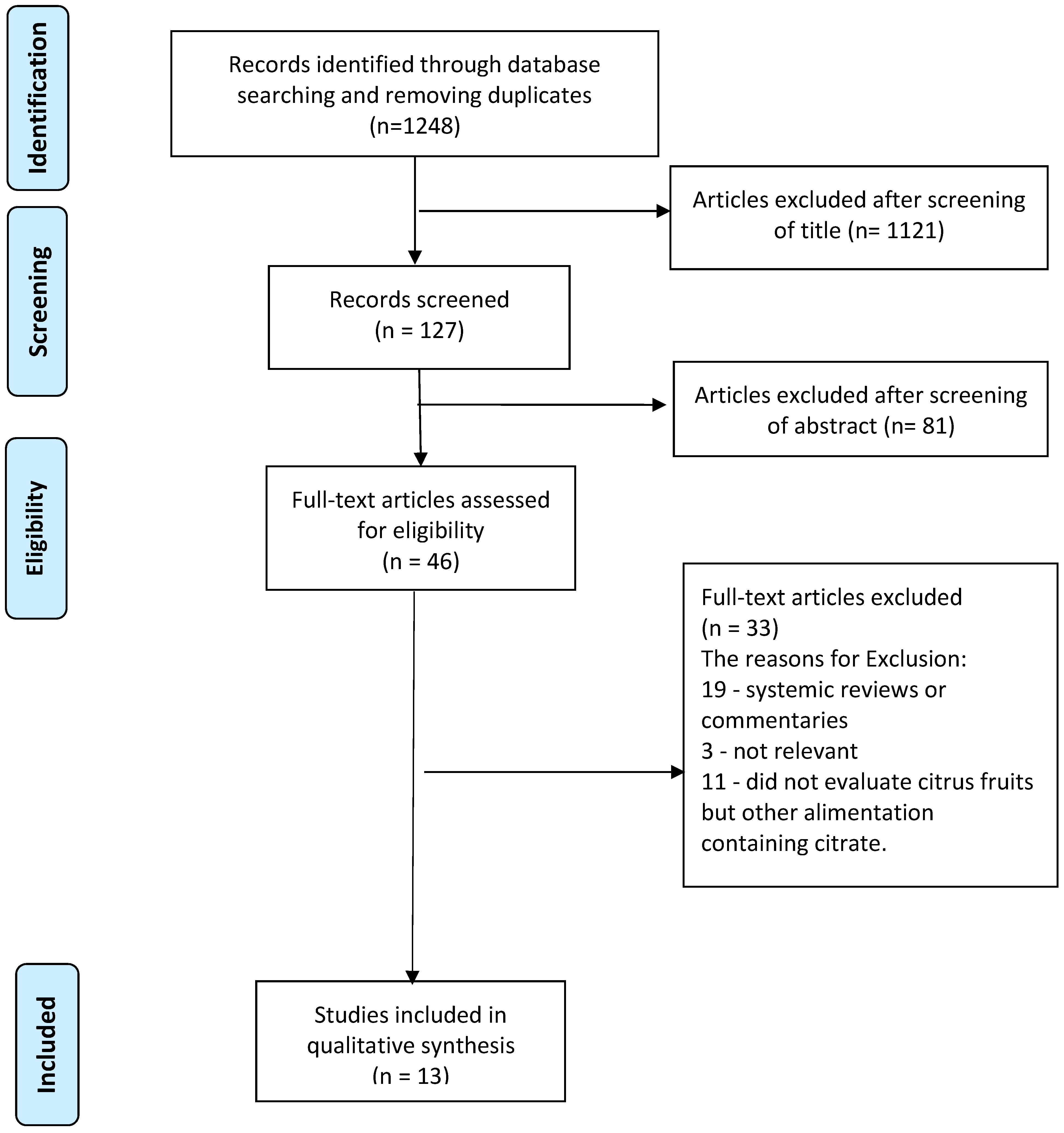
2.2. Search Strategy and Study Selection
3. Results
4. Discussion
4.1. Role of Citrus Juices, Mechanism of Action, and Comparison between Studies
4.2. Strengths, Limitations and Areas of Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| KSD | Kidney Stone Disease |
| CaOx | Calcium Oxalate |
References
- Curhan, G.C. Epidemiology of Stone Disease. Urol. Clin. N. Am. 2007, 34, 287–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daudon, M.; Traxer, O.; Lechevallier, E.; Saussine, C. Epidémiologie des lithiases urinaires. Prog. Urol. 2008, 18, 802–814. [Google Scholar] [CrossRef]
- Rukin, N.J.; Siddiqui, Z.A.; Chedgy, E.C.; Somani, B.K. Trends in Upper Tract Stone Disease in England: Evidence from the Hospital Episodes Statistics Database. Urol. Int. 2017, 98, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Letendre, J.; Cloutier, J.; Villa, L.; Valiquette, L. Metabolic evaluation of urinary lithiasis: What urologists should know and do. World J. Urol. 2014, 33, 171–178. [Google Scholar] [CrossRef]
- Türk, C.; Skolarikos, A.; Thomas, K. EAU Guidelines. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines (accessed on 10 November 2021).
- Pearle, M.; Preminger, G.; Turk, T.; White, J.R. AUA Guidelines on Medical Management of Kidney Stones (2019). Available online: https://www.auanet.org/guidelines/kidney-stones-medical-mangement-guideline (accessed on 10 November 2021).
- Gamage, K.N.; Jamnadass, E.; Sulaiman, S.K.; Pietropaolo, A.; Aboumarzouk, O.; Somani, B.K. The role of fluid intake in the prevention of kidney stone disease: A systematic review over the last two decades. Turk. J. Urol. 2020, 46, S92–S103. [Google Scholar] [CrossRef]
- Pattaras, J.G.; Moore, R.G. Citrate in the Management of Urolithiasis. J. Endourol. 1999, 13, 687–692. [Google Scholar] [CrossRef]
- Lemann, J., Jr.; Piering, W.F.; Lennon, E.J. Possible role of carbohydrate—Induced calciuria in calcium oxalate kidney stone formation. N. Engl. J. Med. 1969, 280, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Curhan, G.C.; Willett, W.C.; Rimm, E.B.; Spiegelman, D.; Stampfer, M.J. Prospective Study of Beverage Use and the Risk of Kidney Stones. Am. J. Epidemiol. 1996, 143, 240–247. [Google Scholar] [CrossRef]
- Curhan, G.C.; Willett, W.C.; Speizer, F.E.; Stampfer, M.J. Beverage use and risk for kidney stones in women. Ann. Intern. Med. 1998, 128, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, P.M.; Taylor, E.N.; Gambaro, G.; Curhan, G.C. Soda and Other Beverages and the Risk of Kidney Stones. Clin. J. Am. Soc. Nephrol. 2013, 8, 1389–1395. [Google Scholar] [CrossRef] [Green Version]
- Baia, L.D.C.; Baxmann, A.C.; Moreira, S.R.; Holmes, R.; Heilberg, I.P. Noncitrus Alkaline Fruit: A Dietary Alternative for the Treatment of Hypocitraturic Stone Formers. J. Endourol. 2012, 26, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Hönow, R.; Laube, N.; Schneider, A.; Kessler, T.; Hesse, A. Influence of grapefruit-, orange- and apple-juice consumption on urinary variables and risk of crystallization. Br. J. Nutr. 2003, 90, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odvina, C.V. Comparative Value of Orange Juice versus Lemonade in Reducing Stone-Forming Risk. Clin. J. Am. Soc. Nephrol. 2006, 1, 1269–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seltzer, M.A.; Low, R.K.; McDonald, M.; Shami, G.S.; Stoller, M.L. Dietary Manipulation with Lemonade to Treat Hypocitraturic Calcium Nephrolithiasis. J. Urol. 1996, 156, 907–909. [Google Scholar] [CrossRef]
- Wabner, C.L.; Pak, C.Y. Effect of Orange Juice Consumption on Urinary Stone Risk Factors. J. Urol. 1993, 149, 1405–1408. [Google Scholar] [CrossRef]
- Large, T.; Williams, J.C.; Asplin, J.R.; Krambeck, A. Using Low-Calorie Orange Juice as a Dietary Alternative to Alkali Therapy. J. Endourol. 2020, 34, 1082–1087. [Google Scholar] [CrossRef]
- Goldfarb, D.; Asplin, J.R. Effect of grapefruit juice on urinary lithogenicity. J. Urol. 2001, 166, 263–267. [Google Scholar] [CrossRef]
- Trinchieri, A.; Lizzano, R.; Bernardini, P.; Nicola, M.; Pozzoni, F.; Romano, A.-L.; Serrago, M.; Confalonieri, S. Effect of acute load of grapefruit juice on urinary excretion of citrate and urinary risk factors for renal stone formation. Dig. Liver Dis. 2002, 34, S160–S163. [Google Scholar] [CrossRef]
- Koff, S.G.; Paquette, E.L.; Cullen, J.; Gancarczyk, K.K.; Tucciarone, P.R.; Schenkman, N.S. Comparison Between Lemonade and Potassium Citrate and Impact on Urine pH and 24-Hour Urine Parameters in Patients with Kidney Stone Formation. Urology 2007, 69, 1013–1016. [Google Scholar] [CrossRef]
- Penniston, K.L.; Steele, T.H.; Nakada, S.Y. Lemonade Therapy Increases Urinary Citrate and Urine Volumes in Patients with Recurrent Calcium Oxalate Stone Formation. Urology 2007, 70, 856–860. [Google Scholar] [CrossRef]
- Jones, P.; Sulaiman, S.K.; Gamage, K.N.; Tokas, T.; Jamnadass, E.; Somani, B. Do Lifestyle Factors Including Smoking, Alcohol, and Exercise Impact Your Risk of Developing Kidney Stone Disease? Outcomes of a Systematic Review. J. Endourol. 2021, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, J.I.; Antonelli, J.A.; Pearle, M.S. Diet: From food to stone. World J. Urol. 2014, 33, 179–185. [Google Scholar] [CrossRef]
- Sulaiman, S.K.; Enakshee, J.; Traxer, O.; Somani, B.K. Which Type of Water Is Recommended for Patients with Stone Disease (Hard or Soft Water, Tap or Bottled Water): Evidence from a Systematic Review over the Last 3 Decades. Curr. Urol. Rep. 2020, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- De La Guéronnière, V.; Le Bellego, L.; Jimenez, I.B.; Dohein, O.; Tack, I.; Daudon, M. Increasing water intake by 2 litres reduces crys-t¬allisation risk indexes in healthy subjects. Arch. Ital. Urol. Androl. 2011, 83, 43–50. [Google Scholar]
- Pak, C.Y. Citrate and renal calculi: An update. Miner. Electrolyte Metab. 1994, 20, 7783699. [Google Scholar]
- Pak, C.Y. Citrate and Renal Calculi: New Insights and Future Directions. Am. J. Kidney Dis. 1991, 17, 420–425. [Google Scholar] [CrossRef]
- Goldberg, H.; Grass, L.; Vogl, R.; Rapoport, A.; Oreopoulos, D.G. Urine citrate and renal stone disease. Can. Med. Assoc. J. 1989, 141, 217–221. [Google Scholar]
- Hamm, L.L. Renal handling of citrate. Kidney Int. 1990, 38, 728–735. [Google Scholar] [CrossRef] [Green Version]
- Simpson, D.P. Citrate excretion: A window on renal metabolism. Am. J. Physiol. Physiol. 1983, 244, F223–F234. [Google Scholar] [CrossRef]
- Zuckerman, J.M.; Assimos, D.G. Hypocitraturia: Pathophysiology and Medical Management. Rev. Urol. 2009, 11, 134–144. [Google Scholar]
- Corrales, M.; Doizi, S.; Barghouthy, Y.; Traxer, O.; Daudon, M. Classification of Stones According to Michel Daudon: A Narrative Review. Eur. Urol. Focus 2021, 7, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Rimer, J.D.; Sakhaee, K.; Maalouf, N.M. Citrate therapy for calcium phosphate stones. Curr. Opin. Nephrol. Hypertens. 2019, 28, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Haleblian, G.E.; Leitao, V.A.; Pierre, S.A.; Robinson, M.R.; Albala, D.M.; Ribeiro, A.A.; Preminger, G.M. Assessment of Citrate Concentrations in Citrus Fruit-Based Juices and Beverages: Implications for Management of Hypocitraturic Nephrolithiasis. J. Endourol. 2008, 22, 1359–1366. [Google Scholar] [CrossRef]
- Penniston, K.L.; Nakada, S.Y.; Holmes, R.; Assimos, D.G. Quantitative Assessment of Citric Acid in Lemon Juice, Lime Juice, and Commercially-Available Fruit Juice Products. J. Endourol. 2008, 22, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Maalouf, N.M. Nephrolithiasis. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Herder, W.W., Dhataria, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2020. [Google Scholar]
- Gridley, C.M.; Sourial, M.W.; Lehman, A.; Knudsen, B.E. Medical dissolution therapy for the treatment of uric acid nephrolithiasis. World J. Urol. 2019, 37, 2509–2515. [Google Scholar] [CrossRef] [PubMed]
- Embil, K.; Litwiller, D.C.; Lepore, R.A.; Field, F.P.; Torosian, G. Effect of Orange Juice Consumption on Urinary pH. Am. J. Health Pharm. 1976, 33, 1294–1297. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Bargagli, M.; Trinchieri, A.; Gambaro, G. Risk of Kidney Stones: Influence of Dietary Factors, Dietary Patterns, and Vegetarian–Vegan Diets. Nutrients 2020, 12, 779. [Google Scholar] [CrossRef] [Green Version]
- Littlejohns, T.J.; Neal, N.L.; Bradbury, K.; Heers, H.; Allen, N.E.; Turney, B.W. Fluid Intake and Dietary Factors and the Risk of Incident Kidney Stones in UK Biobank: A Population-based Prospective Cohort Study. Eur. Urol. Focus 2020, 6, 752–761. [Google Scholar] [CrossRef] [Green Version]
- Barilla, D.E.; Townsend, J.; Pak, C.Y. An exaggerated augmentation of renal calcium excretion after oral glucose ingestion in patients with renal hypercalciuria. Investig. Urol. 1978, 15, 486–488. [Google Scholar]
- Walker, R.W.; Dumke, K.A.; Goran, M.I. Fructose content in popular beverages made with and without high-fructose corn syrup. Nutrition 2014, 30, 928–935. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author. | Year | Study Type | Orange/Grapefruit/Lemon | Sample Size | Assessment | Study Goal | Conclusion |
|---|---|---|---|---|---|---|---|
| Curhan [10] | 1996 | Prospective cohort study | Orange, Grapefruit | 45,289 | Questionnaire | The relation between intake of 21 different beverages and the risk of symptomatic kidney stones in men. | Grapefruit juice was directly associated with risk of stone formation. No increased risk for orange juice consumption. |
| Curhan [11] | 1998 | Prospective cohort study | Orange, Grapefruit | 81,093 | Questionnaire | The association between the intake of 17 beverages and risk for kidney stones in women. | Grapefruit juice was directly associated with risk of stone formation. No increased risk for orange juice consumption. |
| Ferraro [12] | 2013 | Prospective cohort study | Orange, Grapefruit | 217,883 | Questionnaire | The association between intake of several types of beverages and incidence of kidney stones. | Protective effect for the consumption of orange juice. Risk of grapefruit juice not significant. |
| Baia [13] | 2012 | Prospective clinical study | Orange, Lime | 30 hypocitraturic stone forming patients | Urine analyses | To compare the acute effects of a non-citrus fruit (melon) vs. citrus fruits (orange and lime) on citraturia and other lithogenic parameters. | Significant and comparable increases of mean urinary citrate were observed in all groups. Mean urinary pH significantly increased after orange juice but not after lime juice consumption. |
| Hönow [14] | 2003 | Prospective clinical study | Orange, Grapefruit | 9 non-stone formers | Urine analyses | To evaluate the influence of grapefruit and apple juice consumption on urinary variables and crystallization, in comparison with orange juice. | Both grapefruit juice and apple juice reduce the risk of CaOx stone formation at a magnitude comparable with the effects obtained from orange juice. |
| Odvina [15] | 2006 | Prospective randomized study | Orange, Lemonade | 13 volunteers (9 healthy and 4 stone formers) | Blood and urine analyses | To compare the effects of orange juice with those of lemonade on acid–base profile and urinary stone risks under controlled metabolic conditions. | Orange juice has greater alkalinizing and citraturic effects than lemonade. Orange juice is associated with lower calcium-oxalate supersaturation and lower uric acid. |
| Seltzer [16] | 1996 | Prospective clinical study | Lemonade | 12 hypocitraturic stone formers | Urine analyses | To evaluate the urinary biochemical effects of dietary citrate supplementation (lemonade). | Lemonade results in elevated urinary citrate levels and can be a possible treatment in hypocitraturic calcium stone formers. |
| Wabner [17] | 1993 | Prospective clinical study | Orange | 13 volunteers (8 healthy and 3 hypocitraturic stone formers) | Urine analyses | To evaluate the urinary biochemical effects of orange juice compared to potassium citrate. | Compared to potassium citrate, orange juice caused a similar increase in urinary pH and urinary citrate but increased urinary oxalate and did not reduce calcium excretion. |
| Large [18] | 2020 | Prospective randomized study | Orange, Artificial lemonade | 10 non-stone formers | Urine analyses | To evaluate urinary citrate and pH changes with consumption of low-calorie orange juice and artificial lemonade. | Daily consumption of orange juice can raise urinary pH. |
| Goldfarb [19] | 2001 | Prospective clinical study | Grapefruit | 10 non-stone formers | Urine analyses | To study the basis of the lithogenic effect of grapefruit juice demonstrated in epidemiologic studies. | Grapefruit juice associated with an increase in mean oxalate and citrate excretion. However, no net change in calculated supersaturation or lithogenicity. |
| Trinchieri [20] | 2002 | Prospective clinical study | Grapefruit | 7 non-stone formers | Urine analyses | To investigate changes in urinary stone risk factors after consumption of grapefruit juice. | Grapefruit juice significantly increases urinary excretion of citrate, calcium, and magnesium. |
| Penniston [21] | 2007 | Retrospective analysis | Lemonade | 100 CaOx stone formers | Urine analyses | To evaluate the urinary biochemical effects of lemonade compared to K-citrate + lemonade. | Lemonade raised urinary citrate and total urine volume but was less effective than K-citrate + lemonade. |
| Koff [22] | 2007 | Prospective clinical trial | Lemonade | 21 stone formers | Urine analyses | To evaluate the urinary biochemical effects of lemonade compared to potassium citrate. | Lemonade did not increase urinary citrate or pH levels. |
| U-pH | U-Citrate | U-Potassium | U-Oxalate | U-Calcium | CaOx Crystallization Risk | |
|---|---|---|---|---|---|---|
Baia [13]
| Increase Increase NS change | Increase Increase Increase | NS Increase Increase NS change | Not measured (N/A) | N/A | N/A |
Hönow [14]
| NS Increase Increase Increase | Increase Increase Increase | Increase Increase Increase | NS Increase NS Increase NS Increase | Decrease Decrease NS decrease | Decrease NS Decrease NS Decrease |
Odvina [15]
| NS change Increase | NS Increase Increase | NS change Increase | No Significant Change Increase | NS Decrease NS Decrease | NS Decrease Decrease |
Seltzer [16]
| Not Measured | Increase | N/A | NS change | NS Decrease | N/A |
Wabner [17]
| Increase | Increase | Increase | Increase | NS Decrease | NS Change |
Large [18]
| Increase | Increase | NS Increase for Orange Juice No Change for Lemonade | NS Increase for Orange Juice No Change for Lemonade | NS changes | N/A |
Goldfarb [19]
| NS Increase | Increase | Increase | Increase | NS Decrease | No Change |
Trinchieri [20]
| NS Decrease | Increase | NS Decrease | NS Increase | NS Increase | No Change |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barghouthy, Y.; Somani, B.K. Role of Citrus Fruit Juices in Prevention of Kidney Stone Disease (KSD): A Narrative Review. Nutrients 2021, 13, 4117. https://doi.org/10.3390/nu13114117
Barghouthy Y, Somani BK. Role of Citrus Fruit Juices in Prevention of Kidney Stone Disease (KSD): A Narrative Review. Nutrients. 2021; 13(11):4117. https://doi.org/10.3390/nu13114117
Chicago/Turabian StyleBarghouthy, Yazeed, and Bhaskar K. Somani. 2021. "Role of Citrus Fruit Juices in Prevention of Kidney Stone Disease (KSD): A Narrative Review" Nutrients 13, no. 11: 4117. https://doi.org/10.3390/nu13114117
APA StyleBarghouthy, Y., & Somani, B. K. (2021). Role of Citrus Fruit Juices in Prevention of Kidney Stone Disease (KSD): A Narrative Review. Nutrients, 13(11), 4117. https://doi.org/10.3390/nu13114117